
Abstract
Background Management of COVID-19 in transplant patients is a big challenge. Data on immunosuppression management, clinical picture, and outcomes are lacking.
Objectives To summarize the current literature on COVID-19 in transplant patients especially the data regarding the immunosuppression protocols, clinical presentation, and outcomes.
Search strategy A systematic search of MEDLINE, EBSCO, CENTRAL, CINAHL, LitCovid, Web of Science, and Scopus electronic databases. The references of the relevant studies were also searched. The search was last updated on June 3, 2020.
Selection Criteria Primary reports of solid organ transplant patients who developed COVID-19. An overlap of cases in different reports was checked.
Data collection and analysis A descriptive summary of immunosuppression therapy (before and after COVID-19), clinical presentation (symptoms, imaging, laboratory, and disease severity), management (oxygen therapy, antiviral, and antibacterial), major outcomes (Intensive care admission, invasive mechanical ventilation, acute kidney injury), and mortality.
Main results We identified 74 studies reporting 823 cases of solid organ transplantation with COVID-19. Among 372 patients, 114 (30.6%) were mild COVID-19, 101 (27.2%) moderate, and 157 (42.2%) severe or critical.
Major outcomes included intensive care unit admission, invasive ventilation, and acute kidney injury, which occurred in 121 (14.7%), 97 (11.8%), and 63 (7.7%) of patients, respectively. Mortality was reported in 160 (19.4%) patients. Missing individual data hindered making clinical correlations.
Conclusion COVID-19 in solid organ transplant patients probably has a more disease severity, worse major outcomes (Intensive care admission, invasive ventilation, acute kidney injury), and higher mortality than in non-transplant patients.
Introduction
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) causes the clinical syndrome called COVID-19. Infections in organ transplant patients are of special concern due to lifelong immunosuppression, common comorbidities, and the effects of some immune suppressants (diabetogenesis, neutrocytopenia, or lymphopenia).1 Reports are controversial regarding the clinical presentation and outcomes in those patients in comparison to the general population.
The ideal management of immunosuppressive therapy during COVID-19 in transplant patients is unclear. The balance between the increased risk of infections and graft rejection is vital. Theoretically, immunosuppression may reduce the cytokine storm syndrome - a major pathology in COVID-19 - and calcineurin inhibitors (CNI) reduce in vitro viral replication.2
The lack of data in the time of the COVID-19 pandemic pushed us to systemically review and summarize the available knowledge of COVID-19 in transplant patients, especially as regards the immunosuppressive management, clinical presentation, and major outcomes (admission to Intensive Care Unit (ICU), invasive mechanical ventilation (MV), acute kidney injury (AKI)), and mortality.
Material and Methods
This review followed the Arksey and O’Malley framework for scoping reviews and the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) – extension for scoping review.3,4
I- Identifying research questions
Our main research questions were: (1) What is the common immunosuppressive protocol in transplant patients with COVID-19?; (2) What is the clinical presentation and disease severity in transplant patients with COVID-19?; (3) What are the major outcomes including the incidence of ICU admission, Invasive MV, AKI, and mortality?
II- Identifying relevant studies
A systematic search in MEDLINE, EBSCO, CENTRAL, CINAHL, LitCovid, Web of Science, and Scopus electronic databases was conducted with no language restrictions. The search was last updated on June 3, 2020.
We searched the list of references for the selected study and contacted authors of published reports for additional information. The detailed search strategy is supplemented in the file (S1).
III- Study selection
Two authors (MME and MEs) independently screened the titles and abstracts of the primary search results, then reviewed the full relevant articles. We included any article reporting original research on organ transplant patients with COVID-19.
The diagnosis of COVID-19 was considered either by clinical, radiological, or reverse-transcription polymerase chain reaction (rt-PCR). We reported case severity as reported in the primary studies.
If MME and MEs could not agree on the inclusion of any study, a third reviewer’s opinion (AY or AN) was asked.
IV- Data charting
A data-charting electronic sheet was developed by MME and revised by all authors. Two authors (MEs and HN) independently extracted data and (MEm and MA) continuously updated the datasheet. Then, the data was collated by MME.
We extracted the following data: (1) General data (title, year of publication, authors, and country); (2) Methodological data (study design, sample, and patient characteristics - e.g. age, the transplanted organ, from living or deceased donor, duration since transplantation); (3) Immunosuppressive therapy (before and after COVID-19); (4) Clinical data (clinical presentation, imaging, laboratory investigations, and disease severity); (5) Management including (oxygen therapy, antiviral, antibacterial, mechanical ventilation); (6) Outcomes (ICU admission, Invasive MV, AKI, mortality).
This scoping review did not include a critical appraisal of the primary studies.
V- Summarizing results
We organized our results in categories: immunosuppression, the clinical presentation including severity, and major outcomes. We presented the results as number (%) based on the available data.
Results
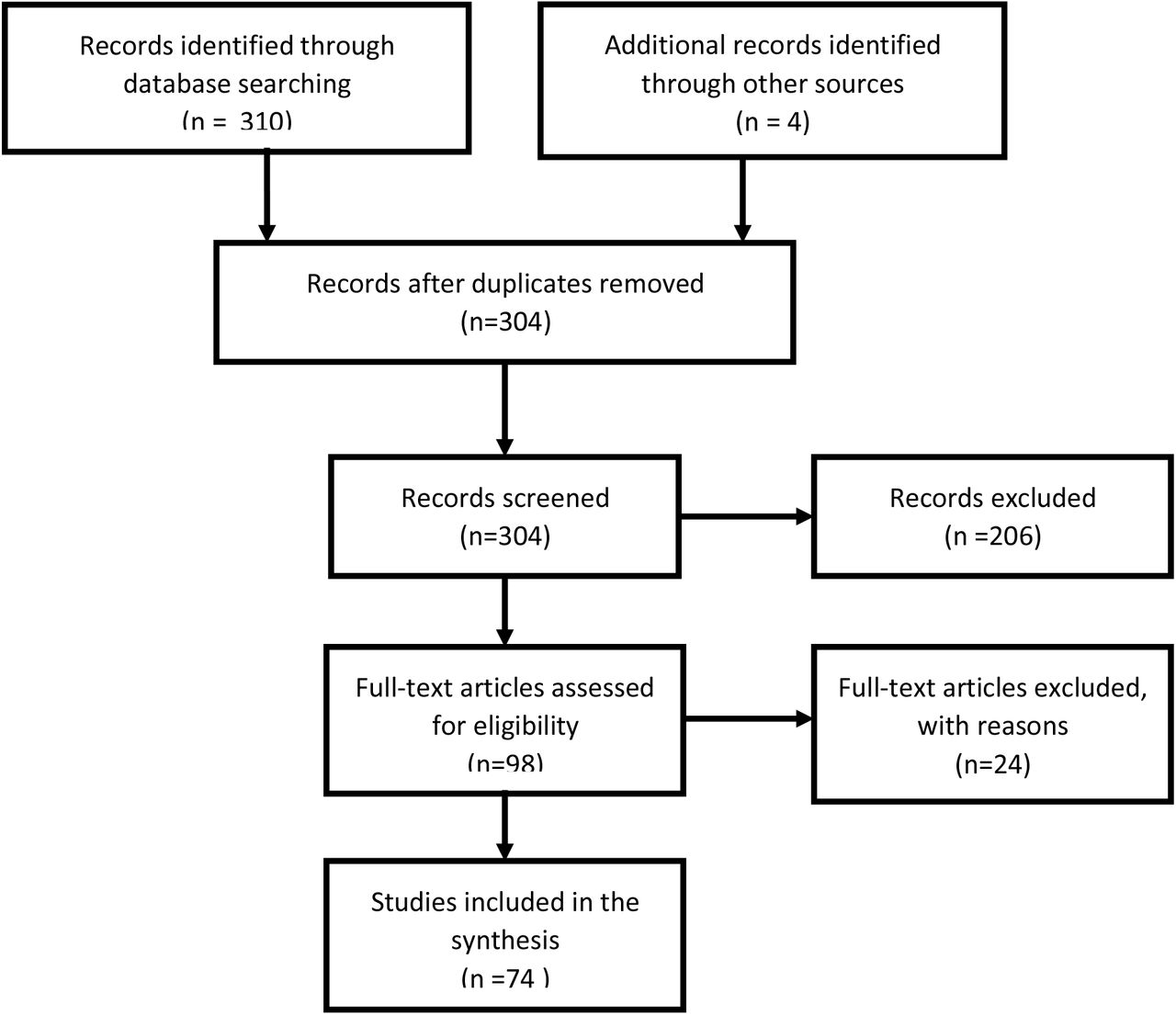
We identified 74 primary studies reporting 823 organ transplant cases who developed COVID-19 after organ transplantation. (Figure 1) charts the process of studies’ inclusion.

Study flowchart
These reports included 617 kidney, 98 liver, 59 heart, 31 lung, 17 combined-organ transplants, and 1 pancreas.
We tabled the studies according to the study design, country, and the number of cases (Table 1).5-78
Demographic data
Adult patients’ age ranged from 19-81 years. Seven pediatric patients – aged 6 months, 3 years, 4.5 years, 13 years, and 3 with unavailable age data – were also reported.
According to the available data, 554 (68.4%) male and 256 (31.6%) female patients, and 208 (75.6%) deceased-donor and 67 (24.4%) living-donor transplantation were reported.
Twenty-six cases developed COVID-19 within 1 year after transplantation (including 13 cases in the 1st 3 months) and 111 cases after 1 year. Time since transplantation was not mentioned or detailed in 686 cases.
Immunosuppression
Baseline immunosuppression could be only identified in 524 cases. Calcineurin inhibitors (CNI) were given in 463 cases (88.4%), mycophenolate mofetil (MMF) in 358 (68.3%), steroids in 313 (59.7%), mammalian target of rapamycin inhibitors (mTORi) in 40 (7.6%), and others (azathioprine, belatacept, or basiliximab) in about 6.3% of patients.
In response to COVID-19, immunosuppressive management differs between reports. CNI was reduced in 168 cases, discontinued in 91, maintained in 60, while newly started in 4 patients. MMF was discontinued in 203 cases, reduced in 34 cases, maintained in 21 cases, and started in 1 after COVID-19.
Patients started new steroids in 143 cases, continued or increased the dose of steroids in 104, discontinued in 8, and reduced the dose in 5. Adding or increasing the dose of steroids may be as a replacement of other immunosuppressants or as a treatment option of Acute Respiratory Distress Syndrome (ARDS). mTORi was discontinued in 14 patients, continued in 2, and reduced in one patient. (Table 2) summarizes the immunosuppressive management in COVID-19 transplant cases.
Thirty-five cases reported no immunosuppressive changes, and 36 cases reported a reduction of immunosuppression without details. Three-hundred and fifteen cases did not report immunosuppressive management after COVID-19.
Clinical presentation, diagnosis, and case severity
The most common symptoms were fever (n= 577, 70%), cough (n= 520, 63%), dyspnea (n= 277, 33.7%), diarrhea (n= 153, 18.6%), myalgia (n= 105, 12.7%), and fatigue (n= 104, 12.6%). While, anorexia, loss of smell or taste, sore throat, nausea, and nasal congestion were infrequent (6.8%, collectively).
SARS-CoV-2 was confirmed with rt-PCR in 300 cases (36.5%). Chest x-ray and computed tomography (CT) scans showed abnormalities at the time of presentation in 255 (31%) and 97 (11.8%), respectively. Radiological findings were variable (bilateral or unilateral) in the form of ground-glass opacity, interstitial thickening, or infiltration. Lung ultrasound was available only in one case that showed progressive thick and confluent B lines, which improved with patient improvement.9 Sixty patients and twelve cases showed no abnormalities in chest x-ray and CT scans, respectively, at the time of presentation.
Laboratory results showed lymphopenia in 398/442 cases (90%), elevated C-reactive protein 213/302 (70.5%), elevated D-dimer 104/191 (54.5%), elevated ferritin 93/173 (53.8%), elevated troponin 71/132 (53.8%), elevated lactate dehydrogenase (LDH) 48/95 (50.5%), and elevated liver enzymes 25/158 (15.8%).
Among 372 patients, 114 (30.6%) were mild COVID-19, 101 (27.1%) moderate, and 157 (42.2%) severe or critical.
(Table 3) shows the distribution of case severity according to the transplanted organ.
Treatment
Four-hundred and sixty-nine patients (57%) received chloroquine or hydroxychloroquine, 170 (20.7%) ritonavir/lopinavir, 15 (1.8%) oseltamivir. Fifty-two (6.3%) patients received no antiviral therapy.
Two-hundred and eleven (25.6%) patients received prophylactic antibiotics, including 88 (10.7%) who received azithromycin – alone or in-combination with hydroxychloroquine.
Seventy-one patients received tocilizumab and 6 received leronlimab.
Oxygen therapy was reported in 212 patients (53 nasal cannulas, 20 non-invasive ventilation (NIV), 13 high-flow nasal cannula, and 126 non-specified) and 46 cases reported no oxygen therapy.
Outcomes
One-hundred and twenty-one (14.7%) cases required ICU admission and 97 (11.8%) were mechanically ventilated.
Acute kidney injury (AKI) developed in 63 (7.7%) of cases. Twenty-two (35%) were kidney, 14 (22.2%) liver, 14 (22.2%) heart, 1 lung, and 12 non-specified organ transplant.
De novo dialysis started in 29 (3.5%) cases (14 kidney, 5 heart, 1 lung, and 9 non-specified organ transplant patients) and extracorporeal membrane oxygenation (ECMO) in 3 patients.
Mortality was reported in 160 (19.4%) of cases. None of the 7 pediatric patients in our cohort died. Of those 160 patients, 104 were kidney-transplant patients, 20 liver, 9 heart, 1 lung, and 26 non-specified organ-transplant patients.
Discussion
The present scoping review identified 74 studies reporting 823 cases of COVID-19 infection in solid organ transplantation recipients. The common immunosuppressive practice was the dose reduction of CNI (52%), discontinuation of CNI (27.7%), discontinuation of MMF (78.7 %), discontinuation of mTORi (82.4%), and continuation (40%) or commencing (55%) steroids. Of 372 cases, COVID-19 was mild in 114 (30.6%) patients, moderate in 101 (27.1%), and severe or critical in 157 (42.2%). We found 121 (14.7%) ICU admissions, 97 invasive mechanical ventilation, and 63 (7.7%) with AKI. Mortality was reported in 160/823 (19.4%) of cases.
The variations in immunosuppressive therapy after COVID-19 reflect the theoretical controversies. Due to their immunosuppressed state, organ transplant recipients may be at higher risk for both being infected with SARS-CoV-2 and severe forms of COVID-19. On the other hand, immune suppression may ameliorate the cytokine surge, which is responsible for the systemic hyperinflammatory manifestations of COVID-19, including ARDS, multiorgan dysfunction syndrome, shock79, and the secondary hemophagocytic lymphohistiocytosis syndrome.80 Furthermore, immunosuppression reduction may cause graft rejection and immune constitution reaction causing paradoxical disease worsening.80 There are no solid recommendations regarding immunosuppressive protocol in transplant patients with COVID-19. There is even a recommendation against the routine reduction of CNIs.79
Generally, immunosuppressed patients present with atypical or attenuated signs and symptoms of infection, often leading to late presentations, worse outcomes, and prolonged virus shedding and infectivity.24
Table 4 presents the common presentations of those patients versus non-transplant COVID-19 patients.81 Diarrhea was more frequent in transplant patients with COVID-19 (18.6% versus 3.8%); however, some reports showed a higher incidence of diarrhea in COVID-19 non-transplant cases.82 In a report of 90 organ transplant recipients, the incidence of diarrhea was even higher (31%).48 This may be attributed to MMF, which causes diarrhea.83 Diarrhea may be also associated with COVID-19 severity and the need for MV.81 Fatigue was less common in the transplant population (12.6% vs 38%). Dyspnea is the third common in both groups with a greater presence in transplant, 33.7 % vs 18.7% in non-transplant patients. In Covid-19 patients, dyspnea upon presentation is associated with a severe clinical course.48 This may be a marker of pulmonary disease severity in transplant recipients.
Among 442 available laboratory results, 90% of transplant patients showed lymphopenia vs 83.2% in the non-transplant population.81 Lymphopenia is associated with more ARDS, ICU admission, higher troponin, and more myocardial injury, and death.84
According to our findings, elevated CRP, D-dimer, ferritin, troponin, and LDH were higher in transplant patients when compared with the general population.81 Elevation of some or all of these parameters is associated with a severe COVID-19 course and a more unfavorable outcome. 48,81
Unfortunately, among our 823 cases, we could identify the disease severity of only 372 patients. Classification of severity was different between reports; some classified cases as mild, moderate, and critical, while others classified cases as mild, moderate, and severe.5,48 Therefore, we collected severe and critical cases in the same category as severe or critical illness. In our review, 42.2 % of reported patients were severe or critical, which is significantly higher when compared with the general population (15.7%).81 In a large non-transplant Chinese cohort, severe cases represented 14% and critical cases represented 5%.85 This copes with that immunosuppressed transplant recipients are at a higher risk for severe COVID-19 course.79
In a case-control study, one transplant patient died and transplant patients showed more severe course than non-transplant patients. The length of hospital stay and the duration of virus shedding (positive PCR) were longer in transplant cases. Therefore, transplant patients with COVID-19 might take a longer time to recover and remain infective for a longer duration.5
Nine (64.3%) of our 14 lung transplant patients were classified as severe or critical. Despite being a small cohort, being primarily a respiratory disease, COVID-19 may be more severe among lung transplant recipients.
Compared to non-transplant patients81, ICU admission was needed in 121 (14.7% versus 5%), invasive mechanical ventilation in 97 transplant cases (11.8% versus 2.3%),, and mortality in 160 (19.4% versus 1.4%) of cases.
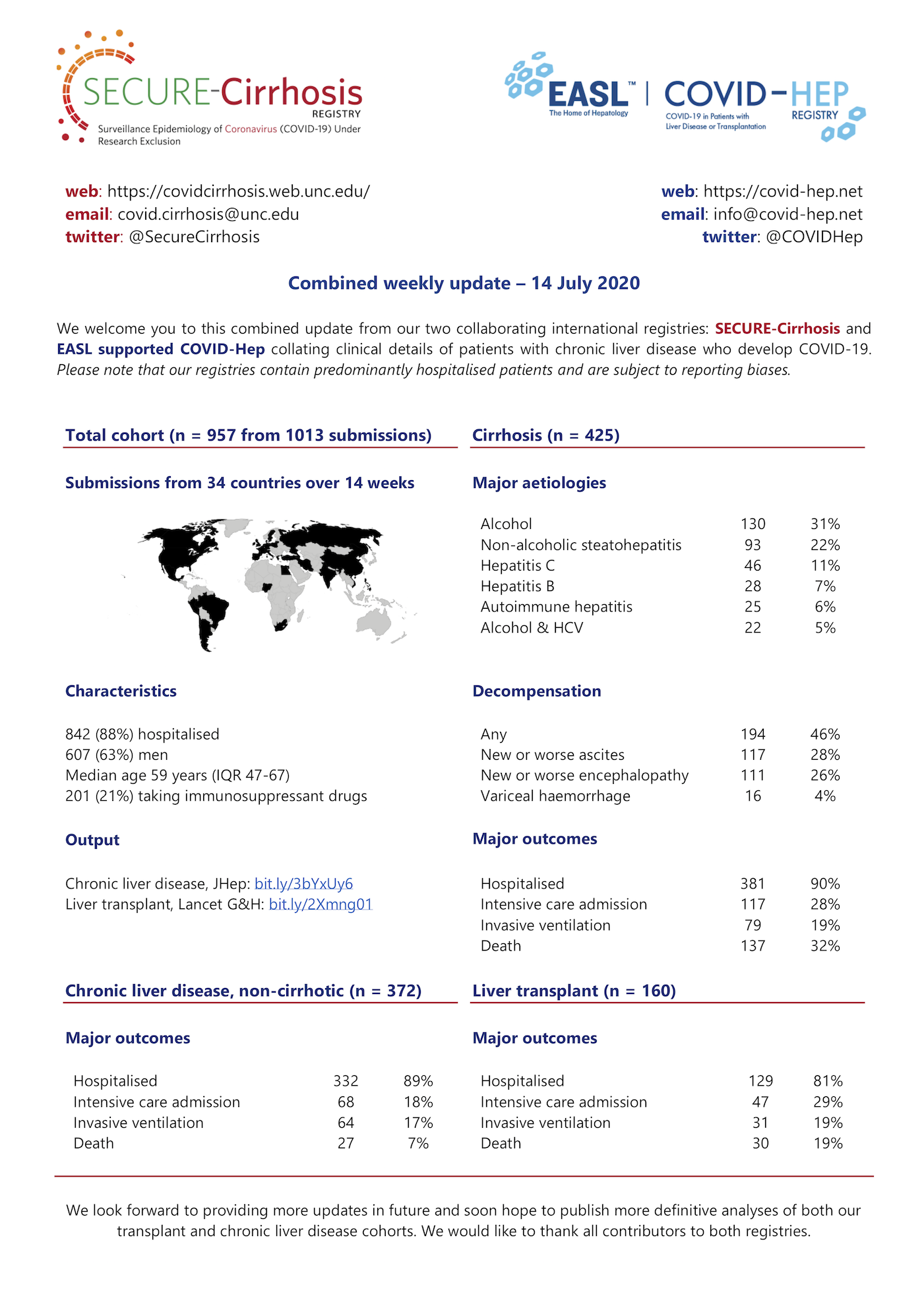
On July 14, 2020, the combined SECURE-Cirrhosis and COVID-HEP registries reported ICU admission in 47/160 (29.4%), invasive ventilation in 31/160 (19.4%), and mortality in 30/160 (18.8%) in liver transplant recipients.86 Along with our results, these findings support more illness severity and fatality among transplant recipients with COVID-19.
Acute kidney injury (AKI) developed in 63 (7.7%) of cases including 29 patients who needed de novo dialysis. While AKI developed only in 0.5% of COVID-19 as found by Guan et al.81 This may be due to the more severe course of COVID-19 in transplant recipients, nephrotoxicity of some immune suppressants, and chronic rejection process in kidney transplant patients.
Forty-six hospitalized patients did not receive oxygen therapy and some reported no hospitalization for mild cases with favorable outcomes.48 Therefore, transplant patients with SARS-CoV-2 can be managed safely in the outpatient settings. This decision should be taken case-by-case keeping in mind the comorbidities and ability of rapid transfer to a transplant center in case of deterioration.87
Chloroquine, hydroxychloroquine, and various antiviral therapies were commonly used despite the lack of evidence and the known interactions with CNI.87
We had some limitations in our scoping review. This report only included case-reports, case series, and one case-control study; however, this was the best available data. Missed individual data and the aggregate data from the case series hindered us from extracting proper associations between case severity, immunosuppression protocol, and major outcomes. Our reporting was only up to the date of June 3, 2020. We did not include a critical appraisal of the primary reports. Patient duplication should be minimal as we traced cases carefully and contacted authors for primary source overlap.
In conclusion, our results suggest that COVID-19 in transplant patients has a more severe course, worse major outcomes (ICU admission, Invasive MV, AKI), and higher mortality than non-transplant patients.
Data Availability
Data will be available on request.
Supporting information statement
Additional supporting information may be found online in the Supporting Information Section at the end of the article.
Footnotes
Authorship: 1. Moataz Maher Emara (MME): performed the electronic serach on the databases, screened for the relevant studies, created the data charting file, continuously updated the search results, collated the data from the all data collectors, and wrote the primary manuscript.
2. Mahmoud Elsedeiq (MEs): screened for the relevant studies, independently collected data from the selected studies, approved and revised the final manuscript.
3. Mohamed Elmorshedi (MEm): continuously updated the data collection from the continuously added studies, helped in writing the manuscript, approved and revised the final manuscript.
4. Hamed Neamatallah (HN): screened for the relevant studies, independently collected data from the selected studies, approved and revised the final manuscript.
5. Mostafa Abdelkhalek (MA): continuously updated the data collection from the continuously added studies, approved and revised the final manuscript.
6. Amr Yassen (AY): guided the search and writing of the manuscript.
7. Ashraf Nabhan (AN): guided the search and writing of the manuscript.
All authors participated conceptually in the study, revised, and accepted the final manuscript.
Disclosure and funding: The authors declare no conflicts of interest and did not receive any financial support.
Abbreviations
- AKI
- Acute Kidney Injury
- ARDS
- Acute Respiratory Distress Syndrome
- CNI
- Calcineurine inhibitor
- CRP
- C-reactive protein
- CT
- Computed Tomography
- ECMO
- Extracorporeal Membrane Oxygenation
- ICU
- Intensive Care Unit
- LDH
- Lactate Dehydrogenase
- mTORi
- mammalian Target Organ of Rapamycin inhibitor
- MV
- Mechanical Ventilation
- MMF
- Mycophenolate Mofetil
- PRISMA
- Preferred Reporting Items for Systematic Review and Meta-Analysis
- rt-PCR
- reverse transcription – Polymerase Chain Reaction
- SARS-CoV-2
- severe acute respiratory syndrome – coronavirus-2




{kind=link}
{kind=link}