
Abstract
Background The introduction of the bacterium Wolbachia (wMel strain) into Aedes aegypti mosquitoes reduces their capacity to transmit dengue and other arboviruses. Evidence of a reduction in dengue case incidence following field releases of wMel-infected Ae. aegypti has been reported previously from a cluster randomised controlled trial in Indonesia, and quasi-experimental studies in Indonesia and northern Australia.
Methods Following a period of intensive community engagement, deployments of adult wMel-infected Ae. aegypti mosquitoes were conducted in Niterói, Brazil during 2017 – 2019. Deployments were phased across four release zones, with a total area of 83 km2 and a residential population of approximately 373,000. A quasi-experimental design was used to evaluate the effectiveness of wMel deployments in reducing dengue and chikungunya incidence. An untreated control zone was pre-defined, which was comparable to the intervention area in historical dengue trends. The wMel intervention effect was estimated by controlled interrupted time series analysis of monthly dengue and chikungunya case notifications to the public health surveillance system before, during and after releases, from release zones and the control zone.
Results Three years after commencement of releases, wMel introgression into local Ae. aegypti populations was heterogeneous throughout Niterói, reaching a high prevalence (>80%) in the earliest release zone, and more moderate levels (prevalence 40–70%) elsewhere. Despite this spatial heterogeneity in entomological outcomes, the wMel intervention was associated with a 69% reduction in dengue incidence (95% confidence interval 54%, 80%) and a 60% reduction in chikungunya incidence (95%CI 21%, 80%), in the aggregate release area compared with the pre-defined control area. This significant intervention effect on dengue was replicated across all four release zones, and in three of four zones for chikungunya.
Conclusions We demonstrate that wMel Wolbachia can be successfully introgressed into Ae. aegypti populations in a large and complex urban setting, and that a significant public health benefit from reduced incidence of dengue and chikungunya accrues even where the prevalence of wMel in local mosquito populations is moderate and spatially heterogeneous. These findings are consistent with the results of randomised and non-randomised field trials in Indonesia and northern Australia, and demonstrate the effectiveness of the Wolbachia biocontrol method as a multivalent intervention against both dengue and chikungunya.
Background
Dengue is a mosquito-borne disease transmitted primarily by the Aedes aegypti mosquito, which has increased globally in both case burden and geographic footprint over the past 50 years. Approximately 40% of the world’s population are at risk of dengue transmission, with an estimated 400 million infections per year resulting in 50 – 100 million clinical cases and 3.6 million hospitalisations.1,2 The economic cost to health systems and communities has been estimated at $8.9 billion per annum.3 In Brazil, more than 1.5 million dengue cases and 782 deaths were reported nationally in 2019, with in excess of 1300 cases per 100,000 population in the worst affected Central-West region. In the same year 132,000 cases of chikungunya - also transmitted by Ae. aegypti mosquitoes - were reported, including 92 deaths.
Current strategies for dengue control are limited to efforts to suppress immature and adult mosquito numbers, through spraying of insecticides and community campaigns to reduce breeding sites. Even where considerable resources are invested in these activities, sustained suppression of mosquito densities has been elusive, and seasonal outbreaks continue to occur.4,5 There is a well-recognised need for new, affordable and effective tools for control of dengue and other Aedes-borne arboviruses, including chikungunya and Zika.4,6
Stable introduction of the common insect bacterium Wolbachia into Ae. aegypti has been shown in the laboratory to result in a reduced capacity of Ae. aegypti to transmit dengue and other Aedes-borne arboviruses including chikungunya, Zika, Yellow Fever and Mayaro virus.7–14 Accumulating evidence from field sites in Australia and Indonesia has demonstrated a collapse in local dengue transmission in areas where short-term releases of Wolbachia-infected mosquitoes have resulted in introgression and sustained high prevalence of Wolbachia in local Ae. aegypti populations.15–17 A recently completed cluster randomised trial of wMel Wolbachia deployments in Yogyakarta, Indonesia, conclusively demonstrated the efficacy of the method, with a 77% reduction in dengue incidence in Wolbachia-treated neighbourhoods compared to untreated areas.18 The Yogyakarta CRT included chikungunya and Zika as secondary endpoints, but insufficient cases were detected to permit an evaluation of efficacy against these arboviruses. Acquiring field evidence for the effectiveness of Wolbachia in reducing transmission of these arboviruses is a priority, as is the accumulation of real-world evidence for public health impact from large-scale implementations of wMel-infected Ae. aegypti in the complex urban environments common throughout dengue-endemic areas.
Pilot releases of Wolbachia-infected mosquitoes started in 2015 in Rio de Janeiro and Niterói, Brazil. In 2017 Niterói became the first site in Brazil to move to scaled deployments across a large urban area. The intervention involved a phased approach including engagement with and acceptance by the community, communication strategies to ensure the communities were informed and supportive, releases of Wolbachia-infected Ae. aegypti mosquitoes, and monitoring of the levels of Wolbachia in Ae. aegypti in the field.
We report here the entomological and epidemiological outcomes of a large-scale non-randomised deployment of Wolbachia-infected Aedes aegypti mosquitoes in the Brazilian city of Niterói, for the control of dengue and other Aedes-borne diseases. The impact of Wolbachia deployment on dengue and chikungunya incidence was evaluated via a quasi-experimental study, using controlled interrupted time series analysis of routine notifiable disease surveillance data together with monitoring of disease activity with outbreak signals routinely used in public health disease surveillance.
Methods
Study setting
Niterói, a municipality of the state of Rio de Janeiro is situated in the Guanabara Bay across from Rio de Janeiro city (22°52’58”S 43°06’14”W). According to the last national census in 2010 it had a population of 484,918 living in an area of 135 km2. The city is divided into 7 health districts for administrative planning. For the evaluation of the impact of Wolbachia mosquito deployments, Niteroi was divided into four release zones and 1 control zone, which are aligned with neighbourhood administrative boundaries (Figure 1). Table 1 shows the baseline characteristics and release summary of each zone.
Baseline characteristics and release summary by zone

showing the municipality of Niterói, comprising four zones in which releases of wMel-infected Aedes aegypti have been undertaken and one pre-defined parallel untreated control zone. Neighbourhood boundaries are shown in white. The inset shows the location of Niterói within the state of Rio de Janeiro, Brazil.
Ethics and approvals
Approval to release Wolbachia-carrying Ae. aegypti mosquitoes into urban areas was obtained from three Brazilian governmental bodies: the National Agency of Sanitary Surveillance (ANVISA); the Ministry of Agriculture, Livestock and Supply (MAPA); and the Brazilian Institute of Environment and Renewable Natural Resources (IBAMA), which issued a Temporary Special Registry (Registro Especial Temporário (RET), nr. 0551716178/2017). Ethical approval was also obtained from the National Commission for Research Ethics (CONEP - CAAE 59175616.2.0000.0008).
Community engagement
WMP Brazil’s Communication and Engagement (C&E) strategy was developed prior to mosquito releases, following a thorough analysis of geographical, social, political, economic and cultural factors in the proposed release areas as previously described.19
In Niterói the C&E plan was focused on three key areas: public schools, primary health care units and social leaders, due to their reach and influence within the release area, including into vulnerable communities. Community Reference Groups (CRGs) were also created, to serve as advisory committees populated by representatives of the planned release areas, to inform the activities of WMP Brazil. This group was also responsible for providing feedback on all communication materials and C&E strategies that were proposed throughout the WMP’s activities in their areas.
Prior to the release of wMel-infected mosquitoes in each area, a survey of awareness and acceptance of the method was conducted by an independent company. In order to reach a wide range of people living and working in the release areas, time-location sampling was used to survey passers-by in busy public locations in each neighbourhood. Respondents (n= 3485 in total) were 18 years and over, and lived or worked in the neighbourhood where the survey was conducted. The questionnaire was developed with the CRG, and included questions on awareness, understanding and acceptance of the proposed wMel releases.
Mosquito production
The Rio wMel-infected Ae. aegypti line described in Garcia et al 201920 was used for releases. The wMel-infected lines were maintained in controlled laboratory conditions, in 900 cm2 mesh-sided rearing cages. Each cage contained 2500-2750 adults, and was fed using donated non-transfusional usable human blood (agreement FIOCRUZ/ Hemominas OF.GPO/CCO-Nr224/16), once per week for two to three gonotrophic cycles. As a quality assurance procedure each blood bag was previously tested for dengue, Zika, chikungunya, mayaro and yellow fever, as described previously21. These colonies consisted of a broodstock (kept in Belo Horizonte) and a release-production colony (kept in Rio de Janeiro). Male Ae. aegypti adults (from F0–F1 field collected material) were introduced into the broodstock cages at a rate of 10-20% every 5 generations. Material from the broodstock colony was then transferred to the release-production colony where it was amplified through 2 generations without the addition of field collected males.
From April 2017 until April 2018 immature stages for adult releases were reared at a density of approximately 1.0 larvae/ml and fed a diet of ground Tetramin Tropical Flakes (Tetra Holding [US] Inc. Germany, Product number 77101). From May 2018, immature stages for adult releases were reared at a density of approximately 2.75 larvae/ml and fed a diet of fish food: liver powder: yeast extract (4:3:1). In both rearing regimes, when approximately 10-30% of larvae had pupated, the larvae/pupae were sieved and between 180-220 larvae/pupae were placed in a release device. Adults were allowed to emerge for 5–6 days and were maintained on a 10% sugar solution for 12-36 hours prior to releases. The release devices were then stacked into boxes for transport to the release site.
Wolbachia deployments
Mosquito deployments took place over a release area of 40 km2 during a period of 35 months (February 2017 - December 2019). Adult wMel-infected mosquitoes were released weekly from a moving vehicle. In Zones 1 - 3 mosquito release points were spaced at regular 50 meter intervals. In Zone 4 the density of release points was adjusted for the residential population in each neighbourhood, with the aim of releasing a total of 100 mosquitoes per resident (average distance between release points was 41 meters). Releases were staged throughout each release zone. Initial release periods were 10-16 weeks duration, with subsequent re-releases conducted in local areas where wMel prevalence was <40% in 3 consecutive monitoring events at least 4 weeks after the conclusion of releases. Most areas of Zones 1 and 2 received two rounds of releases, Zone 3 received 3 rounds of releases and Zone 4 only 1 round of releases.
Wolbachia monitoring
Mosquitoes were collected weekly during and after releases using a network of BG Sentinel traps (Biogents AG, Regensburg, Germany, Product number NR10030) at an average density of 16 BG traps/km2 throughout release areas. Mosquitoes were sent to the laboratory for sorting, morphological identification and counting. The number of mosquitoes caught in each BG trap was recorded by species, sex, and in total. Mosquito samples were stored in 70% ethanol until screening for wMel-strain Wolbachia. Screening was performed weekly until week ending 8 April 2018 and fortnightly thereafter.
Wolbachia molecular detection
A maximum of 10 adult Ae. aegypti per BG trap per collection were screened for the presence of wMel using either quantitative polymerase chain reaction (qPCR), or a colorimetric loop-mediated isothermal amplification (LAMP) assay. Taqman qPCR was performed on a Roche LightCycler 480 as described previously (Dar et al., 2008; O’Neill et al., 2018). Briefly, the qPCR cycling program consisted of a denaturation at 95°C for 5 min followed by 40 cycles of PCR (denaturation at 95 °C for 10 min, annealing at 60 °C for 30 sec, and extension at 72 °C for 1 sec with single acquisition) followed by a cooling down step at 40°C for 30 sec. LAMP reactions were performed in a Bio-Rad C1000 96-well PCR thermocycler with a 30min incubation at 65°C as previously described (O’Neill et al., 2018). Individual reactions consisted of 2X WarmStartR Colorimetric LAMP Master Mix (New England BioLabs, Cat# M1800S), primers and 1 μL of target DNA from a 50μl single mosquito squash buffer extraction assay, in a total reaction volume of 17 μL.
Epidemiological data
Data on dengue and chikungunya cases notified to the Brazilian national disease surveillance system (SINAN) were used to evaluate the epidemiological impact of Wolbachia releases. Reporting of both diseases is mandatory in Brazil. Dengue notification data for Niterói is available from SINAN since 2007 and chikungunya since 2015. Notified dengue and chikungunya cases reported to SINAN are predominantly suspected cases based on a clinical case definition.22
Between 2007 - 2014, approximately 15% of notified dengue cases had supportive laboratory test results, usually from IgM serology. Since the Zika epidemic in Brazil in 2015, laboratory confirmation of dengue has relied on PCR only due to cross-reactive serological responses, and only one dengue case notified in 2015 - 2020 included laboratory confirmation. For chikungunya, 24% of cases notified in 2015 - 2020 had supportive IgM serology results. For the purpose of this analysis, we include all notified dengue and chikungunya cases (suspected and laboratory confirmed).
Anonymized disaggregate data on notified suspected and laboratory-confirmed dengue and chikungunya cases were obtained from the SINAN system through the Health Secretariat of Niterói, for the period from January 2007 (January 2015 for chikungunya) to June 2020. Population data by neighborhood of residence from the Brazilian 2010 census (IBGE) was used to estimate the population in each Wolbachia release zone.
Statistical analysis
The wMel intervention effect was estimated using controlled interrupted time series analysis performed separately for each release zone compared with the pre-defined control area, and for the aggregate release area compared with the control area. The primary analysis included data from January 2007 (dengue) or January 2015 (chikungunya), until June 2020, encompassing 8-37 months of post-intervention observations. For zone-level analyses, negative binomial regression was used to model monthly dengue and chikungunya case counts in the intervention and control areas, with an offset for population size. Seasonal variability in dengue incidence was controlled using flexible cubic splines with knots placed at 6-monthly intervals. For the primary analysis, a binary ‘group’ variable indicated the study arm (intervention or control). A binary ‘treatment’ variable distinguished the pre-intervention period and the post-intervention period. The zone-level post-intervention period was defined as four weeks after wMel releases had commenced throughout the whole zone; the corresponding post-intervention period was also applied to the control area for each zone-level analysis. The intervention effect was estimated from the interaction between the ‘group’ and ‘treatment’ variables, which allows explicitly for a level change in the outcome (dengue/chikungunya case incidence) in both intervention and control areas in the post-intervention period. Robust standard errors were used to account for autocorrelation and heteroskedasticity. A mixed-effects negative binomial regression was used to model monthly dengue and chikungunya case counts in the aggregate release area compared with the control area, with an offset for population size and controlling for seasonal variability in incidence using flexible cubic splines with knots placed at 6-monthly intervals. Clustering of dengue/chikungunya cases by release zone was modelled as a random effect by including a random intercept at the zone level and allowing for a random slope on the intervention. A binary ‘treatment’ variable distinguished the pre-intervention period and the post-intervention period, with the control area classified as ‘pre-intervention’ throughout. Robust standard errors were used to account for autocorrelation and heteroskedasticity.
To account for within-zone heterogeneity in wMel establishment and dengue incidence, a secondary neighbourhood-level analysis was also performed in which Wolbachia exposure was determined by the measured wMel prevalence in Ae. aegypti collected from each neighbourhood, each month, categorised into quintiles of exposure. This analysis included data to March 2020 only, as no Wolbachia monitoring was possible April – June 2020 due to restrictions on movement in response to the Covid-19 pandemic. Mixed-effects negative binomial regression was used to model monthly dengue/chikungunya case notifications by neighbourhood, in each of the four release zones individually and in all zones combined, compared with the pre-specified control zone. The model included population size as an offset and neighbourhood as a random effect. The Wolbachia intervention was modelled as quintiles of monthly neighbourhood-level wMel prevalence, first using the current month and then as a three-month moving average to smooth the variability in monthly wMel prevalence. Given the large number of zero dengue case counts (zero-inflation) at the neighbourhood level, an alternative analysis using a zero-inflated negative-binomial model with robust standard errors to account for clustering was considered. Model fit was not improved by accounting for zero-inflation, as assessed using the Akaike Information Criterion (AIC), and was thus not used in the analyses.
Sensitivity analyses
As a sensitivity analysis, we excluded the neighbourhood of Jurujuba where wMel releases were staggered across seven sectors over a period of 16 months23 and wMel monitoring was initially only done in small pockets of the neighbourhood where releases had already occurred, resulting in a wMel time-series that gradually represents larger portions of the neighbourhood until wMel releases were completed in all parts of Jurujuba. We also excluded pre-intervention observations prior to 2012 to achieve greater balance between pre-intervention and post-intervention period lengths while maintaining sufficient data to inform on pre-intervention trends.24
Power estimation
Power was estimated for the ITS analysis using 1000 simulated datasets drawn from a negative binomial distribution fitted to a ten-year time series (2007–2016) prior to Wolbachia deployment, of monthly dengue case notifications from release and control zones in Niterói and Rio de Janeiro. The simulated time series of dengue case numbers in the control zones as well as the pre-Wolbachia release dengue case numbers in the treated zones were drawn directly from this model-generated distribution. Post-Wolbachia release dengue case numbers in the treated zones were drawn from the same model-generated distribution, modified by an additional parameter for an intervention effect of Relative Risks = 0.6, 0.5, 0.4, 0.3. For each of these four ‘true’ effect sizes and a null effect (RR = 1), applied to each of the 1000 simulated time series, the ‘observed’ effect size was calculated from a negative binomial regression model of monthly case counts in the treated and untreated zones, as described above. Post-intervention time periods of 1, 2 or 3 years were simulated, with the pre-intervention period fixed at 7 years. The estimated power to detect a given effect size was determined as the proportion of the 1000 simulated scenarios in which a significant intervention effect (p<0.05) was observed. These simulations indicate 80% power to detect a reduction in dengue incidence of 50% or greater after three years of post-intervention observations, and a reduction of 60% or greater after two years.
Results
Wolbachia establishment in Niterói
Awareness (prior knowledge of the Wolbachia method) ranged from 36 to 50% and acceptance (agreement with the proposed wMel releases in the neighbourhood) ranged from 65 to 92%, in the public survey conducted prior to releases in Niterói. No negative media nor negative community incidents were registered, and the Community Reference Group endorsed the start of releases.
Heterogeneity in wMel Wolbachia establishment was observed in three of the four release zones (Figure 2). In the initial release area of zone 1, Wolbachia prevalence was greater than 80% in the first quarter of 2020 (up to 11 months post-release) and there was low variability across the neighbourhoods. Local wMel introgression has been more variable in zones 2 and 3, with a median wMel prevalence of 40–70% among neighbourhoods during the post-release period (11 months and 9 months, respectively). In zone 4, a longer post-intervention observation period is required to evaluate the trajectory of wMel establishment.

Circle markers represent the aggregate wMel infection prevalence in each zone in each calendar month from February 2017 to March 2020. Open circles indicate months when Wolbachia releases took place in any part of that zone; filled circles are months with no releases. Horizontal lines represent the median wMel infection rate among the individual neighbourhoods in each zone (n=4 neighbourhoods in Zone 1; n=11 in Zone 2; n=13 in Zone 3; n=5 in Zone 4). Shaded bars show the interquartile range (IQR) of wMel infection rates among the individual neighbourhoods in each zone, each month.
Arboviral disease trends pre- and post-Wolbachia intervention
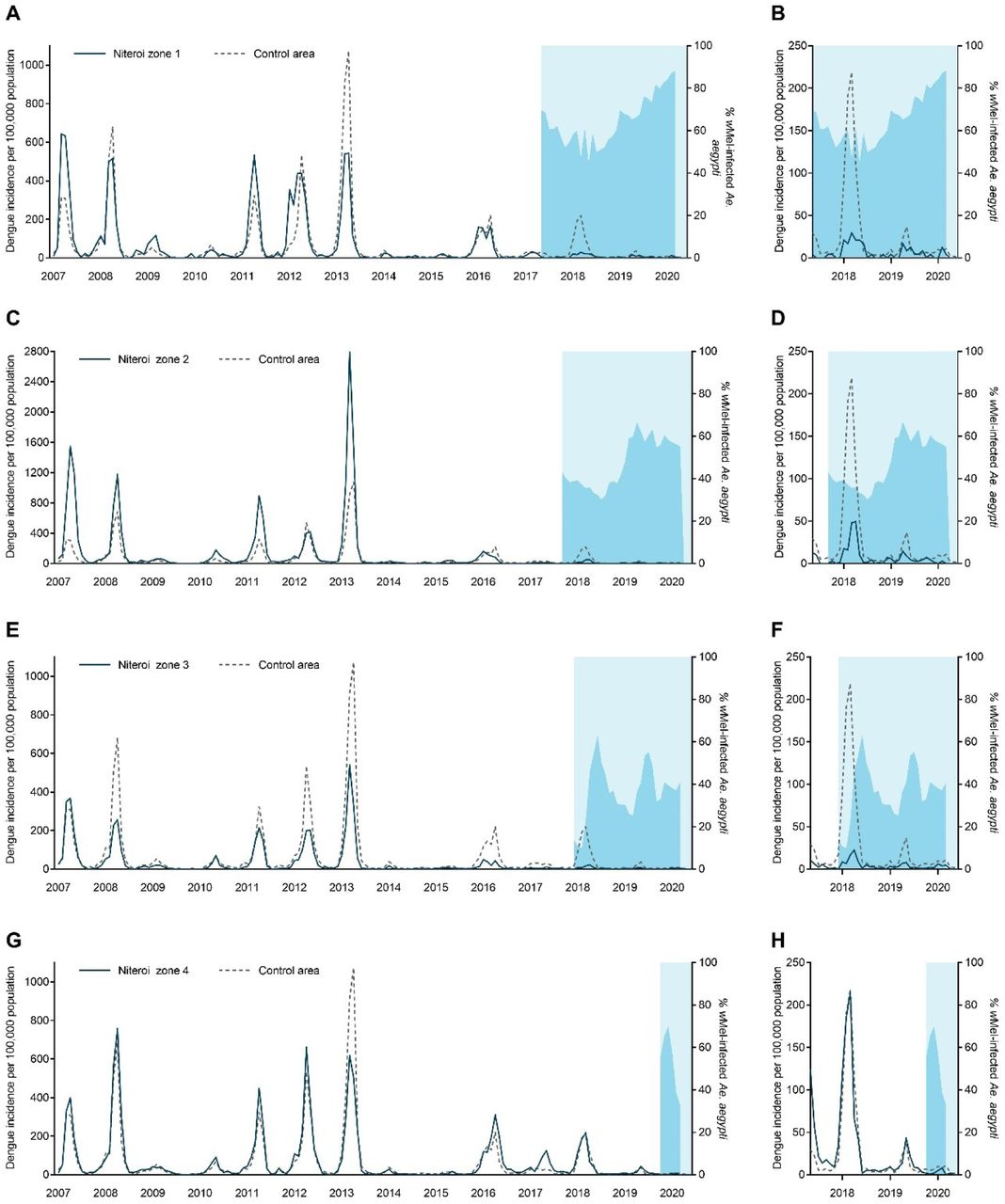
During the ten years prior to the start of scaled Wolbachia mosquito releases in Niterói in early 2017, seasonal peaks in dengue case notifications occurred each year (Figure 3a), usually in March and April (Figure 3b). A median of 2,818 dengue cases were notified each year 2007 - 2016 (per capita incidence 581/100,000 population), with a minimum of 366 cases in 2014 (75/100,000) following a maximum of 11,618 in 2013 (2,396/100,000). In the three years following the start of phased Wolbachia releases, annual city-wide dengue case notifications were 895, 1,729 and 378 in 2017, 2018 and 2019 respectively, and the seasonal peaks in dengue incidence occurred predominantly in the areas of Niterói that had not yet received Wolbachia deployments (Figure 4).

Monthly dengue (a) and chikungunya (b) case notifications in Niterói from January 2007/2015 – June 2020, and dengue (c) and chikungunya (d) case notifications aggregated by calendar month, across the same period.

Panels A,C,E,G: Lines show the monthly incidence of dengue case notifications per 100,000 population (left-hand Y axis) in Niterói release zones 1 - 4 (solid line in each panel) compared with the untreated control zone (dashed line), January 2007 - June 2020. Light blue shading indicates the beginning of the epidemiological monitoring period in each zone, one month after initial releases were completed in each respective zone. Darker blue shading indicates the aggregate wMel infection prevalence (right-hand Y axis) in each zone in each calendar month from the start of the epidemiological monitoring period until March 2020 (no wMel monitoring April-June 2020). Panels B,D,F,H show the same data but zoomed into the period from May 2017 – March 2020 and with the dengue incidence axis rescaled, to show more clearly the trends in release and control zones in the post-intervention period.
Chikungunya surveillance commenced in January 2015. Between 44 and 533 chikungunya cases were notified annually in Niterói in 2015 - 2019, with the exception of 2018 when an explosive outbreak resulted in 3091 reported cases; 95% of those occurred in the six months January to June. The highest per capita incidence of chikungunya during the 2018 outbreak was in the untreated control zone (1,413 cases/100,000 population; Figure 5), followed by Zone 4 where Wolbachia deployments had not yet commenced (958/100,000). In Zones 1, 2, and 3 where deployments were underway and zone-level Wolbachia prevalence was between 20 – 55%, the incidence of chikungunya case notifications during the 2018 outbreak was 106/100,000, 244/100,000 and 201/100,000, respectively.

Lines show the monthly incidence of dengue case notifications per 100,000 population (left-hand Y axis) in Niterói release zones 1 - 4 (solid line in each panel) compared with the untreated control zone (dashed line), January 2015 - June 2020. Light blue shading indicates the beginning of the epidemiological monitoring period in each zone, one month after initial releases were completed in each respective zone. Darker blue shading indicates the aggregate wMel infection prevalence (right-hand Y axis) in each zone in each calendar month from the start of the epidemiological monitoring period until March 2020 (no wMel monitoring April - June 2020).
Reduction in dengue and chikungunya incidence post-Wolbachia intervention
Using interrupted time series (ITS) analysis to account for underlying temporal trends in case incidence and staggered implementation of the intervention, we found that wMel Wolbachia deployments were associated with a significant reduction in dengue incidence in each of the four release zones (Figure 6a). The magnitude of this reduction ranged from 43.8% (95%CI 17.6, 61.7) in Zone 3 to 77.2% (95%CI 63.7, 85.7) in Zone 2. Overall, Wolbachia deployments were associated with a 69.4% (95%CI 54.1, 79.6) reduction in dengue incidence in Niterói (Figure 6a).
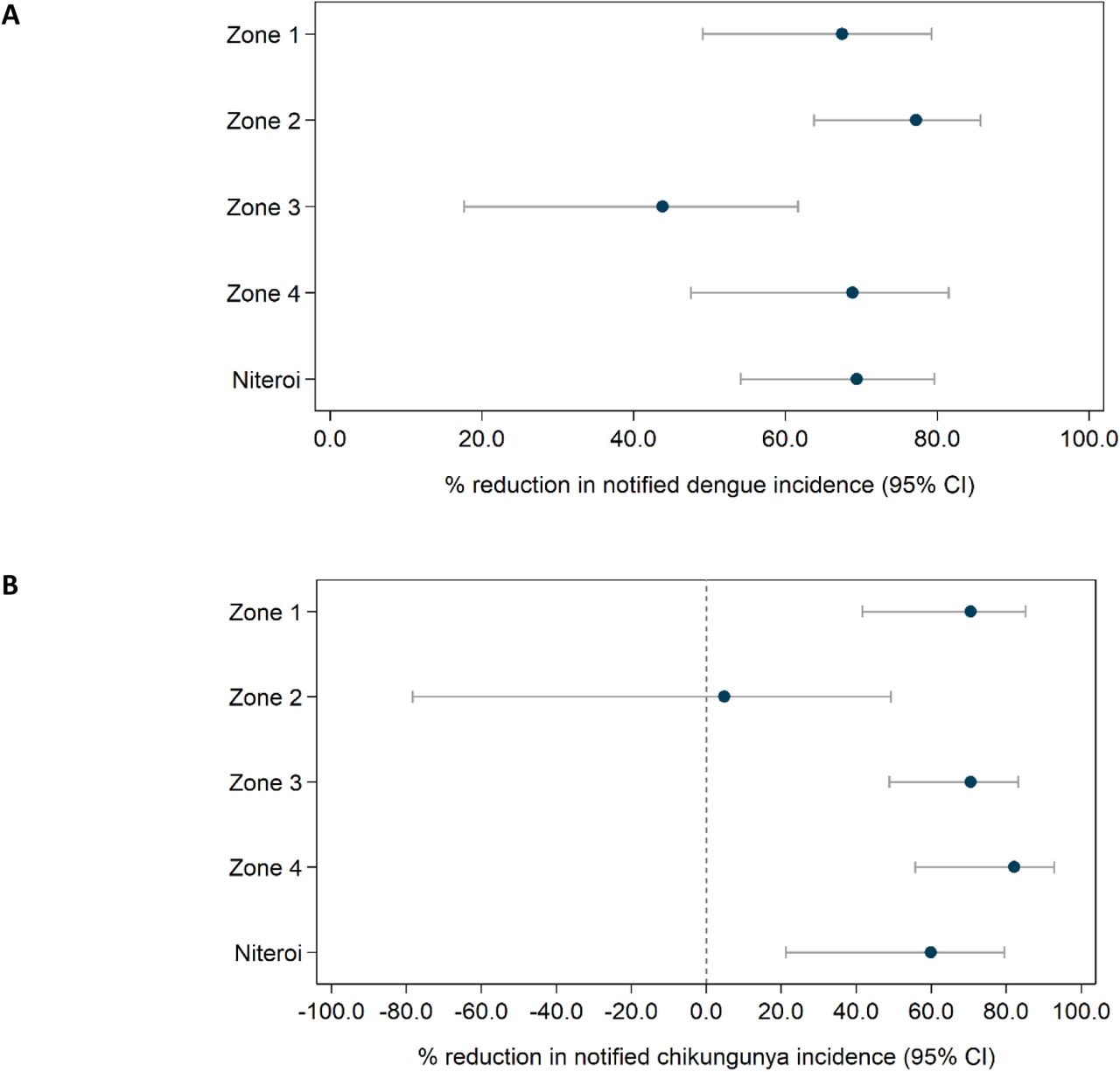
Estimated reduction in the incidence of dengue (A) and chikungunya (B) following Wolbachia deployments in Niterói, in each release zone individually and in the aggregate release area. Point estimates (circles) and 95% confidence intervals (horizontal bars) from controlled interrupted time series analysis of monthly dengue (Jan 2007 – June 2020) and chikungunya (Jan 2015 – June 2020) case notifications to the Brazilian national disease surveillance system).
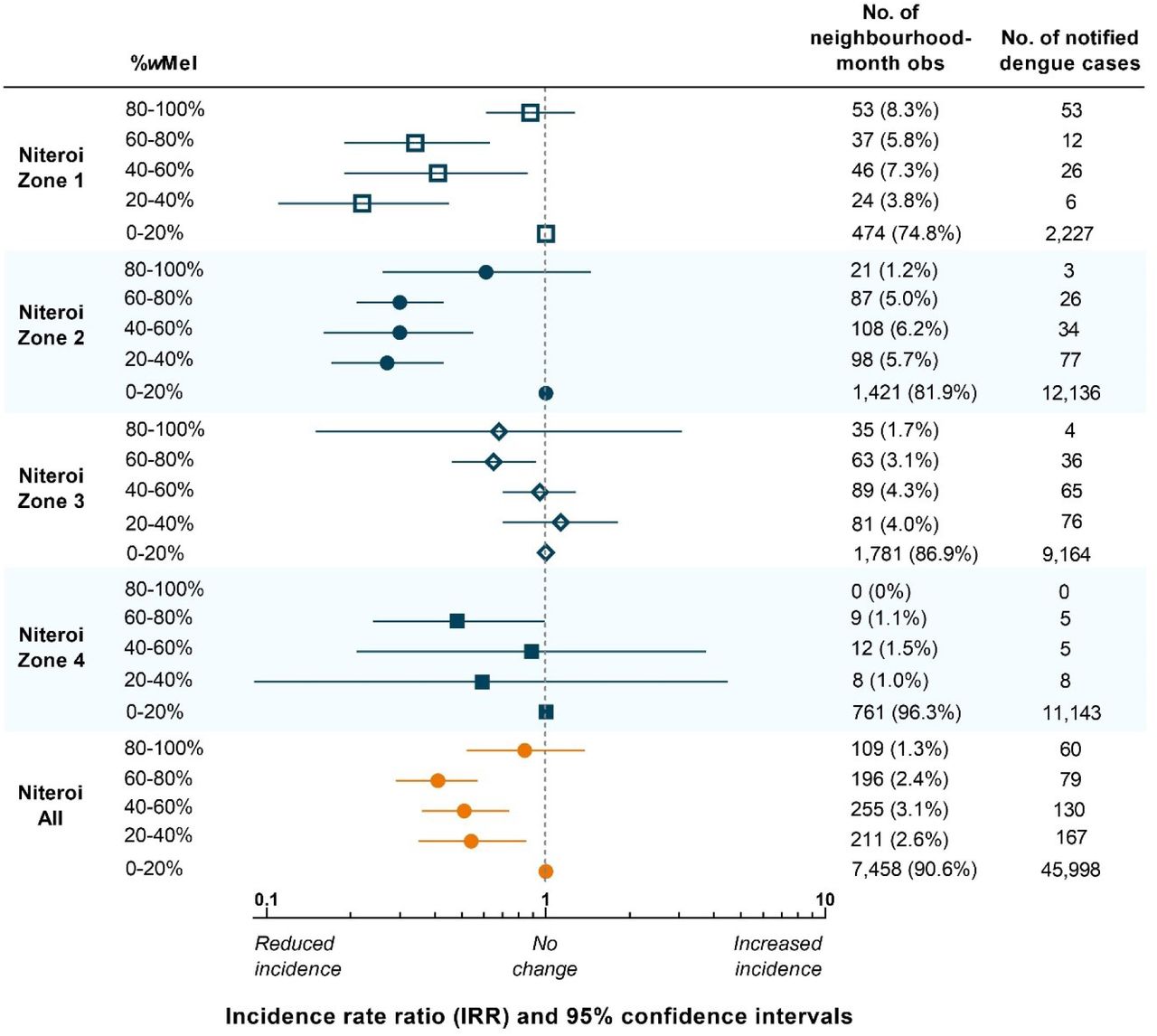
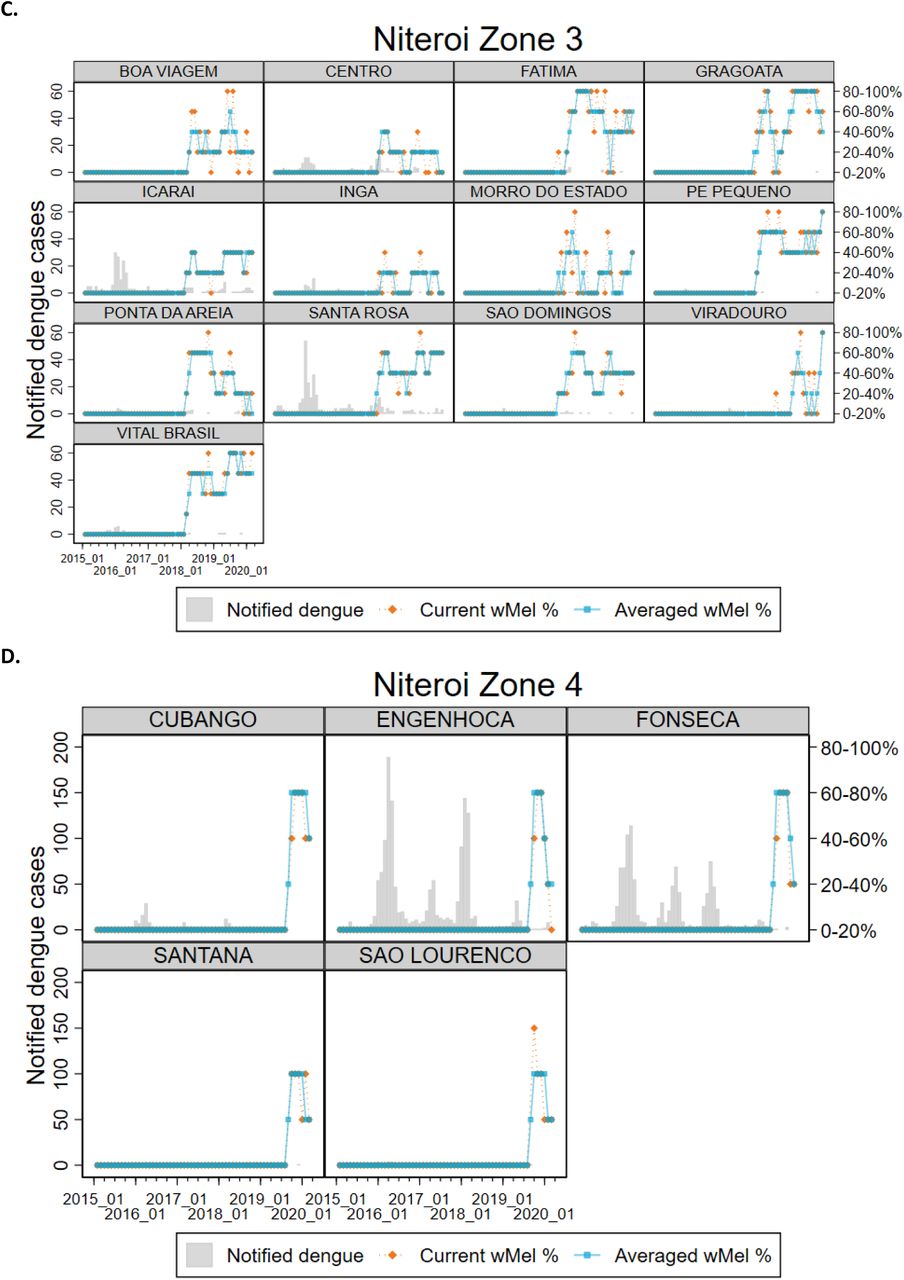
This Wolbachia intervention effect against dengue was also apparent overall, and in each zone, in the neighbourhood-level analysis that considered quintiles of wMel prevalence in local Ae. aegypti populations, although there was no evidence of additional reductions in dengue incidence at higher levels of Wolbachia beyond 20 – 40% wMel prevalence (Supplementary figure 1). There was substantial month-to-month variation in wMel quintiles within neighbourhoods (Supplementary figure 2), which was reduced but not removed by taking a three-month moving average of wMel prevalence. The sensitivity analysis, which used the three-month moving average of wMel prevalence as the exposure measure and excluded Jurujuba and pre-intervention observations prior to 2012, hints at possible greater reduction in dengue incidence at higher levels of Wolbachia, particularly in zone 1 and overall (Supplementary figure 3).

Point estimates (markers) and 95% confidence intervals (horizontal bars) are from controlled interrupted time series analysis of monthly dengue case notifications to the Brazilian national disease surveillance system (Jan 2007 – June 2020), by neighbourhood, in each release zone and in the aggregate release area. wMel prevalence was calculated as the percentage of trapped Ae. aegypti positive for wMel, in each neighbourhood each month, grouped by quintile. The lowest quintile (wMel 0-20%) served as the reference category for calculation of the incidence rate ratio (IRR) and included the monthly observations within that quintile from the respective release zone, as well as all observations from the untreated control zone (n=3,021 neighbourhood-months observed and n=11,278 notified dengue cases).


wMel% quintile was based on the wMel prevalence in a single month (current wMel%) or a three-month moving average (Averaged wMel%).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
This sensitivity analysis uses a three-month moving average of wMel% (instead of a single month) and excludes the Zone 1 pilot release area of Jurujuba and all observations prior to 2012, five years prior to the start of releases. Point estimates (markers) and 95% confidence intervals (horizontal bars) are from controlled interrupted time series analysis of monthly dengue case notifications to the Brazilian national disease surveillance system (Jan 2012 – June 2020), by neighbourhood, in each release zone and in the aggregate release area. wMel prevalence was calculated as the percentage of trapped Ae. aegypti positive for wMel, in each neighbourhood in a moving three-month window, grouped by quintile. The lowest quintile (wMel 0-20%) served as the reference category for calculation of the incidence rate ratio (IRR) and included the observations within that quintile from the respective release zone, as well as all observations from the untreated control zone (n=1,881 neighbourhood-months observed and n=6,996 notified dengue cases).
We found in ITS analysis that chikungunya incidence was also significantly reduced following Wolbachia deployments in Niterói as a whole (59.9% reduction in incidence; 95%CI 21.3, 79.6) and in three of the four individual release zones (Figure 6b).
Discussion
Large-scale phased deployments of wMel strain Wolbachia-infected Aedes aegypti mosquitoes in Niterói, Brazil during 2017 - 2019, resulted in moderate to high levels of wMel establishment in local Ae. aegypti populations by March 2020, when field monitoring was paused due to the emergence of SARS-CoV-2 in Brazil. More than one-quarter of the total 373,000 residents of the intervention area were living in neighbourhoods where local wMel prevalence was 60% or greater by March 2020, predominantly in zones 1 and 2 where releases commenced earliest. In the remaining intervention areas, wMel prevalence was more heterogeneous and a resumption of entomological monitoring is planned in order to evaluate the long-term trajectory of wMel introgression into the local Ae. aegypti population.
Despite this heterogeneity in Wolbachia establishment, a significant reduction in the incidence of both dengue and chikungunya case notifications was observed in Wolbachia-treated areas of Niteroi, compared with a pre-defined untreated control area. This epidemiological impact on dengue was replicated across all four release zones, and in three of the four zones for chikungunya. Aggregate across the whole intervention area, the wMel deployments were associated with a 69% reduction in dengue incidence and a 60% reduction in chikungunya incidence. Given the recognised lack of evidence for efficacy of routinely available approaches to arboviral disease control4 based on elimination of breeding sites and insecticide-based suppression of adult mosquito populations, and considering the magnitude of the historical dengue burden in Niteroi, an intervention effect of this magnitude represents a substantial public health benefit.
Results from a recent cluster randomised trial of wMel-infected Ae aegypti deployments in Yogyakarta Indonesia demonstrated 77% efficacy in preventing virologically confirmed dengue cases,18 with comparable efficacy against all four dengue virus serotypes. Previous non-randomised controlled field trials in Indonesia15 and northern Australia16,17 demonstrated 76% and 96% effectiveness, respectively, in reducing the incidence of dengue cases notified to routine disease surveillance systems. In each of those sites the trajectory of wMel establishment was more rapid and more homogeneous across the release area than observed in Niterói. In the present study, the epidemiological impact in the area of Niterói where wMel introgression occurred most rapidly and homogeneously (Zone 1) was highly comparable with the Indonesian studies: 77% (95%CI 64, 86).
The reasons for slower and more heterogeneous wMel introgression here, compared to Indonesia and Australia, are not fully understood. A likely contributing factor is that these scaled deployments have largely used adult mosquitoes delivered from vehicles, which does not deliver as spatially homogeneous a deployment as the egg-based community-hosted releases that were employed in other sites. Additionally, release areas were complex urban environments with high rise areas, cryptic mosquito breeding sites, and large informal settlements – where field activities were frequently interrupted by security issues – which all likely contributed to slower wMel introgression. Regular monitoring of the wMel-Ae. aegypti broodstock has demonstrated consistently high wMel frequencies (>95%) and insecticide susceptibility profiles comparable with wild-type material, so theoretical concerns of imparied wMel maternal inheritance or increased susceptibility to insecticide are not considered to be contributing factors to the wMel introgression patterns observed in Niterói.
In large and complex urban environments, a homogeneous high level of introgression of wMel may prove operationally challenging and slow to achieve, even with optimised release methods and longer post-release monitoring. This poses the question of what minimum threshold of wMel prevalence is needed to achieve interruption of local arbovirus transmission, and whether a dose-response relationship is observed between wMel prevalence and disease reduction. Predictions from mathematical models have suggested that even in conservative scenarios where scaled Wolbachia deployments only reduced the arboviral transmission potential of the mosquito population by 50%, this could lead to reductions in case incidence of 70%.25 Our findings support this by demonstrating that measurable reductions in both dengue and chikungunya disease accrue even at a moderate prevalence of wMel in local Ae. aegypti populations. A secondary analysis based on measured wMel prevalence and dengue case notifications at the neighbourhood-level found little marginal increase in the wMel intervention effect beyond 20 – 40% prevalence. This analysis also indicated substantial variability in wMel prevalence over time (within neighbourhoods). This may be attributable in part to sampling variability due to small Ae. aegypti catch numbers in some areas but may also indicate true local instability in Wolbachia levels which, combined with people’s mobility outside their neighbourhood of residence, would imply that the measured neighbourhood-level monthly wMel% is an imperfect metric of local residents’ individual wMel exposure and thus their dengue risk.
This study has some limitations. Deployments of wMel-infected Ae. aegypti were not randomised, so there is the potential for measurement of the intervention effect to be confounded by other factors that differ between the release areas and the pre-defined control area. Routine disease surveillance data is imperfect both in specificity (not all notified cases are true dengue/chikungunya cases) and in sensitivity (not all dengue/chikungunya cases are notified). However the risk of these factors influencing the measurement of the epidemiological endpoint here is reduced by the inclusion of a parallel control with a historical dengue time series that is highly synchronous with each of the release areas for ten years pre-intervention. The replication of the intervention effect in each of the four release zones also mitigates the possibility that any parallel change in vector control practices or healthcare seeking behaviour in intervention areas could have confounded the observed result.
We have demonstrated that wMel introgression can be achieved across a large and complex urban environment over a period of three years to a prevalence in local Ae. aegypti which, while still heterogeneous, is sufficient to interrupt arbovirus transmission and result in a measurable reduction in both dengue and chikungunya case incidence. Ongoing entomological and epidemiological monitoring will provide additional information on the trajectory of wMel establishment in areas where releases have occurred more recently, or introgression has been slower, and on the full magnitude and durability of the public health benefit.
Data Availability
The data underlying the results presented in this study are publicly available at 10.6084/m9.figshare.13662203 (zone-level data) and 10.6084/m9.figshare.13662230 (neighbourhood-level data).
Acknowledgments
The authors acknowledge the municipality of Niterói for their partnership and logistical support for this study.
References



