
Abstract
The emergence of SARS-CoV-2 variants raises concerns about their resistance to neutralizing antibodies elicited from previous infection, or from vaccination. Here we examined whether sera and monoclonal antibodies from convalescent donors, prior to and following a single immunization with the Pfizer or Moderna mRNA vaccines, neutralize the Wuhan-Hu-1 strain and a variant, B.1.351 from South Africa. Pre-vaccination sera weakly neutralized Wuhan-Hu-1 and sporadically neutralized B.1.351. Immunization with either vaccine generated anamnestic B and CD4+ T cell responses and a 1000-fold increase in neutralizing antibody titers against both strains and SARS-CoV-1. Neutralization was likely due to anti-RBD and anti-S2 antibodies. Our study highlights the importance of vaccination of both uninfected and of previously infected subjects, as the elicited immune response will neutralize distinct viral strains.
Introduction
The SARS-CoV-2 betacoronavirus first emerged in the Hubei Province of China in late 2019 and has since infected over 95 million people and caused over 2 million deaths in 191 countries (1-3).
Infection is mediated by the viral spike protein (S) which is comprised of an N-terminal S1 domain that contains a N-terminal domain (NTD), a C-terminal domain (CTD), and a receptor binding domain (RBD) which mediates attachment to the entry receptor angiotensin converting enzyme 2 (ACE2) and a C-terminal S2 domain that contains the fusion machinery (4-8).
Pre-existing immunity to SARS-CoV-2 is associated with protection against re-infection in humans (9-11) and in non-human primates (12, 13). Although the correlates of protection in humans against repeat infection or following vaccination have not been firmly established, neutralizing antibodies are thought to be an important component of a protective immune response against SARS-CoV-2 infection (14, 15). In support of this, passive transfer of neutralizing antibodies limits respiratory tract infection and protects against symptomatic infection in animal models (16-20). Moreover, neutralizing antibodies may contribute to protection against infection in humans (9). SARS-CoV-2 infection rapidly elicits neutralizing antibody responses (16, 21-24) that decline, but remain detectable over several months (25-29).
The majority of serum neutralizing antibody responses elicited during natural infection are directed at the RBD (21, 23, 30-32). Numerous neutralizing anti-RBD monoclonal antibodies have been characterized, the most potent of which block the RBD-ACE2 interaction (16, 17, 22-24, 33-37). Neutralizing mAbs targeting epitopes on the NTD of S1 (24, 34, 38-40) and S2 have also been identified (41, 42).
Two mRNA-based vaccines from Pfizer/BioNTech and Moderna have received emergency use authorization in several countries and mass vaccination efforts are underway. Both encode a stabilized ectodomain version of the S protein derived from the Wuhan-Hu-1 strain of SARS-CoV-2 isolated in December 2019(43), show greater than 94% efficacy at preventing COVID-19 illness (44-47) and elicit neutralizing antibodies (48, 49).
Due to the high global burden of SARS-CoV-2 transmission viral evolution is occurring. It is estimated that circulating SARS-CoV-2 lineages accumulate nucleotide mutations at a rate of 1-2 mutations per month (Duchene et al. 2020). Recently, viral variants of concern have emerged in the United Kingdom (B.1.1.7), South Africa (B.1.351), and Brazil (P.1) that harbor specific mutations in their S proteins that may be associated with increased transmissibility (50-55).
Of particular concern are mutations found in the B.1.351 lineage which is defined by the D80A and D215G in the NTD, and the K417N, E484K, N501Y mutations in the RBD and the D614G mutation in S2 (52, 56). An A701V mutation in S2 is also observed at high frequencies, while deletions in 242-244 and a R246I mutation in the NTD and a mutation in the leader peptide (L18F) are present at lower frequencies (52).
The B.1.1.7, B.1.351, and P.1 lineages all harbor a N501Y mutation in the receptor binding domain which increases the affinity for the ACE2 receptor (57, 58), and a D614G mutation which increases virion spike density and infectivity(59). The B.1.351 and P.1 lineages also share the E484K mutations in the RBD and both variants are mutated at 417 (K417T in P.1).
Because mutations found in emergent S variants, decrease sensitivity to neutralization by monoclonal antibodies (mAbs), convalescent plasma and sera from vaccinated individuals (27, 58, 60-70), there is concern that these and other emerging variants can evade neutralizing antibody responses generated during infection with variants circulating earlier in the pandemic and also from neutralizing antibody responses elicited by vaccines that are based on the Wuhan-Hu-1 strain. Indeed, there is concern that these mutations are responsible for reduced efficacy observed in ongoing trials of SARS-CoV-2 vaccines in South Africa (71, 72).
Here we evaluated the susceptibility of a spike variant harboring lineage-defining and prevalent B.1.351 mutations found in circulating variants in South Africa to sera from 10 donors who recovered from COVID-19 and then later received a single immunization with either mRNA vaccine, as well as anti-spike mAbs isolated from infected but not vaccinated patients. Sera from recovered donors displayed weak neutralizing activities to the Wuhan Hu1 strain but only half were able to neutralize the
B.1.351 strain, albeit weakly prior to vaccination. Immunization led to a significant increase in S- and RBD-specific memory B cell frequencies, serum IgG and IgA responses to RBD, IgG antibody responses against cell surface expressed Wuhan Hu1 and B.1.351 spike proteins. Moreover, an ∼1000-fold increase in serum neutralizing antibody responses against both the vaccine-matched Wuhan Hu1 and mis-matched B.1.351 strain was observed, although the median neutralizing titers were significantly (2-3 fold) lower against the latter. Importantly, the post-vaccine sera were able to cross-neutralize a highly divergent SARS-CoV pseudovirus. Our neutralization studies with mAbs suggest that the observed neutralizing activities of post-vaccination sera are likely due to antibodies recognizing the RBD and S2, but not the NTD domain.
Overall, our results strongly suggest that boosting pre-existing immunity through vaccination with the Wuhan Hu1 spike will lead to an increase of neutralizing antibody responses not only against the vaccine-matched strain but also against emerging mutant variants.
Results
Antibody neutralization experiments were performed with pseudoviruses expressing either the full-length Wuhan Hu1 spike, or a spike containing the B.1.351-lineage defining S mutations D80A, D215G, K417N, E484K, N501Y and D614G mutations and the A701V mutation which is highly prevalent in this lineage. The viral stocks were appropriately diluted to achieve comparable entry levels during the neutralization experiments (Fig. S1).
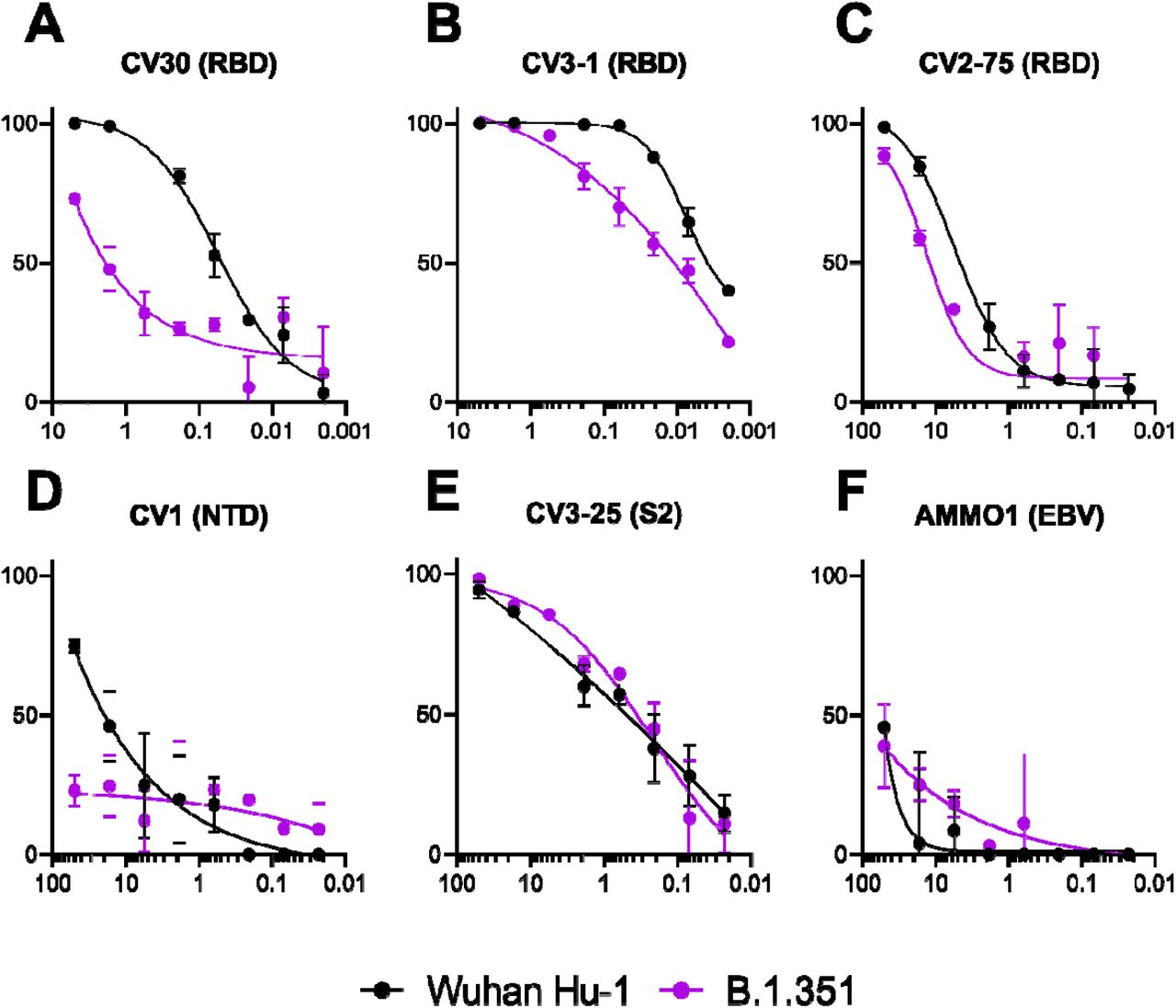
We first evaluated the neutralizing potency of several mAbs targeting different epitopes: three against the RBD (CV30, CV3-1 and CV2-75) that inhibit the ACE2-RBD interaction, one against the NTD (CV1) and one against the S2 subunit (CV3-25) (Fig. S2). CV30 is a member of the VH3-53 class of antibodies that binds to the receptor binding motif (RBM) (22, 33, 73-78). CV30 makes direct contact with the K417 and N501 residues in the RBM that are mutated in the B.1.351 and P.1 lineages, but unlike other known VH3-53 mAbs it does not contact E484 (78). The neutralization potency of this mAb was ∼10 fold weaker towards B.1.351 (Fig. 1A). Similarly, the non-VH3-53 mAbs CV3-1 and CV2-75, were 3- and 4-fold less potent against B.1.351 (Fig. 1B and C). In contrast, the anti-NTD CV1 mAb was unable to neutralize B.1.351 (Fig. 1D). The anti-S2 mAb CV3-25 neutralized both variants comparably (Fig. 1E). As expected, the anti-EBV control mAb AMMO1 (79) failed to neutralize either variant (Fig. 1F). Collectively these data indicate that the B.1.351 virus is more resistant to neutralizing antibodies generated during infection with viral variants from early in the pandemic. We therefore sought to determine whether B.1.351 is resistant to sera from recovered SARS-CoV-2 donors.
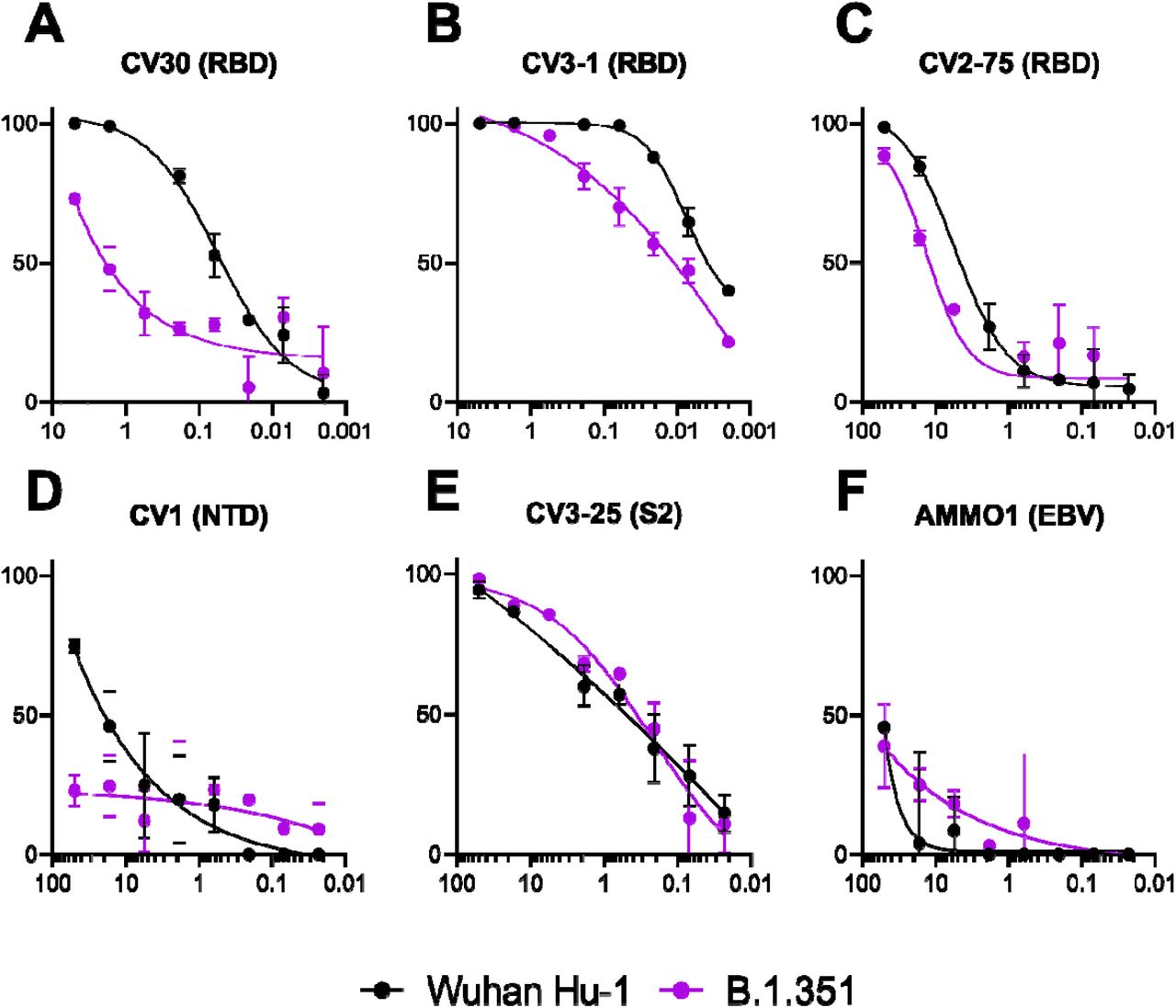
The ability of the mAbs to neutralize Wuhan Hu1 and B.1351 pseudovirus infectivity in 293-ACE2 cells was measured as indicated. The epitope specificity of each mAb is shown in parentheses (RBD: receptor binding domain; NTD: N terminal domain; S2: S2 subunit; EBV: Epstein-Barr virus). Data is represenative of two independent expeiments.
We collected blood and isolated serum and PBMC from persons with previously confirmed SARS-CoV-2 infection who later received a single dose of either the Pfizer/BioNTech or Moderna mRNA vaccine (Table 1). The RBD-specific IgG, IgM and IgA binding responses to the RBD from the Wuhan-Hu1 strain were measured before (average, 202 days post symptom onset; Table 1), and 13-20 days after immunization (average 16 days, Table 1). We observed a significant ∼500-fold increase in median RBD-specific IgG titers (Fig. 2A, paired Wilcoxon p=0.002), and a significant 200-fold increase in median RBD-specific IgA titers (Fig. 2B, paired Wilcoxon p=0.004) after vaccination. RBD-specific IgM titers were generally lower and were not significantly boosted in response to vaccination (Fig. 2C). The antibody titers corresponded to an increase in RBD- (Fig. 2D) and S-specific IgG+ (Fig. 2E) memory B cell frequencies. Consistent with the serology data, an increase in the frequency of IgA+ (Fig. 2F) but not IgM+ spike-specific memory B cells was observed (Fig. S3). In addition to memory B cell responses, vaccination also induced an S-specific CD4+ T cell response (Fig. 2G). The increase in class switched B cells, CD4+ T cells and antibody titers is consistent with an anamnestic response to the vaccine.
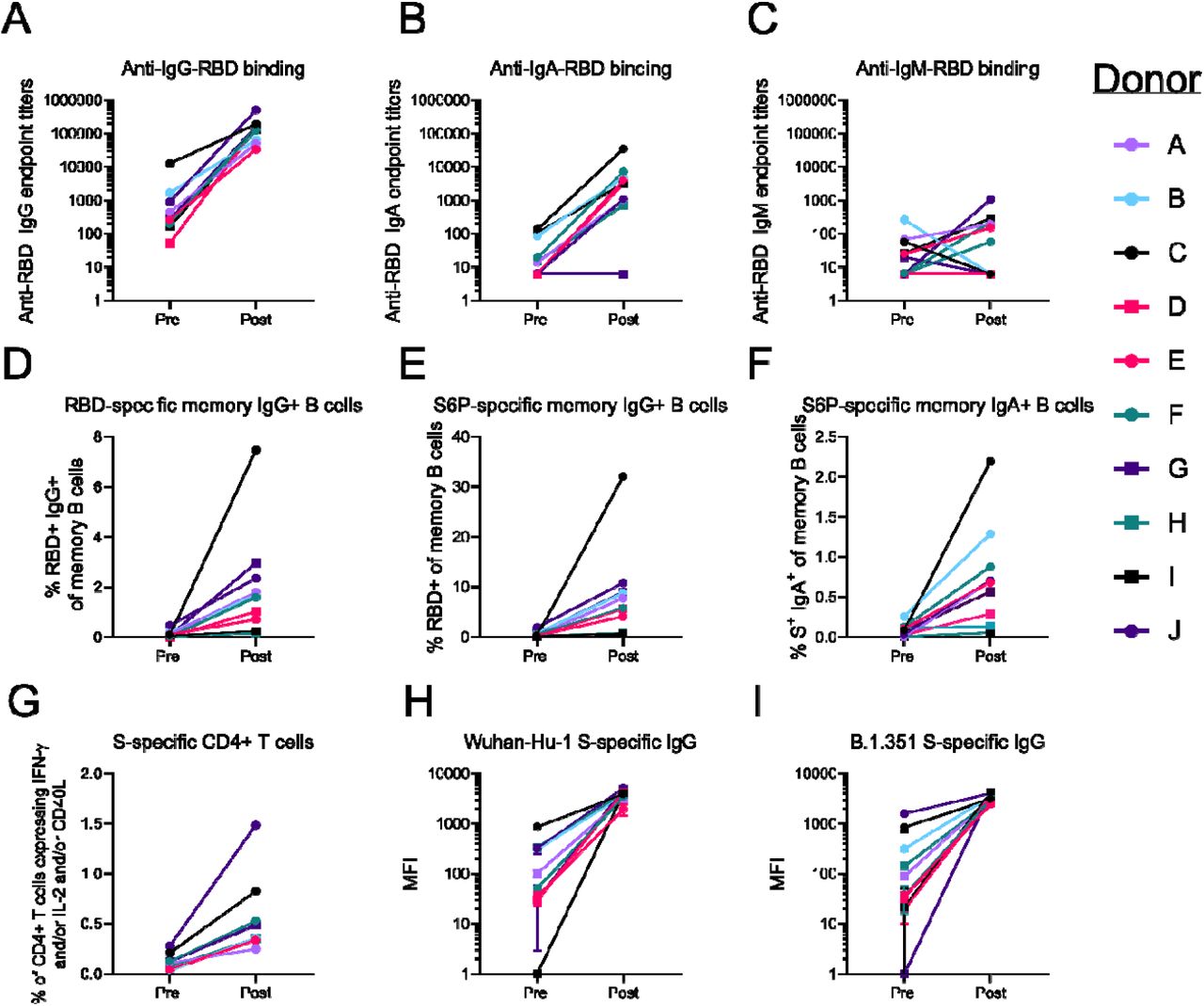
IgG (A) IgA (B) and IgM (C) antibody responses specific to the receptor binding domain of the Wuhan Hu-1 strain from recovered SARS-CoV-2-infected donors were measured prior to and after a single vaccine dose as indicated. (D) Frequency of Wuhan Hu-1 RBD-specific IgG+ memory B cells (live, IgD-, CD19+, CD20+, CD3-, CD14-, CD56-, singlet, lymphocytes) before and after immunization. S6P-specific IgG+ (E) and IgA+ (F) memory B cells before and after immunization. (G) Frequency of S-specific CD4+ T cells expressing IFN-γ and/or IL-2 and/or CD40L. Binding of serum IgG was measured against cell-surface expressed Wuhan-Hu-1 (H) or B.1.351 (I) spike before and after immunization as indicated.
We next compared the binding of serum IgG to full-length SARS-CoV-2 S proteins derived from the Wuhan Hu-1 and the B.1.351 variant expressed on the surface of 293 cells using flow cytometry. Prior to immunization, the IgG responses to the Wuhan-Hu-1 spike were variable, with up to a 1000-fold difference between donors, one of whom had undetectable serum responses (Donor I) (Fig. 2H, median MFI = 70). A similar range of IgG responses were observed against the B.1.351 spike (Fig. 2I, median MFI = 73) before immunization. After vaccination, there was ∼50-fold increase in binding signal to both spikes but binding to the B.1.351 variant was significantly lower (Figs. 2H and I, median MFI 3850 and 3331 for Wuhan-Hu1 and B.1.351, respectively, paired Wilcoxon p=0.049).
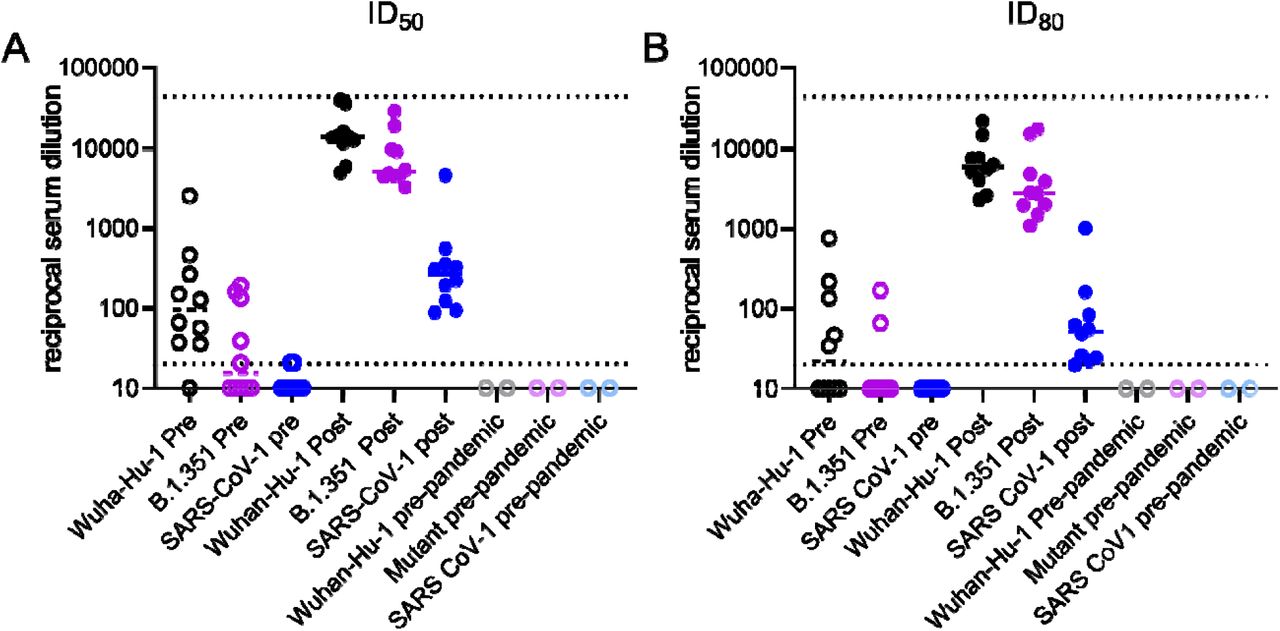
We next compared the ability of pre- and post-vaccine serum to neutralize the Wuhan Hu1 and B.1.351 pseudovirus. Sera from 9 of 10 COVID-19 donors sampled before vaccination were able to neutralize the Wuhan-Hu-1 virus (Fig. 3A and S4). In contrast 5 of 10 pre-vaccine donor sera were unable to neutralize the B.1.351 virus, only 3 had ID50 titers above 100; (Fig. 3A and S4). The median ID50 of the pre-vaccination sera were significantly lower for the Wuhan Hu-1 as compared the B.1.351 virus (97 vs. 15, respectively, paired Wilcoxon p = 0.004), and only two achieved 80% neutralization of the B.1.351 (Fig. 3B and S4).

{kind=link}
{kind=link}
{kind=link}
Neutralizing activities in serum from recovered COVID-19 donors prior to and following a single immunization with the Pfizer/BioNTech or Moderna vaccines against Wuhan-Hu-1 and B.1351 SARS CoV-2 pseudoviruses and SARS-CoV-1 pseudoviruses. (A) Serum dilution resulting in 50% neutralization (ID50).(B) Serum dilution resulting in 80% neutralization (ID80). Samples that did not achieve 50% or 80% neutralization were plotted as 10 which is half the value of the lowest serum dilution. Each dot represents a different donor and the horizonal bars represent the medians. The dashed lines demarcate the highest and lowest serum dilutions tested.
Consistent with the observed increase in binding antibodies following immunization (Figs. 2 and 3), the neutralizing titers were boosted approximately 1000-fold against both strains (Fig. 3A and B, and S4). The half-maximal neutralizing antibody titers (ID50) were significantly higher against the Wuhan Hu1 variant than against B.1.351 (medians, 14,100 vs. 5,156: paired Wilcoxon p=0.002) (Fig. 3A). The median ID80 values were also significantly higher for the Wuhan Hu1 variant compared to the B.1.351 (5,935 vs. 2,814; paired Wilcoxon p=0.02) (Fig. 3B). The neutralizing titers to either strain before or after immunization were not correlated with the time of symptom onset and did not differ by COVID-19 severity (Figs. S5-S8).
The B.1.351 spike examined here contains 7 mutations making it 0.5% divergent from the Wuhan-Hu-1 strain. To assess whether the sera could neutralize representative variant that is much more divergent, we assessed their neutralizing potentials against a SARS-CoV-1 pseudovirus. SARS-CoV-1 and SARS-CoV-2 are 24%, 26% and 50% divergent in the overall S protein, RBD and receptor binding motif respectively (80). As a consequence, several mAbs that potently neutralize SARS CoV-2 fail to bind SARS-CoV-1 (16, 22-24). Consistent with the high level of sequence disparity, sera from recovered donors prior to vaccination were unable to neutralize SARS-CoV-1. However, a single dose of either mRNA vaccine elicited SARS CoV-1 neutralizing titers in all donors (Figs. 3A and B and S6) that were ∼100 fold lower than the titers against the vaccine-matched Wuhan Hu1 strain (median ID50 = 265 and median ID80 = 52, paired Wilcoxon p’s=0.002).
Discussion
Our study reveals that sera from persons who were infected with SARS-CoV-2 early in the pandemic display generally weak neutralizing activities against the Wuhan Hu-1 virus at 4-8 months post-infection but a single immunization with either mRNA vaccines encoding the Wuhan Hu-1 spike, elicited a robust recall response that boosted the neutralizing tiers by approximately 1000-fold.
The SARS-CoV-2 variant B.1.351 which carries several mutations found in highly transmissible variants circulating in South Africa and Brazil, and in agreement with another report was resistant to neutralization by several donors previously infected with SARS-CoV-2 (66). Importantly, vaccination elicited a robust neutralizing antibody response against B.1.351, albeit the neutralizing titers were significantly (2-3) fold lower than they were to the vaccine matched Wuhan-Hu-1 variant. A similarly reduced sensitivity to vaccine-elicited neutralizing antibodies has been reported for B.1.351 (67). Moreover, the vaccine elicited antibody responses capable of neutralizing SARS-CoV-1 that were absent in the pre-vaccine sera. Collectively our data suggest that vaccines based on one of the earliest clinical samples of SARS-CoV-2 is capable of boosting pre-existing antibody titers such that they can neutralize highly divergent neutralization-resistant viral variants.
Both the Pfizer and Moderna vaccines elicit high tiers of anti-RBD and/or S1-directed antibodies (48, 49). Anti-RBD mAbs isolated from convalescent patients retain varying degrees of neutralizing activity against the mutant virus and immunization with either vaccine led to an increase in anti-RBD antibody responses. Collectively, our results suggest that the observed increase in neutralizing antibody responses post-vaccination is primarily due to an increase in anti-RBD antibodies. The inability of an NTD-directed mAb to neutralize B.1.351 however, suggests anti-NTD neutralizing antibodies generated in response to infection with variants from early in the pandemic, may not be effective against emerging mutant variants. Particularly since this region appears to tolerate antigenic variation in SARS-CoV-2 and other coronaviruses (50, 52, 55, 81).
Very few SARS-CoV-2 anti-S2 neutralizing mAbs have been characterized to date (41, 42). The anti-S2 neutralizing mAb CV3-25 tested here displayed comparable potency against the Wuhan Hu-1 and mutant strain evaluated here, indicating that anti-S2 antibodies may also have contributed to the observed increase in neutralizing antibody responses against both strains. This is further supported by the observed neutralization against SARS-CoV-1, which is more divergent from SARS-CoV-2 in the RBD and more conserved in S2. Also, CV3-25 may prove particularly useful for therapeutic or prophylactic applications against emerging viral variants.
Although the correlates of protection for SARS CoV-2 vaccines have not been established, studies in non-human primates indicate that even low titers of neutralizing antibodies are sufficient to prevent experimental SARS-CoV-2 infection in NHPs (18). Our study strongly suggests that previously infected subjects will benefit from even a single immunization with either the Pfizer or Moderna vaccines. They also suggest that boosting pre-existing antibody responses to the spike protein will lead to significant increases in serum neutralizing antibody responses against vaccine-matched and emerging variants.
Material and Methods
Human Subjects
Peripheral blood mononuclear cells (PBMCs) and serum were collected from donors who recovered from SARS-CoV-2 infection and were the first 10 who then subsequently received a SARS-CoV-2 vaccine as part of the study, “Seattle COVID-19 Cohort Study to Evaluate Immune Responses in Persons at Risk and with SARS-CoV-2 Infection”. Serum from pre-pandemic controls were blindly selected at random from the study, “Establishing Immunologic Assays for Determining HIV-1 Prevention and Control”, with no considerations made for age, or sex. Both studies were recruited at the Seattle HIV Vaccine Trials Unit (Seattle, Washington, USA). Informed consent was obtained from all participants and the Fred Hutchinson Cancer Research Center Institutional Review Board approved the studies and procedures (IR10440 and IR5567).
Cell Lines
All cell lines were incubated at 37°C in the presence of 5% CO2. 293-6E (human female) and 293T cells (human female) cells were maintained in Freestyle 293 media with gentle shaking. HEK-293T-hACE2 (human female) were maintained in DMEM containing 10% FBS, 2 mM L-glutamine, 100 U/ml penicillin, and 100 µg/ml streptomycin (cDMEM).
Recombinant CoV proteins and mAbs
A stabilized version of the recombinant SARS-CoV-2 spike protein (S2P) and the SARS CoV-2 RBD were produced in 293E cells as previously described (8, 22). Recombinant CV1, CV30 and AMMO1 were expressed in 293 cells and purified using protein A resin as previously described (22, 79). CV3-1, CV3-25, CV2-75 mAbs were isolated from donors previously infected with SARS-CoV-2 using recombinant S2P as bait using methods outlined in (22)
Generation of plasmids expressing SARS-CoV-1 and SARS-CoV-2 spike variants
To generate a plasmid encoding the SARS-CoV-2 spike B.1.351 variant (pHDM-SARS-CoV-2-Spike-B.1.351) we designed primers that anneal 5’ of the D80 codon and just 3’ of the A701 codon on the pHDM-SARS-CoV-2 Spike Wuhan-Hu-1 plasmid that were used to amplify cDNA corresponding to the N and C termini of the spike protein and the plasmid backbone using Platinum SuperFi II DNA Polymerase (Thermofisher Cat# 12368010) according to the manufacturer’s instructions. cDNA encoding the rest of the spike protein including the D80A, D215G, K417N, E484K, N501Y, D614G and A701V mutations was synthesized as two g blocks (Integrated DNA technologies). The first had 30nt of homology with the PCR amplified vector backbone at the 5’ end. The second included and 30nt of homology with the 3’ end of the first block at the 5’ end and 30nt of homology with the PCR amplified vector backbone at the 3’ end. The g blocks and PCR product were ligated together using InFusion HD cloning Plus (TakaraBio Cat#638920).
To generate a plasmid encoding the SARS-CoV-2 spike, codon-optimized cDNA corresponding to the SARS-CoV S protein (Urbani, GenBank: AAP13441.1) flanked on the 5’ end by 30nt of homology upstream of and including the EcoRI site, and flanked on the 3’ end by 30nt of homology downstream of and including the HindIII site on the pHDM-SARS-CoV-2 Spike Wuhan-Hu-1 plasmid was synthesized by Twist Biosciences. The synthesized DNA was cloned into the pHDM-SARS-CoV-2 Spike Wuhan-Hu-1 plasmid that was cut with EcoRI and HindIII and gel purified to remove the SARS-CoV-2 Spike cDNA using InFusion HD cloning Plus (TakaraBio Cat#638920). The sequences of the cDNA in pHDM-SARS-CoV-Spike-B.1.351 and pHDM-SARS-CoV Spike were verified by Sanger sequencing (Genewiz Inc.).
Pseudovirus neutralization assay
HIV-1 derived viral particles were pseudotyped with full length wildtype S from Wuhan Hu1, B.1.351, or SARS CoV-1 using a previously described reporter system (82), Briefly, plasmids expressing the HIV-1 Gag and pol (pHDM540 Hgpm2), HIV-1Rev (pRC-CMV-rev1b), HIV-1 Tat (pHDM-tat1b), the SARS-CoV-2 spike (pHDM-SARS-CoV-2 Spike Wuhan-Hu-1, pHDM-SARS-CoV-2 Spike B.1.351, or pHDM-SARS-CoV-1 Spike) and a luciferase/GFP reporter (pHAGE-CMV-Luc2-IRES542 ZsGreen-W) were co-transfected into 293T cells at a 1:1:1:1.6:4.6 ratio using 293 Free transfection reagent according to the manufacturer’s instructions. Pseudoviruses lacking a spike protein were also produced as a control for specific viral entry. Pseudoviron production was carried out at 32 °C for 72 hours after which the culture supernatant was harvested, clarified by centrifugation and frozen at −80°C.
293 cells stably expressing human ACE2 (293T-ACE2)(82) were seeded at a density of 4×103 cells/well in a 100 µL volume in 96 well flat bottom black-walled, clear bottom tissue culture plates (Greiner CELLSTAR Cat#655090). The next day, mAbs or sera were serially diluted in 70 µL of cDMEM in 96 well round bottom master plates in duplicate wells. 30 µL of serially diluted mAbs or sera from the master plate were replica plated into 96 well round bottom plates. An equal volume of viral supernatant diluted to achieve comparable luciferase values between SARS-CoV-2 variants (Fig S1) was added to 96 well round bottom plates containing identical serial dilutions from the same master plate, and incubated for 60 min at 37 °C. Meanwhile 50 μL of cDMEM containing 6 µg/mL polybrene was added to each well of 293T-ACE2 cells (2 µg/mL final concentration) and incubated for 30 min. The media was aspirated from 293T-ACE2 cells and 100 µL of the virus-antibody mixture was added. The plates were incubated at 37°C for 72 hours. The supernatant was aspirated and replaced with 100 μL of Steadyglo luciferase reagent (Promega) and read on a Fluorskan Ascent Fluorimeter. Control wells containing virus but no antibody (cells + virus) and no virus or antibody (cells only) were included on each plate.
Percent neutralization for each well was calculated as the RLU of the average of the cells + virus wells, minus test wells (cells +mAb/sera + virus), and dividing this result difference by the average RLU between virus control (cells + virus) and average RLU between wells containing cells alone, multiplied by 100. The antibody concentration, or serum dilution that neutralized 50% or 80% of infectivity (IC50 and IC80 for mAbs, ID50 and ID80 for serum) was interpolated from the neutralization curves determined using the log(inhibitor) vs. response -- Variable slope (four parameters) fit using automatic outlier detection in Graphpad Prism Software.
Cell surface SARS-CoV-2 S binding assay
pHDM-SARS-CoV-2 Spike Wuhan-Hu-1, or pHDM-SARS-CoV-2 Spike B.1.351 were transfected into suspension-adapted 293 cells using 293 Free transfection reagent according to the manufacturer’s instructions. Transfected cells were incubated for 24h at 37°C with shaking and then harvested, washed with chilled FACS wash buffer (PBS +2% FBS + 1 mM EDTA) and placed on ice.
To analyze serum antibody binding, serum was diluted 1:100 in triplicate wells. An equal volume containing 5×105 293 cells expressing SARS-CoV-2 spike protein was added to each well and incubated for 30 min on ice. The cells were then washed with FACS buffer and then incubated with a PE-conjugated AffiniPure Fab fragment goat anti-human IgG (1:100 dilution, Jackson Immuno Research, Cat # 2-1565-050) and a fixable live/dead stain (1:200 dilution, eBioscience, Cat # 65-0866-18) in 50µl FACS buffer and incubated for an additional 20 min on ice. The cells were then washed with FACS buffer and fixed with 10% formalin. The mean fluorescence PE intensity (MFI) on live cells was measured on a BD LSR-II cytometer and the data analyzed using Flow Jo version 9.9.4. For each serum sample or mAb dilution the average MFI of PE signal measured on mock transfected was subtracted from the MFI of cells expressing spike.
RBD ELISAs
Half-well area plates (Greiner) were coated with purified RBD protein at 16.25ng/well in PBS (Gibco) for 14-24h at room temperature. After 4 150ul washes with 1X PBS, 0.02% Tween-2 (Sigma) using the BioTek ELx405 plate washer, the IgA and IgG plates were blocked at 37° C for 1-2 hours with 1X PBS, 10% non-fat milk (Lab Scientific), 0.02% Tween-20 (Sigma); IgM plates were blocked with 1X PBS, 10% non-fat milk, 0.05% Tween-20.
Serum samples were heat inactivated by incubating at 56° C for 30 minutes, then centrifuged at 10,000 x g / 5 minutes, and stored at 4° C previous to use in the assay. For IgG ELISAs, serum was diluted into blocking buffer in 7-12 1:4 serial dilutions stating at 1:50. For IgM and IgA ELISAs, serum was diluted into 7 1:4 serial dilutions stating at 1:12.5 to account for their lower concentration. A qualified pre-pandemic sample (negative control) and a standardized mix of seropositive serums (positive control) was run in each plate and using to define passing criteria for each plate. All controls and test serums at multiple dilutions were plated in duplicate and incubated at 37° C for 1 hour, followed by 4 washes in the automated washer. 8 wells in each plate did not receive any serum and served as blocking controls.
Plates then were plated with secondary antibodies (all from Jackson ImmunoResearch) diluted in blocking buffer for 1h at 37C. IgG plates used donkey anti-human IgG HRP diluted at 1:7500; IgM plates used goat anti-human IgM HRP diluted at 1:10,000; IgA plates used goat anti-human IgA HRP at 1:5000. After 4 washes, plates were developed with 25ul of SureBlock Reserve TMB Microwell Peroxide Substrate (Seracare) for 4 min, and the reaction stopped by the addition of 50μl 1N sulfuric acid (Fisher) to all wells. Plates were read at OD450nm on SpectraMax i3X ELISA plate reader within 20 min of adding the stop solution.
OD450nm measurements for each dilution of each sample were used to extrapolate endpoint titers when CVs were less than 20%. Using Excel, endpoint titers were determined by calculating the point in the curve at which the dilution of the sample surpassed that of 5 times the average OD450nm of blocking controls + 1 standard deviation of blocking controls.
Spike and RBD memory B cell flow cytometry assays
Fluorescent SARS-CoV-2-specific S6P (83) (provided by Roland Strong, Fred Hutchinson Cancer Research Center, Seattle, WA) and RBD probes were made by combining biotinylated protein with fluorescently labeled streptavidin. The S6P probes were made at a ratio of 1:1 molar ratio of trimer to SA. Two S6P probes, one labeled with AlexaFluor488 (Invitrogen), one labeled with AlexaFluor647 (Invitrogen), were used in this panel in order to increase specificity of the detection of SARS-CoV-2-specific B cells. The RBD probe was prepared at a 4:1 molar ratio of RBD monomers to SA, labeled with R-phycoerythrin (Invitrogen). Cryopreserved PBMCs from SARS-CoV-2-convalescent participants and a pre-pandemic SARSCoV-2-naïve donor were thawed at 37°C and stained for SARS-CoV-2-specific memory B cells with a flow cytometry panel shown in Supplementary Table 1. Cells were stained first with the viability stain (Invitrogen) in PBS for 15 min at 4°C. Cells were then washed with 2% FBS/PBS and stained with a cocktail of the three probes for 30 min at 4°C. The probe cocktail was washed off with 10% FBS/PBS and the samples were stained with the remaining antibody panel and incubated for 25 min at 4°C. The cells were washed two times and resuspended in 1% paraformaldehyde/1x PBS for collection on an LSR II flow cytometer (BD Biosciences). Data was analyzed in Flow Jo version 9.9.4.
Intracellular Cytokine Staining (ICS) Assay
Flow cytometry was used to examine SARS-CoV-2-specific CD4+ T-cell responses using a validated ICS assay. The assay was similar to published reports(84, 85) and the details of the staining panel are included in Supplemental Table 2. Two peptide pools (15 amino acids overlapping by 11 amino acids, provided by BioSynthesis) covering the spike protein of SARS-CoV-2 were used for the six-hour stimulation. Peptide pools were used at a final concentration of 1 µg/ml for each peptide. As a negative control, cells were not stimulated, only the peptide diluent (DMSO) was included. As a positive control, cells were stimulated with a polyclonal stimulant, staphylococcal enterotoxin B (SEB). Cells expressing IFN-γ and/or IL-2 and/or CD154 was the primary endpoint for antigen-specific CD4+ T cells. The overall response to spike was defined as the sum of the background-subtracted responses to the spike 1 and spike 2 individual pools. The total number of CD4+ T cells must have exceeded 10,000 the assay data to be included in the analysis.
Biolayer interferometry (BLI)
BLI experiments were performed on an Octet Red instrument at 30°C with shaking at 500-1000 rpm. mAbs were loaded at a concentration of 20 mg/mL in PBS onto Anti-Human IgG Fc capture (AHC) biosensors (Fortebio) for 300s, followed by a 60s baseline in KB buffer (1X PBS, 0.01% Tween 20, 0.01% BSA, and 0.005% NaN3, pH 7.4). Probes were then dipped in KB containing either; SARS-CoV-2 RBD (2.0µM), S-2P (0.5µM), S1 NTD (0.5µM, SinoBiological Cat # 40591-V49H) or S2 (0.5µM, SinoBiological Cat # 40590-V08B) for a 300s association phase, followed by a 300s dissociation phase in KB. The binding of mature VRC01 (86) was used as negative control to subtract background binding at each timepoint.
Data Availability
All data is provided in the manuscript.
AUTHOR CONTRIBUTIONS
Conceptualization M.J.M., A.T.M., and L.S.; Investigation, Y-H. W., E.S., M.L., V.R., K.W.C. Z.M., M.N., L.J.H., A.J.M., M.J, J.F, G.M., H.G., A.J.M; Writing-Original Draft, A.T.M., and L.S.; Writing-Review & Editing, A.T.M., L.S., M.J.M., E.S., Funding Acquisition, L.S. M.J.M; Resources, M.J.M.,J.C., A.F.; Supervision, A.T.M.
ACKNOWLEDGMENTS
This work was supported by generous donations to Fred Hutch COVID-19 Research Fund, and to MJM from the Paul G. Allen Family Foundation, the Joel D. Meyers Endowed Chair, and NIAID UM1 AI068618-14S1, 2UM1 AI069481-15, and UM1A057266-S1. We thank Laura Richert Spuhler for assistance with figure preparation, Trevor Bedford for assistance in selecting the appropriate mutations in the SARS-CoV-2 spike, and Todd Haight and the Seattle Vaccine Unit specimen processing lab and staff for their service, and the study participants for their dedication to this project.,
References
- 1.↵
- 2.
- 3.↵
- 4.↵
- 5.
- 6.
- 7.
- 8.↵
- 9.↵
- 10.
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.
- 27.↵
- 28.
- 29.↵
- 30.↵
- 31.
- 32.↵
- 33.↵
- 34.↵
- 35.
- 36.
- 37.↵
- 38.↵
- 39.
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.
- 46.
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.
- 52.↵
- 53.
- 54.
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.↵
- 67.↵
- 68.
- 69.
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.
- 75.
- 76.
- 77.
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵



