
Abstract
Summary box
What is already known about this topic?
What is already known about this topic?A new variant of concern of SARS-CoV-2 (P.1). emerged in the city of Manaus in November 2020. Since then, a sharp increase in COVID-19 cases in Manaus led to the collapse of the health system in early 2021.
What is added by this report?
What is added by this report?Transmissibility and reinfection of P.1 were estimated using an epidemiological model-based fitting and public health data. The transmissibility is 2.5 times greater than the wild variant and reinfection probability is 6.4% on average.
What are the implications for public health practice?
What are the implications for public health practice?This new variant poses a global threat due to its very high transmissibility. The results highlight the need to urgently monitor and contain its spread.
Introduction
The variant of concern (VOC) P.1 emerged in the Amazonas state (Brazil) and was sequenced for the first time on 6-Jan-2021 by the Japanese National Institute of Infectious Diseases. It contains a constellation of mutations, ten of them in the spike protein. Consequences of these mutations at the populational level have been poorly studied so far. From December-2020 to February-2021, Manaus was devastated by four times more cases compared to the previous peak (April-2020). Here, data from the national health surveillance of hospitalized individuals were analysed using a model-based approach to estimate P.1 parameters of transmissibility and reinfection by maximum likelihood. Sensitivity analysis was performed changing pathogenicity and the period analysed (including/excluding the health system collapse period). In all analysed cases, the new variant transmissibility was found to be about 2.5 times higher compared to the previous variant in Manaus. A low probability of reinfection by the new variant (6.4%) was estimated, even under initial high prevalence (68%) by the time P.1 emerged. Consequences of a higher transmissibility were already observed with VOC B.1.1.7 in the UK and Europe. Urgent measures must be taken to control the spread of P.1.
The National Institute of Infectious Diseases in Japan alerted about the new variant from travelers who have been in the state of Amazonas on 6-Jan-2021 (1). P.1 was first detected in Brazil in Manaus, the Amazonas state capital city on 11-Jan-2021 (2). Later, the same variant was identified in samples from Manaus dating from 6-Dec-2020 (3). According to phylogenetic studies, P.1 likely emerged in the Amazonas state in November of 2020, with no consensus when it occurred, if early (3) or late (4) November. The P.1 variant shares mutations such as E484K, K417T, and N501Y and a deletion in the orf1b protein (del11288-11296 (3675-3677 SGF)) with other VOCs previously detected in the United Kingdom and South Africa (B.1.1.7 and the B.1.351, respectively). From December 2020 to February 2021, after a period of high but relatively stable incidence, Manaus was devastated by a health system collapse and oxygen supplies shortage, which remained until the beginning of February 2021 (5). Prevalence of P.1 increased sharply from 0% in November 2020 to 73% in January 2021 and in less than 2 months replaced previous lineages (4). Effects at the population level of mutations P.1 variant carries are yet to be fully understood.
Methods
Dataset
This study uses the Brazillian epidemiological syndromic surveillance system for influenza, SIVEP-Gripe (publicly available at https://opendatasus.saude.gov.br), to track COVID-19 hospitalized cases. All patients with Severe Acute Respiratory Infections (SARI) that are hospitalized must be reported with first symptoms onset date and tested for SARS-CoV-2. Data of Manaus residents from 01-Nov-2020 to 31-Jan-2021 were fitted using the database published on 15-Feb-2021. The last 10 weeks of hospitalization cases time series were estimated via nowcasting (6) to correct for notification delay. Time-series of relative frequency of sequenced genomes identified as P.1 in Manaus was extracted from published datasets. (3,7)
Model
An extended SEIR deterministic compartmental model (SEAIHRD, see Figure 1) was developed. It models the infection of Susceptible individuals transiting to the Exposed (pre-symptomatic) compartment, who can progress to three alternative compartments: Hospitalized (severely ill), Infected (symptomatic but non-hospitalized), and Asymptomatic. Eventually, individuals transit to Recovered or Deceased. Two variants are considered: 1-wild and 2-new/P.1. The latter is assumed to infect Recovered individuals previously infected by the wild type, and no reinfections of wild type due to waning immunity occur. Dynamics is replicated for three age classes: young (<20y.o.), adult (≥20 and <60y.o.) and elderly (≥60y.o.), with different rates for outcomes (symptoms, hospitalizations, and deaths). Twenty-four out of 29 model parameters are fixed, using current values from the literature. Further details of the model are available in the Supplementary Material (SM).
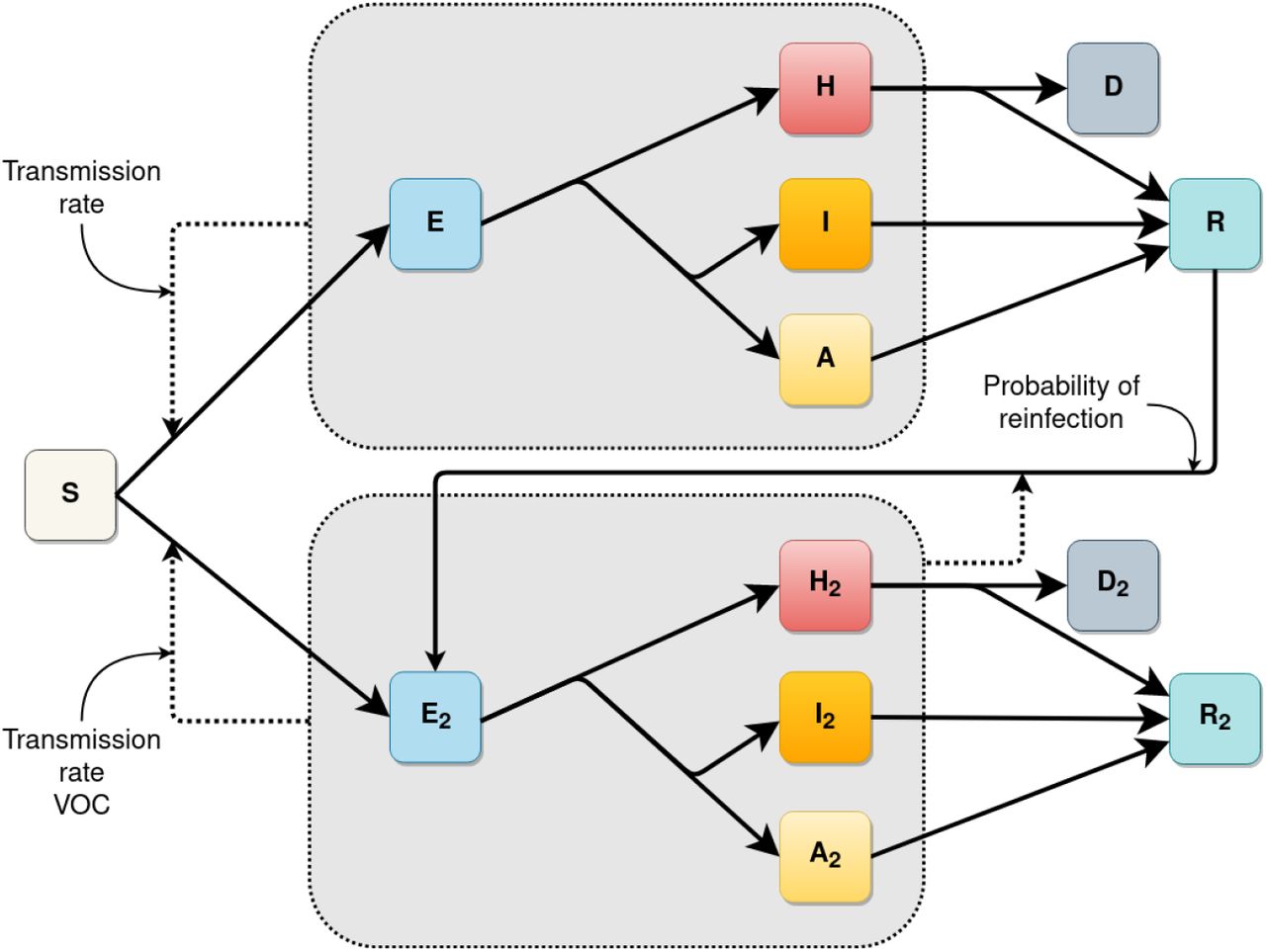
Diagram of the SEAIHRD model. S: Susceptible, E: Exposed (pre-symptomatic), H: Hospitalized (severe infected individuals), I: Infected (symptomatic individuals, not hospitalized), A: Asymptomatic. D: Deceased, R: Recovered. All the compartments are subdivided into 3 age classes, not represented here for simplicity. Compartments with no subindex are related to the wild variant, compartments with subindex 2 are related to the VOC P.1. Continuous lines represent flux between each compartment. Dashed lines represent infection pathways. Three parameters fitted by the model are indicated by the small arrows.
Estimation of transmissibility rate and reinfection probability
Relative transmissibility and reinfection probability of P.1 were estimated by a maximum likelihood fitting to the weekly number of new hospitalizations and to genomic surveillance data (3,7). Other three nuisance parameters were also fitted, namely, fraction of cases at the beginning of simulation that were caused by the new variant, total infection prevalence at the emergence of the variant (assumed to be 01-Nov-2020), and intrinsic growth rate of the wild variant, which comprises effects related to contact rates, such as non-pharmacological interventions relaxation, elections, and others. Hospitalization counts and recorded numbers of P.1 cases were assumed to follow Poisson and binomial distributions, respectively. The set of parameters values that provide the best fit to the data was found by computational minimization of the negative log-likelihood. Further details about fitting procedures are available in the SM.
Sensitivity analysis
The estimation assumes a constant Infection Hospitalization Rate (IHR) for each age group over time for both variants. An increase in IHR caused by P.1 would increase the number of hospitalizations even without any increase in transmissibility or reinfection. Since the pathogenicity of the P.1 variant is unknown, the model fitting was repeated assuming that the odds ratio of the IHR in each age class was twice for P.1 cases compared to wild variant cases (SA1). Moreover, as the collapse of Manaus health system hindered hospitalizations of new severe cases and may have affected case recording in surveillance databases, the model fitting was repeated considering only the period prior to the collapse (10-Jan-2021) (SA2).
Results
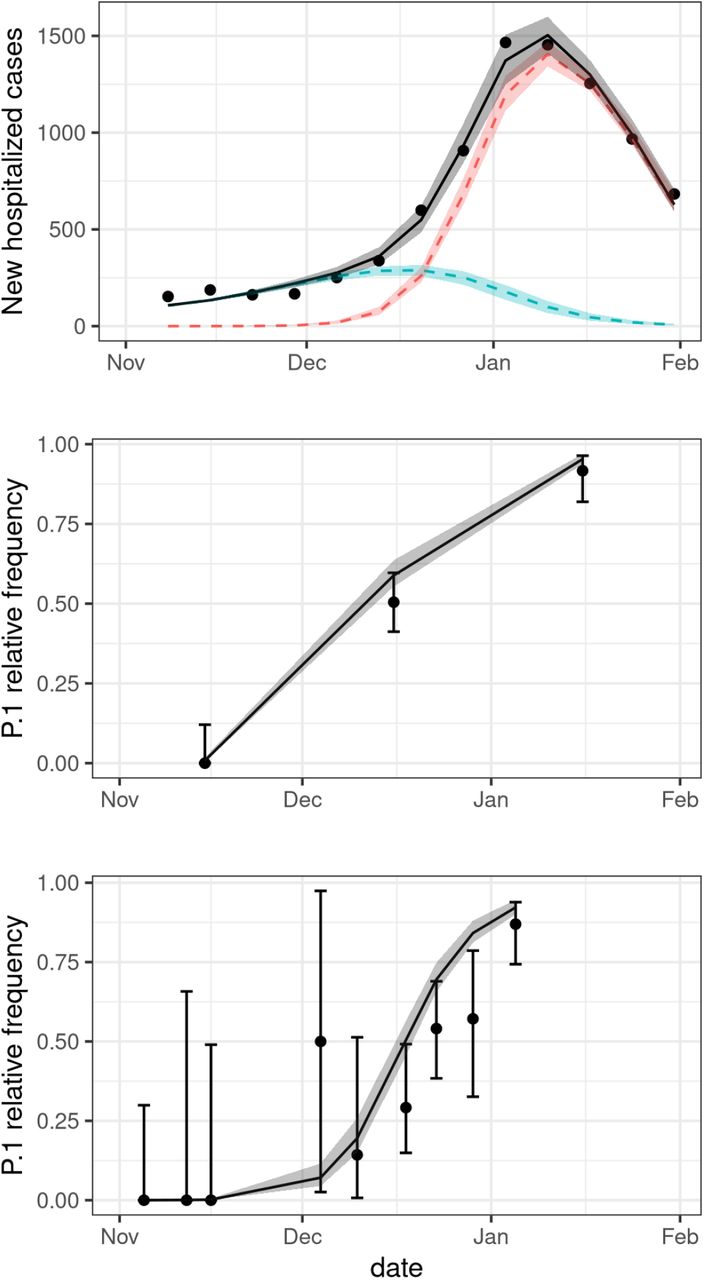
The estimated relative transmissibility of P.1 is 2.5 (95% CI: 2.3-2.8) times higher than the infection rate of the wild variant, while the reinfection probability due to the new variant is 6.4% (95% CI: 5.7 - 7.1%). The model also estimated that, at the time the new variant emerged, the prevalence of the wild variant was 68% (95% CI: 63-74%), and that the number of cases by the wild variant were increasing, with an estimated daily intrinsic growth rate of cases of 0.053 days-1 (0.047-0.058 days-1). See Table 1 and Fig. 2 for fitted parameters results.
The first part of the table summarizes the fitted parameters and respective confidence intervals considering the entire period between November 1, 2020 and January 31, 2021 and the same pathogenicity of the previous variant. In the second part of the table, the sensitivity analysis is presented: SA1 considers greater pathogenicity of the P.1 variant. SA2 considers the data censured on 10-Jan-2021 (before the collapse).

{kind=link}
{kind=link}
First panel: Weekly new hospitalized COVID-19 cases in Manaus city. Grey line represents the fitted values of total cases (all variants) by maximum likelihood estimation (MLE) of the parameters. Red (blue) line represents the fitted values of cases due to P.1 (wild) variant, black dots are nowcasted observed data of hospitalization. Second and third panels show the fittings to the P.1 time-series frequency of P.1 on datasets provided by (7) and (3) respectively. The area around the lines indicate the 95% CI of the expected values. The fitted values of the model parameters are presented in the first part of Table 1.
For the model with increased IHR of P.1 cases (SA1, Table 1), the estimated relative transmissibility didn’t change much (2.6, 2.3-2.8), nor did the estimated prevalence (68%, 49-82%). The estimated probability of reinfection by this model was three times lower, but with a wider confidence interval (2.0%, 0.2-19.0%). Estimates from data up to 10-Jan-2021 were even larger for transmissibility (SA2, Table 1).
Discussion
Reported COVID-19 hospitalizations and the frequency of the P.1 variant in clinical samples showed a sharp increase in Manaus starting November 2020. The fitted model suggests this joint increase was the result of the emergence of P.1, estimated to be 2.5 times more transmissible than the wild variant. The spread of P.1 occurred despite an existing high estimated prevalence of infection by the wild virus and a small probability of reinfection by the invading variant. The pathogenicity of P.1 is still unknown, but even assuming higher Infection Hospitalization Rates for the P.1 variant, the estimated transmissibility remained above twice that of the wild variant.
Two recent studies analysed genomic data of SARS-CoV-2 from Manaus evaluating the transmissibility of the new variant. Faria and collaborators (3) integrated mortality and genomic data, and by using a semi-mechanistic Bayesian model, estimated a transmissibility 1.4–2.2 times higher and 25-61% evasion of protective immunity related to the P.1 variant. Naveca and collaborators (4) estimated a 2.2 times higher effective reproduction number (Re) for the P.1 variant using phylogenetic methods, and suggested that P.1 can be at least two times more transmissible than the parental lineage, assuming reinfections as rare events. The present work follows a different approach that can be defined as an epidemiological, model based, and data fitting approach. It is worth mentioning that, using different approaches the three studies (the abovementioned and this work) have found similar results: higher transmissibility of the variant P.1.
Data from the Amazonian region are scarce. The existing prevalence data were obtained from convenience samples and P.1 frequency over time is based on small sample sizes. With the collapse of the healthcare system it can be inferred that epidemiological data are incomplete, which poses limitations to this study, that were minimized by a very rigorous analytic approach, that led us to reach similar results to other recent studies conducted in Manaus.
The consequences of the introduction of a highly transmissible variant have already been observed with VOC B.1.1.7 in the UK, USA and Europe. Higher transmissibility of the P.1 variant raises important concerns about the possibility of more accelerated upsurges in the number of cases once P.1 spreads in the community in other parts of Brazil as well. This calls for urgent mitigation measures to control the spread of P.1.
Data Availability
All data used are publicly available. The data sources are described in the manuscript and in supplementary file.
Funding
This work was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brazil (Finance Code 001 to FMDM, LSF and TPP), Conselho Nacional de Desenvolvimento Científico e Tecnológico – Brazil (grant number: 315854/2020-0 to MEB, 141698/2018-7 to RLPS, 313055/2020-3 to PIP, 312559/2020-8 to MASMV, 311832/2017-2 to RAK, 305703/2019-6 to AAMS) and Fundação de Amparo à Pesquisa do Estado de São Paulo-Brazil (grant number: 2019/26310-2 and 2017/26770-8 to CF, 2018/26512-1 to OC, 2018/24037-4 to SPL and contract number: 2016/01343-7 to RAK).



