
Abstract
Background Multiple COVID-19 vaccines appear to be safe and efficacious, but only high-income countries have the resources to procure sufficient vaccine doses for most of their eligible populations. The World Health Organization has published guidelines for vaccine prioritisation, but most vaccine impact projections have focused on high-income countries, and few incorporate economic considerations. To address this evidence gap, we projected the health and economic impact of different vaccination scenarios in Sindh province, Pakistan (population: 48 million).
Methods and Findings We fitted a compartmental transmission model to COVID-19 cases and deaths in Sindh from 30 April to 15 September 2020. We then projected cases, deaths, and hospitalization outcomes over 10 years under different vaccine scenarios. Finally, we combined these projections with a detailed economic model to estimate incremental costs (from healthcare and partial societal perspectives), disability adjusted life years (DALYs), and incremental cost-effectiveness ratio (ICER) for each scenario.
We project that one-year of vaccine distribution, at delivery rates consistent with COVAX projections, using an infection-blocking vaccine at $3/dose with 70% efficacy and 2.5 year duration of protection is likely to avert around 0.9 (95% Credible Interval: 0.9, 1.0) million cases, 10.1 (95% CrI: 10.1, 10.3) thousand deaths and 70.1 (95% CrI: 69.9, 70.6) thousand DALYs, with an ICER of $27.9 per DALY averted from the health system perspective. Varying these assumptions, we generally find that prioritizing the older (65+) population prevents more deaths, but broad distribution from the outset is economically comparable in many scenarios, and either scheme can be cost-effective for low per-dose costs. However, high vaccine prices ($10/dose) may not be cost-effective.
The principal drivers of the health outcomes are the fitted values for the overall transmission scaling parameter and disease natural history parameters from other studies, particularly age specific probabilities of infection and symptomatic disease, as well as social contact rates. Other parameters are investigated in sensitivity analyses.
These projections are limited by the mechanisms present in the model. Because the model is a single-population compartmental model, detailed impacts of non-pharmaceutical interventions (NPIs) such as household isolation cannot be practically represented or evaluated in combination with vaccine programmes. Similarly, the model cannot consider prioritizing groups like healthcare or other essential workers. Additionally, because the future impact and implementation cost of NPIs is uncertain, how these would interact with vaccination remains an open question.
Conclusions COVID-19 vaccination can have a considerable health impact, and is likely to be cost-effective if more optimistic vaccine scenarios apply. Preventing severe disease is an important contributor to this impact, but the advantage of focusing initially on older, high-risk populations may be smaller in generally younger populations where many people have already been infected, typical of many low- and -middle income countries, as long as vaccination gives good protection against infection as well as disease.
Why Was This Study Done?
- The evidence base for health and economic impact of COVID-19 vaccination in low- and middle-income settings is limited.
- Searching PubMed, medRxiv, and econLit using the search term (“coronavirus” OR “covid” OR “ncov”) AND (“vaccination” OR “immunisation”) AND (“model” OR “cost” OR “economic”) for full text articles published in any language between 1 January 2020 and 20 January 2021, returned 29 (PubMed), 1,167 (medRxiv) and 0 (econLit) studies: 20 overall were relevant, with only 4 exclusively focused on low- or middle-income countries (India, China, Mexico), while 3 multi-country analyses also included low- or middle-income settings,
- However only three of these studies are considered economic outcomes, all of them comparing the costs of vaccination to the costs of non-pharmaceutical interventions and concluding that both are necessary to reduce infections and maximise economic benefit.
- The majority of studies are set in high-income settings and conclude that targeting COVID-19 vaccination to older age groups is the preferred strategy to minimise mortality, particularly when vaccine supplies are constrained, while other age- or occupational risk groups should be priorities when vaccine availability increases or when other policy objectives are pursued.
What Did the Researchers Do and Find?
- We combined epidemiological and economic analysis of COVID-19 vaccination based on real-world disease and programmatic information in the Sindh province of Pakistan.
- We found vaccination in this setting is likely to be highly cost-effective, and even cost saving, as long as the vaccine is reasonably priced and efficacy is high.
- Unlike studies in high-income settings, we also found that vaccination programmes targeting all adults may have almost as much benefit as those initially targeted at older populations, likely reflecting the higher previous infection rates and different demography in these settings.
What Do These Findings Mean?
- Lower- and middle-income countries (LMICs) and international bodies providing guidance for LMICs need to consider evidence specific to these settings when making recommendations about COVID-19 vaccination.
- Further data and model-based analyses in such settings are urgently needed in order to ensure that vaccination decisions are appropriate to these contexts.
Introduction
The Coronavirus Disease 2019 (COVID-19) pandemic has resulted in over 50 million cases and nearly 2 million deaths in 2020, with cases in nearly every country (1). To reduce transmission of the causal SARS-CoV-2 virus, many countries have imposed physical distancing measures such as closure of schools and workplaces, and restrictions on public gatherings (2). Such measures often incur socioeconomic costs that are not indefinitely sustainable, particularly in resource poor settings (3), and, when these measures are lifted, transmission has readily resumed in most places (4).
Vaccination may provide a durable option to protect individuals. If a vaccine also reduces transmission (e.g., by preventing infection or limiting infectiousness of disease), even unvaccinated individuals would have reduced infection risk. As of January 2021, 3 vaccines have completed phase III trials and at least 20 other vaccine candidates were in phase III trials, with over 250 in earlier trials or pre-clinical studies (5,6).
Many high-income and large middle-income countries have signed bilateral agreements with manufacturers, pre-ordering enough vaccines to cover their populations, some multiple times (7). However, many small and/or lower income countries individually lack the resources for such arrangements. The World Health Organization (WHO); Gavi, the Vaccine Alliance; and the Coalition for Epidemic Preparedness Innovations (CEPI) launched the COVAX Facility to enable these countries to pool their purchasing power. To date, 141 countries and territories have started the COVAX participation process, which will distribute vaccines to participating countries according to population size (8,9). This distribution will cover a small proportion (3%) of those populations in the months following vaccine approval, aiming to expand to 20% by the end of 2021 (10). Additionally, they face substantial other health sector resource constraints that may require external funding including scale-up of vaccine delivery infrastructure and workforce, and continued care and treatment of those with COVID-19.
The WHO’s Strategic Group of Experts on Immunization (SAGE) has issued a roadmap to help countries prioritise distribution of these limited doses. This roadmap draws from work across multiple disciplines, including modelling to project the health outcomes, health sector financing and broader economic consequences of different vaccine prioritisation strategies, but much of the available research has focused on high-income settings (11–14).
To address this gap, we assessed the health impact, economic impact and cost-effectiveness of COVID-19 vaccination in Sindh province, Pakistan, using a combined epidemiological and economic model. We chose a specific setting to ensure our model could incorporate local mobility and cost data. Sindh province initially confirmed a large number of cases, followed by declining incidence after a nationwide lockdown. Our analysis addresses vaccine prioritisation questions faced by both global (WHO) and national (Pakistan Ministry of Health) decision-makers, and illustrates the decision support analysis that should be applied more broadly in low- and middle-income countries.
Methods
Epidemiological model
To capture the natural history and transmission of SARS-CoV-2, we used a previously published compartmental model (15–17) tailored to the population of Sindh using population data from WorldPop (18) and assumed baseline population contact rates from previously estimated national patterns for Pakistan (19).
Briefly, the model compartments are an extended SEIRS+V (Susceptible, Exposed, Infectious with multiple sub-compartments, Recovered and/or Vaccinated, potentially converting either to Susceptible or if in the combined state to only Recovered or Vaccinated) system with births, deaths, and age structure. For all compartments other than Recovered and/or Vaccinated, we use event-time distributions derived from global observations (Table 1). For Recovered and/or Vaccinated, we consider multiple characteristic protection durations, given the uncertainty in these durations. For the Recovered compartment (with and without vaccination), we assume perfect protection; we address the Vaccinated compartment protection along with the vaccination programme details in the “Vaccine Programme’’ section. The modelled loss of protection can represent a range of phenomena, from antibody waning to shifts in the circulating pathogen with time leading to immune escape.
We assumed that contact patterns changed over the course of the epidemic, and estimated these changes using Google Community Mobility indicators (20) for Sindh and school closures as reflected in the Oxford Coronavirus Government Response Tracker (2). For projections, we assume that contact patterns return to the baseline contract matrix at the end of May 2021, and no further physical distancing interventions are imposed.
Model fitting and projections
Using Bayesian inference via Markov Chain Monte Carlo, we fit five elements of the model: the effective introduction date, t0, as number of days after 1 January 2020; the basic reproduction number in Sindh without any interventions, R0; a time-varying ascertainment rate for both COVID-19 deaths and cases; and the standard deviation characterising the distribution of reported data points around the model-predicted mean value. We fitted the model to the new daily cases and deaths in Sindh reported by the Government of Pakistan COVID-19 Dashboard (21) from 30 April to 14 September 2020 (Figure 1A-B).
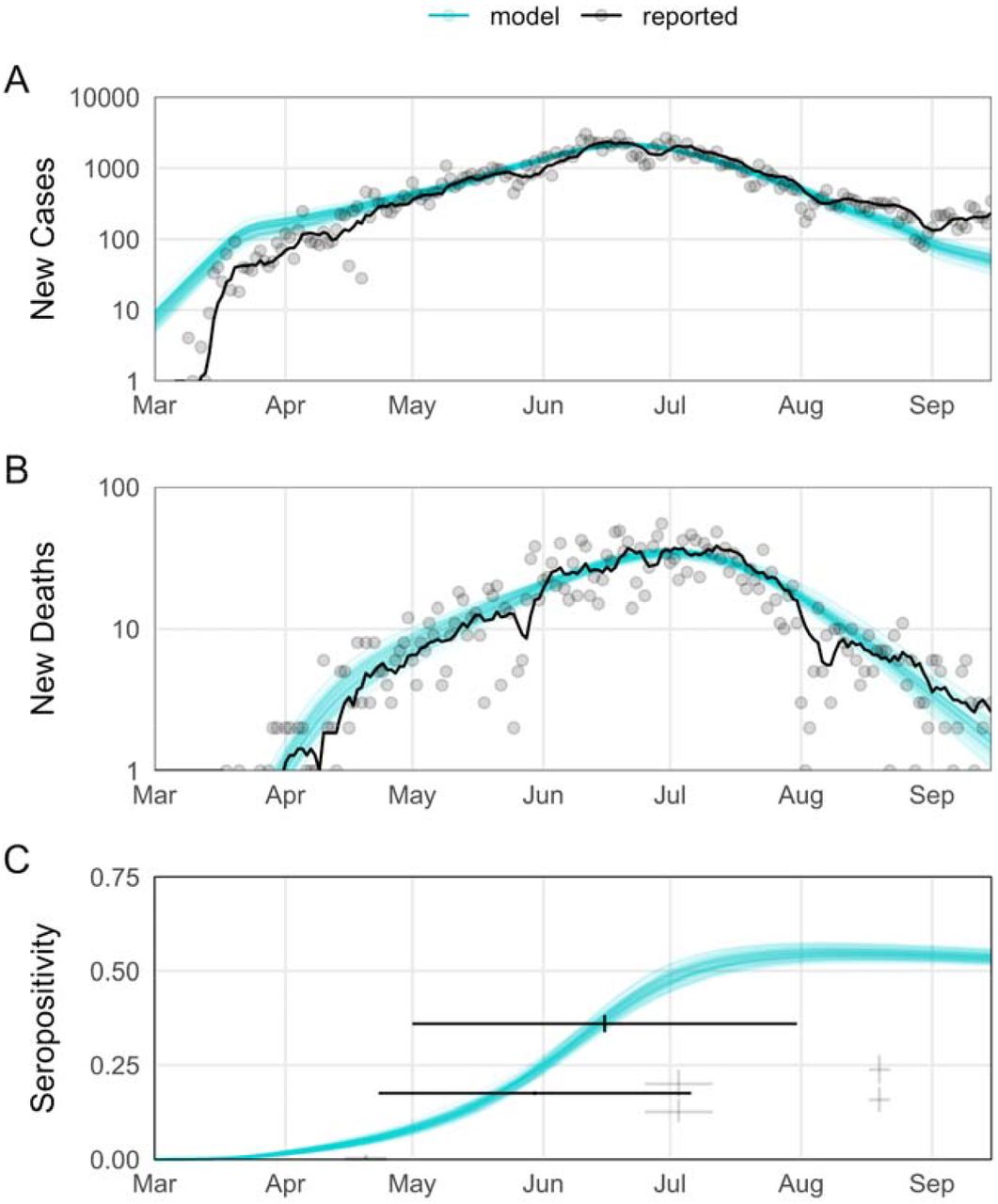
Sample ascertained trajectories (n=250) from the posterior of model parameters (blue) compared to observed outcomes (black). For observed cases and deaths, the solid line is the seven-day average, with points corresponding to daily reports. For the limited serological data, the crosshairs show the collection period and binomial confidence interval on the seropositivity estimates. The serial study results with expected low seropositivity are faded. Expected duration of infection-derived immunity assumed to be 2.5 years; other immunity assumptions in SI Figure S3. All of the assumptions considered produce comparable fits to reported cases and deaths through September 2020.

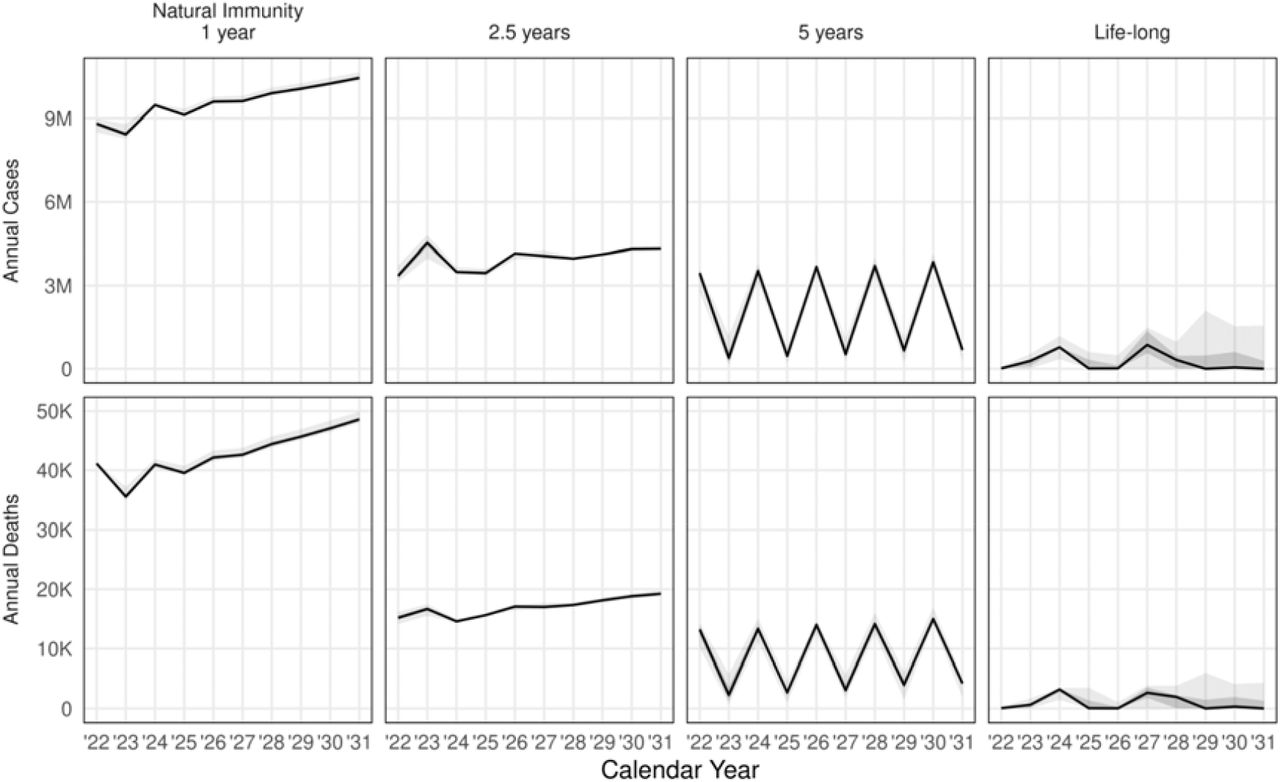
Black line shows median simulation, and grey windows mark 50 and 95% simulation intervals.
As a validation, we compared model outputs to three reports of SARS-CoV-2 seroprevalence (Figure 1C), all from Karachi (22–24). Two concerned broad population samples over an extended period (23,24): these generally overlap with model estimates, but are aggregated over time making precise comparison difficult. The third conducted repeat surveys in two specific regions (22), finding clear qualitative trends which match model trends - limited exposure pre-May, rapid rise through July and subsequent plateau - but recorded lower levels. Additional figures in that study, however, indicate that the specific study sites recorded lower positivity trends generally than their broader districts, and particularly during the case surge in June, suggesting the measured values may be lower than those in the broader population. As another out-of-sample validation, we also compared forward projections to Sindh data for 15 September 2020 to 15 January 2021.
Since the waning rate of infection-acquired immunity is unknown and the benefits of vaccination highly sensitive to this parameter, we repeated the fitting exercise with four assumptions for waning of infection-acquired immunity: life-long, and exponentially waning immunity with expected durations of 1, 2.5, and 5 years.
Vaccine programme
We assumed vaccination distribution consistent with the availability of doses indicated by WHO SAGE’s Working Group on COVID-19 Vaccines (25). We assumed that vaccination required two doses per course, since this is true of most vaccines in the COVAX portfolio.
The number of full courses available each month was assumed to be divided among all COVAX participating countries proportional to population, and likewise for subnational regions. Additionally, we assumed 15% of courses would be wasted for reasons such as cold chain failures, incorrect use, or failure to complete second doses (which we pessimistically assume means lack of vaccine protection). Hence we assumed that Sindh would complete 4000 courses/day in the first three months (with a 30 day delay accounting for timing of second dose) after a vaccine is approved. We assumed courses delivered would increase to 16000, 24000 then 32000 in subsequent quarters using the schedule suggested by WHO SAGE (25) modified to reflect the current vaccine landscape (See SI Section 5). For sensitivity analyses, we also consider a) a constant 4000 courses per day and b) a sufficient constant rate to cover the eligible population in 6 months, 184k courses per day, which is comparable to peak rates achieved in highly developed settings (around 0.4% of the population per day).
For primary vaccine scenarios, we assumed the vaccine is infection-blocking and that protection is complete for some individuals and absent in others (i.e. “all-or-nothing” protection); we considered other vaccine models (every exposure tests the efficacy independently, i.e. “leaky” protection, and/or disease-only blocking) as sensitivity studies. Vaccine doses are distributed amongst individuals in the Susceptible and Recovered compartments; Susceptible individuals become Vaccinated, and Recovered individuals become Recovered and vaccinated.
We considered different durations of protection: once vaccinated in the model, individuals lose vaccine protection with an exponentially distributed duration. Finally, we considered different efficacy levels of protection. A wide variety of COVID-19 vaccines are available to Pakistan via COVAX, which have reported different efficacy levels (26). Instead of modelling a particular vaccine, for our base case scenario, we assume a vaccine with 70% efficacy that protects for 2.5 years on average. As alternatives, we considered a higher efficacy (90%) or longer duration of protection (5 years). See SI for more combinations.
We track vaccine impact for 10 years, and assume that vaccination continues at the same rate (after initial scale up) for 1 (base case), 5 or 10 years, or for 0.5 year for the sensitivity study of high delivery rate. For simplicity, during the time the vaccine programme is active, vaccination occurs on each day of the week, rather than excluding weekends and holidays. We assume that vaccination cost does not fundamentally change as the programme continues and coverage increases; this implicitly assumes a linear average in the costs of vaccination across groups and time.
Given the emphasis on prioritising older adults in WHO’s vaccine prioritisation roadmap (27), we considered two scenarios for distribution: either individuals 15+ years old for the duration or individuals 65+ years old for the first two quarters of the first year before shifting to 15+. For all scenarios, we assume vaccine doses are uniformly (i.e., proportional to fraction of population) distributed in the targeted populations.
Health and economic outcomes
We modelled the impact of COVID-19 vaccination on cases, deaths and Disability Adjusted Life Years (DALYs) compared to counterfactual scenarios with no vaccination over a 10 year time-horizon. For different vaccination scenarios the averted DALYs were combined with the costs of the vaccination programme and any reduction in COVID-19 case management costs from vaccination to calculate incremental cost-effectiveness ratios (ICERs). Our analysis followed the Consolidated Health Economic Evaluation Reporting Standards (CHEERS; for checklist see SI section 10) and base case model parameters are listed in Table 1.
DALYs
For each scenario we modelled the health burden in Disability Adjusted Life Years (DALYs) for symptomatic cases, non-fatal hospitalisations, non-fatal admissions to critical care, and premature death due to COVID-19. For the non-fatal outcomes, and in the absence of specific DALY data, we used Quality Adjusted Life Years (QALYs) reported by Sandmann et al. (28) based on pandemic influenza studies treated one QALY gained as equivalent to one DALY averted.
For COVID-19 deaths we estimated DALYs, guided by the approach presented by Briggs et al. (29). We generated age at death in 5-year age-bands, and then applied age-specific life-expectancy at death using national life-tables for Pakistan (United Nations estimates for 2015-2020 (30)). We adjusted Years of Life Lost (YLLs) considering the overall level of disability for any remaining years of life using data on QoL by age-band from Zimbabwe (31) since all other countries with available data were high-income. However, in our base case analysis, we did not adjust standard life-tables to take into account any reduced life-expectancy due to specific comorbidities associated with COVID-19. As a sensitivity analysis, since risk of severe COVID-19 is higher for people with comorbidities (32), we modelled an alternative scenario in which half of COVID-19 related deaths were assumed to occur in individuals with higher baseline mortality (Standardised Mortality Ratio = 1.5) and 10% lower baseline QoL. We calculated the average DALYs per death using both 3% (base case) and 0% discounting (SI Table S7).
Costs
We estimated annual economic costs of vaccine introduction and of diagnosis and treatment in 2020 values, using an exchange rate of 155 PKR for one USD on 1 January 2020 (33) and adjusting earlier data by the Gross Domestic Product (GDP) deflator for Pakistan (34). Following WHO guidelines, we used a 3% discount rate for future costs and for annualising capital investments, while health outcomes are discounted at either 0% (base case) or 3% (35). The costing was carried out from a health system (vaccination, testing and care and treatment costs) and partial societal perspective (including household costs incurred by COVID-19 illness and case management or costs of illness, but excluding benefits of reduced non-pharmaceutical interventions (NPIs)), using a bottom-up ingredients-based approach.
Costs of COVID-19 vaccine introduction
It was assumed that all vaccine doses would be delivered through campaigns in the community. Vaccine and immunisation costs, including supplies costs per dose with freight charges and wastage are in Table 1. Full costing details are given in SI section 6.
The price of the COVID-19 vaccine itself was set at USD 3 per dose, at which the Serum Institute of India has capped prices for low- and middle-income countries (36). The cost per dose of expanding national and provincial level cold chain equipment was obtained from a model of the costs of delivering COVID-19 vaccines in the 92 COVAX countries developed by UNICEF (37). The additional cold chain costs at the facility level were calculated by allocating a proportion of existing equipment and electricity costs to the COVID-19 vaccine relative to the volume of other vaccines in the immunisation programme.
We estimated vaccine delivery costs via a state-wide campaign by adding together the costs of human resources, social mobilization, and transport. We assumed nurses and vaccinators would deliver the vaccines. We carried out a microcosting of human resource costs using data from the Disease Control Priorities project (38,39). Social mobilisation costs were obtained from budgets from a poliovirus campaign (40). Transportation costs of delivering vaccines to the distribution sites were obtained from the UNICEF model (39). Transportation costs associated with campaigns originating at facilities were calculated by estimating the catchment areas for facilities and assuming daily vehicle journeys corresponding to the radius of the catchment area.
Our delivery costs did not include additional health system activities, such as planning and coordination, pharmacovigilance and waste management. Accordingly, we added a 31% mark-up on the delivery costs, obtained from the UNICEF model (37).
Costs of COVID-19 diagnosis and treatment
The economic impact of COVID-19 on the health system includes diagnosis and clinical management. Costing methods and estimates are reported in full elsewhere (17,43). Briefly, unit costs of outputs, such as bed-days or outpatient visits, were sourced from a range of primary published and unpublished sources in Pakistan. These estimates represent the economic cost of all resources required to deliver health services, including staff time, capital and equipment, drugs, supplies and overhead costs. Quantities of resources used were defined following WHO guidelines and refined based on expert advice to identify less-resource intensive activities in the area of case management that were more feasible in low- and middle-income settings. More information on unit costs calculations can be found in SI sections 6-7.
Household costs of COVID-19 diagnosis and treatment include out-of-pocket expenses for care seeking, funeral expenses and productivity losses due to lost income from isolation of cases, and were sourced from previously published work (17).
Outcome Evaluation
For our scenarios, we simulate 100 matched replicates sampling from the epidemiological parameter distribution developed by the fitting process. We calculate the resulting epidemiological and economic outcomes (e.g., cumulative DALYs averted, costs and ICERs at annual increments after start of vaccination) for each intervention scenario matched to the corresponding non-intervention scenario (i.e., by draw from the parameter distribution). We then take the relevant quantiles of these simulation outcomes across the samples.
Results
Fit to data and epidemic projections without vaccination
Our transmission model is able to fit reported COVID-19 cases and deaths in Sindh for April to September 2020 for different infection-induced immunity assumptions; each gives comparable quality fits (deviance information criterion (DIC) values: no waning protection, 2771; expected protection 5 years, 2772; 2.5 years, 2778; 1 year, 2766). The model also produces seropositivity comparable to three serosurveys in Karachi. At the end of the fitting period, we estimate 48.1K deaths (95% CrI: 45.3-49.7K) and 10.5M cases (95% CrI: 9.9-10.9M), with ascertainment of 5.3% (95% CrI: 4.8-5.8%) of deaths and 1.4% (95% CrI: 1.2-2.0%) of cases. Figure 1 shows our baseline assumption of 2.5 years for infection-derived immunity. When the best fitting parameters are used to project cases and deaths beyond September 2020, however, only the shorter durations of protection appear to give a reasonable fit (SI Figure 3).
In forward projections of epidemics between 2022-2030 in the absence of vaccination, we found that the duration of immunity following infection is the major determinant of the size of epidemics, as measured by annual incidence (Figure 2). If immunity largely wanes within a year, the region will rapidly settle into recurring epidemics of comparable scale to the 2020 waves. For longer durations of protection, there will tend to be some inter-annual oscillation. Life-long immunity results in transmission only at very low residual levels, though we do not consider external re-introductions. This is consistent with epidemic theory, where low immunity duration leads to a rapidly stabilizing endemic disease burden while intermediate durations lead to a series of shrinking epidemic waves settling eventually to lower endemic transmission.
Impact of vaccination on projected cases and deaths
In our base case scenario vaccination averts 0.93 (95% Crl: 0.91, 1.0) million cases, 7.3 (95% CrI: 7.2, 7.4) thousand deaths over 10 years (Table 2.) We found that the annual cases averted by vaccination are higher for longer duration of vaccine-induced immunity, in scenarios targeting people aged over 15 or over 65 for vaccination (Figure 3). For 70% efficacious vaccines that generated 1, 2.5, and 5 years of protection the median cumulative cases averted was negative in 2022, and for vaccines of 1 and 2.5 years protection, also negative in 2023. Only duration of immunity of 1 and 2.5 years showed negative deaths averted in 2022 when targeting 15+, and duration of 1 year when targeting 65+.

For a vaccine efficacy of 70%, delivered in a 2 dose schedule over a 1 year vaccine campaign, and expected duration of infection-derived immunity assumed to be 2.5 years, the median averted disease (lines; darker ribbon 50% IQR, lighter ribbon 95% IQR) with varying vaccine protection duration (from dark to light, increasing vaccine protection duration) and initial target age group (either 15+ or 65+; after the first quarter of vaccination, 15+ is targeted in both cases); other scenarios and health outcomes in in SI Figures S4-S5.
The base case vaccination scenario assumes: a 1 year campaign using a 2-dose vaccine regimen with 70% efficacy at a price of $3 per dose; 2.5 year duration of natural and vaccine induced immunity; and costing from a health-care perspective. dom=dominant (less costly & more effective); DALY=Disability Adjusted Life Year; USD=United States Dollars
These temporary negative years are an outcome of delaying a wave of infections (without replacing lost immunity ongoing vaccination beyond the initial year in the base scenario), leading to offset epidemic years which ultimately has some net reduction in cases and deaths, but in the short term experiences an epidemic when with no intervention the infection-induced immunity would be preventing that epidemic. In general, a vaccine with low duration of immunity delayed and slowed the oscillation of epidemics, but does not substantially reduce total burden because rapid waning leads to relatively low effective coverage.
Economic outcomes of vaccination strategies
The cost of delivery per dose was estimated to be $1.01, excluding vaccine price, wastage and freight charges. Based on a vaccine price of $3 per dose the total undiscounted cost of the vaccination programme was estimated to be $64.1 million, $496 million and $1.04 billion for a 1-year, 5-year and 10-year campaign respectively.
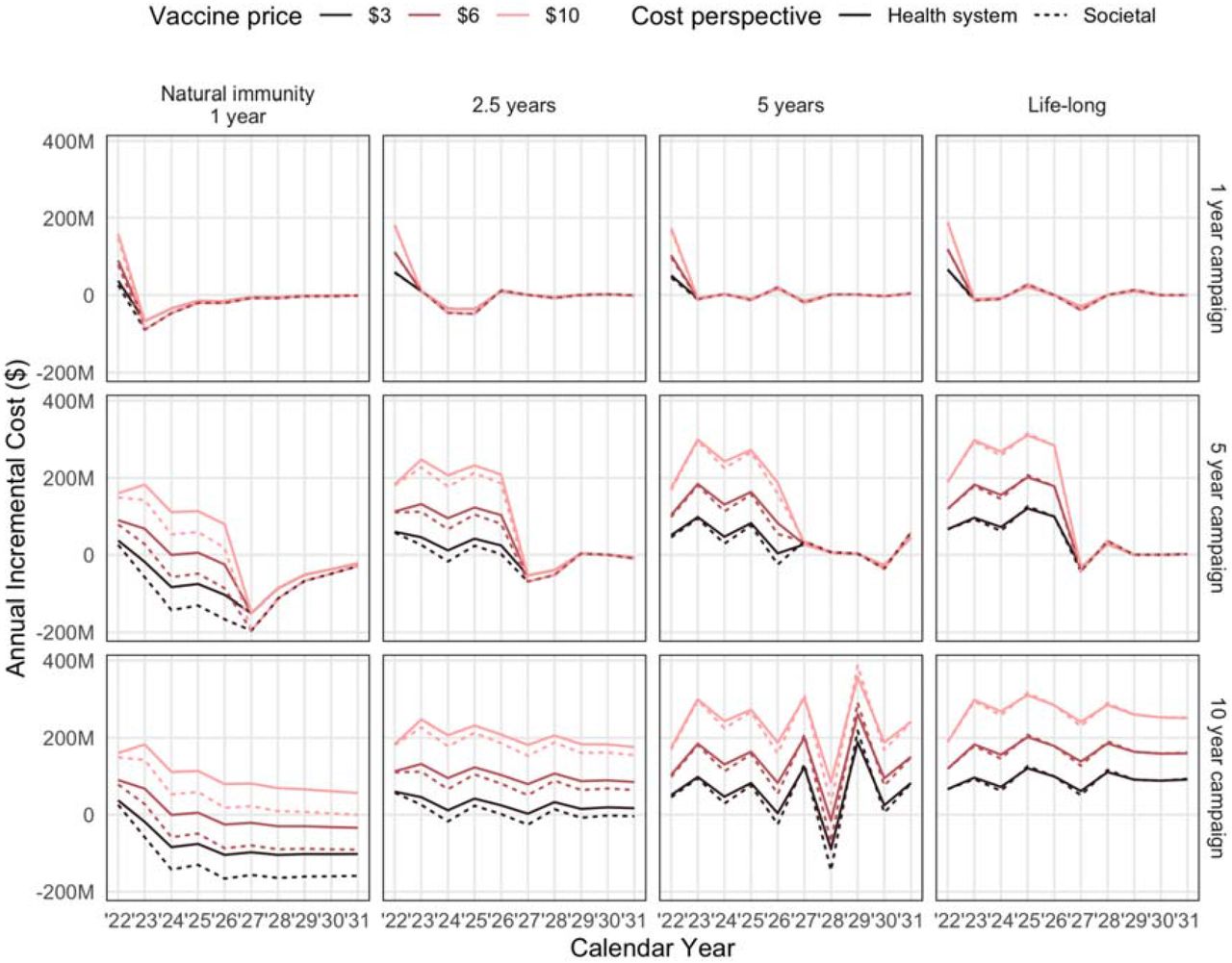
The incremental cost, taking into account cost savings from reduced COVID-19 burden, was influenced by the duration of infection-induced immunity (Figure 4). When this duration was short (1-2.5 years), then annual incremental costs are likely to be cost-saving in the long run. For longer durations of infection-induced immunity, the duration of the campaign affected the annual incremental costs, with the potential for negative costs at the cessation of 5-year campaigns from a health sector perspective. If the infection-induced immunity is life-long, then the extra protection from the vaccine is of limited benefit. The cumulative number of DALYs averted over the entire 10 year time horizon is positive for all vaccine strategies, although it is especially high for a short duration of natural immunity and long vaccine campaign (Figure 5).

Results are shown for vaccination using a 2-dose vaccine regimen with 70% efficacy and 2.5 year duration. The societal perspective includes household out-of-pocket payments and lost income, but excludes wider economic impacts of the pandemic. Red lines show different vaccine prices, and the solid and dashed lines show health system costs and with societal costs respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
For vaccination using a 2-dose vaccine regimen with 70% efficacy and 2.5 year duration.
Cost-effectiveness of vaccination scenarios
Over 10 years our base case vaccination scenario averts 70.1 (95% CrI: 69.9, 70.6) thousand DALYs, at an additional cost of 2.0 (95% CrI: 0.1, 2.9) million USD after deducting the cost of the vaccination programme (Table 2). These results are relatively stable when vaccination is not age-targeted (i.e. the entire population 15 years and older are given vaccination from the outset), DALYs are discounted at 0%, or COVID-19 patients are assumed to have a higher rate of comorbidities.
A one dose regimen (assuming no loss in efficacy) with twice the rate of people vaccinated results in greater health gains averting 105.8 thousand DALYs, and is cost saving.. Extending the length of the vaccination campaign to 5 or 10 years also substantially increases health benefits, but also leads to higher costs yielding ICERs of USD 248.1 and USD 482.1 respectively.
Increasing the vaccine price to $10 per dose would dramatically increase the net costs leading to an ICER of USD 1782 per DALY averted. On the other hand, a vaccine with higher efficacy, longer duration of vaccine protection, or using a societal perspective would make vaccination cost saving.
Discussion
Under a variety of practically relevant epidemiological and economic assumptions, this model of COVID-19 projects that a vaccine programme consistent with the rollout speed projected by COVAX can avert millions of cases and tens of thousands of deaths, and do so in a cost-effective or even cost-saving manner. The particular context considered, Sindh, is a setting with a young population, high SARS-CoV-2 transmission in the past and limited resources. Many lower-and middle-income settings have similar age distributions and contact patterns, pandemic history, costs, and income levels. As such, we expect these qualitative conclusions to apply broadly, though with detailed quantitative outcomes depending on the location-specific values for those parameters.
Reiterating our base case scenario, results: assuming that SARS-CoV-2 does not produce life-long infection-induced immunity, reaching the COVAX-proposed level of coverage (20%) of an efficacious vaccine (70% efficacy for 2.5 years) within a year (and then ceasing vaccination) may avert 900,000 cases and 10000 deaths.
Under our base case assumptions, a single year of vaccination would cost an additional USD 2 million compared to no vaccination, and would avoid 70,000 DALYs resulting in an ICER of USD 28 per DALY averted. This assumes that vaccination can be delivered at USD 1 a dose, in line with incremental economic cost estimates from the EPIC vaccine delivery costs catalogue, which range between USD 0.48-1.38 for new vaccines (44). A vaccination campaign extended to 5 years or 10 years would avert substantially more DALYs, but with higher incremental costs, resulting in ICERs of USD 248 and USD 482 per DALY averted respectively. Pakistan does not have a fixed cost-effectiveness threshold. However, a recently conducted exercise defining Pakistan’s Essential Package of Health Services found that over half of the interventions included had an ICER higher than USD 500 per DALY averted (38,39).
This model also indicates that these benefits are not particularly dependent on the target population. We found that initially prioritizing 65+ year olds would avert 60% more COVID-19 deaths compared to vaccinating everyone 15+ years, although the two strategies had similar cost-effectiveness since the broader strategy would prevent more cases and more deaths in younger individuals. This differs from other model-based analyses set in high-income countries (11–13,28), which find targeting older adults initially would be much more cost-effective. Potential reasons for these differences include the younger age structure of Sindh compared to high-income countries, and the inferred seroprevalence which was greater than 50% by September 2020. Initial epidemic waves in Sindh (and other settings) may have raised population-level immunity to a point where transmission-reducing vaccination in high transmission subgroups (i.e. younger, working age) can indirectly protect subgroups at high risk of severe disease (i.e. older, comorbid). While the quantitative benefits decline if the vaccine only provides protection against disease, the conclusions about comparable benefits for either age prioritization scheme hold.
However, vaccination would be substantially less cost-effective, and potentially not cost-effective from a purely health-care payer perspective, if the vaccine could only be procured and delivered at USD 10 a dose or had efficacy as low as 30%. Also, even if a large-scale multi-year mass-vaccination programme is cost-effective, it may none-the-less drain scarce financial and human resources from other essential health services. In addition, there are many non-financial constraints (e.g. trained personnel), meaning that health opportunity cost may be higher without careful delivery planning. Decisions about vaccination should also take account of other factors besides cost-effectiveness, such as the disproportionately high burden of COVID-19 and related interventions on socio-economically marginalised groups, and the urgent need to return the economy and society to normal. To effectively inform policy decisions, analyses such as this should be combined with analyses of macro-economic impact and data on broader societal impacts in a transparent decision framework (e.g. health technology assessment).
In general, our epidemiological projections have relatively narrow uncertainty intervals. While there remains substantial uncertainty on a daily basis, this tends to be off-setting: cases may shift a little in time, but an annual aggregation results in fairly narrow estimates. These relatively small intervals propagate through the rest of the analysis. These narrow intervals are an accurate reflection of the model assumptions, but the model is fixing many aspects of the real world that are likely to shift unpredictably over the next several years.
As demonstrated by recent emergence of novel variants, the underlying epidemiology may shift, as will technological and social trends, including the relative prices of the inputs to the economic estimation. Variants able to escape vaccine-induced immunity may be introduced either through importation or local mutation. This process is partially addressed by considering loss of infection- and vaccine-derived immunity. For the fastest immunity loss we considered, expected protection durations of a year, a consistently efficacious vaccine (as might be produced by annual updates) can still be cost saving. If variant emergence was more rapid, revaccination with updated formulations might not be able to keep pace, corresponding to lower efficacy. Lower efficacy vaccine (30%) scenarios for rapid protection loss generally resulted in much worse costs per DALY averted (order 1000s of USD per DALY).
We also assumed that within a particular age group, there is no association between probability of getting vaccinated and risk of disease. This may not be accurate if for example vaccination targets people with comorbidities (and hence higher risk of severe COVID-19 disease), or people who are risk averse (and hence less likely to be infected) are also more likely to get vaccinated. We do not consider future non-pharmaceutical interventions beyond May 2021 or innovative coordination with vaccination. If there are substantial changes from the impacts integrated into the fitted estimates of local transmission, our projections will not reflect those.
Given these core limitations and uncertainties, the intervals ought to be thought of as about our estimate of the central trend conditional on the scenarios, rather than as reflecting the total volatility in the system.
We used a range of scenarios for the duration of natural immunity, although the shortest duration (1 year) best fitted case and death data. This is because the apparent loss of natural immunity may be driven by other factors we did not consider such as behaviour change or emergence of escape variants. If natural immunity is indeed short-lived, this will further strengthen the conclusion that vaccination is likely to be cost saving.
Our findings provide an example of the type of analysis that low- and middle-income countries can employ to inform vaccination strategies in terms of target populations and financing requirements. While the economic and societal impact of COVID-19 is substantial, the real resource constraints within the health sector in many low- and middle-income countries mean that vaccination strategies need to balance the current emergency and the longer term needs of the health sector. The slow rate of vaccine distribution is the major impediment to larger health impact. Administering vaccine doses in line with projected COVAX availability in a province of roughly 50 million people, it would take around 3 years to reach 60% population coverage. Such a long-term programme may not be feasible if vaccine delivery disrupts delivery of other health services, which is a possibility given that the vaccine is targeted at an age group outside the usual Expanded Program on Immunization (EPI). Hence both short-term rapid response and longer-term consideration about how COVID-19 vaccination can be incorporated in the broader package of essential health services are important in Pakistan and beyond.
Declaration of Interests
The authors have no interests to declare.
Data Sharing
Model code is available at: https://github.com/cmmid/vaxco
Data from Sindh province is publicly available data but is included in the repository.
Ethics
All clinical data used were obtained from publicly available sources, so no ethical approval was required for this study.
Acknowledgements
We thank Ulla Griffiths (UNICEF) for information on the cost of COVID-19 vaccine delivery.
Footnotes
CMMID COVID-19 Working Group: Mihaly Koltai, Fiona Yueqian Sun, W John Edmunds, Sophie R Meakin, Samuel Clifford, Kevin van Zandvoort, Yang Liu, Yalda Jafari, Timothy W Russell, Sam Abbott, Graham Medley, Alicia Showering, Katherine E. Atkins, Yung-Wai Desmond Chan, Emily S Nightingale, Anna M Foss, Kiesha Prem, Rachel Lowe, Damien C Tully, Oliver Brady, Rosanna C Barnard, Amy Gimma, Christopher I Jarvis, William Waites, Hamish P Gibbs, Frank G Sandmann, Stefan Flasche, Thibaut Jombart, Joel Hellewell, Jack Williams, Gwenan M Knight, C Julian Villabona-Arenas, Matthew Quaife, Fabienne Krauer, Billy J Quilty, Petra Klepac, Naomi R Waterlow, Sebastian Funk, Akira Endo, Jiayao Lei, Kaja Abbas, Adam J Kucharski, Kathleen O’Reilly, James D Munday, Nikos I Bosse, Alicia Rosello.
Manuscript revisions submitted based on reviewer feedback.
References



