
Abstract
Over the past decades, the possibility of using non-invasive brain stimulation (NIBS) to treat mental disorders received considerable attention. To date, no recommendation is available for anxiety disorders, suggesting that evidence is still limited. Here, we systematically revised the existing literature, and quantitively analyzed the effectiveness of transcranial magnetic stimulation and transcranial direct current stimulation in anxiety disorders treatment.
Following PRISMA guidelines, three electronic databases were screened to the end of February 2020 to select English-written peer-reviewed articles, including a clinical anxiety sample, a NIBS technique, and a control condition. Overall, ten papers met the inclusion criteria.
TheHedge g for scores at the specific and generic anxiety questionnaires before and after the treatment was computed as effect size and analyzed in two independent random-effects meta-analyses. Moreover, considering the well-known comorbidity between anxiety and depression, a third meta-analysis was run, analyzing depression scores’ outcomes. Albeit preliminary, our findings highlighted that real stimulation significantly reduced anxiety and depression scores compared to the control condition, suggesting that NIBS can alleviate clinical symptoms.
Introduction
Anxiety disorders are the most prevalent class of mental disorders in most western societies (James et al., 2018; Wittchen et al., 2011) and are one of the foremost cause of disability (GBD 2015 Risk Factors Collaborators, 2016; see Craske et al., 2017 for epidemiologic details). The onset of anxiety disorders typically occurs within young adulthood (see Lijster et al., 2017 for a recent meta-analysis). It seems to take a chronic course, with differences in stability rates varying across studies and specific diagnosis (Beesdo, Knappe, & Pine, 2009).
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM), Fifth Edition (American Psychiatric Association, 2013), the anxiety disorders category includes specific phobia, social anxiety disorder, panic disorder, agoraphobia, and generalized anxiety disorder1. DSM-5 anxiety diagnostic criteria are similar to those included by the other standard classification system, namely the International Classification of Diseases, Tenth Edition, or ICD-10 (World Health Organization, 1993). Across the two systems, anxiety disorders are a spectrum of multidimensional phenotypes (Schmidt, Khalid, Loukas, & Tubbs, 2018), that share clinical features, such as excessive and stable anxiety, physiological symptoms, such tachycardia, and chest tightness, typical behavioral responses, such as avoiding perceived threats, places or situations, thus impairing individuals’ psychological well-being and quality of life.
The neurobiology of anxiety disorders is far from being clarified. Indeed, studies have been conducted over small participant samples, with heterogeneous imaging methods, paradigms, and patients’ comorbidities (e.g. Bas-Hoogendam et al., 2020).
Despite disease-specific differences, converging evidence suggests that anxiety disorders are characterized by structural and functional alterations, primarily involving a meso cortico limbic pathway (see for a review Duval et al., 2015). According to this neurobiological account, the amygdala, the prefrontal cortex (PFC), the anterior cingulate cortex (ACC), the hippocampus, and their functional connections, might play a key role in generating and regulating fear, anxiety, and threat detection (see for revisions Craske et al., 2017; Schmidt et al., 2018). Amygdala hyperactivity is one of the most consistent findings (Holzschneider & Mulert, 2011; Taylor & Whalen, 2015). This abnormal activity has been reported across several specific diseases and tasks, such as anxiety-provoking public speaking (Furmark et al., 2004; Lorberbaum et al., 2004; Tillfors et al., 2001), fear-conditioning (Schneider et al., 1999), or emotional images/threatening faces presentation tasks in social phobia or generalized social anxiety disorder (Labuschagne et al., 2010; Shah, Klumpp, Angstadt, Nathan, & Phan, 2009). Moreover, amygdala activation positively correlated with symptoms’ severity (Ball et al., 2012; Lipka, Miltner, & Straube, 2011) and decreased after medication and psychotherapy interventions (Gingnell et al., 2016; Lipka et al., 2011; Månsson et al., 2013; Phan et al., 2013). Amygdala response to threat is regulated through bidirectional connections to the ACC and vmPFC in animals and humans (see Maren & Holmes, 2016 for a review; Maroun, Kavushansky, Holmes, Wellman, & Motanis, 2012). In line with this finding, human neuroimaging studies highlighted PFC hypoactivity in anxious patients, suggesting that amygdala hyperactivity might be due to a decrease in the top-down inhibitory control exerted by the prefrontal cortex (Etkin & Wager, 2007; Ironside et al., 2019; Kim et al., 2011; Motzkin et al., 2015; but see Kraus et al., 2018 for different results). Considering functional abnormalities in anxiety disorders, it has been suggested that an inter-hemispheric imbalance might be at the basis of the disease, involving a hypoactivation of the left dorsolateral prefrontal cortex (DLPFC) and a hyperactivation of the right DLPFC (Nitschke & Heller, 2005; Prasko et al., 2004; Vicario, Salehinejad, Felmingham, Martino, & Nitsche, 2018).
Anxiety first-line treatments comprise pharmacological or psychotherapeutic interventions, with Cognitive-Behavioral therapy considered as the most effective treatment according to several international guidelines (Bandelow, Lichte, Rudolf, Wiltink, & Beutel, 2015; Katzman et al., 2014; NICE, 2014). However, a consistent number of patients do not respond to traditional treatment or go through relapse and recurrence of their symptoms (Fernandez, Salem, Swift, & Ramtahal, 2015; S. Taylor, Abramowitz, & McKay, 2012).
In the search for alternative treatments, in the last thirty years, the use of non-invasive brain stimulation (NIBS) has rapidly grown both as a stand-alone therapy or combined with cognitive interventions (Andre R Brunoni et al., 2019; Sathappan, Luber, & Lisanby, 2019; Wessel, Zimerman, & Hummel, 2015). NIBS’ rationale in psychiatric treatment is the possibility of re-balancing maladaptive activity and functional connectivity between brain structures, which can be altered in these disorders. Indeed, there is a consensus that aside genetic, hormonal, social, and cognitive factors, psychiatric disorders involve also pathologically altered neural plasticity, which can be modulated through NIBS with biochemical effects that outlast the time of stimulation (Nitsche, Müller-Dahlhaus, Paulus, & Ziemann, 2012) see for recent reviews (Kronberg, Bridi, Abel, Bikson, & Parra, 2017; Ziemann, 2017). Although their precise action mechanisms are still under investigation, NIBS effects on synaptic plasticity involve several phenomena ultimately leading to long-term potentiation (LTP) – or synaptic strengthening – and long-term depression (LTD) – or synaptic weakening – processes (Reis et al., 2008), for a review and discussion see Cirillo and colleagues (Cirillo et al., 2017).
Among NIBS techniques, the two most used methods are transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS). TMS is a technique based on delivering a strong, short magnetic pulse to the participants’ head, inducing neuronal firing by suprathreshold neuronal membrane depolarization (e.g., Kobayashi & Pascual-Leone, 2003). When used to generate long-term effects, TMS is typically applied using repetitive (rTMS) protocols, with inhibitory (≤1 Hz and continuous theta burst stimulation, cTBS), or excitatory (higher than 5 Hz and intermittent theta burst stimulation, iTBS) protocols (e.g., Fregni & Pascual-Leone, 2007). In turn, tDCS is a neuromodulatory technique in which weak constant direct current (typically 1-2 mA) is delivered through the scalp using two electrodes, one with positive (anode) and the other with negative (cathode) polarity (Nitsche & Paulus, 2000). tDCS does not generate action potentials per se but induces small changes at the membrane potential level, thus influencing spike frequency and, in turn, cortical excitability (Brunoni et al., 2012; Purpura & McMurtry, 1965). TDCS effects are polarity-dependent, with anodal stimulation depolarizing neuronal membrane and cathodal hyperpolarizing it, increasing and decreasing cortical excitability, respectively (e.g., Nitsche et al., 2008). Usually, among the NIBS parameters, the stimulation frequency for TMS (either high or low) and the polarity for tDCS (either anodal or cathodal) are considered the determinants for an expected effect in cortical excitability and behavior: excitatory-enhancing effect or inhibitory-disrupting effect. Although a detailed discussion of the two techniques goes beyond this meta-analysis scope, it seems crucial to highlight that such expectation can be misleading. Indeed, the NIBS outcome - in terms of both cortical excitability and behavioral modulation - can’t be clearly determined in advance, but is the result of more complex interactions involving stimulation parameters (intensity, orientation), cerebral regions and their connections, individual anatomical features, and state dependency (Castrillon et al., 2020; López-Alonso, Cheeran, Río-Rodríguez, & Fernández-del-Olmo, 2014; Pell, Roth, & Zangen, 2011; Pisoni et al., 2017).
Among psychiatric disorders, the main fields of application of NIBS as an alternative treatment is the major depression disorder (MDD). rTMS clinical use to treat MDD has been approved by the Food and Drug Administration in 2008 using high-frequency (10 Hz) left-side dorsolateral prefrontal cortex stimulation, and in 2018 applying iTBS protocols over the same region (Hui, Tremblay, & Daskalakis, 2019). The effectiveness of rTMS and tDCS in other psychiatric disorders has been explored by several reviews and meta-analyses, targeting schizophrenia (Kennedy, Lee, & Frangou, 2018; Kostova, Cecere, Thut, & Uhlhaas, 2020), substance abuse (Trojak et al., 2017), and obsessive-compulsive disorders (Brunelin et al., 2018; Trevizol et al., 2016), highlighting promising yet preliminary results.
Aiming at providing shared recommendations for good practice, periodically revised guidelines of independent expert panels review and analyze studies investigating rTMS (Lefaucheur et al., 2020, 2014) and tDCS (Fregni et al., 2020; Lefaucheur et al., 2017) protocols applied to a broad spectrum of neurological and psychiatric disorders. According to the guidelines’ classification, Level A (“definitely effective or ineffective”) indicates that evidence is sufficient (in terms of number and studies quality) to establish whether a specific protocol applied over a certain region can be useful or not in a particular disorder. Only few protocols reached level A of efficacy. Specifically, for TMS Level A effectiveness is attributed to i) high frequency rTMS applied to the left DLPFC to treat depression; ii) high frequency TMS to the primary motor cortex (M1) contralateral to the painful side for neuropathic pain; iii) low-frequency rTMS applied over the contralesional M1 for hand motor recovery in the post-acute stage of stroke (Lefaucheur et al., 2020). Concerning tDCS, level A effectiveness is attributed only to anodal stimulation over the left DLPFC in depression (Fregni et al., 2020), while anodal tDCS over the ipsilesional primary motor cortex is considered definitely not effective for enhancing robotic therapy in the motor rehabilitation in subacute stroke. Critically, to date, no recommendation has been made for the use of rTMS or tDCS in anxiety disorders treatment. Indeed, the available data are not sufficient to make recommendations to its use or a claim for an absence of an effect (Fregni et al., 2020; Lefaucheur et al., 2020).
Trying to fill the gap in the literature, in the last few years, several reviews examined the available literature concerning the therapeutic effects of rTMS and tDCS in anxiety disorders treatment (Iannone, Cruz, Brasil-Neto, & Boechat-Barros, 2016; Vicario et al., 2018), anxiety symptoms arising from other pathologies (Rodrigues et al., 2019), and specific anxiety disorders (e.g., generalized anxiety disorder, Sagliano, Atripaldi, De Vita, D’Olimpio, & Trojano, 2019). These works testified the general interest around this topic and showed promising yet preliminary results. However, so far, previous reviews also included single-case studies and protocols without a control condition, thus providing an overview of the literature state-of-the-art, but without cumulatively quantifying the results.
To our knowledge, three previous meta-analyses (Cirillo et al., 2019; Cui et al., 2019; Trevizol et al., 2016) investigated rTMS efficacy from a quantitative perspective. Specifically, Cui and colleagues investigated rTMS efficacy in treating GAD. The meta-analysis included 21 studies (2 English-written and 19 Chinese), with the inclusion criteria of a control group receiving sham rTMS or no intervention, suggesting rTMS as a useful option in decreasing GAD anxiety symptoms. The review and meta-analysis by Trevizol et al. (2016) investigated rTMS efficacy in randomized clinical trials addressing anxiety disorders. This work included 14 papers; however, five works addressed post-traumatic stress disorder and eight obsessive-compulsive disorders, which are now considered as independent diagnostic categories (APA, 2013). The authors concluded that real TMS was not superior to the sham condition in reducing anxiety symptoms. In line with the previous study, Cirillo and colleagues (2019) systematically reviewed and analyzed anxiety and posttraumatic stress disorders (PTSD), including 17 papers: nine concerning PTSD, two specific phobia, two panic disorder and four addressing GAD. Authors then run two independent meta-analyses, one concerning PTSD and the second including GAD. Authors considered the mean difference of sham vs. real TMS in pre and post treatment scores when the two conditions were available, only pre-post scores mean difference when sham stimulation was not tested. Results showed a large treatment efficacy for both disorders.
To our knowledge, no previous meta-analyses combined TMS and tDCS in investigating NIBS effectiveness in treating anxiety disorders. Moreover, some of the previous works included research not involving a control group or considering disorders that are now considered as separated nosological entities. Therefore, the present work aims to qualitatively visualize and quantitatively evaluate the effect induced by ether rTMS and tDCS protocols in anxiety disorders, trying to overcome the limitation of individual studies which have been typically conducted on small sample sizes and applying heterogeneous stimulation parameters and sessions number (e.g., Vicario et al., 2019).
Since a similar neurobiological pattern of imbalance of cortical excitability between right and left DLPFC has been reported in major depression disorder (Grimm et al., 2008; J. P. Hamilton et al., 2012; Siegle, Thompson, Carter, Steinhauer, & Thase, 2007), which is in line with the frequent comorbidity of the two disorders (Beesdo et al., 2007; Bittner et al., 2004; Ressler & Mayberg, 2007), studies in which anxious patients had a comorbid depression diagnosis were included in our meta-analysis. Indeed, despite anxiety and depression have been considered two nosologically independent categories according to the traditional classifications, their comorbidity is well-known in clinical practice and research (for a recent revision on comorbid anxiety and depression syndrome, see Choi, Kim, & Jeon, 2020).
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2015; Shamseer et al., 2015) were used to conduct this systematic review and meta-analysis.
Literature search
PubMed, Web of Science, and Scopus were used to select peer-reviewed original papers published in English and before the end of February 2020, exploring the application of rTMS or tDCS in samples of patients suffering from anxiety-related disorders. We combined keywords related to the brain stimulation techniques “rTMS”, “tDCS” with the relevant anxiety disorders labels “generalized anxiety disorder”, “agoraphobia”, “panic disorder”, “specific phobia”, “social anxiety”. We excluded non-English written papers, case reports, systematic and narrative reviews, meta-analyses, conference proceedings, and abstracts. Papers measuring anxiety within non–clinical populations, without a sham or behavioral controlled condition and at least one clinical validated questionnaire were also excluded. Moreover, when multiple papers were based on the same dataset, we included only the first paper reporting the relevant results on the clinical sample.
Records screening and data extraction
To blind the screening process, we used Rayyan (https://rayyan.qcri.org/), a web and mobile systematic reviews manager (Ouzzani, Hammady, Fedorowicz, & Elmagarmid, 2016). After removing duplicates, three researchers (A.V., A.G., A.P.) independently filtered the records as “include”, “exclude”, or “maybe” considering publications’ titles and abstracts. Reasons for exclusion were specified through defined labels based on the inclusion and exclusion criteria. Then, the full text of the remaining records was analyzed by three researchers (A.V., A.G., A.P.), who independently select the eligible studies. When the articles’ full versions were not available, the corresponding authors of the papers were contacted. In both the title/abstract and full-text screening phase, conflicting decisions were solved by consensus. One researcher (A.P.) extracted data by using a previously prepared structured form (Table1), checked for consistency and accuracy by other to authors (A.V., A.G.). Discrepancies were resolved by agreement of three authors (A.V., A.G., A.P.). Measures of anxiety levels were extracted from the selected studies, namely a more “general”one, typically consisting of the Hamilton Anxiety Rating Scale (HAM-A or HARS, Hamilton, 1959) or the Beck Anxiety Interview (BAI, Beck & Steer, 1988), and, when present, a disorder-specific one, which changed depending on the specific disorders (e.g., the Panic Disorder Severity Scale, PDSS, Shear et al., 1997, when participants were recruited based on panic disorder, see the outcome measure paragraph for details). Moreover, given the high comorbidity of anxiety and depressive disorders, when available, depression measures, the Hamilton Depression Rating Scale (HAM-D or HDRS, Hamilton, 1960) or the Beck Depression Inventory (BDI, Beck, Ward, Mendelson, Mock, & Erbaugh, 1961) were also collected and analyzed.
summarizes studies’ features used for the quantitative analysis.
Qualitative analysis
Two researchers (A.V., A.G.) independently assessed the quality of the studies retrieved based on the following Cochrane Collaboration’s Risk-of-Bias Tool (Higgins et al., 2011) criteria: random sequence generation, allocation concealment, blinding strategy, incomplete outcome data, selective outcome reporting. For the selection bias, the random sequence generation item was rated as “low risk” only when the randomization procedures (e.g., random number table, computer-generated randomization, randomization envelops) were reported. The allocation concealment item was rated as “low risk” only for studies that recruited a group of patients who received sham stimulation. For the reporting bias, when available, we checked the registered protocol of the included records. Conflicts were solved by consensus of the two researchers and by consulting a third researcher when needed (A.P.).
Quantitative analysis
For each included study, relevant information was extracted, including means, standard deviations of the scores at the clinical scales, NIBS protocol (technique, number of sessions, stimulation location), and patients characteristics. As the primary outcome measure, the pre-post treatment mean difference in specific scales for anxiety disorders (9 studies included, see the outcome measures paragraph for details) was extracted for the experimental and the control group to measure the impact of the NIBS protocol over the anxiety symptoms. When sufficient information was not reported in the articles’ text, tables, or supplementary material, the authors were contacted to obtain these missing data (de Lima et al., 2019; Dilkov, Hawken, Kaludiev, & Milev, 2017; Notzon et al., 2015). The standard deviation of the change score (pre-to post-NIBS treatment) was calculated, as suggested by the Cochrane handbook for systematic reviews of interventions (Higgins et al., 2019), as:
 where corr is the correlation between pre and post measurements variances, set at .5 as suggested by Follman and colleagues (Follmann, Elliott, Suh, & Cutler, 1992).
where corr is the correlation between pre and post measurements variances, set at .5 as suggested by Follman and colleagues (Follmann, Elliott, Suh, & Cutler, 1992).
Sampling variance, standardized mean difference (SMD), and summary analyses were computed for each included study, using the “escalc” function of “metafor” package for R, version 3.4.3 (Viechtbauer & Cheung, 2010). SMD was corrected for the positive bias for small group within the function, computing Hedge’s g (Hedges, 1981), which was used as an effect size measure. In this meta-analysis, we computed the global effect of NIBS protocol in reducing anxiety symptoms using a random-effects model with the “rma” function of the “metaphor” R package regardless of the heterogeneity tests values: studies, indeed, vary according to their characteristics (e.g., patients’ characteristics, stimulation interventions, associated therapies, etc.). Nevertheless, heterogeneity was assessed through both the variation due to the sampling error (Q statistic) and the percentage of variation between studies due to heterogeneity rather than chance (I2 statistics, Higgins, Thompson, Deeks, & Altman, 2003). Potential outliers were identified with the analysis of influence (Del Re, 2015; Kovalchik, 2013; Polanin, Tanner-Smith, & Hennessy, 2016), implemented in the “inf” function of the “metaphor” R package. Finally, publication bias was controlled for with the funnel plot, the Egger’s regression test (Egger, Smith, Schneider, & Minder, 1997) and the rank correlation test (Begg & Mazumdar, 1994), and eventually corrected with the “trim and fill” method (S. Duval & Tweedie, 2000), which creates dummy potential missing studies to create a more symmetrical funnel plot. Finally, we run a moderation analysis to test whether the duration of the treatment (computed in the number of stimulation sessions), the stimulation technique applied (iTBS, rTMS, tDCS), the protocol type (excitatory vs. inhibitory), the target region2 (left vs. right DLPFC) and comorbid depression (presence vs. absence) influenced the obtained effects.
The same procedures were adopted for the secondary outcome measures, namely the general anxiety scale (HAM-A or BAI, nine studies included) and depressive interview/self-report questionnaire (HAM-D or BDI, seven studies included).
Results
Studies selection
Eight hundred seventy-six publications were identified. We removed duplicates and carefully reviewed the title and abstract of the remaining 637 records. Among these, 605 were excluded since the inclusion criteria were not met, while the full texts of the remaining 32 papers were examined. Ten studies met the qualitative and quantitative analysis inclusion criteria. Four records were excluded because they were conference proceedings (Assaf et al., 2017, 2014; Deppermann et al., 2013; Griffiths, O’Neill-Kerr, & De, 2019), two did not include patients (Ironside et al., 2019), one included patients but without a diagnosis of an anxiety-related disorder (Caulfield & Stern, 2020), and one did not test anxiety as an outcome measure (Heeren et al., 2017). Six studies were excluded because they did not consider a control condition, namely sham stimulation or a control group (Bystritsky et al., 2008; Clarke et al., 2019; Kumar, Singh, Parmar, Verma, & Kumar, 2018; Lu et al., 2018; Mantovani et al., 2007; White & Tavakoli, 2015), six because they involved samples already tested by one of the ten eligible papers (Assaf et al., 2018; S Deppermann et al., 2016; Saskia Deppermann et al., 2017; Diefenbach, Assaf, Goethe, Gueorguieva, & Tolin, 2016; Diefenbach et al., 2019; Praško et al., 2009). The full text of the remaining two studies was not available (He, Zheng, Cai, & Zou, 2011; Wu, Hu, Yu, Liu, & Wang, 2016). Table 2 summarizes the selection procedure.
Flowchart of study selection process.
Quality Assessment
Results of the quality assessment are reported in Table 3. We calculated the percentage of the high-risk judgments to obtain a quality score for each study. The average quality of the studies included in the present review was high to intermediate (range 0-42.86%), with the random sequence generation as the primary source of methodological bias, followed by the blinding mode. Indeed, most of the studies did not describe the randomization procedures, and two studies employed a single-blind design (Movahed, Goradel, Pouresmali, & Mowlaie, 2018; Notzon et al., 2015).
Risk of bias evaluation of papers included in the meta-analysis.
Finally, three studies (Deppermann et al., 2014; Dilkov et al., 2017; Notzon et al., 2015) reported confusing information about the number of patients excluded from the final sample analyzed.
Reporting bias was evaluated considering the details reported in the full-texts, except for three studies (de Lima et al., 2019; Diefenbach, Bragdon, et al., 2016; Nasiri, Mashhadi, Bigdeli, Chamanabad, & Ellard, 2020) whose registered protocol was available to check the completeness and the consistency of the findings. Among these, one study (Nasiri et al., 2020) did not report analyses and results of some of the pre-registered outcome variables, being part of a larger project.
Regarding the allocation concealment, only Nasiri et al. (2020) obtained a high-risk judgment as they used a cognitive treatment and not a sham stimulation as a control condition.
Participants’ characteristics and inclusion/exclusion criteria
Ten studies were included in the meta-analysis, involving 134 participants assigned to the experimental condition with real stimulation and 145 assigned to the control groups. Concerning demographic variables, participants’ age ranged between 18 and 65 years; when reported (8 out of 10 studies), the mean age of participants was 33.7 years for real stimulation conditions (SD± 8.7) and 32.2 (SD± 9) for control groups. In most studies, the number of females was greater than the number of males, and secondary school was the most common education level. Specific participants’ features of the included studies are reported in Table 4.
Summarizes participants’ characteristics of the included studies
The studies differed regarding the number of stimulation sessions (ranging from 1 to 25 sessions),the intervention technique (rTMS, tDCS, intermittent theta-burst stimulation, or iTBS) (see the “stimulation intervention” paragraph), the presence or absence of concomitant treatments (pharmacological or psychological interventions, see the “associated therapies” paragraph), and the patients’ diagnosis.
Concerning inclusion and exclusion criteria, they changed across studies. Participants were typically included if they were in a certain age range, had a specific diagnosis (according to DSM) and reached a certain questionnaire score. Conversely, exclusion criteria typically concerned prior psychiatric history - except for the actual disorder - and suicidality (see Table 7 for details).
The following paragraph will report the details of the samples included.
Patients’ diagnosis
Studies were included if participants received a primary diagnosis of anxiety disease, which could be in comorbidity with depression. Studies in which anxiety was secondary to other conditions (e.g., organic/neurological condition, substance use, etc.) were excluded. Concerning the ten included studies, participants had a diagnosis of generalized anxiety disorder in 6 out of 10 studies (de Lima et al., 2019; Diefenbach, Bragdon, et al., 2016; Dilkov et al., 2017; Huang et al., 2018; Movahed et al., 2018; Nasiri et al., 2020) - in 1 out of 6 combined with insomnia(Huang et al., 2018) and in another one with major depression disorder (Nasiri et al., 2020), panic disorder with or without agoraphobia in 3 out of 10 (Deppermann et al., 2014; Mantovani, Aly, Dagan, Allart, & Lisanby, 2013; Prasko et al., 2007) - in 1 out of 3 major depression disorder was in comorbidity (Mantovani et al., 2013), specific phobia (spider) in 1 out of 10 (Notzon et al., 2015).
Associated therapies
Concerning the associated psychological therapies, 2 out of 10 studies (Deppermann et al., 2014; Nasiri et al., 2020) provided psychological intervention as part of the treatment; however, it was not time-locked to the stimulation. Specifically, in Deppermann et al. (2014), participants took part in three group sessions of psychoeducation concerning the panic disorder, while Nasiri et al. (2020) added the NIBS treatment to the last two weeks of a 12 unified protocol (UP3, Barlow et al., 2011) weekly sessions. Even Notzon and colleagues (2015) applied iTBS before virtual reality exposure, even though the interventions were used in a single session. In 2 out of 10 studies, (Dilkov et al., 2017; Mantovani et al., 2013) individual or supportive psychotherapy was allowed during NIBS sessions, while in 4 out of 10 studies (de Lima et al., 2019; Diefenbach, Bragdon, et al., 2016; Huang et al., 2018; Movahed et al., 2018), psychological interventions were not permitted during NIBS treatment. One study (Prasko et al., 2007) did not report information about this aspect.
Concerning concurrent pharmacotherapy treatment, 3 out of 10 studies (Movahed et al., 2018; Nasiri et al., 2020; Notzon et al., 2015) did not allow medication intake during the NIBS treatment, while the other 7 out of 10 (de Lima et al., 2019; Saskia Deppermann et al., 2014; Diefenbach, Bragdon, et al., 2016; Dilkov et al., 2017; Huang et al., 2018; Mantovani et al., 2013; Prasko et al., 2007) reported that stable medication treatment was accepted. Medication stability was differently defined across the studies, ranging from 4 weeks before treatment onset (Mantovani et al., 2013) to the three months before (Huang et al., 2018; Diefenbach et al., 2016) (see Table 5 for details).
Summarizes stimulation protocols details, treatment strategy and associated therapies.
Stimulation protocols
Of the final ten studies, 5 used an rTMS protocol (Diefenbach, Bragdon, et al., 2016; Dilkov et al., 2017; Huang et al., 2018; Mantovani et al., 2013; Prasko et al., 2007), three a tDCS (de Lima et al., 2019; Movahed et al., 2018; Nasiri et al., 2020), and two an iTBS protocol. RTMS was applied at a frequency of 1 Hz in 4 out of 5 studies (Diefenbach, Bragdon, et al., 2016; Huang et al., 2018; Mantovani et al., 2013; Prasko et al., 2007) and 20 Hz in 1 study (Dilkov et al., 2017). The target region for rTMS intervention was the right DLPFC in 4 out of 5 articles and the right posterior parietal cortex (PPC) for 1 study (Huang et al., 2018). The two iTBS protocols were applied over the left DLPFC. Concerning the three tDCS studies, stimulation was delivered with the cathodal polarity over the right DLPFC in 2 out of 3 studies (Movahed et al., 2018; Nasiri et al., 2020) and with anodal polarity over the left DLPFC in the remaining one (de Lima et al., 2019). Overall, inhibitory protocols (cathodal tDCS, 1 Hz rTMS) were applied over the right DLPFC in 5 out of 6 studies, while only one targeted the right PPC. Facilitatory protocols (iTBS, anodal tDCS, and 20HZ rTMS) were delivered over the left DLPFC in 3 out of 4 studies and over the right DLPFC in 1study (see Figure 1 for a graphical representation of targeted regions). Stimulation intensity range in TMS studies was comprised between the 80% and the 110% of the individual rest motor threshold (RMT). Magnetic pulses were always delivered with a figure of eight shaped coils. tDCS protocols were administered at 2mA intensity in the three protocols, with unipolar montages and intracephalic reference in 1 out of 3 studies (de Lima et al., 2019) and a deltoid reference in 2 out of 3 protocols (Movahed et al., 2018; Nasiri et al., 2020).
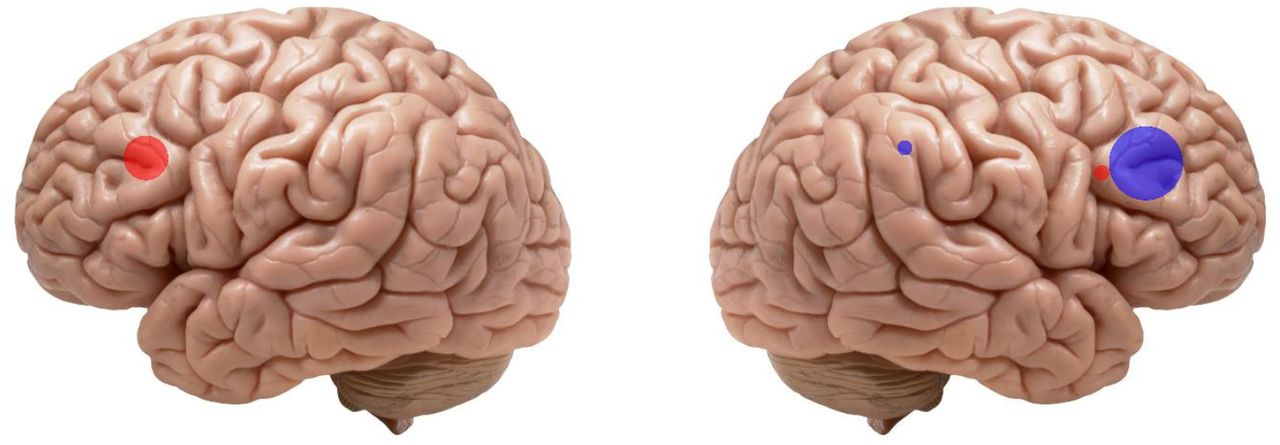
summarizes the type of stimulation and target regions of included studies. Red dots indicate excitatory stimulation protocols (i.e. anodal tDCS, iTBS and high frequency rTMS), while blue dots indicate inhibitory stimulation (i.e., cathodal tDCS and low frequency rTMS). Dots size corresponds to the number of studies applying excitatory or inhibitory protocol over a specific region: five studies applied inhibitory protocols over the right DLPFC, three delivered excitatory protocols to the left DLPFC, one excitatory stimulation over the right DLPFC, one inhibitory stimulation over the right PPC.
Stimulation duration ranged from 10 to 30 minutes. See Tables 5 and 6 for details.
Summarizes stimulation protocol, statistical analyses, main results, additional groups and measures.
summarizes inclusion and exclusion criteria of the selected studies.
Control condition
The presence of a control condition was established as an inclusion criterion in our meta-analysis. For 9 out of 10 studies, it consisted of a sham condition. In contrast, in one study (Nasiri et al., 2020), the control group did not receive a sham stimulation but took part in the UP treatment. For rTMS studies, sham stimulation was induced by varying the coil inclination at 90° with respect to the stimulation site in 4 out of 7 studies (Deppermann et al., 2014; Dilkov et al., 2017; Notzon et al., 2015; Prasko et al., 2007). In contrast, in 3 out of 7studies (Diefenbach, Bragdon, et al., 2016; Huang et al., 2018; Mantovani et al., 2013), experimenters used a sham coil, which had the same appearance and produced the same noise as the real one. Considering the three tDCS studies, 1 applied the typical sham-tDCS protocol (de Lima et al., 2019), namely the stimulation was on for the first 30 seconds, thus inducing the same skin sensation as compared to the real one (Gandiga, Hummel, & Cohen, 2006); Mohaved and colleagues (2018) did not report the sham protocol parameters, and Nasiri et al. (2020) did not have a sham condition but included a control group, in which participants did not receive sham stimulation, but only take part to the cognitive treatment.
Considering the blinding procedure, 8 out of 10 protocols were double-blind, with both experimenters and participants naïfs to participants’ assigned condition. In contrast, 2 out of 10 studies (Movahed et al., 2018; Notzon et al., 2015) used a single-blind design, in which only participants were naïfs to the stimulation group. In 3 out of 10 studies, participants’ blinding was checked with specific questionnaires (Deppermann et al., 2014; Mantovani et al., 2013; Notzon et al., 2015).
Outcome measures
As previously reported, we chose three outcome measure, namely i) a specific anxiety measure centered on the specific disorder investigated in each study, which was reported in 9 out of 10 studies (all but Dilkov et al., 2016); ii) a general anxiety measure, investigating general anxiety symptoms, reported in 9 out of 10 studies (all but Notzon et al., 2015); iii) a measure of depression, which was included in 7 out of 10 studies (depression was not included in Deppermann et al., 2014; Prasko et al., 2007; Notzon et al., 2015).
The specific anxiety outcome measure included scores from a heterogeneous pool of clinical validated questionnaires, depending on the specific disease. For the panic disorder, 2 out of 3 studies (Prasko et al., 2007; Mantovani et al., 2013) administered the Panic Disorder Severity Scale, PDSS (Shear et al., 1997), and the other one (Deppermann et al., 2014) the Panic and Agoraphobia Scale, PAS (Bandelow, 1995). For the specific phobia study (Notzon et al., 2015), the German version of the Spider Phobia Questionnaire, SPQ (Klorman, Weerts, Hastings, Melamed, & Lang, 1974; Watts & Sharrock, 1984) was included. Concerning generalized anxiety disorder, the Penn State Worry Questionnaire, PSWQ (Meyer, Miller, Metzger, & Borkovec, 1990) was included for 2 out of 6 studies (Diefenbach, Bragdon, et al., 2016; Movahed et al., 2018), the Generalized Anxiety Disorder Questionnaire, GAD-Q-IV (Newman et al., 2002) was included for one study (Nasiri et al., 2020), the Lipp Inventory of Stress Symptoms for Adults-ISSL (Lipp, 2000) for another one (de Lima et al., 2019) and the Pittsburgh Sleep Quality Index, PSQI (Buysse, Reynolds, Monk, Berman, & Kupfer, 1989), investigating insomnia symptoms for the fifth (Huang et al., 2018). The sixth GAD study (Dilkov et al., 2017) did not include a disorder-specific questionnaire; therefore, it was not included in the specific anxiety disorders analysis (see Results section).
Concerning the general anxiety measure, for 8 out of 9 studies we included the Hamilton anxiety rating scale, HAM-A or HARS (Hamilton, 1959), which is a 14-item clinical interview targeting somatic and psychic anxiety symptoms. For 1 out of 9 studies (Nasiri et al., 2020), we included the Beck Anxiety Inventory (Beck, Epstein, Brown, & Steer, 1988), a 21-items self-report questionnaire focusing on the somatic symptoms of anxiety occurring over the past week. Notzon and colleagues (2015) study did not include a general anxiety measure; therefore, it was not included in the analysis of general indexes of anxiety (see Results section).
Considering depression outcome measure, for 5 out of 7 studies (Huang et al., 2018; Dilkov et al., 2017; Diefenbach et al., 2016; Movahed et al., 2018; Mantovani et al., 2013) we included the Hamilton Depression Rating Scale, HAM-D or HDRS (Hamilton, 1960) a 21-items (but only the first 17 concurred to the total score) clinical interview targeting somatic and neurovegetative aspects of depression, and for 2 out of 7 (de Lima et al., 2019; Nasiri et al., 2020) theBeck Depression Inventory, BDI(Beck et al., 1961) a 21-items self-report questionnaire investigating disorder’s cognitive and affective dimensions (for a comparison between HDRS and BDI, see Brown, Schulberg, & Madonia, 1995). When both the clinical and the self-report measures of general anxiety or depression were reported only the clinician-administered version was considered.
Meta-analyses results
Anxiety specific disorders
Nine out of ten studies reported scores at specific anxiety disorders scales (see Table1). A meta-analysis was run on these studies to compute the global effect of NIBS on the reduction of anxiety specific symptoms compared to a sham intervention. The random-effects model showed a significant medium impact of non-invasive brain stimulation on patients’ improvement compared to pre-post sham scores (overall SMD of -.49; 95% CI =[-.88, -.09], p=.016; see Table8 for the complete results and Fig. 2 for the forest plot).
shows summarizes results of the three meta-analyses.

Forest plot of the effect size of NIBS on continuous specific anxiety questionnaire scores.
Q-statistic and I2suggest a high heterogeneity between studies (Tab. 8), and this may be due to the differences in methodological aspects across studies. The inclusion of moderators (stimulation sessions number, specific NIBS technique used, protocol type) was not significant (all ps> .103, see Table 9 for the moderators’ statistical results).
shows the results of the moderation analysis for specific and general anxiety scores and depression scores. The applied technique (iTBS, rTMS, tDCS), target region (rPAR, left and right DLPFC), protocol type (excitatory vs. inhibitory) moderators are categorical variables, while session number is a numerical variable. Only for the depression outcome measure, we computed whether the presence of comorbid depression influences the outcome of the scores.
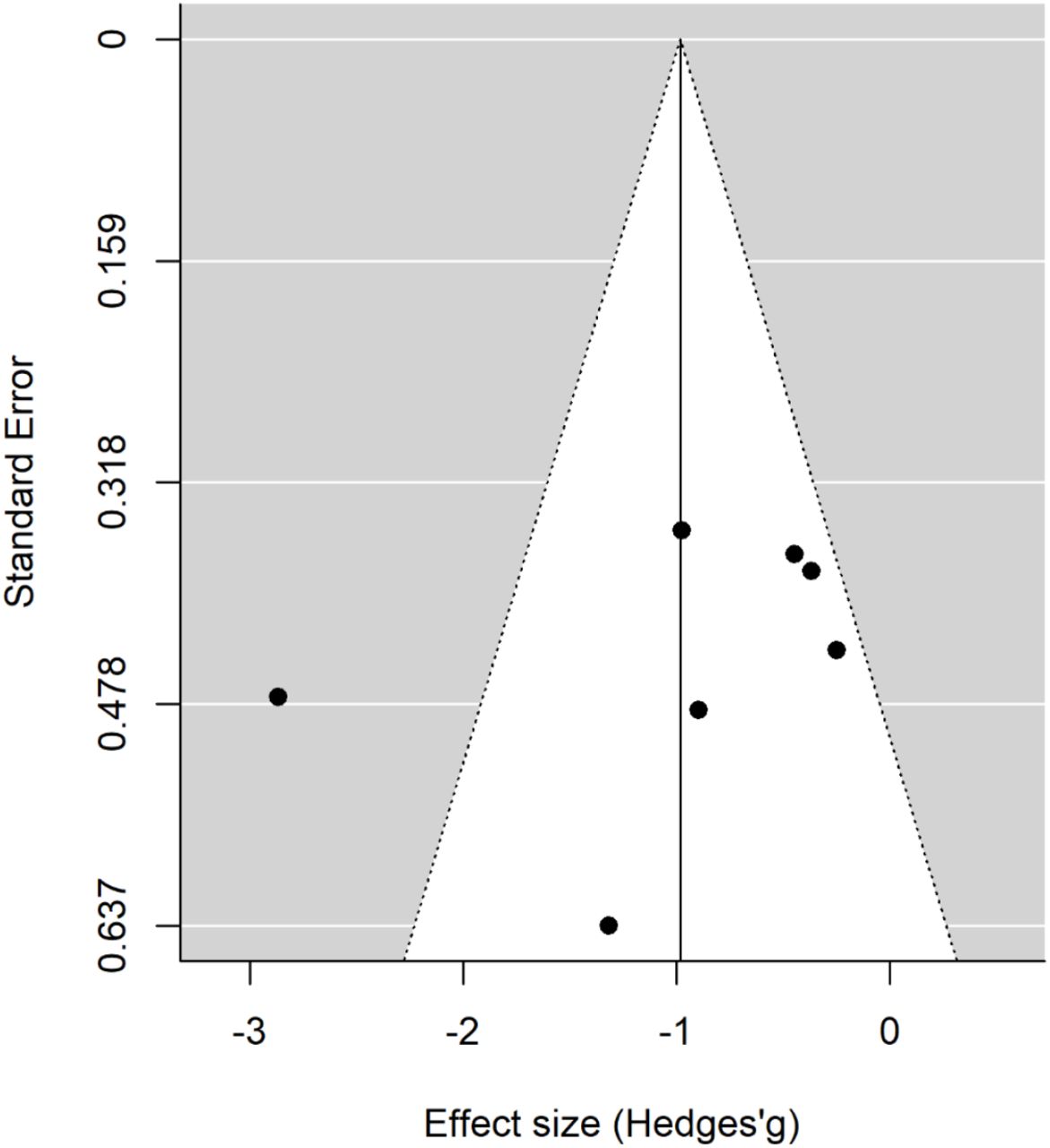
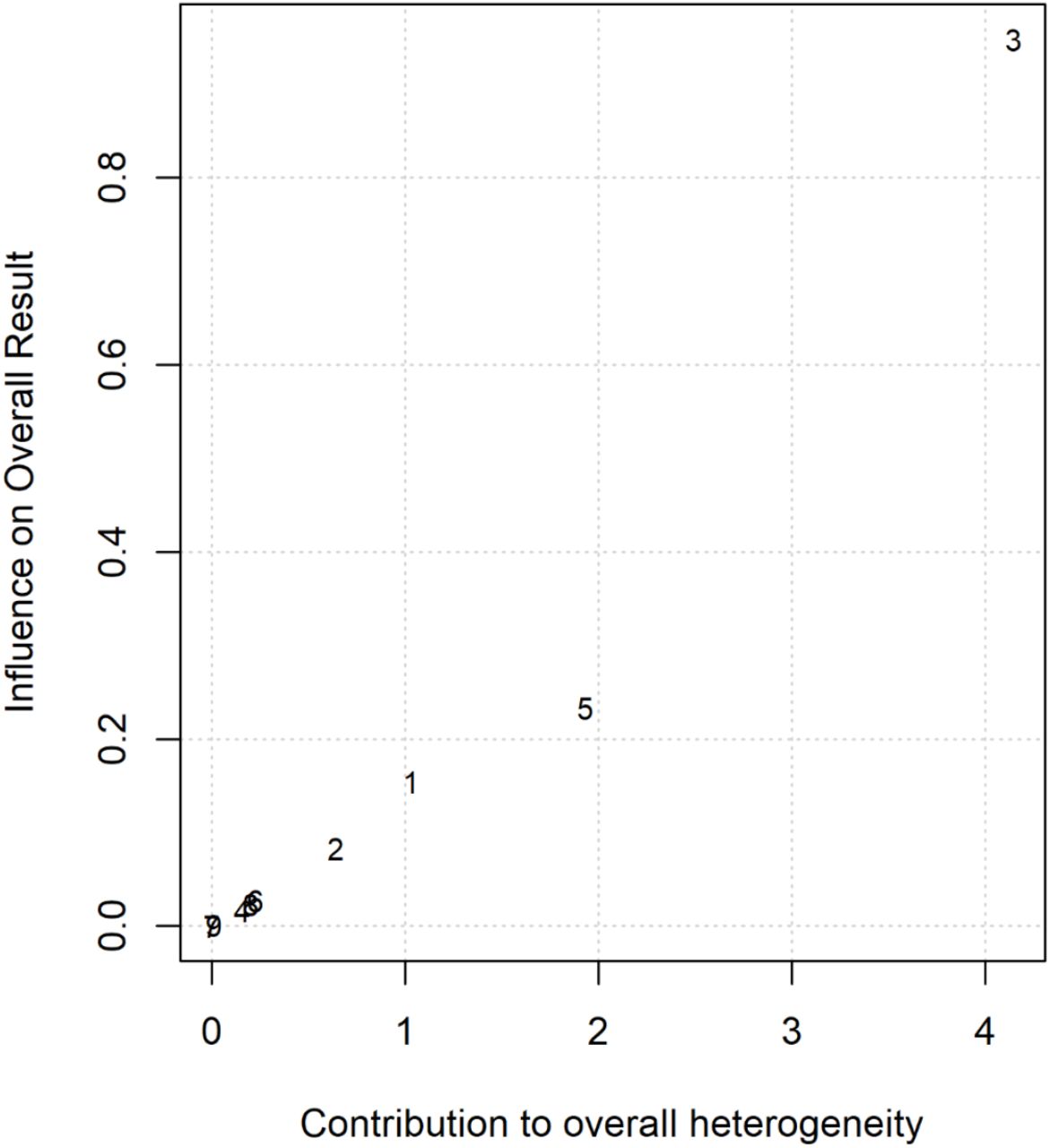
Baujat plot inspection (Baujat, Mahé, Pignon, & Hill, 2002; ; Fig. 3) suggests that study 8 (Mantovani et al., 2013) greatly contributed to meta-analysis heterogeneity. Nevertheless, testing for a possible outlier influence of the included studies in the results (Viechtbauer & Cheung, 2010) showed no study significantly differed from the rest of the data (Table8). Concerning publication bias, the funnel plot (Fig. 4) showed no asymmetry according to both Egger’s regression test (z = −1.2; p=.22) and the Rank correlation analysis (Kendall’s tau = −0.28; p = 0.36).

Baujat plot of studies distribution in terms of heterogeneity. At a visual inspection, study 8 (Mantovani et al., 2013) seems to contribute to the statistical heterogeneity in the analyzed studies.
Publication bias assessed by the funnel plot.
General anxiety indexes
Since nine of the ten included studies reported, alongside with the specific anxiety measures, the pre-post real and sham treatments Hamilton anxiety scores, we run a separate meta-analysis on this scale. As for the specific anxiety symptoms, the random effect model showed a significant medium to the large effect of NIBS protocols in scores reduction as compared to sham treatments (overall SMD of-.81; 95% CI =[-1.45, -.18], p=.012; see Tab 8 for the complete results and Fig. 5 for the forest plot). As for specific symptoms, I2and Q-statistic suggest a high heterogeneity across studies, and Baujat plot suggests study 3 (Dilkov et al., 2017) as the main source of variance (see Fig. 6). The influence test indeed highlighted this study as an outlier (see Table 8). Thus, the random effect model was re-run, excluding this study from the pool. The global effect of NIBS over general anxiety scores reduction remained significant (overall SMD= -.57; 95% CI=[-1.06, -.07], p=.024; see Table8 for the complete results). No other study resulted in a significant outlier. We thus proceeded with the moderation analysis with the original set of 9 studies. The inclusion of moderators in the model was not significant (ps> .192, see Table 9). Funnel plot asymmetry (Fig. 7) tested non-significant for both the Egger’s regression test (z = −0.31, p= 0.76) and the Rank correlation analysis (Kendall’s tau = −0.17; p= 0.61).

Forest plot of the effect size of NIBS on continuous general anxiety questionnaire scores.

Baujat plot of studies distribution in terms of heterogeneity. At a visual inspection, study 3 (Dilkov et al., 2017) seems to contribute to the statistical heterogeneity in the analyzed studies.

Publication bias assessed by the funnel plot.
Depression scales
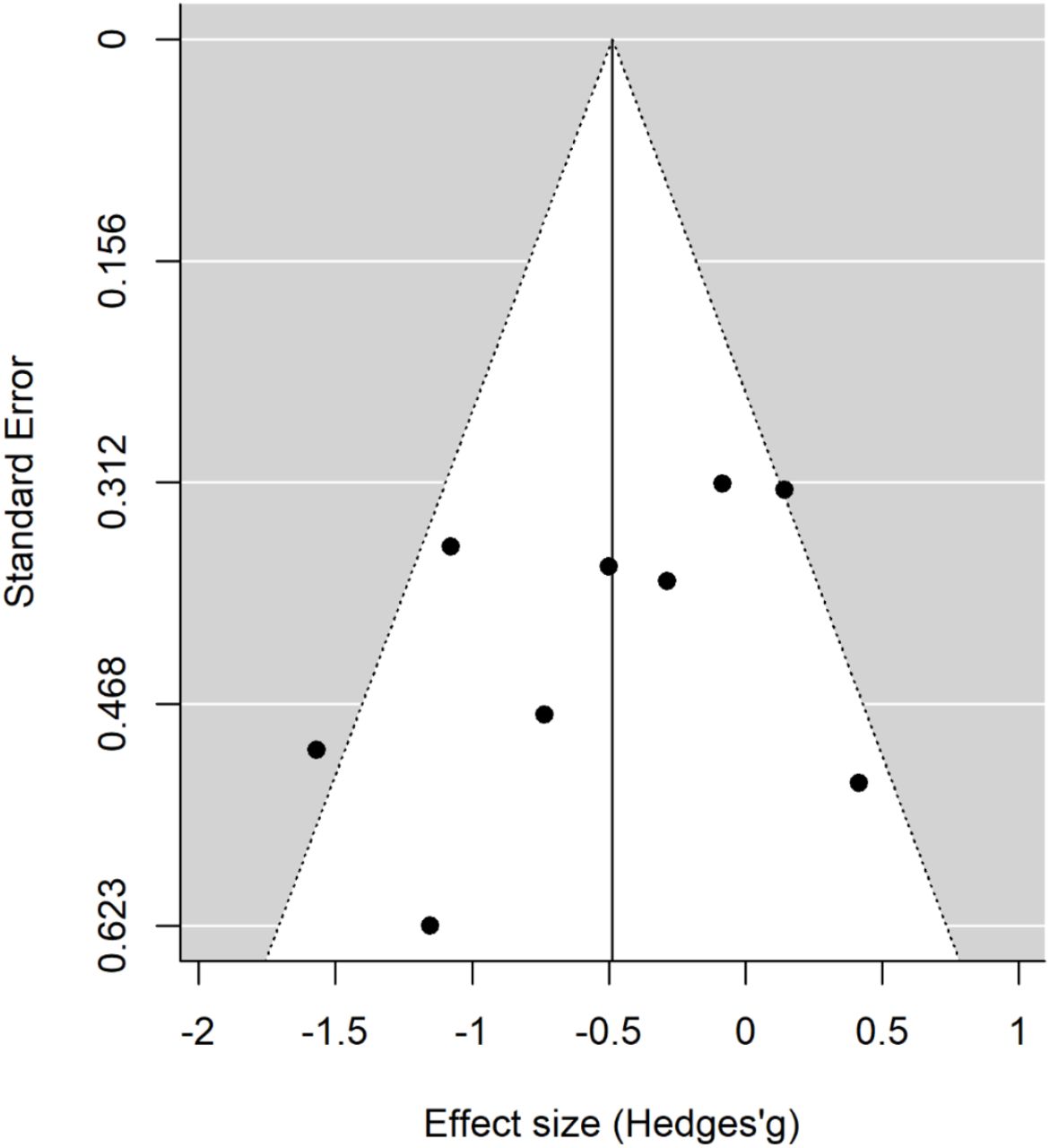
Seven of the final pool studies reported depression scale scores (see Table 1) both before and after the intervention. The random effect model reported a significant global effect of NIBS in reducing the scores at the depression inventories compared to sham interventions (overall SMD= -.98; 95% CI=[-1.62, -.35], p= .002; see Tab 8 for the complete results and Fig. 8 for the forest plot). I2and Q-statistic suggest a high heterogeneity across studies. The Baujat plot suggests study 3 (Dilkov et al., 2017) as the main variance source. The influence test identified this study as an outlier (see Table 8). Even excluding this study from the meta-analysis, the model highlighted a significant effect of NIBS on depression scores reduction (overall SMD= -.64; 95% CI= [-0.98, −0.31], p<.001; see Tab 8 for the complete results). No further study resulted in an outlier from the influence analysis. We thus proceeded with the moderation analysis with the original set of 7 studies. Analysis of moderators indicated a trend toward significance for the effect of the number of stimulation sessions on depression symptoms reduction (QM(1)= 3.1, p= 0.076), with a higher reduction when the number of sessions increased. No effect was found for the presence of comorbidity in the depression scores after treatment (p=.157). Funnel plot asymmetry (Fig. 9) tested non-significant for both the Egger’s regression test (z = −0.8, p= 0.43) and the Rank correlation analysis (Kendall’s tau = −0.07; p= 1).
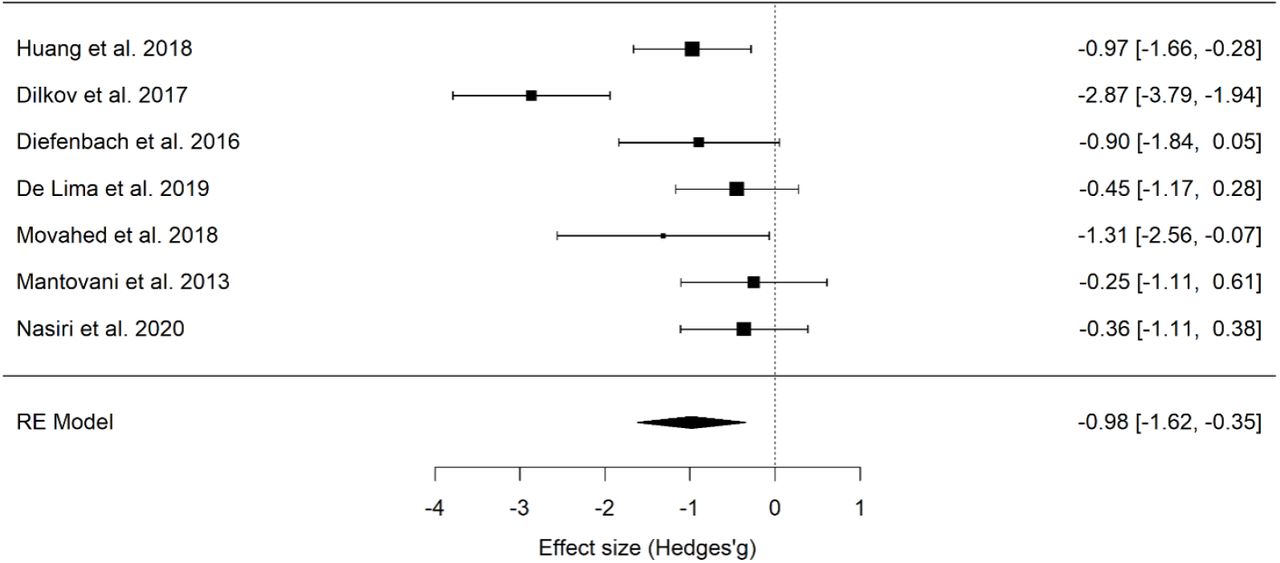
Forest plot of the effect size of NIBS on continuous depression questionnaire scores.

Baujat plot of studies distribution in terms of heterogeneity. At a visual inspection, study 2 (Dilkov et al., 2017) seems to contribute to the statistical heterogeneity in the analyzed studies.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Publication bias assessed by the funnel plot.
Discussion
Over the last decades, the debate concerning the high rate of psychiatric patients not responding to the conventional treatment and the low compliance to the pharmacological intervention due to the significant side effects brought to the increasing demand for novel and complementary approaches, among which the application of NIBS.
Despite the effectiveness of rTMS in depression is well-recognized, its clinical use worldwide accepted (e.g. Brunoni et al., 2019), and recent tDCS panel experts guidelines points the same direction (Fregni et al., 2020), to date no evidence for efficacy have been suggested yet for anxiety disorders(Fregni et al., 2020; Lefaucheur et al., 2020, 2017; Milev et al., 2016), due to the low number of studies specifically investigating this topic.
Therefore, in the present work, we systematically reviewed and quantitatively analyzed the effectiveness of NIBS in ameliorating the clinical symptoms of anxiety disorders. Peer-review, English-written original studies were included in the present work. Given the importance of comparing real stimulation with a placebo or control treatment, we only included studies that randomized participants in these two categories, excluding studies reporting only real stimulation conditions.
Overall, ten articles were included following the highlighted criteria. Studies differed for the specific disease in the anxiety spectrum: nine out of ten studies (all except Dilkov et al., 2017), indeed, reported questionnaires investigating specific anxiety disease symptoms (e.g., the PDSS in panic disorder). Additionally, nine out of ten studies (all but Notzon et al., 2015) included a general anxiety measure, namely the HAMA, the BAI, or both. Therefore, we decided to run two separated meta-analyses concerning anxiety symptoms. The first included for each paper a specific-disorder questionnaire, which should be the specific target of each treatment approach. The second one included a general anxiety questionnaire, namely the HAMA or the BAI; in this case, the clinician-administered HAMA was preferred when available. Interestingly, seven papers (excluded Deppermann et al., 2014; Prasko et al., 2007; Notzon et al., 2015) also included scores at a depression scale (HAM-D or BDI), which was the focus of our third meta-analysis. Indeed, it is well-known that anxiety and depression disorders are often in comorbidity and share some commonalities in the neural substrate involved. Therefore, we wanted to investigate whether NIBS could be useful in reducing depression symptoms.
Our findings highlighted a significant medium effect of the real stimulation in decreasing anxiety scores compared to the control condition, thus suggesting that NIBS can be useful in reducing anxious symptoms in patients. This effect was significant for both the disorder specific and general anxiety measures, which is in line with the high correlation found between the two measures of anxiety (0.6) and might be due to changes in symptoms that are shared by the different anxiety disorders. Crucially, the effect was not likely influenced by publication or reporting bias. In line with previous systematic reviews (Vicario et al., 2018) and meta-analyses (Cui et al., 2019; Trevizol et al., 2016), we also acknowledge the limitation of the present results, which are based on a restricted sample of studies, but a relatively big pool of patients (279 in total).
Concerning the moderation analysis, we included only representative moderators in our analyses, due the small number of studies included. For example, only one study (Huang et al., 2018) targeted the parietal region (PPC), therefore the moderation analysis concerning the target region was run only comparing left vs. right DLPFC stimulation. The analysis of moderators did not highlight significant predictors, possibly due to the limited number of available studies. Only the number of stimulation sessions revealed a trend to significance, with depressive symptoms decreasing for studies including more sessions, in line with a recent meta-analysis (Moffa et al., 2020). The influence of NIBS sessions number in modulating depressive symptoms is debated but still controversial. Some studies and meta-analyses reported a non-significant effect of dosage on symptoms modulation (Brunoni et al., 2017; Razza et al., 2020), while others suggest that at least 20-30 sessions (or more) are required for optimal effects (McClintock et al., 2017; Yip et al., 2017).
Concerning the statistical variability, Q-statistic and I2suggest a high heterogeneity across studies, probably due to the methodological differences across the selected works. Indeed, protocols varied considering participants’ diagnosis and treatment, the inclusion of associated therapies, as well as protocols’ specific parameters, the target brain regions, and interventions duration. Indeed, participants’ diagnosis included generalized anxiety disorder - also combined with insomnia or major depression -, panic disorder with or without agoraphobia – sometimes in comorbidity with major depression -, specific spider phobia. Heterogeneity also characterized the possibility of participants to combine a medication or psychological treatment. Indeed, in three studies (Movahed et al., 2018; Nasiri et al., 2020; Notzon et al., 2015) participants were not allowed to follow a drug therapy, while in others they could continue their treatment or follow a new one (e.g. Deppermann et al., 2014). In the latter situation, a time interval was established before to start the NIBS treatment, which varied across studies but was three weeks at minimum. As for the psychological treatment, only three protocols (Deppermann et al., 2014; Nasiri et al., 2020; Notzon et al., 2015) included a psychological intervention, which was applied before or in parallel to the stimulation sessions. However, psychological and stimulation interventions were not always combined in the same sessions or, in other words, they were not sequentially or simultaneously time-locked (Sathappan et al., 2019). Indeed, in Deppermann et al. (2014) participants took part in three group sessions of panic disorder psychoeducation, separately from NIBS intervention. In Nasiri et al. (2020) tDCS was applied in the last two weeks of an emotional disorder psychological treatment (UP), but authors did not specify whether tDCS was applied before, during or after the treatment. Only Notzon and colleagues (2015), provided a combined approach to the specific phobia, delivering a single session of iTBS before the virtual reality exposure, without effective results concerning the reported scores. As previously highlighted by other researchers (see Sathappan, Luber, & Lisanby, 2019 for a recent review), the lack of combination between behavioral or cognitive interventions with NIBS is a gap in neuropsychiatric literature research. Indeed, it is well-known that NIBS effects are known to be state-dependent, meaning that the state of the stimulated regions during NIBS administration has a great influence on the effects of stimulation on cortical excitability (Bortoletto, Pellicciari, Rodella, & Miniussi, 2015; Romero Lauro et al., 2014; Pisoni et al., 2018; Romero Lauro et al., 2016) and behavior (Luber & Lisanby, 2014; Romei, Thut, & Silvanto, 2016; Silvanto, Bona, Marelli, & Cattaneo, 2018). Moreover, converging evidence suggested that both stimulation and psychotherapy can modulate brain connectivity (Moody et al., 2017; Yoshimura et al., 2017), thus suggesting the importance of time-locking brain stimulation and behavioral engagement to investigate the possibility of maximizing their effects. A similar approach has been initially applied with stroke patients in the neuro-rehabilitation field, combining NIBS with motor and speech trainings(for recent reviews see Breining & Sebastian, 2020; Pruski & Cantarero, 2020). In neuropsychiatric disorders, combined interventions are still in their infancy (Sathappan et al., 2019; Tsagaris, Labar, & Edwards, 2016), even in treating depression that received stronger attention by researchers (Razza et al., 2020; Sathappan et al., 2019). Concerning anxiety disorders, for example, Heeren et al., (2017) combined the Attentional Bias Modification technique with anodal and sham tDCS to reduce the bias for threat in patients diagnosed with social anxiety. The study had a crossover design, indeed participants performed only two sessions: a sham and a real one, and authors reported a significant reduction in the bias in the real vs. sham stimulation. As for other disorders, Segrave and colleagues (Segrave, Arnold, Hoy, & Fitzgerald, 2014) combined tDCS with a simultaneous cognitive treatment (cognitive control therapy) in patients with major depression disorders in a five consecutive daily session treatment. Real and sham tDCS equally improved depression symptoms after the fifth session of the protocol; however, effects were maintained at the three-weeks follow up only for the group assigned to the real stimulation. In schizophrenic patients, brain stimulation has been combined with cognitive remediation, trying to improve the cognitive deficits typical of the disease, but produced mixed results (Jahshan, Rassovsky, & Green, 2017). In conclusion, there is evidence from experimental, behavioral and clinical research suggesting that the coupling of NIBS with a concomitant treatment might enhance the efficacy of each intervention alone. However, results are scarce and controversial, and the topic needs further investigation to sustain this claim.
As for the included NIBS techniques, most studies included a TMS intervention, being either rTMS (Diefenbach, Bragdon, et al., 2016; Dilkov et al., 2017; Huang et al., 2018; Mantovani et al., 2013; Prasko et al., 2007) or iTBS (Deppermann et al., 2014; Notzon et al., 2015). Only three studies (de Lima et al., 2019; Movahed et al., 2018; Nasiri et al., 2020) were based on a tDCS intervention. This choice is in line with knowledge concerning depression treatment, in which rTMS is considered a useful method to treat drug resistant depression and with the idea that rTMS has stronger spatial resolution as compared to tDCS (e.g. Polania, Nitsche, & Ruff, 2018). In a combined approach perspective, however, tDCS can be a convenient option, by reducing exogenous “distractions” due to the rTMS-induced noise and muscular contractions. The latter can be annoying or painful, especially when applied to the prefrontal regions, which are the one typically targeted in the revised treatments.
Recently, besides tDCS and rTMS, deep TMS gained ground in treating OCD (Carmi et al., 2018, 2019) and MDD symptoms (see Gellersen & Kedzior, 2019 for a meta-analysis), receiving FDA clearance for both treatments. This technique used the same principles of TMS, but delivers current through a specially designed H-coil, that can modulate cortical excitability up to 6 cm of depth, therefore reaching not only cerebral cortex activity but also the activity of deeper neural circuits (Roth, Amir, Levkovitz, & Zangen, 2007). To our knowledge, no previous studies investigate deep TMS application to anxiety disorders, and no articles concerning this technique came from our literature search combining “transcranial magnetic stimulation” or “TMS” with the five anxiety categories. However, considering that “deep TMS” was not systematically searched, we combined the keywords “deep TMS” with each of the anxiety disorders in the three previously investigated databases. Pubmed and Scopus research reported no results, while Web of Science search produced three results4: a non-original study (Rakofsky, Holtzheimer, & Nemeroff, 2009), one including animals (Stehberg, Levy, & Zangen, 2009), one involving depressed patients (Berlim et al., 2014). The lack of studies combing deep TMS with anxiety disorders reflects the general limited number of studies investigating NIBS and anxiety disorders as compared to other psychiatric conditions, thus highlighting the importance of shedding light in this field.
Concerning the clinical comorbidity of anxiety and depressive disorders, our results highlighted the efficacy of NIBS in reducing depression scores as compared to the control condition, an effect which was not merely trained by studies in which comorbidity was formally diagnosed in the tested sample. This finding is in line with previous studies that investigated rTMS effectiveness in reducing anxiety symptoms during the treatment of depressed patients. In one of the largest studies, Chen and colleagues (Chen, Hudaib, Hoy, & Fitzgerald, 2019) investigated the efficacy of left-DLPFC high-frequency, right-DLPFC low-frequency and sequential bilateral rTMS (i.e., high-frequency left-followed by low-frequency right DLPFC) in a sample of 697 participants. The stimulation protocols showed an overall efficacy of the three protocols in reducing anxiety and depressive symptoms, without indicating a stronger therapeutic effectiveness of one more than other treatment. In another study, Clarke and colleagues (Clarke et al., 2019), analyzed data on a sample of 248 patients with treatment resistant depression, of which 172 had one or more comorbid anxiety disorders. rTMS was applied using 1 Hz to the right DLPFC or a sequential bilateral protocol (10 Hz over the left DLPFC and 1 HZ over the right DLPFC). Interestingly, rTMS reduced anxiety levels in patients with and without a formal anxiety diagnosis, as showed by the significant reduction of HAM-A scores in both sub-groups. Similarly, in our sample nine out of ten interventions targeted the left or right DLPFC, while only one study (Huang et al., 2018) targeted the right PPC. Crucially, when applied over the right hemisphere (DLPFC or PPC) stimulation was inhibitory (with the only exception of Dilkov et al., 2017, who applied an excitatory protocol over the rDLPFC), with cathodal tDCS or low frequency (1 Hz) rTMS application, while over the left DLPFC, all studies applied excitatory protocols, as iTBS and anodal tDCS. This choice is in line with previous knowledge concerning neural underpinning of anxiety disorders, which suggests the left DLPFC is typically hypoactive in anxiety disorders, while right DLPFC seems to hyperactive (Nitschke & Heller, 2005; Prasko et al., 2004; Uchida & Hirao, 2020). The overlap between the targeted regions and inhibition/excitation protocols explain the reported efficacy of NIBS in reducing both anxiety and depression scores compared to the control conditions. Indeed, despite international guidelines and FDA approval recommend the application of excitatory (high frequency rTMS / deep TMS or anodal tDCS) over the left DLPFC, it is known that NIBS can influence brain excitability also through interhemispheric projections. According to this idea, a change in excitability in one hemisphere, also induced by an exogenous stimulation as NIBS delivery, might induce indirect changes in the other hemisphere excitability and eventually in the behavioral outcome. Such effect has been previously reported for cognitive and motor tasks involving prefrontal and frontal regions (Gilio, Rizzo, Siebner, & Rothwell, 2003; Smirni, Turriziani, Mangano, Cipolotti, & Oliveri, 2015; Vergallito, Romero Lauro, et al., 2018) and neurorehabilitation, especially involving post-stroke patients (Otal et al., 2015)(Bertolucci, Chisari, & Fregni, 2018).
This result is exciting and pave the way to future avenue to specifically investigate the phenomenological overlapping of depression and anxiety disorders. Indeed, not only the stimulation of a similar brain network modulates both anxiety and depression symptoms, but also some antidepressant drugs – primarily serotonin/adrenaline reuptake inhibitors show an effectiveness in treating both disorders, suggesting a similarity also concerning the neurochemical basis of the two syndromes. A recent study by Maggioni and colleagues (Maggioni et al., 2019) specifically investigated neural commonalities and differences between anxiety and depression by using structural magnetic resonance imaging. Albeit preliminary, authors’ findings suggested that the clinical similarities between major depression and anxiety might rely on common prefrontal alterations, involving left orbitofrontal thinning, while frontotemporal abnormalities are traceable in major depression disorder and parietal are specific to panic and social anxiety disorders.
It is interesting to highlight that prefrontal regions are generally linked to emotional processing and regulation (Morawetz, Bode, Derntl, & Heekeren, 2017; Motzkin et al., 2015; Phillips, Ladouceur, & Drevets, 2008; Vergallito, Riva, Pisoni, & Romero Lauro, 2018), which are known to be at the basis of both anxiety and depression development and maintenance.
For instance, previous studies with healthy participants suggested that left DLPFC stimulation has positive effects in modulating several cognitive, emotional and neural processes which are relevant to anxiety (Baumert et al., 2020; Heeren et al., 2017; Ironside et al., 2019; Ironside, O’Shea, Cowen, & Harmer, 2016; see Stein, Medeiros, Caumo, & Torres, 2020 for a systematic revision of tDCS effects in anxiety disorders or anxious behaviors in healthy participants).
A last comment should be done on the outcome measures. In the included papers, nine out of ten studies used as outcome measure scores at validated explicit questionnaires investigating physical and psychological anxiety and depressive symptoms. Only one study (Notzon et al., 2015), investigated psychophysiological measures in addition to questionnaires, namely skin conductance level (SCL) and heart rate variability (HRV). Authors did not report differences in SCL but found a modulation in HRV in real vs. sham iTBS, which was independent from participants’ sample (patients vs. healthy individuals). To date, it is not usual measuring implicit psychophysiological measures as indicators of treatment effectiveness when applying NIBS (e.g. Vicario et al., 2018). However, they might be an index not only to assess treatment improvements, but also to “dose” the intervention in a flexible way and use these measures as a predictor of treatment outcome. For example, in a previous study with Veterans affected by PTSD, baseline startle response to virtual reality combat-related scenes was predictive of the clinical outcome, with higher startle responses predicting greater changes in symptoms severity at the end of the 6 weeks treatment (Norrholm et al., 2016).
To conclude, research investigating the relationship between NIBS and anxiety disorders is still in an embryonal state. Overall, only few studies targeting patients with anxiety disorders are available: many authors, indeed, focused on healthy participants with high trait of anxiety. Concerning the studies including a clinical sample, only few protocols investigated NIBS efficacy at a group-level. Moreover, the inclusion of a sham or control condition to be compared to the real stimulation is not the standard in researchers’ procedure, despite the placebo effect of NIBS techniques is well-known, in both participants and experimenters, thus highlighting the importance of applying double blind procedures (Dawood et al., 2019; Turi et al., 2018). Future studies should also move in the direction of coupling NIBS with behavioral / cognitive interventions, investigating whether coupled treatment can be more effective than monotherapies.
Although preliminary, our results suggest that NIBS can be effective in decreasing anxiety and depressive symptoms in anxiety disorders, thereby paving the way for treatment protocols including NIBS. However, further research is necessary to optimize the protocols in terms of duration, location, intensity, technique, also related to potential inter-individual differences in response to neuromodulation induced by these NIBS (López-Alonso et al., 2014).
Data Availability
Data are available upon reasonable request
Footnotes
AV was supported in part by a 2019 NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation.
↵1 Post-traumatic stress disorder and obsessive-compulsive disorders no longer fall in this grouping, and therefore will be not considered in the present meta-analysis.
↵2 Only one study (Huang et al., 2018) targeted a region different from the left and right DLPFC, therefore we did not include it when analyzing the moderation effect of the target region.
↵3 The UP is a transdiagnostic protocol treatment of emotional disorders, which aims at targeting common features of anxiety and mood disorders, using a single psychological treatment.
↵4 The three results came from the combination of “deep TMS” AND “generalized anxiety disorder” (Rakofsky et al., 2009), “deep TMS” AND “specific phobia” (Stehberg et al., 2009), “deep TMS” AND “social anxiety disorder” (Berlim et al., 2014).
References



