
Abstract
Background The ongoing COVID-19 pandemic has profoundly affected the mental health of health care workers (HCWs), and optimal strategies to provide psychological support for HCWs are not currently established.
Aims To rapidly review recently-published literature on the mental health of HCWs during the COVID-19 pandemic.
Methods Query of all quantitative research through the PubMed database on the mental health of HCWs during the COVID-19 pandemic which utilized validated mental health instruments. 723 articles were screened and 87 articles were included.
Results Nearly all included studies were cross-sectional, survey-based assessments of the prevalence of and risk factors for mental illness. Only one interventional study was identified. Prevalence of mental health outcomes varied widely: 7.0-97.3% anxiety, 10.6-62.1% depression, 2.2-93.8% stress, 3.8-56.6% post traumatic stress, 8.3-88.4% insomnia, and 21.8-46.3% burnout. Risk and protective factors were identified in personal and professional domains, including degree of COVID-19 exposure, adequacy of protective equipment, and perception of organizational support.
Conclusions The myriad risk factors for poor mental health among HCWs suggests that a comprehensive psychosocial support model with individual- and organization-level interventions is necessary. Further longitudinal research on specific evidence-based interventions to mitigate adverse mental health outcomes among HCWs is urgently needed as the pandemic continues.
Introduction
The COVID-19 pandemic is an unprecedented phenomenon that has profoundly affected health care delivery on a global scale. As the pandemic has evolved and various regions in the United States as well as across the world have experienced cycles of outbreaks and recovery, the laypress and academic literature have increasingly focused on the impact of the pandemic on the mental health of health care workers (HCWs).1 Research from previous epidemics, particularly the Severe Acute Respiratory Syndrome (SARS) epidemic of 2003, has demonstrated high rates of both acute and chronic mental health among HCWs who cared for patients with SARS.2,3 With headlines detailing the ‘moral injury’ of clinicians and the effects of repeated psychological trauma from caring for patients with COVID-19,4 it is critically important to review the current literature base to inform our approach towards caring for the psychological needs of HCWs, which may be different from previous infectious epidemics. In this manuscript, we perform a rapid review of literature on the mental health of HCWs during the ongoing COVID-19 pandemic, and evaluate evidence-based interventions to mitigate adverse mental health outcomes in HCWs.
Materials and methods
In this rapid review of quantitative research studies assessing the mental health of HCWs during the COVID-19 pandemic, we searched for potential eligible articles on the PubMed online database on September 14, 2020 using the following search term: (COVID*) AND (health worker OR healthcare worker OR healthcare professional OR health professional) AND (mental OR psych*). Inclusion criteria were as follows: primary research on the mental health or psychological effects of the COVID-19 pandemic on HCWs, use of a validated psychometric instrument, published in a peer-reviewed journal, and written in English. Exclusion criteria included systematic reviews, meta-analyses, qualitative studies, pre-prints, and studies of only dentists. Studies which included both the general public and HCWs were included if the outcomes for HCWs could be easily distinguished from the general public. Interventional studies were only included if specific validated instrument outcomes resulting from the intervention were studied. Data extraction was performed in Microsoft Excel and relevant information, including country, dates of survey assessment, sample size, types of HCWs workers studied, instruments used, and outcomes were noted. Specific topic areas and themes of included studies were combined and presented as follows.
Results
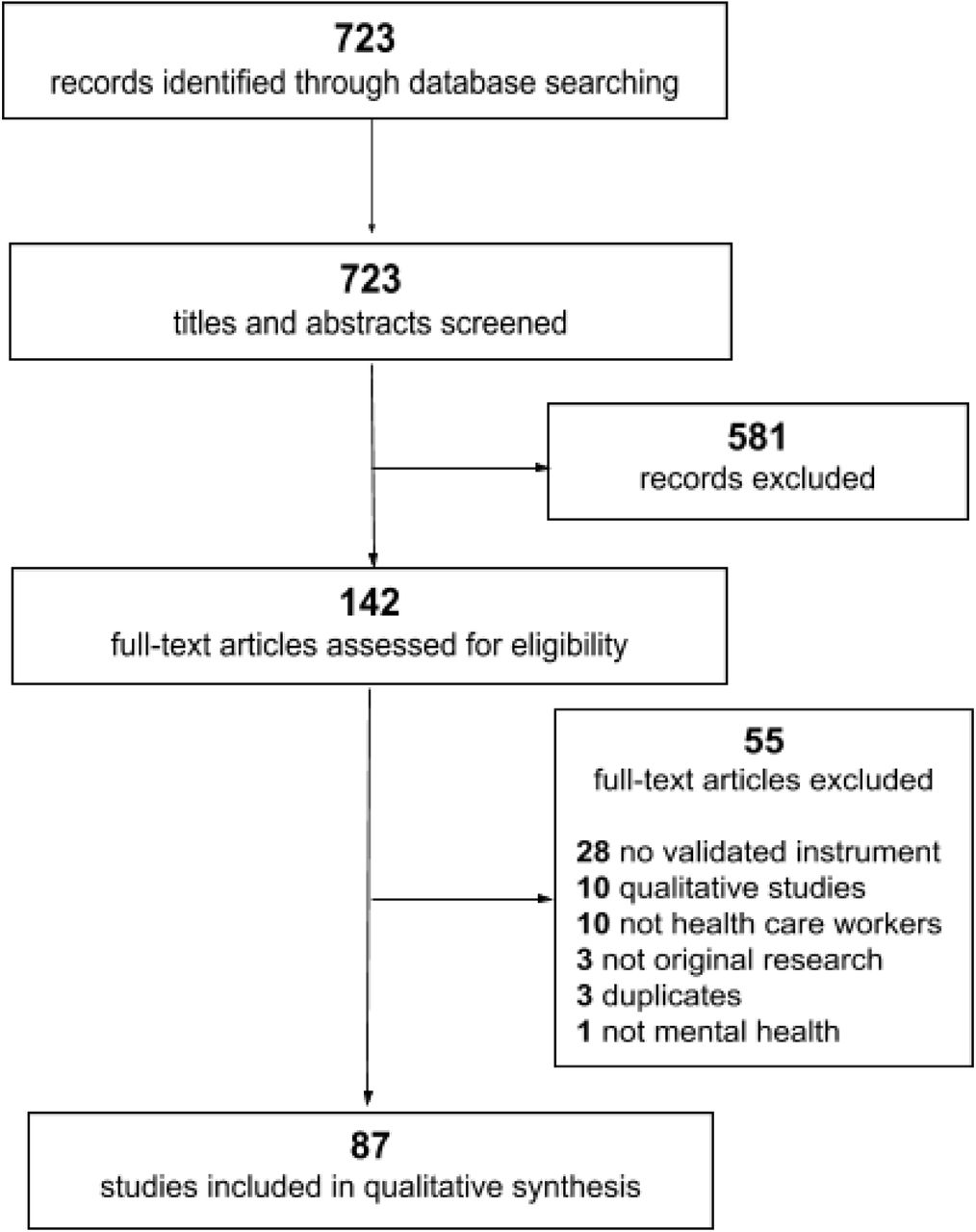
The database search identified 723 articles, as shown in the PRISMA diagram in Figure 1. After screening titles and abstracts, 581 were excluded based on the aforementioned inclusion and exclusion criteria. A total of 87 studies met inclusion criteria and were included for qualitative synthesis after full-text reading. Of these, 86 were epidemiological studies of HCWs and 1 was an interventional study. The full list of included articles are summarized in Table 1.
Summary of all included studies.

{kind=link}
As shown in Table 1, the majority of studies were from China (n = 43, 49%), followed by the United States (n = 7), Italy (n = 5), Singapore (n = 3), Turkey (n = 4), Iran (n = 3), Pakistan (n = 3), India (n = 2), Poland (n = 2), Saudi Arabia (n = 2), Spain (n = 2), Colombia (n = 1), Ecuador (n = 1), Germany (n = 1), Ireland (n = 1), Japan (n = 1), Oman (n = 1), Romania (n = 1), Serbia (n = 1), Singapore and India (n = 1), South Korea (n = 1), and Vietnam (n = 1). The majority of studies occurred early in the pandemic, with 10 studies beginning in January, 27 in February, 20 in March, 15 in April, and 4 in May. Nearly all of the epidemiologic studies were cross-sectional survey-based studies, with the exception of one case-control study.5
As displayed in Table 1, there was considerable heterogeneity in the mental health outcomes studied and the types of quantitative mental health instruments used. Prevalence of mental health outcomes also varied widely, from 7.0-97.3% anxiety, 10.6-62.1% depression, 2.2-93.8% stress, 3.8-56.6% post traumatic stress (PTS), 8.3-88.4% insomnia, and 21.8-46.3% burnout. These outcomes also varied by country and over time, with very high levels of mental illness in Iran in February6 and Pakistan in May,7 compared to very low levels in China8,9 and Singapore10,11 in February.
Risk factors for adverse mental health outcomes
The majority of studies were epidemiologic and assessed risk factors for adverse mental health or psychological outcomes for HCWs during the COVID-19 pandemic. Risk factors are summarized in Table 2 and are categorized as follows.
Summary of risk factors and protective factors for mental health in health care workers.
Frontline workers
Frontline HCWs had worse mental health outcomes than non-frontline HCWs in multiple studies, including increased rates and severity of anxiety, depression, fear, and distress.12,13,14,15,16,17,18,19,20 The only case-control study in this review compared 1173 frontline HCWs with 1173 age- and sex-matched non-frontline HCWs across China and found that frontline HCWs had significantly higher rates of any mental health issue than non-frontline HCWs, at 52.6% versus 34.0%, but no significant difference in suicidal ideation, help-seeking, or mental health treatment.5
Nurses
Nurses experienced poor mental health outcomes compared to physicians and other HCWs,14,21,22,23,24,25,26 with several studies identifying specific subsets of the nursing profession at risk for adverse mental health outcomes. Nurses in COVID-19 wards had higher self-reported rates of stress, exhaustion, and depression and lower job fulfillment than nurses in non-COVID wards,27 nurses with more work-hours and more night shifts experienced more fatigue,28 and nurses without intensive care unit (ICU) experience deployed to COVID-19 ICUs experienced more stress.29 Physical and mental fatigue have been associated with anxiety, depression and stress in nurses as well.28 One study in Turkey surveyed nursing students before and after the outbreak and found that over half of the nursing students reported anxiety, and anxiety was associated with negative perspectives on the nursing profession as well as unwillingness to practice the profession of nursing in the future.30
Women
Many studies found that women experience worse mental health outcomes on multiple instruments as compared to men.6,8,14,17,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45
COVID exposure and infection
Direct contact with COVID-19 patients was associated with poor mental health outcomes,8,13,31,35,36,43,45,46,47,48 as well as personal fear of infection and perceived threat of contagion.13,21,22,27,32,37,49,50,51 These adverse outcomes were also seen in HCWs with friends or family with COVID-19 infection22,32,33,34,49 and in HCWs with colleagues who were hospitalized or died of COVID-19.39 Further, working in COVID-19 designated hospitals compared to non-designated hospitals25,49,52 and working in COVID-19 specific isolation wards13,22,40,45 were associated with poorer mental health outcomes. However, smaller single-institution studies in Romania53 and in Guangzhou, China,54 where there were fewer COVID-19 cases, did not find differences in mental health outcomes between HCWs working in dedicated versus non-dedicated wards. In this same vein, geographic regions with higher rates of COVID-19 cases, such as Wuhan and Hubei province, had worse mental health outcomes than other less affected areas.9,14,32,46,49,50,55 This finding was also demonstrated in Italy16 and the United States.44 One study of 595 HCWs in Italy compared mental health outcomes between HCWs with positive COVID-19 testing, HCWs with COVID-19 exposure, and control HCWs, and found fourfold worse anxiety and depression in COVID-infected HCWs.48
Quarantine
One large study in China of 1443 Chinese citizens under quarantine (22% HCWs) and 836 Chinese citizens not under quarantine (64% HCWs) did not find a difference in anxiety, depression or distress,56 although PTS was found to be more severe in quarantined HCWs in a separate study.57 A single-institution study of quarantined HCWs in Vietnam found evidence of social stigma, negative self-image, and guilt towards family and friends.58
Trainees
Several studies assessed mental health in trainee physicians, finding more depression24 and loneliness26 in trainees compared to other HCWs. A large multicenter survey of trainees in the United States found that frontline trainees have worse burnout and stress, but similar anxiety and depression, to non-frontline trainees, and that trainees who were COVID-19 exposed, women, and unmarried also have worse outcomes.59 Medical students have also been studied, with one single-institution study in Iran of 886 Iranian citizens, which included 207 (23%) medical students, finding worse mental health in medical students compared to medical staff and the general population.6
Pediatric HCWs
Several studies assessed pediatric HCWs, revealing that they reported poorer mental health outcomes than the general population.60 With respect to risk factors, working in outpatient, emergency and ICU departments61 and COVID-19 exposure60,62 were associated with worse mental health outcomes. A large multicenter study of 2031 pediatric HCWs from 29 provinces across China found that frontline HCWs, men, physicians, HCWs aged 31-60 years, HCWs with senior job titles, and HCWs who had experience combating similar outbreaks were more likely to have stress, depression and anxiety.62
Organizational characteristics
Lack of access to adequate personal protective equipment (PPE) was associated with increased anxiety and depression in several studies.13,21,31,50 Poor supervisor support was associated with worse mental health in a large single-institution study of 5550 HCWs in the United States.45
Professional characteristics
Various professional risk factors for poor mental health outcomes were identified, including increased work-hours,24,42,63 more than 10 years of working experience,33,34 HCWs without public health emergency experience,64 hospital-based physicians,16 more night shifts,16 lower job seniority,16 significant work adjustments,65 physicians worried about training or professional growth,66 and physicians with difficulty meeting living expenses.66
Personal characteristics
The majority of studies found that younger HCWs had worse mental health outcomes than older HCWs,17,37,38,39,41,42,43,45,66 although one study of nurses and health care technicians in radiology departments in China found that older HCWs had increased anxiety.21 HCWs with comorbid chronic diseases,33,34,36,67 history of mental illness,33,34 and increased alcohol consumption16 experienced poorer mental health outcomes. Low psychological resilience and worse perceived self-efficacy were associated with worse mental health,21,32 and increased attention paid to negative information about the pandemic were also associated with worse outcomes.12,61 One multinational study in Singapore and India found that presence of physical symptoms was associated with significantly worse anxiety, depression, stress, and post-traumatic stress disorder (PTSD).11 One small study in China found that lack of knowledge about COVID-19 was associated with worse mental health outcomes,32 and another small study in Ecuador found that belief in conspiracy theories surrounding the origin of COVID-19 was associated with worse mental health in HCWs.68
Social supports
Mental health outcomes were poorer in HCWs who were only children,63 reported loneliness,13,16,38 had children of their own,34,69 lived in rural areas,36 and felt lack of family support.12,32,49
Previous epidemic exposure
A single-institution study conducted in Saudi Arabia surveyed HCWs in February prior to any documented COVID cases in the country and found moderate to severe anxiety in over 31.8% of HCWs.70 Additionally, 41.5% of HCWs were more stressed about COVID-19 than they had about the previous MERS-CoV SARS outbreak in 2002-2003.
Protective factors for mental health
Social support was found to be a protective factor for mental health in HCWs in several studies,9,23,27,51,71 including one study which found that personal resilience mediated the relationship between social support and mental health.9 Further, greater support at work was found to mitigate adverse mental health outcomes in one multicenter study in the United States,72 and a large single-institution study in China found that increased perception of institutional and administrative support, as well as satisfaction with PPE, were associated with less stress among HCWs.33 Several other studies also found that adequate access to PPE was associated with better mental health outcomes.37,41 In one large multicenter study in China, HCWs receiving psychological support were significantly less likely to report adverse mental health outcomes.15 HCWs with higher psychological resilience,21 more frequent exercise,28,34 higher education level,37,42 physicians,42 more knowledge about COVID-19,43 and HCWs working in private hospitals in Iran37 were found to have better mental health.
Sleep quality
Numerous studies in this review specifically assessed sleep and risk factors for poor sleep quality in HCWs. Sleep quality was related to anxiety, depression and PTS in several studies.19,32,61,73,74,75,76 Sleep quality was also found to mediate the association between COVID-19 exposure level and PTS symptoms8 as well as the association between occupational stress and anxiety.48 Improved sleep quality was found in HCWs with adequate social support.71 HCWs reported more sleep disturbances than non-HCWs in several studies,41,77,78 as well as worse sleep in frontline HCWs compared to non-frontline HCWs78,79 and worse sleep in medical HCWs compared to non-medical HCWs.36 Risk factors for worse sleep quality include nurses,26,39 HCWs working in Wuhan, China,55 working in a COVID-designated hospital or COVID isolation unit,52,80 fear about infection and uncertainty about epidemic control,80 lack of psychological support,80 health care assistants,39 direct contact with COVID patients,74 being an only child,74 and having a colleague die due to COVID-19.39
Acute traumatic stress and PTS symptoms
The presence of acute traumatic stress and PTS symptoms in HCWs was assessed in numerous studies in this review. Nonmedical HCWs were found to have increased PTS compared to medical HCWs in one study in Singapore, although the overall prevalence of PTS was much lower at 7.7% compared to other studies.10 Risk factors for increased PTS symptoms included working in a COVID-designated hospital or ward,40,52 working in a region with more COVID cases,42 direct contact with COVID patients,8 women,40,42 older HCWs,40,57 quarantined HCWs,57 frontline HCWs,39 general practitioners,39 having a colleague be hospitalized or die from COVID,39 anxiety about COVID infection,81 exhaustion,81 and working night shifts.42 A single-institution study of physicians in the United States found higher PTS symptoms in HCWs with more inpatient shifts, higher perceived workplace stress, and increased sleep difficulties, although the study also found that greater frequency of shift work was protective of PTS.76 A multicenter study of 349 otolaryngology physicians in the United States found 27.5% reported moderate to severe PTS.44
Burnout
A large multicenter study of 1422 HCWs in Spain found 41.1% prevalence of burnout, with burnout positively and significantly related to anxiety, depression and PTS symptoms.42 Risk factors for burnout identified in this review included women HCWs,44,82 nurses,82 direct contact with COVID patients,45 fear of infection,27 increased work stress,27 and presence of somatic symptoms.82 In a single-institution study in China, burnout was significantly lower in frontline HCWs compared to non-frontline HCWs.83 However, in a multicenter study of trainee physicians in the United States, frontline trainees had higher burnout scores than non-frontline trainees.59 Burnout scores in trainees varied depending on the specialty studied, with lower burnout scores in surgery residents in a single-center study in Pakistan compared to before the pandemic, likely due to less work-hours,84 but higher burnout scores in otolaryngology residents compared to attending physicians in a multicenter study in the United States.44
Secondary traumatic stress and vicarious traumatization
Several studies specifically assessed vicarious traumatization, also known as secondary traumatic stress, in HCWs. One multicenter study in China compared vicarious traumatization scores of 214 non-HCW citizens with 526 nurses and found that the general public and non-frontline nurses had higher vicarious traumatization scores than frontline nurses.85 This is contrary to a multicenter study in Turkey, which also compared 312 citizens with 251 HCWs and found worse secondary traumatic stress scores in frontline HCWs compared to non-frontline HCWs and the general public.20 This study also found worse secondary traumatic stress in HCWs who were women, early in their careers, living with parents, had a chronic disease, and reported increased social media use.20 Another multicenter study of 339 psychotherapy HCWs in the United States found 77.6% of them had at least moderate vicarious trauma, with higher trauma scores in younger and early-career therapists.86
Moral distress and injury
One single-institution study in the United States specifically assessed moral injury in 219 HCWs, specifically trainees and attending physicians.76 This study found that a higher proportion of inpatient time and insomnia were associated with higher moral injury, while a supportive workplace environment was associated with less moral injury.
Longitudinal assessments of mental health
There were two studies which performed longitudinal assessments of mental health, both performed in China. In the first single-institution study, 60 HCWs were surveyed during the outbreak from January to February 2020, and then 60 different HCWs were surveyed after the outbreak in March 2020.87 The study found that mental health outcomes were worse during the outbreak compared to the post-outbreak period. A similar single-institution study surveyed 92 nurses after they had worked 7-10 days in COVID isolation wards and compared them to 86 nurses after they had worked 2 months in isolation wards.88 This study also found that mental health outcomes were worse earlier during the outbreak, and additionally found that there were different stressors and mental health needs by HCWs during both time periods.
Comparison between medical HCWs, nonmedical HCWs, and non-HCWs
Studies which compared mental health outcomes of HCWs with non-HCWs generally found that HCWs had worse outcomes than non-HCWs in the general population, including in China,49 Poland,41 Saudi Arabia,18 and Turkey.25 However, a study in Colombia found similar rates of stress between HCWs and other professions,89 a study in Spain found no difference in anxiety and depression between HCWs and non-HCWs, but did find higher acute stress in HCWs,24 and a study in India found no difference in psychological distress in HCWs compared to non-HCWs.90 Several studies also compared medical HCWs with non-medical HCWs. A large multicenter study of 2182 HCWs in China found higher anxiety, depression, and insomnia among medical HCWs,36 with similar findings of higher fear and anxiety in medical HCWs as compared to non-medical HCWs in another large multicenter study of 2299 HCWs in China.13 This is contrary to a multicenter study of 470 HCWs in Singapore which found higher anxiety, stress and PTS among non-medical HCWs compared to medical HCWs.10 This was also demonstrated in a single-center study of 240 HCWs in Ireland, which found higher anxiety and depression scores were in administrators compared to medical HCWs.38 A multicenter study of 122 laboratory HCWs in Singapore found high rates of depression, anxiety and fear among laboratory technicians, and also found that previous experience handling high-risk specimens during the previous SARS outbreak did not influence mental health outcomes.75
Interventional studies
There was only one interventional study identified in this review that assessed mental health using a validated instrument. The study is a pilot study at a single institution in Iran of 10 HCWs who participated in online Balint groups.91 The study found that mean anxiety and resilience scores significantly improved after the online Balint groups.
Discussion
This rapid review describes risk factors for various adverse mental health outcomes among HCWs during the ongoing COVID-19 pandemic, as well as supportive measures which may mitigate these risks. There is clearly a dire need for effective mental health interventions as new outbreaks develop and HCWs incur repetitive trauma, and further study on other HCW-specific sources of stress, including burnout and moral injury, will be required to comprehensively describe the acute and long-term mental health effects of COVID-19.
The vast majority of studies in this review were cross-sectional survey-based studies that assessed mental health, predominantly anxiety, depression, and acute stress, at a single point in time during the early pandemic. As shown in Table 1, there is large between-study heterogeneity in these mental health outcomes, likely due to the wide variety of validated instruments used as well as different definitions or score cutoffs that defined mental illness in each study. There was relatively high prevalence of clinical anxiety and depression among HCWs, with rates appearing to increase in countries other than China as the pandemic continued from March onwards.
Although these cross-sectional studies identified important risk factors, they do not assess how these risk factors or mental health outcomes may change over time. There were only two studies which collected longitudinal data,87,88 and both demonstrated poor mental health among HCWs during the main outbreak in China compared to the post-outbreak period. This phenomenon has been previously demonstrated in longitudinal studies during other epidemics,92,93 with research from the SARS era finding that frontline HCWs suffered increased stress up to 1 year after the epidemic compared to non-frontline HCWs.94 Future longitudinal studies are necessary as the COVID-19 pandemic continues, as the effect of prolonged trauma on HCWs, including repeated cycles of outbreaks and recovery, is not known.
As shown in Table 2, there are considerable similarities between risk factors for poor mental health during COVID-19 and previous epidemics such as SARS, including the important role of adequate training, access to PPE, and clear communication in protecting mental health.92,95 However, there are also some key differences, as illustrated in this review. Previous research by Chong et al. modeled two distinct psychological phases of HCWs workers during the SARS outbreak in Taiwan: an initial shock and reaction phase, when SARS cases were exponentially growing, and a repair and reorientation phase, when the outbreak was brought under control.96 Each phase had distinct psychological findings in HCWs, with anxiety predominating in the initial phase due to feelings of vulnerability, loss of control, high job-related stress, and perceived threat from lack of safeguards and personal protective equipment. The repair and reorientation phase revealed predominant depression and PTS symptomatology, including avoidance, intrusion, and interpersonal difficulty, with many workers considering resigning during this phase. This landmark study demonstrated that, due to different psychopathologies in HCWs at different phases of epidemics, mental health interventions must be comprehensive to address the changing needs of workers as the pandemic progresses. However, studies from the COVID era have demonstrated high prevalence of anxiety in HCWs in Saudi Arabia70 and Iran6 before the pandemic reached those countries, suggesting that there may be an antecedent phase of anticipatory anxiety or stress in pandemics that may be amenable to prophylactic intervention to prevent worsening mental health. High prevalence of anticipatory anxiety was not universally demonstrated in this review, with much lower rates of pre-pandemic anxiety in Singapore10,11 which may be due to their previous experience with the SARS epidemic.
Quarantine increased the risk of PTSD and mental illness during the SARS epidemic,97,98 but findings have been more mixed in the COVID-19 literature, possibly due to reduction of quarantine-related stigma for HCWs as widespread community-level quarantine was used during the initial pandemic. Although burnout was not as extensively studied in the literature at the time of the SARS epidemic, studies found worse burnout in frontline HCWs during SARS,92 which was redemonstrated in the COVID-19 era in this review. Only a minority of studies specifically studied burnout, as well as other traumatic exposures such as moral injury and vicarious traumatization, which limits conclusions about how those psychological phenomena may affect HCWs. Moral injury in particular suffers from a lack of validated instruments in HCWs, and there are not currently well-described approaches to treating moral injury in HCWs, with further study needed.99,100
Access to mental health services and psychological support were found to be protective of adverse mental health outcomes in this review, although there is a suggestion that frontline HCWs may not seek out or receive mental health treatment despite their higher rates of mental illness.5 This may represent an unmet need for this at-risk population that is amenable to targeted organizational interventions. Several studies in this review also found that higher personal resilience was protective of mental health, including that resilience may mediate the relationship between psychosocial support and mental health.9 The sole interventional study in this review found improved anxiety and personal resilience after exposure to online Balint groups,91 also suggesting that mental health is interrelated with resilience. These findings have important implications in designing mental health support programs, as a multipronged approach with organizational-level and individual-level interventions is required.
Evidence-based mental health frameworks
The present review only identified one interventional study which used a validated mental health instrument to study the effects of a mental health program on HCWs. With few COVID-specific interventional studies to guide mental health support for HCWs, the following evidence-based mental health frameworks, many based on previous epidemics which share similarities to COVID-19, can serve as models to execute and study novel mental health interventions.
Psychological First Aid
Psychological First Aid (PFA) was developed by the National Center for PTSD in 2006 after it was recognized that traditional trauma debriefing interventions, such as critical incident stress debriefing, did not promote recovery from traumatic incidents and in fact may increase the risk of PTSD.101,102 PFA was based on the observation that most psychological responses to mass trauma are appropriate reactions to distressing situations rather than psychiatric illness, and that social support can mitigate this distress.103 As such, PFA involves empowering traumatized persons with safety, promotion of self-efficacy, calmness, social connectedness, and optimism, and is designed to be implemented by HCWs or the general public.102 PFA is promoted by multiple mental health organizations as an evidence-based approach to supporting HCWs in crisis, although a systematic review did not find strong evidence of its risks or benefits.104 Further, because PFA was designed based on the experience of mass casualty or mass trauma incidents, it is unclear if PFA will be effective for repetitive stressors during a pandemic.105 A brief PFA model has been developed in Malaysia and implemented with HCWs, although quantitative data are currently lacking.106,107
Stress Continuum Model and Stress First Aid
With increasing literature suggesting that traumatic stressors are frequently not due to a single event but are instead longitudinal and cumulative in nature, a related psychological support framework was developed by the United States military and called Stress First Aid (SFA).108 Unlike PFA, SFA is embedded in a larger Stress Continuum Model which recognizes that traumatized individuals exist on a spectrum of appropriate reactive distress to frank mental illness, and may move along that spectrum as they are exposed to different stressors.108 Further, SFA is specifically designed as a peer-to-peer model, and informed the creation of a COVID-19-specific peer-to-peer Battle Buddies intervention with HCWs that is currently under study.109 Although there is little research on the efficacy of these models, the findings in this review that mental health outcomes are extremely variable, that there are myriad risk factors which differ based on type of HCW and other personal or professional characteristics, and that social support mitigates the risk of adverse outcomes, suggests that SFA as a comprehensive psychosocial support model may effectively address the needs of the majority of stressed HCWs.
Personal resilience training
As low psychological resilience and perceived self-efficacy were associated with worse mental outcomes in this review, study of interventions that build personal resilience in HCWs are warranted. Several computer-based resilience training modules were developed in Toronto after the SARS epidemic, with low-quality evidence of improvement in mental health with these modules.110
Organizational resilience and organizational justice
Findings from the SARS epidemic that mental health of HCWs was improved when they were provided with adequate training and protective equipment, organizational support, and clear communication from leadership led to the conceptualization of organizational resilience or organizational justice.110,111 These frameworks are considered a critical component of pre-pandemic planning, and involve establishment of crisis protocols that provide for the practical and physical needs of HCWs as well as their mental health needs.112 These include equitable access to sleep facilities, childcare, food, and psychological support services, in which leadership ensures that HCWs voices are compassionately heard in all decision-making procedures throughout the pandemic. Further, given that lack of information about COVID-19 and increased attention paid to negative information about the pandemic are associated with worse mental health, timely and supportive crisis communication by leadership is felt to be vital in supporting HCWs.113
Cognitive behavioral therapy and mindfulness
Various cognitive behavioral therapy (CBT) approaches to supporting the mental health of HCWs have been developed, including the Accelerated Recovery Program,114 which has demonstrated efficacy in reducing compassion fatigue, burnout, and secondary traumatization.115,116 A systematic review of randomized controlled trials has confirmed that CBT and mindfulness improve stress, anxiety and depression in HCWs117 and CBT-informed interventions for HCWs during COVID-19 have been proposed.105 Although these interventions are efficacious, further study on how they can be incorporated into larger organizational mental health frameworks is warranted.
Strengths and limitations
Strengths of this rapid review include a broad initial query for all studies on the mental health of HCWs during the COVID-19 pandemic, as well as only including studies that utilized validated mental health instruments. Further, approximately half of the countries represented in this review were outside of China, which enhances the external validity of the review. Limitations include the intrinsic variability and heterogeneity of outcomes and mental health instruments utilized across studies, wide variation in the sample sizes and inclusion of studies with low power, and utilization of only one database. Interventional studies were poorly represented in this review, and future reviews will be required to capture new interventional studies as they are published.
Conclusions
Research from previous epidemics as well as during the current COVID-19 pandemic suggests that HCWs experience disproportionately poor mental health outcomes compared to the general population, particularly among HCWs working in frontline and high-risk environments.
Although this review captures a large body of literature that robustly describes cross-sectional data on risk factors for adverse mental health outcomes in HCWs across multiple countries, there is limited research on the longitudinal effects of the present pandemic, although longitudinal studies are currently ongoing.118 The use of validated mental health instruments is vital, and development of novel instruments for moral injury, secondary traumatic stress, and vicarious traumatization is warranted to elucidate how these phenomena may be affecting HCWs. Further, there is a dearth of literature on interventions that can quantitatively improve mental health outcomes. The heterogeneity of the literature suggests that mental health interventions for HCWs cannot be one size fits all, and must incorporate multifaceted organizational- and individual-level programs that flexibly address the spectrum of acute and chronic stress to which different HCWs are exposed as the pandemic continues.
Data Availability
Not applicable.
Declaration of interest statement
The authors do not have any conflicts of interest to declare.
Funding sources
There are no funding sources to declare.
Acknowledgements
None to declare.
Footnotes
Twitter @majorajay
Twitter @FayUCCancerCr
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵



