
Abstract
To counter the second COVID-19 wave, the Italian government has adopted a scheme of three sets of restrictions (coded as yellow, orange, and red) imposed on a regional basis. We estimate that milder restrictions in regions at lower risk (yellow) resulted in a transmissibility reduction of about 18%, leading to a reproduction number Rt of about 0.99. Stricter measures (orange and red) led to reductions of 34% and 45% and Rt values of about 0.89 and 0.77 respectively.
Starting from the end of September 2020, a second wave of COVID-19 has been spreading throughout Italy [1]. To counter the rise in SARS-CoV-2 infections, the national government has implemented a number of progressive restrictions, initially implemented homogeneously over the country, and then reflecting regional heterogeneities in the transmission and the pressure on healthcare systems [2-5].
In this work, we aim to evaluate the impact of the different restriction levels implemented on a sub-national scale in reducing SARS-CoV-2 transmission.
The study
We collected information about interventions performed in Italy since October 14 from official sources [2-10]. Between October 14 and November 5, 2020, interventions were uniformly enacted at the national level. Starting November 6, different interventions were performed at the regional scale. Three sets of measures were enacted by the central government after epidemiological risk assessments of regions based on the combination of quantitative indicators on: i) the level of transmission, ii) the burden on older age groups and healthcare, and iii) public health resilience [5]. The sets of interventions were labeled according to a color scheme: yellow, orange, and red, corresponding to increasing levels of restrictions (Table 1).
Data for the epidemic curves were collected by regional health authorities and collated by the Istituto Superiore di Sanità (Italian National Institute of Health) within an integrated surveillance system [11]. From the epidemic curves and the distribution of the serial interval [12-13], we estimated the net reproduction number Rt as a measure of transmissibility for each of the 107 Italian provinces, using a well-established method [14-17].
We applied a linear mixed model to assess the impact of regional control measures on SARS-CoV-2 transmissibility (i.e., Rt):
 where
where
Yp,T represents the value of Rt in each of the 107 Italian provinces (p), averaged over two possible time periods (T): October 30 to November 5 (i.e., when national-level interventions were still in place) or November 19 to November 25 (i.e., two to three weeks after the introduction of region-specific measures);
 is a binary variable set to 1 if province p belongs to a region with maximum restriction level l, and 0 otherwise;
is a binary variable set to 1 if province p belongs to a region with maximum restriction level l, and 0 otherwise;ZT is a binary variable set to 0 if T=October 30 – November 5 and to 1 if T=November 19 – November 25;
β0, β1, β2, β3, β4, and β5 are model parameters, with β0 representing the average value of Rt for provinces in yellow level during the period October 30 – November 5.
ar and br,p are random effects, assumed to be normally distributed. ar allows random deviations among regions from the average value of Rt. br,p allows random deviations, among provinces within a region, from the regional average of Rt.
εp,T is random noise assumed to be normally distributed.

Impact of restrictions levels on transmissibility
The temporal dynamics of Rt, as well as the timing of implementation of the three levels of interventions, were highly variable by region and province (Fig. 1). Eleven of 21 regions/autonomous provinces maintained the same level of restrictions throughout the study period; for all remaining regions except Abruzzo, the highest level of restriction corresponded also to the one which has been maintained for the longest time.

Temporal dynamics of the net reproduction numbers Rt and of the restriction levels applied between October 30 and November 25. Each line shows the mean Rt for an Italian province (black) or region (blue). Provinces are grouped by region as interventions were carried out at the regional level. Colored rectangles refer to the timeframe when the different sets of interventions were adopted (see Tab. 1 for color codes).
The model estimated an average absolute reduction in Rt of 0.22 (95%CI: 0.10 - 0.35) for the least restrictive interventions (yellow). On top of this reduction, we estimated an additional reduction of 0.24 (95%CI: 0.09 - 0.39) for the intermediate level of interventions (orange), and an additional 0.40 (95%CI: 0.26 - 0.55) reduction for the most restrictive measures (red) (Appendix). The net reproduction number fell below the epidemic threshold in 42 of 46 (91%) provinces in red regions, in 33 of 41 (81%) provinces in orange regions and only in 10 of 20 provinces in yellow regions (50%), despite the latter starting from a much lower Rt value (Fig. 2, Appendix).

Distribution of the estimated reproduction numbers Rt across provinces aggregated according to the maximum level of regional restrictions and period of observation, with the corresponding fit from the linear mixed model. Boxplots represent the median, interquartile range and 95% quantiles of the Rt distributions. Red dots represent the mean of the model fit and red vertical lines represent the 95% confidence interval around the mean.
Discussion
Our results suggest that the additional restrictions implemented on a regional basis by the Italian government since November 6, 2020 were effective in reducing the transmissibility of the second wave of COVID-19. Milder restrictions (yellow) implemented in regions considered at lower risk provided a transmissibility reduction which brought Rt to values close to 1, resulting in an approximately constant incidence. Stricter restrictions (orange and red) were both able to bring the reproduction number significantly below the epidemic threshold, even though starting from higher values, resulting in a decreasing incidence. Overall, provinces enacting yellow measures achieved a 18.4% reduction of Rt with respect to the transmission level determined by the preceding nationwide interventions while a reduction of 34.0% and 44.9% was observed for orange and red measures respectively (Appendix).
Results were robust when aggregating the analysis at the regional level (although with lower statistical power due to the lower number of data points), when the reproduction number was estimated from the curve of hospitalized cases, and when considering alternative lengths of the observation periods (from 3 to 12 days) (Appendix).
We acknowledge that during high incidence periods there may be significant changes in notification rates due to the saturation of tracing and testing capabilities [15-16]; this may lead to biases in the estimates of the reproduction numbers. During the second wave, the largest increase in the number of cases occurred in October; therefore, we expect the notification rate to have stabilized before the study period (October 30 – November 25). Notification rates are less subject to changes for hospital admissions, and we found similar results when using these data to estimate transmissibility.
National interventions implemented by the Italian government were scaled up in three different occasions (on October 13, 18 and 24 [2-4]) before adopting the color-based regional classification system since November 6, 2020. It is therefore possible that part of the decrease of Rt after November 6 is associated to a residual effect of earlier interventions. Previous studies [17] have shown that most of the reduction in Rt takes place within about two weeks after the introduction of restrictions. Therefore, this limitation should not have a major effect on our conclusions, and especially on the additional effect of orange and red restrictions levels compared to the yellow one. Relatedly, our assumption to classify regions based on their maximal restrictions may not appropriately reflect the dynamical changes in restriction levels occurring for about half of Italian regions (Fig. 1). To evaluate possible biases arising from this assumption, we run a sensitivity analysis where we categorize regions in five groups: regions with yellow, orange, and red levels of restrictions throughout the study period, and regions which had different restrictions levels reaching up to either the orange or the red level. The obtained results were substantially equivalent to those presented in the main text, although with lower statistical power (Appendix).
Finally, we stress that our analysis is not suitable to pinpoint which specific interventions maximized the Rt reduction [18, 19], to disentangle the effect of spontaneous behavioral changes, and could not capture possible cross-regional effects. For example, provinces performing yellow level measures and sharing borders with regions performing orange or red measures may have indirectly benefited from a reduction of inter-regional mobility or that residents were more prone to self-imposing restrictions to their activity patterns.
Conclusion
This study provides a timely assessment of the effectiveness of heterogeneous interventions adopted in Italy on a regional basis, which is essential to support the ongoing effort to curtail the second wave of COVID-19 and to plan the response to possible future resurgence of cases.
Data Availability
Data are available from the corresponding author upon reasonable request.
Appendix
1. Additional results of the main analysis

Timeframe of interventions in each Region and the Autonomous Provinces (AP) of Trento and Bolzano.

Variation of the net reproduction number Rt in each province. The arrows indicate the variation in Rt from the week before the introduction of the regional system of colour-coded measures (October 30- November 5) to the end of our observations (November 19 – 25). Provinces are ordered by decreasing reduction in Rt.
Results of the linear mixed model on the net reproduction number Rt at provincial level. The estimated standard deviation for the random effect between regions, ar, was 0.09, while the one for the random effect between provinces of the same region, bp,r was 7·10−10. The estimated standard deviation for random noise, εp,T, was 0.20.
Estimates of the net reproduction number Rt across regions with different restriction levels, before and after regional interventions.

Analysis of residuals for the linear model. Left: distribution of Pearson residuals (i.e., raw residuals normalized with respect to the variance of residuals); right: scatterplot between Pearson residuals and fitted values of Yp,T.
2. Sensitivity analysis
We evaluated the robustness of our results by re-running the main sensitivity analyses with alternative modelling choices. In particular, we considered the following five sensitivity analyses:
Hospital admission. We used the same model as described in the main text, but considering as dependent variable Yp,T the reproduction number from hospital admissions, Rth, by province and period of observation;
Regional analysis. we used the following model
which is analogous to the one described in the main text, but considering as dependent variable Yr,T the regional values of Rt, and where the independent variables are region-specific;Regional analysis on hospital admission. We used the same model as in (2) but using as dependent variable Yr,T the regional values of Rth;
Alternative time frame. We considered a number of different lengths of periods T for the evaluation of Yp,T ;
Alternative categorization of restrictions. We considered a finer categorization of regions with 5 restriction levels rather than 3, to account for the temporal evolution of regional restrictions.

2.1 Hospital admission
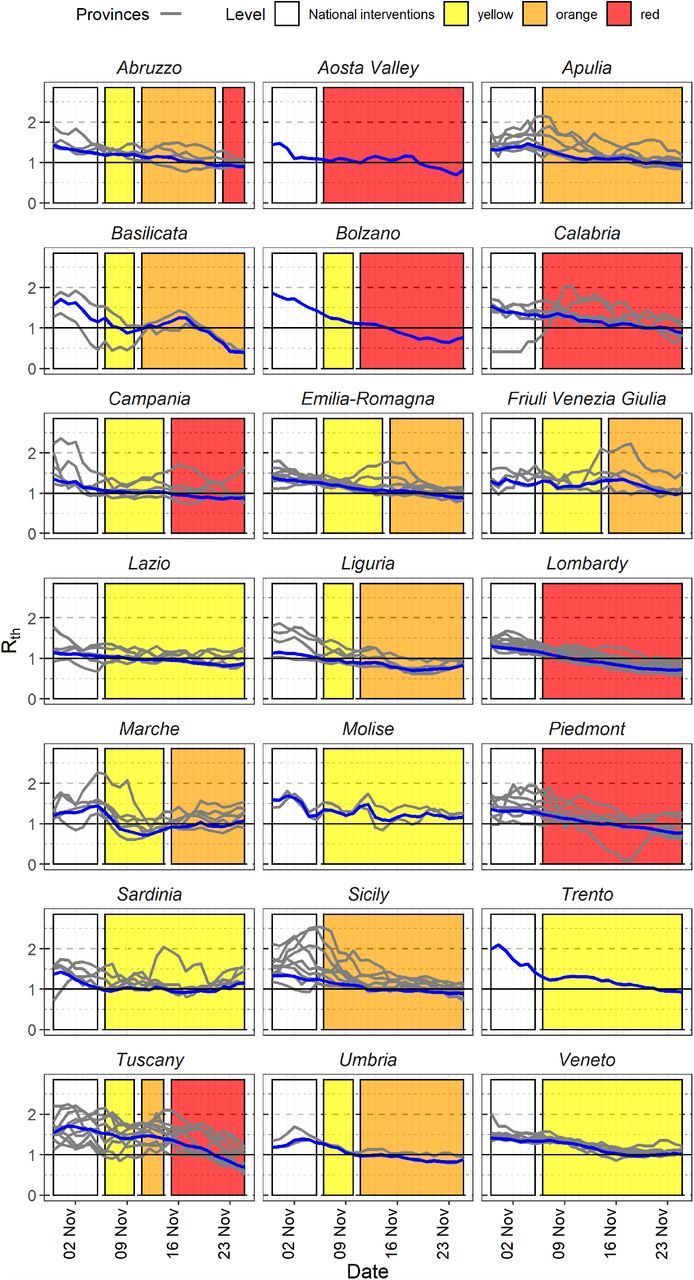
Figure S4 shows the estimated Reproduction number from hospital admissions (Rth) curves for the 107 Italian provinces and regions, as well as restriction levels attributed to each region over time. The obtained results are reported in Tab. S3, Fig. S5, and Tab. S4.

Temporal dynamics of the net reproduction numbers from hospital admissions, Rth, and of the restriction levels applied between October 30 and November 25. Each line shows the mean Rth for an Italian province or region. Provinces are grouped by region as interventions were carried out at the regional level. Coloured rectangles refer to the timeframe when the different packages of interventions were adopted (see Tab. 1 in main text for a description of restrictions corresponding to each colour).
Result of the linear mixed model on the net reproduction number estimated from hospital admissions, Rth, at the provincial level.

Variation in the net reproduction number from hospital admissions (Rth) in each province. The arrows indicate the variation in Rth from the period before the introduction of the regional system of colour-coded measures (October 30-November 5) to the end of our observations (November 19 – 25). Provinces are ordered by decreasing reduction in Rth.
Estimates of the net reproduction number from hospital admissions Rth, across regions with different restriction levels, before and after regional interventions.
2.2 Regional analysis
We applied the same linear mixed model to the Rt values computed at regional rather than at provincial level. Table S5 reports model results for Rt computed from symptom onset, which are compliant with results obtained at provincial level, although they show lower statistical power due to the lower number of observations.
Result of the linear mixed model on the net reproduction number estimated from symptom onset, Rt, at the regional level.
2.3 Regional analysis on hospital admission
Tab. S6 reports similar findings to Tab. S5 starting from the reproduction number estimated from the time series of hospital admissions.
Result of the linear mixed model on the net reproduction number estimated from hospital admission date, Rth, at the regional level.
2.4 Alternative time frame
We applied the same linear mixed model to the Rt values computed at provincial level but within different period lengths ranging from 3 to 11 days. For example, when considering a period length of 3 days, we compared the mean Rt in period November 3 – 5 (before regional interventions) against November 23-25. Figure S6 shows the difference between the model parameters estimated for each period length compared to the baseline (7 days). Estimated variations in parameter estimates are small, confirming the robustness of results in the main analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Variation in estimated model parameters when considering different lengths (in days) of the window over which Rt is averaged. On the x axis the difference between the estimated parameter value of the parameter and the corresponding baseline (using a 7-day window). Parameter names are on the y axis. Colours represent different period lengths. Asterisks represent statistical significance of the estimated model parameters (p-value <0.05).
2.5 Alternative categorization of restrictions
In this sensitivity analysis, we categorize regions in five groups (see Figure S1 for reference):
L1: restriction level constantly yellow (20 provinces): Lazio (5 provinces), Molise (2 provinces), Sardinia (5 provinces), Trento (1 Autonomous Province), Veneto (7 provinces);
L2: restriction level reaching up to orange (26 provinces): Basilicata (2 provinces), Emilia-Romagna (9 provinces), Friuli Venezia Giulia (4 provinces), Liguria (4 provinces), Marche (5 provinces), Umbria (2 provinces);
L3: restriction level constantly orange (15 provinces): Apulia (6 provinces), Sicily (9 provinces)
L4: restriction level reaching up to red (20 provinces): Abruzzo (4 provinces), Bolzano (1 autonomous province), Campania (5 provinces), Tuscany (10 provinces);
L5: restriction level constantly red (26 provinces): Aosta Valley (1 province), Calabria (5 provinces), Lombardy (12 provinces), Piedmont (8 provinces).
The obtained results were substantially equivalent to those presented in the main text (see Table S7).
Result of the linear mixed model on the net reproduction number estimated from symptom onset Rt at provincial level considering 5 groups of interventions
Footnotes
↵# joint senior authors



