
ABSTRACT
Introduction During the COVID-19 pandemic, there have been drastic changes in family life and programs and services that promote and protect early childhood development. Global stakeholders have raised concerns that the pandemic is putting enormous strain on parents and other caregivers, compromising capabilities and enabling environments for nurturing care of young children and therefore likely impacting children’s development.
Methodology This rapid review takes stock of emerging research on nurturing care for young children during the COVID-19 crisis. Two databases were searched in addition to an extensive search for grey literature, drawing on 112 scholarly and scientific studies from more than 30 countries that have examined components of nurturing care during the pandemic, namely: responsive caregiving, early learning and play, and children’s safety and security.
Results There are some reports of unexpected positive benefits of the pandemic on families, including increased father involvement in caregiving. But more commonly, the studies’ findings reveal numerous issues of concern, including parental and caregiver mental health difficulties and less responsive parent-child relationships, increased screen time among children, limited opportunities for outdoor play, and fractured systems for responding to potential child neglect and maltreatment. Evidence suggests limited access and challenges in the provision of remote learning for the youngest learners, such as those in early childhood education.
Conclusion The findings can inform global stakeholders, who have advocated for increased support and funding to ensure young children and other caregivers are supported and protected during the COVID-19 pandemic. There is an urgent need for action-oriented implementation studies – those that go beyond identifying trends and begin to pinpoint “what works” to effectively promote and protect nurturing care during emergencies such as the COVID-19 pandemic.
What is already known?The most fundamental promotive experiences in the early years of life to reach optimal development come from nurturing care and protection received from parents, family, and community, which have lifelong benefits including improved health and wellbeing. Health and other emergencies are detrimental to the provision of nurturing care.
What are the new findings?Findings from this rapid review reveal numerous areas of concern, including families reporting mental health difficulties and less responsive parent-child relationships, increased screen time among children, limited opportunities for outdoor play, and fractured systems for responding to potential child neglect and maltreatment. As with other features of this pandemic, not all families are affected equally: financially vulnerable families are much more likely to experience negative ramifications. The pandemic is also disproportionately affecting parents and other caregivers with young children, particularly mothers, those with pre-existing mental health difficulties, and those caring for children with disabilities.
What do the new findings imply?Findings highlight the need for action by governments, civil society, international and community-based organizations to improve support for families so that the pandemic does not break the provision of nurturing care and wipe out decades of progress, especially for vulnerable families and children.
INTRODUCTION
During the COVID-19 pandemic, there have been drastic changes in family life on every continent. There have been prolonged containment measures in many countries, with second waves and renewed lockdowns. Families are “locked in” together, without access to their usual forms of social support and with disruptions to services and programmes that protect and promote early childhood development (i.e., childcare, early childhood education, parenting programmes, health services). Global stakeholders have raised concerns that essential components of ‘nurturing care’ for early childhood development have been harmed during the pandemic [1, 2]. The World Health Organization (WHO), UNICEF, and World Bank Group advocate that young children require five inter-related components of nurturing care for optimal development and well-being: good health, adequate nutrition, a family environment rich in responsive caregiving, opportunities for formal and informal early learning, and protection from safety risks and maltreatment [3]. During the first years of life, parents, intimate family members and caregivers are the closest to the young child and thus the best providers of nurturing care. This is why secure family environments are important for young children. In order to provide caregivers with time and resources to provide nurturing care, multisectoral policies, services and community supports need to be in place. Health, nutrition, education, social welfare, and child protection all have a role to play in creating an enabling environment for nurturing care (for further details, see https://nurturing-care.org).
Evidence shows that epidemics and pandemics are associated with disruptions to nurturing care and child development, stemming from increased caregiver social isolation and stress [4], disruption to family routines [5], traumatic stress among caregivers [6], household conflict and anxiety [7], early termination of breastfeeding [8], and reduced play among children and engagement in team-based sports [9]. This rapid review aimed to capture the emerging evidence on the effects of the COVID-19 pandemic on three components of nurturing care: responsive caregiving, early learning opportunities, and child safety and protection from violence and neglect. This is a broad inquiry that is explored through different outcomes that are critical for nurturing care and child development. For responsive caregiving, it includes good mental health of parents and caregivers, warm and responsive parent-child relationships, breastfeeding support (to promote emotional bonds and attachment), and fathers’ engagement in caregiving. For early learning, it includes access to formal and home-based learning, parent–child reading and other early learning activities, and safe play spaces. For children’s safety and security, it includes protecting children against injury, neglect and abuse, including child protection and referral services for suspected maltreatment. This review did not examine child health and nutrition, the other components of nurturing care, due to ongoing work and recently published reviews in these areas. The review findings can help identify and conceptualize priority issues for early years’ policy and programming during emergencies such as the COVID-19 pandemic and identify the literature gaps where future studies are required.
METHODS
To generate evidence in a short time, we employed abbreviated systematic review methods. A single reviewer completed the study selection and data extraction with verification by a second reviewer, and we omitted quality assessments of the included studies. The population of interest is young children (birth to 8 years old) and their caregivers, including birth parents, adoptive parents, and formal caregivers. Studies involving children up to 18 years old and their caregivers are included as long as the studies also included results for children under 8 years old. Published quantitative or qualitative studies that document their full methodology are included, and preprints and the grey literature to ensure representativeness and due to the rapidly evolving nature of COVID-19 pandemic impact evidence.
We focused on studies that reported on responsive caregiving during the COVID-19 pandemic (e.g., parental mental health, caregiver stress, parent–child interactions, family functioning, fathers’ engagement in caregiving, gender roles and norms, breastfeeding, skin-to-skin contact, social support). We also included studies that reported on opportunities for early learning during the pandemic (e.g., access to formal and home-based learning, parent–child reading and other early learning activities, outdoor play, physical activity, screen time, sedentary behaviour). Lastly, we included studies that reported on children’s safety and security during the pandemic (e.g., child injuries, child maltreatment referrals, child physical or psychological abuse, family violence). We searched two databases (PubMed and ERIC) based on a search strategy developed and pilot-tested in collaboration with a librarian. Also, for the grey literature, the review team manually searched the websites of more than 80 multilateral and bilateral organizations, internal NGOs, foundations, and so forth. Lastly, we screened the reference lists of the included studies for further relevant citations. We restricted the search to papers available in English, French, Spanish, and Portuguese. Studies were published between 1 January 2020 and 25 October 2020.
Identified records were exported and managed on Zotero. After removing duplicates, the titles and abstracts of the remaining records were screened against the eligibility criteria, followed by full-text screening. We extracted data from the studies using a standardized form, with a second reviewer assessing for completeness and accuracy. Data extracted included, but was not limited to, investigators/authors, year of publication, setting, context, details of the methods and data collection, participants, outcomes, results, and conclusions. Data extraction was guided by Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) checklist items. The preliminary stages of the synthesis involved organizing the extracted data through itemizing the data into thematic areas and tabulating the results to systematically identify patterns within and between studies and variations across studies. Because of the heterogeneity of the available primary studies, we synthesized the results narratively in the report.
RESULTS
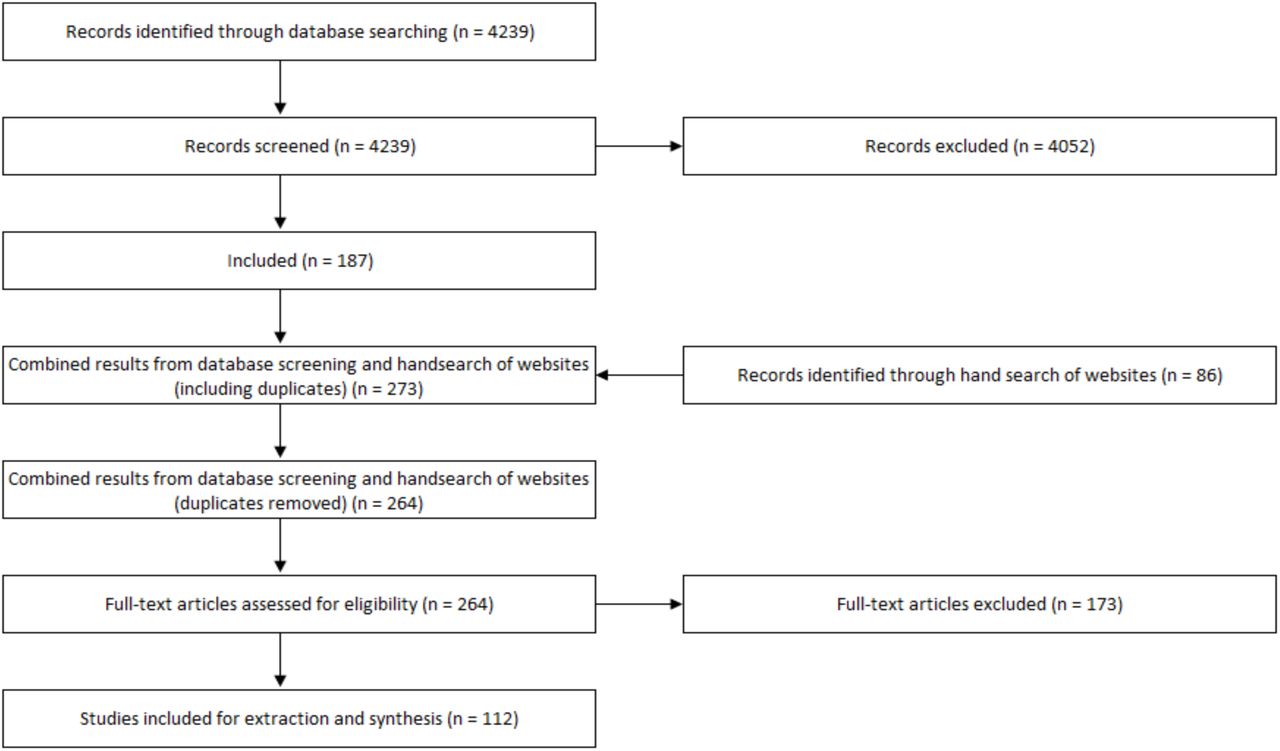
After excluding duplicates, the initial search yielded 4210 papers from the database search and 86 publications through the organizational website search. After the title, abstract and full-text review, 112 publications were included in the review. The PRISMA flow diagram in Figure 1 provides an overview of the study selection process.

PRISMA diagram
While most studies (89) in the review focus on high-income countries, there is increasing geographic diversity from low- and middle-income countries (23). In terms of the thematic areas, the largest number of papers focused predominantly on issues related to ‘responsive caregiving’ (59), which points towards increased parent and other caregiver stress, burnout, depression and anxiety during the COVID-19 pandemic, and harsher parenting and less warm or responsive parenting. Evidence suggests increased fathers’ engagement during the COVID-19 pandemic. On the other hand, evidence indicates that COVID-19 restrictions have hampered access to traditional lactation support services. The next largest number of studies examined issues related to ‘safety and security’ (35), which point towards drop in child abuse and neglect referrals to child protection services, and a reduction in emergency department visits for child injuries. Lastly, a relatively small number of studies addressed opportunities for early learning and play during the COVID-19 pandemic (18). These studies point towards increased screen time among children, and a reduction in outdoor play and physical activities. Evidence is limited on home-based learning for young children (age 3-5 years) during the COVID-19 pandemic. What is available suggests challenges, frustrations and inequitable access to distance learning for the youngest learners. Results include 95 quantitative studies (primarily cross-sectional due to the nature of the pandemic), nine qualitative studies, and eight mixed methods designs. Key findings of included studies are synthesized in the following sections, and a summary of each study can be found in the complementary table.

{kind=link}
{kind=link}
Key review findings on nurturing care during the COVID-19 pandemic.
Parent and caregiver stress, mental health, and responsive caregiving
The review results indicate that parents’ and other caregivers’ mental health has been among the most researched topics related to nurturing care during the pandemic. During the period under review, more than 30 studies across various geographic and demographic contexts examined the implications of the COVID-19 pandemic on parent and caregiver stress, burnout, depression, and anxiety [10–45]. The presented evidence indicates that the pandemic crisis has been detrimental to caregiver stress and mental health, particularly for parents and other caregivers of young children and mothers [14,16,30,31,33], being single [30], economically vulnerable families [14,27,42], and those with pre-existing mental health issues [14, 42]. Parents and other caregivers of children with disabilities also showed a heightened prevalence of depressive symptoms, anxiety, and stress during the pandemic [11,18,43].
While this evidence base is heterogeneous, with variations in the data, context, and methodology, the findings are generally consistent in revealing that the pandemic and its related policy response measures drive increases in caregiver stress and poor mental health. For example, a study of 192 Italian mothers found that 29% of mothers who had given birth during the COVID-19 lockdown had an Edinburgh Postnatal Depression Scale (EPDS) global score above the cut-off score of >12, compared to only 12% in the control group who had given birth during the same period the year before COVID-19 [45]. A study of 651 Finnish parents of children (aged 5 to 8 years old) found that 26% met the clinical EPDS cut-off score for potential depression during the pandemic, compared to 15% among the same sample parents with data collected between 2014 and 2019 [33].
While the literature identified multiple and often overlapping COVID-19-related stressors that adversely affected the mental health of parents and other caregivers of children, economic insecurity stands out as one of the strongest and most consistent sources of parent and caregiver stress [12,24,25,28,42,46–49]. For example, using data from 2,174 Bangladeshi mothers with children aged 0–5 years old, Hamadani et al. [25] found that 96% of respondents experienced a reduction in paid work during a COVID-19 lockdown, with average monthly family income falling from US$212 to US$59, and food insecurity increasing by more than 50%. Self-reported maternal depressive symptoms, as measured by the Centre for Epidemiologic Studies-Depression Scale (CESD-D), significantly increased during the lockdown period compared to before the pandemic; and nearly 70% of the sample reported that their anxiety had risen during the lockdown. A US study of 561 parents and other caregivers of young children (aged 2–7 years old) and who were hourly workers found that the majority of respondents reported a loss of household income (69%) and even job loss (60%), which linked with increased anxiety, depression, anger, and irritability, as well as worse sleep quality [24].
Numerous studies found that parent and caregiver stress, depression, and anxiety during the COVID-19 pandemic was associated with reduced responsive caregiving, including, for example, lower parent–child closeness and more avoidant or harsher parenting attitudes and behaviours [10,13,16,27,28,32,37,38,41,42,48]. A New Zealand study found that parents of young children (aged 4–5 years old) who experienced more significant depressive symptoms and perceived stress during a COVID-19 lockdown reported harsher parenting and less warm/responsive parenting, as measured by the Parenting Styles and Dimensions Questionnaire (PSDQ); and parent–child relationships were also of lower quality [32]. A US study of low-income families with preschool-age children found that parental job loss and income loss during the pandemic were strongly associated with parents’ depressive symptoms, stress, diminished sense of hope, and negative parent–child interactions, including losing their temper or yelling at their child [27]. However, parents who lost their job but did not experience corresponding household income decline, perhaps due to economic stimulus relief for low-income families, were more likely to report enjoying spending time with their child during the COVID-19 pandemic and engaging in positive parent-child interactions, such as playing with or hugging their child, compared to those who experienced a decline in household income. These results suggest that efforts to ensure economic security may help address parents’ and other caregivers’ mental health needs and reduce adverse parenting risk. Studies also noted more couple conflict [50] and increased substance use [51] among parents and caregivers experiencing stress and anxiety during the pandemic.
Few studies to date have discussed potential interventions to support parents and other caregivers with COVID-19-related stress, anxiety, and mental health issues or ways to protect parents’ capacity for responsive caregiving during the crisis. One study found mothers rarely utilized mental health services during the COVID-19 pandemic due to various barriers, such as a lack of time or energy, cost of service, not believing they needed such services, and uncertainty on access [14]. Studies found that partner support and cooperative co-parenting [13,14,20,32] and moderate physical exercise [17, 29] were associated with better mental health and coping among parents and caregivers during the pandemic. Thus pandemic-related strategies for parents and caregivers could focus on supportive parenting interventions and home or internet-based exercise interventions. Lastly, a few studies point towards mixed and potentially positive impacts of the COVID-19 restrictions on deepening family ties, improving couples’ relationships, and developing new family hobbies or activities [13,22,46,52–54]. However, such positive benefits were typically found among the parents and caregivers of older children or adolescents and among families with several protective factors, including financial stability, comfortable and safe homes, enough food to eat, good health, and healthy couple relationships [22, 46].
Breastfeeding support during COVID-19
Breastfeeding not only provides an infant with nutrition, but it is also a process of responsive caregiving in which the mother and her young child interact closely in a safe and secure relationship. Five studies related to breastfeeding support during the pandemic indicate that lockdowns resulted in reduced breastfeeding support and care [55–59]. For example, over a quarter of respondents in a national U.K. study struggled to access breastfeeding support during the pandemic, and some stopped breastfeeding before they intended to [55]. Among the women who stopped breastfeeding during the pandemic, the most common reason was the lack of breastfeeding support and face-to-face help with practical problems, such as latching. Some valued the virtual health appointments among the women who had to shift from face-to-face lactation support to digital consultations. In contrast, others reported feeling violated during this impersonal interaction, describing how they felt discomfort recording their infant trying to latch onto the breast [59]. During the pandemic, some breastfeeding women reported some positive benefits, including having more time to focus on breastfeeding and responsive feeding, with fewer visitors, more, privacy and more significant breastfeeding support from fathers [58].
Fathers’ engagement in childcare and gendered employment patterns
The evidence suggests that increases in fathers’ time at home during COVID-19 have reduced gender gaps in childcare division, which may have promoted positive changes to family dynamics and more similar caregiving arrangements. In total, eight studies reported that fathers took on more childcare responsibilities during the COVID-19 pandemic [60–67]. For example, a survey of 1,536 Australian parents of children (aged 0–16 years old) reported that fathers averaged 2.21 daily hours on active childcare before the pandemic, and this average increased to hours during the pandemic, thereby narrowing the childcare gap between mothers and fathers [62]. However, mothers continued to carry the burden of extra childcare and household responsibilities during the pandemic [68], and gendered employment patterns were exacerbated [60,67,69–71]. In particular, mothers were more likely than fathers to lose their jobs during the crisis, spend less time on paid work, and be interrupted during work hours, principally by childcare [1]. There is an absence of studies examining how parents and other caregivers of young children, including infants and toddlers, negotiate childcare responsibilities and household work during crises. There was also a lack of studies discussing male caregivers’ perspectives and experiences of caregiving during the pandemic and quality of interaction and exploring caregiving responsibilities and arrangements of single parents.
Opportunities for early learning during COVID-19
Evidence on home-based early learning during the COVID-19 pandemic is limited compared to the other thematic areas in the review. What is available indicates that many children in early childhood education did not have contact with teachers or access to remote early learning during school closure [66,72,73]. For example, a study of Ethiopian parents and caregivers of young children found that only 10% of children who enrolled in pre-primary had been in contact with teachers or school principals, with significant differences found by household wealth and across regions [73].In this study, half of parents and caregivers reported supporting educational or learning activities for pre-primary children, including 12% who had used radio lessons while schools were closed. Children living in rural or remote areas had significant disadvantages regarding access to electricity, technologies, and children’s books or learning materials.
Other studies provide evidence of frustration and negative attitudes among caregivers about distance learning benefits and values, especially for preschool-aged children [74–76]. Home-based learning has been challenging for young children for various reasons, including limited learning materials and technological barriers [77, 78]. Children who were looked after by grandparents faced challenges due to their limited awareness about online technologies [77]. Parents noted concerns about lack of social interaction, sedentary behaviour, and limited physical activity during school closures [21,79,80]. A study of parents of children (aged 2-4 years) reported that almost half of the children spent no time playing with another child in their household during lockdowns [21]. Evidence is limited and mixed on the nature and extent of caregiver engagement in adult-child reading, playful parenting, and other early learning activities during the lockdown. Some studies find that parents engaged more in such activities during the lockdown [66, 73] while others reported they engaged less than before the pandemic [72]. Parents who met the criteria for probable major or severe depression and parenting stress were negatively associated with parents’ perceived preparation to educate at home [79].
Children’s play and physical activity during COVID-19
Nine studies reported that COVID-19 restrictions, such as the closure of schools and playgrounds, the cancellation of sports and activity classes, and reduced social interactions with peers, were linked to reduced outdoor play and physical activity and more sedentary behaviour among children [72,81–88]. One study found that nearly 9 out of 10 Canadian parents reported increased screen time since the beginning of the pandemic among young children aged 18 months old to 5 years old [81]. More than half of the parents in this study reported that children’s physical activity decreased during the pandemic, citing challenges due to the lack of indoor space and the variety of available toys. Another study found a dramatic decline in children’s outdoor physical activity and much higher screen time use (average of 5 hrs/day) during the initial period of the COVID-19 outbreak, compared with before the restrictions [83]. Play indoors did not seem to replace active play outdoors, resulting in a net decline in children’s play-based activities. Cities and areas with the highest number of COVID-19 cases, and thus most stringent restrictions, had the most significant drop in children’s outdoor play [84]. Living in houses (as opposed to apartments) was correlated with increased outdoor activities [86].
Child protection from violence and neglect during COVID-19
In terms of children’s safety and security, evidence indicates that COVID-19 has reduced child maltreatment referrals. Thirteen studies across seven countries, mostly utilizing publicly available administrative data, suggest that referrals of potential abuse, neglect, and maltreatment to child protective services were substantially lower during the COVID-19 pandemic than before quarantine measures were put in place [89–101]. Surveys of child protection workers similarly reported decreased referrals and more difficulty identifying children and families in need during lockdown [99,102,103]. For example, a study based on data from January 2015 to May 2020 for New York City’s Administration for Children’s Services reports there were 29% fewer allegations of child maltreatment for March 2020—when school closures first began— compared to previous years [96]. Substantially fewer allegations of child maltreatment were reported by education personnel and other mandated reporters, including childcare personnel and medical health personnel during this time. Non-mandated reporters, including family members and neighbours, also made fewer referrals, which may be linked to social distancing and limited contact between children and those outside their households. Bullinger et al. (2020a, 2020b) found that in Chicago and Georgia in the United States, emergency calls for domestic crimes rose in March and April 2020 but calls for potential child abuse fell, potentially due to the lessened visibility of child victims than adults.
These changes do not reflect an actual reduction in the incidence or prevalence of maltreatment. The decrease in referrals is likely due to the given lockdown measures that preclude children from having regular contact with educators and other mandated reporters. Although many school districts have transitioned to online learning during the COVID-19 pandemic, evidence suggests that educators typically receive inadequate education related to recognizing and responding to child maltreatment. Virtual formats for teaching do not lend themselves readily to the identification of child maltreatment. With reduced exposure to schools and other social services, there is widespread concern that child maltreatment victims are going undetected.
Two studies indicate a striking rise in child abuse-related injuries among babies and toddlers during the pandemic [104, 105]. Comparing cases of children’s head trauma caused by suspected abuse, there were 10 cases at an urban medical facility in the United Kingdom over the March–April 2020 period, representing an increase of 1493% compared to the previous three years preceding the lockdown [105]. Although alarming, it is important to consider that COVID-19 has led to significant healthcare delivery changes, and many centres have diverted non-COVID-related health emergencies to specific healthcare facilities, which may account for the increases in abuse head trauma at particular institutions. One additional study examined the association between COVID-19 and potential child abuse and found that COVID-19 job loss among parents and caregivers was significantly associated with psychological maltreatment, including verbal threats, belittling, and ridiculing, with larger effects for younger children [106]. Given previous evidence detailing the strong links between caregiver stress and the risk of child maltreatment, the economic-related impacts of COVID-19 may contribute to elevated rates of child maltreatment; however, this relationship has not yet been substantiated.
Child injuries during COVID-19
Data on emergency department visits and injuries suggest that children’s environments have shifted during the pandemic and present different child safety threats. Nine studies from eight countries reported a significant reduction in emergency department presentations and operations for injuries among children during government-imposed lockdown restrictions, especially related to admissions and operations for sporting-related injuries and those that occur on playgrounds bans on sports and access to playgrounds [107–115]. For example, a study based on data from a large acute paediatric hospital in London, UK, found that the prevalence of referrals for child injuries was reduced by nearly two-thirds during the lockdown from 17 March to 28 April 2020, compared to in the same period in 2019 [111]. In contrast, some centres found a relative increase in injuries, including bicycle injuries [107, 109], burn injuries [116], ingestions and poisonings [108], and electrical injuries [114]. The higher incidence of child burn injuries during COVID-19 lockdown was equivalent to the percentage of admissions during a typical summer break and suggests that child supervision may be a significant factor during school closures [116]. The general demographic of those presenting with injuries also changed during the pandemic compared to before the pandemic, with a significantly younger median age [111,113,115]. Parents and other caregivers may have treated more minor injuries at home or, in some cases, may have avoided seeking medical attention due to the concern of contracting COVID-19 in hospital facilities. Physical distancing measures, including a ban on sports and children’s use of playgrounds during lockdowns, is likely linked to the overall reduction in child injuries seen through emergency room admissions. At the same time, there may have also been a shift in care-seeking behaviour, with parents and caregivers being more anxious about attending hospital due to the risk to themselves and the child of contracting COVID-19.
DISCUSSION AND CONCLUSION
Emerging evidence from the COVID-19 pandemic, mainly drawn from parents and other caregivers’ surveys, shows striking similarities in how essential components of nurturing care –responsive caregiving, support for young children’s learning, and children’s safety and security-have been disrupted. While there are some reports of unexpected positive benefits of the pandemic on families, such as increased involvement in caregiving among fathers, more commonly, the studies’ findings reveal issues of concern, with parent and caregiver mental health difficulties and strained parent–child relationships, increased screen time among children, limited opportunities for outdoor play, and fractured systems for responding to potential child neglect and maltreatment. As with many other features of this pandemic, not all families are affected equally. Those with salaried jobs are far less likely to experience income loss than those with informal, daily wage jobs. Social safety nets such as stimulus packages for families may reduce parenting stress brought about by COVID-19-related economic hardship and reduce the risk of harsh and non-responsive parenting. The pandemic is disproportionately affecting parents and other caregivers with pre-existing mental health conditions and caregivers of children with disabilities. Families with young children, particularly mothers, may be disproportionately affected by childcare and school closures, the reduced ability to undertake paid work, and increased caregiving demands.
Based on these findings, we suggest policy and programme responses for action by governments, civil society, international and community-based organizations (see Box 1). All of these options should be pursued vigorously and simultaneously so that the pandemic does not break the continuity nor lower the quality of provision of nurturing care and wipe out decades of progress, especially for low-income families and children. These approaches must be coordinated across sectors and aligned with practical social safety support to families and other caregivers of young children who experience socioeconomic hardship.
Key programme and policy implications
Scale-up of social protection mechanisms to ensure families can meet their basic income needs and food and housing security. Governments should reflect on, and rebalance, expenditures going to families and children. Supporting parent and caregiver mental health and minimizing family stress should continue to be a top priority in COVID-19 response plans and prevention-based approaches. There remains a huge unmet need to expand and diversify social protection responses, including the immediate delivery of food packages, longer-term paid parental leave, accessible childcare, universal basic income, and waivers for utility bills and rent or mortgage payments, to avoid further indebtedness or evictions. Families are much less likely to benefit from family and parenting support when their basic needs are not met.
Improve access to and use of mental health and psychosocial support services for parents and other caregivers of young children are essential. Digital interventions for anxiety and depression might include information provision, connectivity and triage, automated and blended therapeutic interventions (such as apps and online programmes), and telephone calls and home visits, especially for those without connectivity. Given the need to disseminate affordable mental health support widely due to COVID-19, group-based telehealth interventions may allow for an increased reach of psychological services in a time of elevated need.
More evidence is needed on scalable responsive caregiving interventions, responsive caregiving, early learning activities and play, appropriate for the conditions of physical distancing and lockdowns. Programs that foster peer support and online platforms should be evaluated to ensure acceptable efficacy in supporting caregivers with young children, particularly on aspects of early learning and play. Guidance and resources to help parents with balancing screen time with physically active, screen-free activities may be warranted.
Child protection systems should be redesigned, and educators trained to identify signs of child abuse and neglect specific to a distance-learning model. Home visitation programmes, with appropriate protection of social service staff, should continue to the extent possible, particularly with high-risk families. To increase awareness and access to reporting hotlines and other maltreatment reporting resources, policy makers may consider a variety of dissemination means, including public signage, as well as broadcast and social media.
A recent report of case studies of programme implementation to support nurturing care during COVID-19 illustrates several innovative examples of how organizations in various contexts have adapted to support nurturing care efforts during COVID-19 [117]. For instance, programmes have organized emergency food delivery services for vulnerable families. Others have developed new training materials for frontline workers that integrate both mental health and nurturing care components. Organizations concerned with children’s health and development in many countries have implemented virtual caregiver support meetings, telephone or internet-guided learning activities for young children, and online stress reduction resources for parents and other caregivers.
The evidence in this rapid review was primarily collected during the pandemic’s first stage of lockdowns, representing only the early phase of the pandemic. Future research must investigate the longer-term impact of the COVID-19 pandemic on families as we enter a period of a gradual relaxation of lockdown measures in some regions and second waves in others. Gaps in the evidence base remain, with a lack of studies in low- and middle-income countries. There is an urgent need for action-oriented implementation studies – those that go beyond identifying trends and begin to pinpoint “what works” to effectively promote and protect nurturing care during health emergencies such as COVID-19. In particular, there is a need to identify effective interventions and strategies for families experiencing income loss, food insecurity, mothers with young children, families with disabled children, and those with pre-existing mental health challenges. Also, further inquiry is needed into the effects of COVID-19 lockdowns on early learning and children’s play, which is transformative for children, allowing them to creatively develop their imagination, dexterity, and growth. The relative absence of studies related to early learning and playful parenting indicates a need for additional evidence on the nature and prevalence of early learning and playful parenting and innovative ways to protect and promote them during health emergencies.
Data Availability
The data supporting the findings of this study are available within the article and its supplementary materials.
SUPPLEMENTARY TABLE: SUMMARY OF INCLUDED STUDIES
Responsive caregiving: Caregiver stress and mental health
Responsive caregiving: Fathers’ engagement in caregiving and gendered division of labour
Responsive caregiving: breastfeeding support
Opportunities for early learning
Opportunities for early learning: Outdoor play and physical activity
Safety and Security: Child protection from violence and neglect
Safety and Security: Child Injury
Footnotes
The Lego Foundation supported this work.
The authors alone are responsible for the views expressed in this article. They do not necessarily represent the views, decisions, or policies of the institutions with which they are affiliated.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.
- 16.↵
- 17.↵
- 18.↵
- 19.
- 20.↵
- 21.↵
- 22.↵
- 23.
- 24.↵
- 25.↵
- 26.
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.
- 35.
- 36.
- 37.↵
- 38.↵
- 39.
- 40.
- 41.↵
- 42.↵
- 43.↵
- 44.
- 45.↵
- 46.↵
- 47.
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.
- 54.↵
- 55.↵
- 56.
- 57.
- 58.↵
- 59.↵
- 60.↵
- 61.
- 62.↵
- 63.
- 64.
- 65.
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.
- 83.↵
- 84.↵
- 85.
- 86.↵
- 87.
- 88.↵
- 89.↵
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.↵
- 97.
- 98.
- 99.↵
- 100.
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.
- 111.↵
- 112.
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵



