
Abstract
Background The interaction between COVID-19, non-communicable diseases, and chronic infectious diseases such as HIV and tuberculosis (TB) are unclear, particularly in low- and middle-income countries (LMIC) in Africa. We investigated this interaction using a nationally representative hospital surveillance system in South Africa.
Methods A national surveillance system for laboratory-confirmed COVID-19 hospital admissions (DATCOV) was established. Using DATCOV data, we describe the demographic characteristics, clinical features, and in-hospital mortality among individuals admitted to public and private hospitals with COVID-19 during 5 March to 11 August 2020. Multivariable logistic regression models were used to assess the role of HIV-status, underlying comorbidities and their interaction on in-hospital COVID-19-associated mortality.
Findings Among the 41,877 individuals admitted with laboratory-confirmed COVID-19, hospital admissions peaked at 1,560 admissions per day, in late July and 7,662 (18.3%) died. Comorbidities were documented in 27,555 (65.8%) individuals, most commonly observed were hypertension (36.8%), diabetes (29.6%), obesity (19.7%), and HIV (8.7%); TB was reported in 0.7% of individuals. Increased risk of in-hospital mortality was associated with HIV and TB, as well as other described risk factors for COVID-19, such as increasing age, male sex, non-White race (Black, mixed and Indian race), chronic underlying conditions particularly hypertension, diabetes and obesity. In particular, HIV-infected individuals with immunosuppression had increased risk of mortality (adjusted odds ratio 2.2; 95% confidence interval 1.6-3.1). Among HIV-infected individuals, the prevalence of other comorbidities associated with severe COVID-19 outcomes was 39.9%. The effect of one or more comorbidities on mortality was similar in HIV-infected and -uninfected individuals.
Interpretation These data provide a better understanding of the interaction of non-communicable diseases, chronic infectious diseases like HIV and TB and COVID-19. Increasing age and presence of chronic underlying comorbidities (particularly hypertension and diabetes) are important additional factors associated with COVID-19 mortality in a middle-income African setting and are common among HIV-infected individuals. HIV- and TB-infected individuals, particularly those with additional comorbidities, would benefit from COVID-19 prevention and treatment programmes.
Funding DATCOV is funded by the National Institute for Communicable Diseases (NICD) and the South African National Government. No additional funding was obtained towards the completion of this analysis and the development of this manuscript.
Research in context
Evidence before this study
Evidence before this study Since the emergence of the COVID-19 pandemic, studies from Brazil, China, India, Iran, United States and several countries in Europe have identified older age, male sex and presence of underlying comorbidities including hypertension, heart disease and diabetes as risk factors for severe disease and death. There are very few studies, however, carried out in low- and middle-income countries (LMIC) in Africa, many of whom have high poverty rates, limited access to healthcare, and high prevalence of chronic communicable diseases, such as HIV and tuberculosis (TB). Data are also limited from settings with limited access to HIV treatment programmes. Early small cohort studies mainly from high income countries were not conclusive on whether HIV or TB are risk factors for disease severity and death in COVID-19 patients. Recent large studies from South Africa’s Western Cape province and the United Kingdom (UK) have found HIV-infected individuals to have a moderately increased risk of COVID-19 associated mortality. However, the UK reported risk among all confirmed cases while data from the Western Cape suggested an increase in both all confirmed cases and those admitted to hospital. Of these, only the Western Cape study presented data on mortality risk associated with presence of high viral load or immunosuppression, and found similar levels of severity irrespective of these factors. No studies reported on the interaction between HIV-infection and other non-communicable comorbidities on COVID-19 associated mortality.
We performed separate literature searches on PubMed using the following terms: “COVID-19” “death risk factors” and “mortality”; “HIV” “COVID-19” and “mortality”; “TB”, “COVID-19” and “mortality”. All searches included publications from December 2019 until July 12, 2020 without language restrictions. Pooled together, we identified 232 published papers. Additionally, we performed two literature searches on MedRxiv using the terms “HIV”, “COVID-19” and “mortality”, and “TB”, “COVID-19” and “mortality” from April 25 until July 12, 2020 without language restrictions. Pooled together, we identified six pre-prints.
Added value of this study
Added value of this study Among a large national cohort of over 40,000 individuals hospitalised with COVID-19 in a high HIV and TB prevalence setting, we found that HIV and TB were associated with a moderately increased risk of in-hospital mortality. We found increasing risk of mortality among HIV-infected individuals with moderate/severe immunosuppression compared to those without immunosuppression. Among HIV-infected individuals, the prevalence of other comorbidities was high (40%) and the effect of increasing numbers of comorbidities on mortality was similar in HIV-infected and -uninfected individuals. Our study included HIV-infected individuals from all provinces in the country with varying levels of access to HIV treatment programmes. Other risk factors described elsewhere in the world such as increasing age, obesity and chronic underlying illness (particularly hypertension and diabetes) were also associated with increased mortality in this cohort.
Implications of all the available evidence
Implications of all the available evidence The evidence suggests that HIV- and TB-infected individuals should be prioritised for COVID-19 prevention and treatment programmes, particularly those with additional comorbidities. Increasing age and presence of chronic underlying illness (particularly hypertension and diabetes) are important additional factors associated with COVID-19 mortality in a middle-income African setting and are common among HIV-infected individuals.
Introduction
The first case of COVID-19 was documented in South Africa on 5 March 2020. By late July 2020, the country had risen to fifth in the global rank of cumulative cases, peaking at around 17,000 new confirmed cases per day. (1) Worldwide, the severity of COVID-19 morbidity and mortality has been linked to older age over 65 years, male sex, and underlying medical conditions. (2-9) The most common comorbidities reported among patients with severe COVID-19 are hypertension, heart disease, diabetes, cancer, chronic pulmonary disease, obesity, and kidney disease. (6, 10-12) Race or ethnicity and poverty are associated with increased risk of severe illness and death in COVID-19 cases. (13, 14)
Case fatality among laboratory-confirmed COVID-19 cases has varied from country to country and even within countries. For example, the in-hospital mortality rate ranges from 24% in Germany, 30-32% in the United Kingdom, and 23-43% in Brazil (15-17). A study from the Democratic Republic of Congo reported an in-hospital mortality of 13% (18). This variability could reflect the testing strategy, age distribution, prevalence of comorbidities in the population, definition of COVID-19-related deaths, death reporting and access to quality healthcare. (7, 19-21)
Characterizing populations disproportionately affected by COVID-19 mortality is important for prioritization of interventions, particularly in low- and middle-income countries (LMIC) where resources are limited. However, available data on risk factors for severe COVID-19 disease, including mortality, are mostly from high-income countries. High poverty rates, limited access to healthcare and high prevalence of chronic communicable diseases such as HIV and TB, likely affects disease severity and the burden of COVID-19 on the healthcare system and society in LMICs. (22)
South Africa is a LMIC country with coinciding epidemics of non-communicable diseases (NCD), obesity and chronic infectious diseases (HIV and TB). According to the 2016 Demographic and Health Survey 41% of adult women and 11% of men were obese, 46% of women and 44% of men were hypertensive, and 13% of women and 8% of men had diabetes. (23) South Africa also has high rates of poverty, with unemployment rates of 30% prior to the pandemic. (24-27) Additionally, only 5% of the population in South Africa is over the age of 65 years, compared to 9% in Brazil and 18% in the United Kingdom. (28, 29) Furthermore, South Africa has a high burden of the co-epidemic of HIV and TB. In 2019, there were 7.5 million people estimated to be living with HIV in South Africa, of which 2.3 million (31%) were eligible but not receiving treatment. (30) In 2018, 301,000 new cases of TB were diagnosed in South Africa. (31)
Understanding whether underlying medical conditions such as HIV and TB are associated with more severe outcomes among individuals hospitalised with COVID-19 is of critical importance for South Africa and other countries in the region with large HIV and/or TB epidemics. Early studies from high income countries with relatively small numbers of HIV-infected people did not find HIV to be a risk factor for severe COVID-19 disease. (32, 33) However, more recent data from the Western Cape Province of South Africa, and the UK found HIV-infected individuals to have an increased risk of COVID-associated mortality but no apparent association between increasing immunosuppression and mortality. (34, 35) Additionally, the interaction between other comorbidities, HIV infection, and COVID-19 mortality is not well described.
In this paper, we examine the role of HIV (including the level of immunosuppression) and comorbidities, and their interaction on COVID-19 mortality using data collected from a national surveillance programme in South Africa from 5 March to 11 August 2020.
Methods
Study setting and data sources
South Africa is administratively divided into nine provinces. Provincial authority is decentralized to lower administrative levels of districts and sub-districts. South Africa has a dual health system with a publicly funded district health system, that serves approximately 84% of the population, and a private health system largely funded by private health insurance schemes. (36)
In the absence of existing hospital surveillance systems, the National Institute for Communicable Diseases (NICD) established DATCOV as a national surveillance system for COVID-19 hospitalizations on 1 April 2020. Although DATCOV initially included only a few participating hospitals, (37) it was adopted for national implementation following South African government endorsement on 15 July 2020. By 11 August 2020, a total of 144 public-sector hospitals (42% of public-sector hospitals) and 236 private-sector hospitals (100% of private hospitals) have reported COVID-19 hospitalisations on DATCOV. The system allows public and private sector hospitals to submit data on hospital admissions for patients diagnosed with COVID-19. The programme aims to monitor trends in COVID-19 admissions and describe the epidemiology of COVID-19 among hospitalised patients in South Africa, to enable appropriate allocation of resources.
Data collection and management
The data collection form was adapted from the World Health Organization (WHO) COVID-19 case reporting tool, (38) recording the following variables: demographic data, exposures such as occupation, and potential risk factors such as obesity, comorbid disease(s), and pregnancy status. Additional variables included level of treatment (ward, high dependency, or intensive care unit), complications, treatment, and outcomes of the hospital admission (discharged, transferred out to another hospital, or died).
Potential risk factors and covariates
Age, sex, race, and comorbidities (hypertension, diabetes, chronic cardiac disease, asthma, other chronic respiratory disease, chronic renal disease, malignancy in the past five years, HIV and past and current TB) were considered as potential risk factors for COVID-19 in-hospital mortality. The presence of comorbidities was recorded by the clinician on DATCOV based on the comorbidity being noted in the patient’s clinical record. Obesity was not consistently recorded and was based on the subjective opinion of the attending healthcare worker. HIV status was assessed by confirmation of previous HIV rapid, ELISA, or PCR test result; and ART status was ascertained from data submitted by the hospital. The level of virological control or immunosuppression was assessed based on available viral load result within the past year and categorised as virologically suppressed (HIV-RNA<1,000 copies/ml) or as viraemic (HIV-RNA≥1,000 copies/ml); and immune reconstituted (CD4 count≥200 cells/μl) or immunosuppressed (CD4 count<200 cells/μl). (39) CD4 count is no longer routinely performed on all patients, as per South African HIV care guidelines. In-hospital mortality was defined as a death related to complications from COVID-19 that occurred during the hospital stay and excluded deaths that occurred due to other causes or after discharge from hospital.
Study population
We download data from DATCOV on all individuals who had a positive reverse transcription polymerase chain reaction (RT-PCR) assay for SARS-CoV-2, with a confirmed duration of stay in hospital of one full day or longer regardless of age or reason for admission. Because the main outcome of the study was in-hospital mortality, all analyses were implemented among COVID-19 hospitalised patients with a known in-hospital outcome (i.e. discharged alive or died) at the time of data extraction (11 August 2020). Individuals determined by a medical panel to have died of other causes, patients transferred to other facilities for continuing care or patients who were residents in long-term facilities and psychiatric hospitals rather than acute hospital admissions were excluded from the analysis.
Statistical analysis
For the main analysis, to account for incomplete data on selected variables, we used chained equation multiple imputations (which allows for the simultaneous imputation of multiple variables with missing values) and generated ten complete imputed datasets that were used for subsequent analyses. Incomplete variables included in the imputation chain were: age, sex, race, month of admission and comorbidities such as HIV and TB infection, hypertension, diabetes, asthma, malignancy and chronic pulmonary, cardiac and renal diseases. ART, HIV viral load and CD4 counts were also incomplete and were conditionally imputed only among HIV-positive patients (either with observed or imputed HIV status). Complete variables included in the imputation process were province, health sector (i.e. public or private) and in-hospital outcome (i.e. discharged alive or died). Descriptive statistics such as frequencies and percentages were used for categorical variables, and continuous variables were expressed as mean with standard deviation (SD) or median and interquartile range (IQR) on the imputed datasets.
We implemented post-imputation random effect (on admission facility) multivariable logistic regression models to: (i) compare individuals who were HIV-infected and HIV-uninfected; (ii) determine the factors associated with in-hospital mortality, including ART, HIV viral load and CD4 count among HIV-positive individuals; and (iii) evaluate the combined effect of multiple non-HIV comorbidities on COVID-19 in hospital mortality. A combined comorbidity variable categorised absence, one, two, and three or more comorbidities among those that were individually significantly associated with in-hospital mortality in model (ii) above. We evaluated the effect of multiple comorbidities among any patient and among HIV-infected and HIV-uninfected patients separately through stratification by HIV infection status. In addition, we assessed potential differential effect (through the inclusion of an interaction term) of multiple comorbidities on in-hospital mortality between HIV-infected and HIV-uninfected individuals.
A random effect on admission facility was included for all analyses to account for potential differences in the service population and the quality of care at each facility. For each multivariable model we assessed all variables that were significant at p<0.2 on univariate analysis and dropped non-significant factors (p≥0.05) with manual backward elimination. Pairwise interactions were assessed by inclusion of product terms for all variables remaining in the final multivariable additive model. We also reported the univariate association of all covariates evaluated in the analyses described above to the main outcomes (i.e. HIV infection or in-hospital mortality) using non-imputed data. The statistical analysis was implemented using Stata 15 (Stata Corp®, College Station, Texas, USA).
Ethical considerations
The Human Research Ethics Committee (Medical), University of the Witwatersrand, approved the project protocol as part of a national surveillance program (M160667). This activity was reviewed by the U.S. Centers for Disease Control and Prevention (CDC) and was conducted consistent with applicable federal law and CDC policy. All personal identifying information was de-linked for our analysis and stored in a secure server.
Results
Study population
From 5 March to 11 August 2020, 49,554 individuals were admitted with a laboratory-confirmed diagnosis of COVID-19 and reported to DATCOV. Of these individuals, 41,877 met the inclusion criteria for the analysis (Figure 1). The percent of missing data for the imputed variables ranged between <0.1% to 15.1% except for race (52.6%), obesity (84.7%), and HIV-specific variables (Table S1).
Missing data and characteristics of COVID-19 hospitalised patients reported to DATCOV, 5 March-11 August 2020, DATCOV, South Africa.
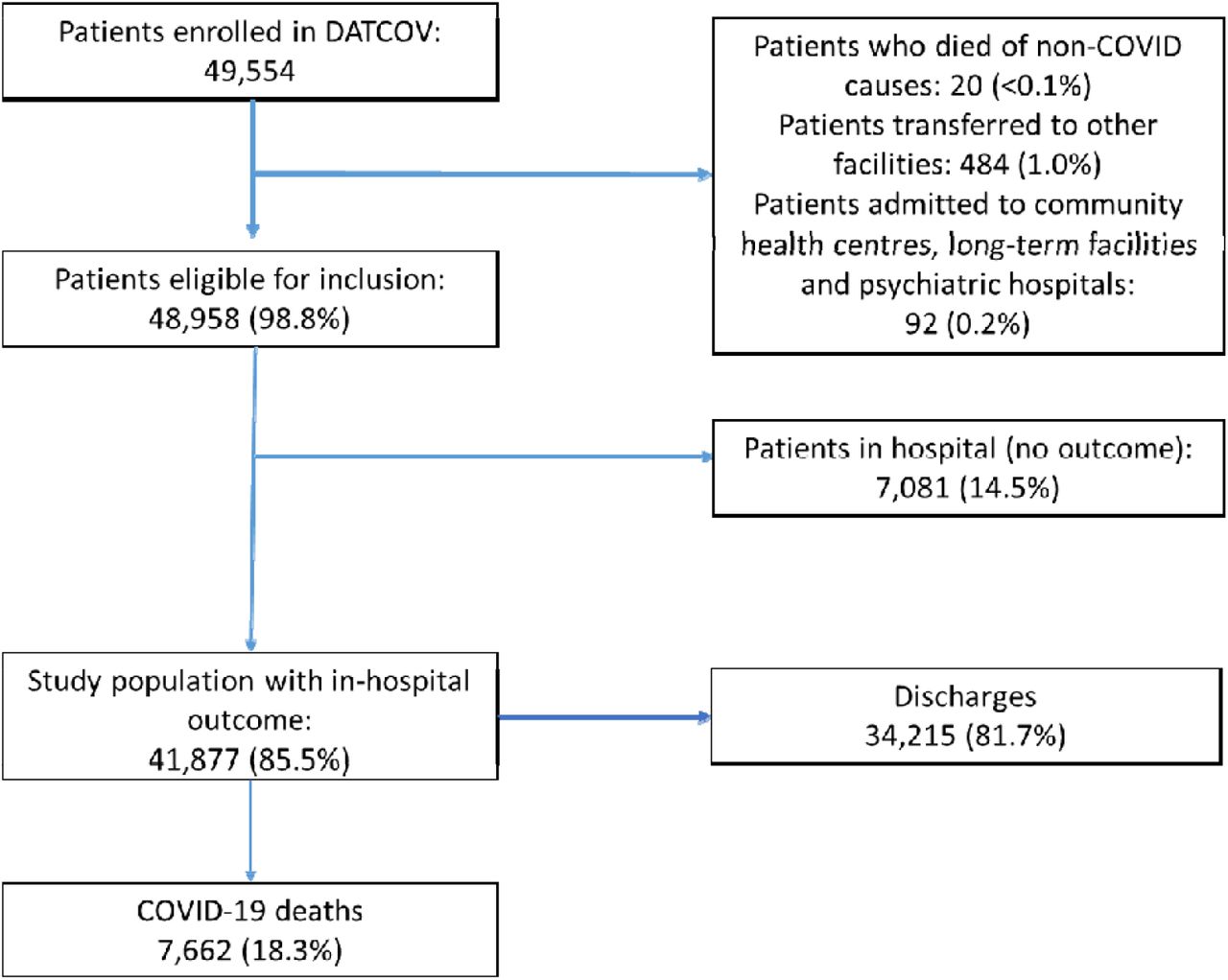
Flow diagram of cohort with numbers excluded at different stages and identification of cases for the main endpoints, 5 March-11 August 2020, DATCOV, South Africa.
The number of hospital admissions increased in both the public and private health sectors, peaking at 1,560 admissions per day in late July (Figure 2). The median age of COVID-19 admissions included in the analysis with available data (n=41,845) was 52 years (interquartile range [IQR] 40 – 63) and 54.4% of patients (22,755/41,862) were female (Table S1). Race information was available for 19,777 (47.2%) patients. Of these patients, 13,444 (68.0%) were black. The public sector accounted for 31.5% (13,208/41,877) of hospitalisations reported to DATCOV. Most admissions (86.3%; 36,128/41,877) were recorded by hospitals in four provinces, namely Western Cape, Gauteng, KwaZulu-Natal and Eastern Cape. The median time from symptom onset to hospital admission was 2 days (IQR 1-4 days). The median duration of hospital admission was 6 days (IQR 3-10 days).

Number of reported COVID-19 admissions by health sector and epidemiological week of diagnosis among 380 hospitals reporting to DATCOV, 5 March-11 August 2020, South Africa (n=41,877) Note: right weeks censored as only individuals with in-hospital outcome were included
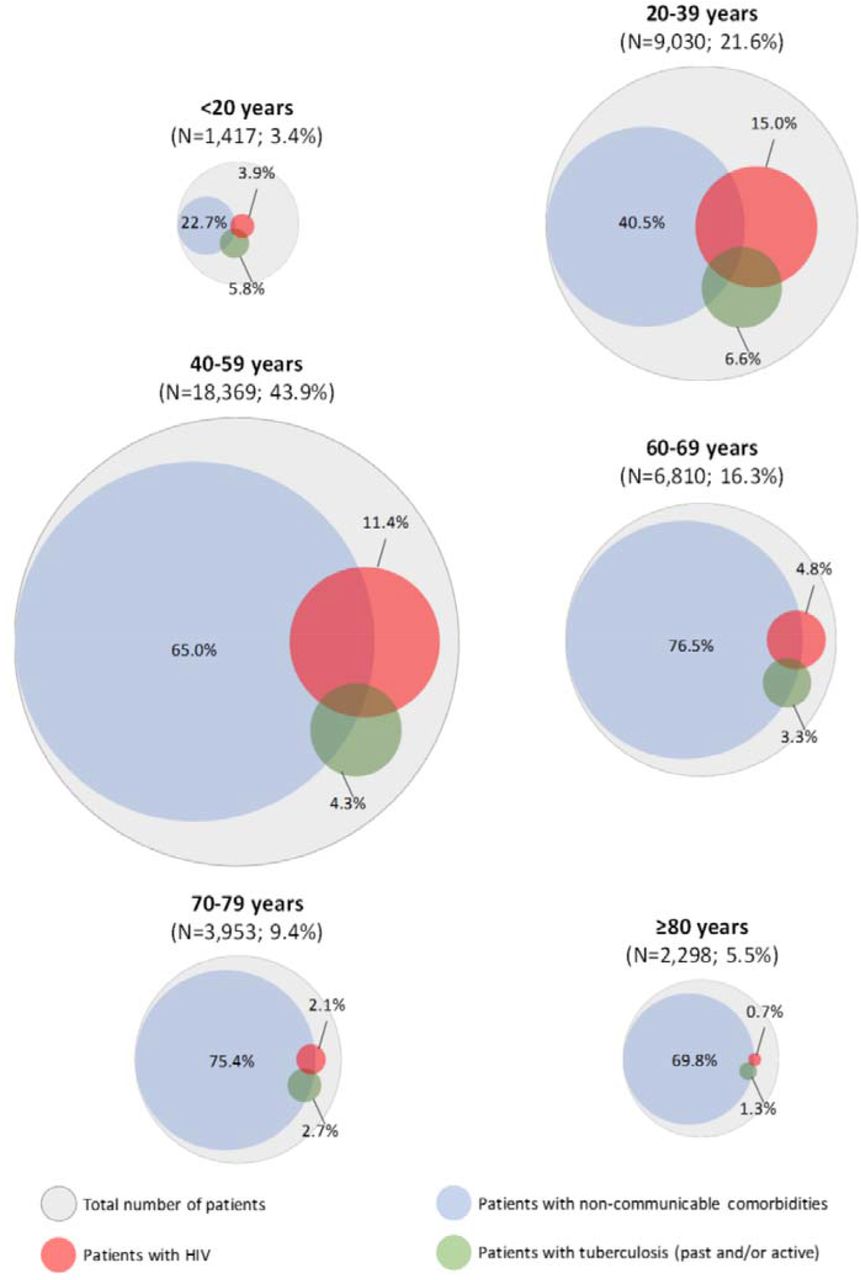
Following multiple imputation, the estimated proportion of individuals reporting at least one comorbidity was 65.8% (95%CI: 65.2%-66.4%) The most prevalent comorbidities were hypertension (36.9%; 13,189/35,789), diabetes (29.6%; 10,603/35,790), obesity (19.7%; 1,039/5,277), and HIV (8.7%; 3,077/35,550). The prevalence of non-communicable comorbidities increased with age, while HIV and TB were most prevalent in individuals aged 20–59 years (Figure 3).

Estimated prevalence of comorbid conditions for COVID-19 hospitalisations by age, 5 March-11 August 2020, DATCOV, South Africa. Note: The percentage of patients within each age group is expressed over the total number of patients included in the analysis (41,877). The circle’s size is proportional to the number of patients it represents. Inner circles represent a sub-population (with prevalence expressed as percentage) of the outer circle. Overlapping circles represent co-infections and comorbidities (e.g., HIV and past/active TB and/or non-communicable comorbidities).
Factors associated with HIV infection
Of 35,550 hospitalised patients with available data on HIV, 3,077 (8.7%) were living with HIV (Table 1). The HIV prevalence was 20.2% in the public sector and was 4.0% in the private sector (age-specific HIV prevalence for public and private sector presented in Table S2). Of HIV-infected individuals with available data, 99.5% (1,271/1,278) were receiving ART, 16.9% (189/1,120) were viraemic (HIV-RNA≥1000 copies/ml) and 28.8% (401/1,390) were immunosuppressed (CD4 count<200 cells/μl).
HIV prevalence amongst COVID-19 hospitalized patients of different age groups reported to DATCOV, in the public and private health sectors, 5 March-11 August 2020, South Africa.
Characteristics of HIV-infected and -uninfected individuals with laboratory-confirmed severe acute respiratory syndrome coronavirus-2 admitted to hospital, 5 March-11 August 2020, DATCOV, South Africa (N=41,877)
Compared to HIV-uninfected COVID-19 hospitalised patients, HIV-infected individuals were more likely to be aged 20-69 years, female, black, admitted in the public health sector, to have comorbid chronic cardiac and renal disease, malignancy, have previous and/or current TB, and to die in hospital; but they were less likely to have comorbid hypertension, diabetes, chronic pulmonary disease, or asthma. The HIV prevalence of COVID-19 patients varied by province (Table 1 and Figure 4). The in-hospital case-fatality ratio (CFR) was higher for HIV-infected (644/3,077 [20.9%]) compared to HIV-uninfected individuals (6,122/32,473 [18.9%]) (p=0.004).

Multivariable analysis of factors associated with HIV infection among laboratory-confirmed severe acute respiratory syndrome coronavirus 2SARS-CoV-2 individuals admitted to hospital, 5 March-11 August 2020, DATCOV, South Africa. (N=41,877) Dots represent adjusted odds ratios and capped lines represent 95% confidence intervals.
Factors associated with COVID-19-associated in-hospital mortality
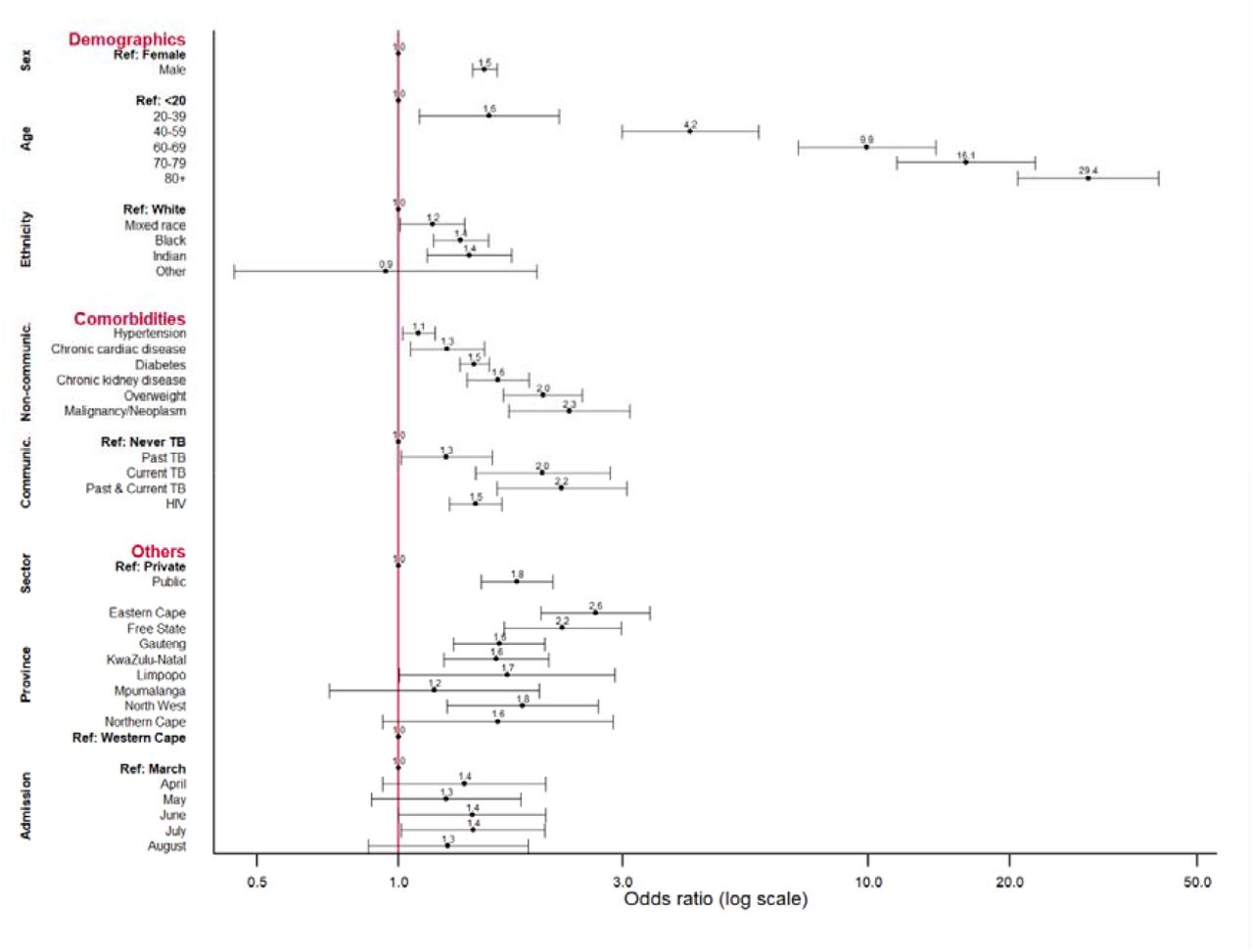
Of the 41,877 hospitalised patients with recorded outcomes, 34,215 (81.7%) were discharged alive and 7,662 (18.3%) died. Factors statistically associated with in-hospital COVID-19 mortality were older age, male sex, non-white (black, Indian and mixed) race, having comorbid hypertension, diabetes, chronic cardiac disease, chronic renal disease, malignancy, obesity, HIV and past or current TB or both, and being admitted in the public health sector (Table 2 and Figure 5). In-hospital mortality increased with each month of the epidemic and was significantly higher in five provinces, Eastern Cape, Free State, Gauteng, KwaZulu-Natal and North West, compared to the Western Cape (Figure 5).
Factors associated with in-hospital mortality among individuals with laboratory-confirmed severe acute respiratory syndrome coronavirus 2SARS-CoV-2 admitted to hospital, 5 March-11 August 2020, DATCOV, South Africa. (N=41,877)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Multivariable analysis of factors associated with in-hospital mortality among laboratory-confirmed severe acute respiratory syndrome coronavirus 2SARS-CoV-2 individuals admitted to hospital, 5 March-11 August 2020, DATCOV, South Africa. (n=41,877) Dots represent adjusted odds ratios and capped lines represent 95% confidence intervals.
Association of in-hospital COVID-19 mortality with immune suppression among HIV-infected individuals
When adjusting for age, sex, race, health sector, province, month of admission, NCDs, and past or active TB, COVID-19 patients with immune suppression (CD4<200 cells/μl) were more likely to die in-hospital when compared to HIV-negative individuals and to those with CD4≥200 cells/μl (Table 3). COVID-19-associated in-hospital mortality was statistically similar between HIV-uninfected and HIV-infected individuals without immune suppression (CD4≥200 cells/μl) and between individuals receiving or not receiving ART and with low (<1,000 RNA copies/ml) or high (≥1,000 RNA copies/ml) HIV viremia (Table 3).
Effect of ART, CD4 count and HIV viral load on in-hospital mortality * among laboratory-confirmed SARS-CoV-2 HIV-infected individuals admitted to hospital, 5 March-11 August 2020, DATCOV, South Africa.
Effect of multiple comorbidities on COVID-19 associated in-hospital mortality
In a multivariable model adjusting for age, sex, race, HIV (for the non-stratified model on HIV status only), health sector, province, and month of admission, there was an increasing odds of in-hospital mortality for individuals with multiple non-HIV comorbidities, irrespective of HIV status as well as among HIV-infected and HIV-uninfected individuals (Table 4). There was no statistical evidence of interaction between the presence of other multiple comorbidities and HIV infection status on in-hospital mortality (Table 4).
Effect of single or multiple non-communicable comorbidities* on in-hospital mortality ** among laboratory-confirmed SARS-CoV-2 individuals admitted to hospital, 5 March-11 August 2020, DATCOV, South Africa.
Discussion
Among a large cohort of hospitalised individuals in a high HIV and TB prevalence setting, we found that HIV and TB were associated with a moderately increased risk of in-hospital COVID-19 mortality. In addition, HIV-infected individuals with immunosuppression were more likely to die compared to those with CD4 count ≥200. Accounting for other differences including age, HIV infected individuals have a higher prevalence of other chronic comorbidities compared to HIV uninfected individuals. Increasing numbers of comorbidities were associated with COVID-19 mortality and this effect was similar in HIV-infected and uninfected individuals.
Early small cohort studies conducted in high income countries were inconclusive on the role of HIV or TB on disease severity and mortality due to COVID-19. (32, 33) However, more recent studies from the Western Cape Province (29) and from the UK (30) demonstrated consistent findings of an increased risk of mortality among HIV-infected individuals. We describe an increased risk for mortality with more severe immunosuppression, but no increased risk associated with higher viral load, while the Western Cape study found similar mortality risk associated with presence of high viral load or immunosuppression. This could be explained by the fact that our study included data from other provinces with different levels of access to care and treatment and different HIV and TB burden. Immunosuppression is likely to be associated with COVID-19 mortality due to impaired immune function.
The prevalence of other comorbidities was high among HIV-infected individuals included in our analysis. This high prevalence could be due to several reasons. Antiretroviral drugs (ARVs) such as tenofovir disoproxil fumarate (TDF) which is part of the first line ART regimen in South Africa, has new or worsening renal failure as one of its side-effects (40, 41). Other ARVs have side effects that include hyperlipidaemia, cardiac disease, diabetes and liver disease. (42) Also, as HIV-infected individuals on ART live longer, the risk of developing NCDs increases with age. HIV-infected individuals with immunosuppression are also more likely to develop TB and HIV-related malignancies. (43) Increasing numbers of comorbidities were associated with increased risk of COVID-19 mortality due to poorer overall health status, more compromised immunity and presence of chronic inflammatory state. The chronic inflammatory state could create a pathway for severe COVID-19 disease. (43) The effect was similar in HIV-infected and uninfected individuals but the borderline significance in multivariable analysis warrants that this interaction between HIV and other NCDs on COVID-19 associated mortality be further investigated.
Increasing age, male sex, and chronic underlying illness (particularly hypertension and diabetes) were also associated with increased mortality in our study population. (4, 11, 13, 44, 45) Impaired immune function may explain the increased risk of COVID-19 mortality among persons with diabetes. (46) For other NCDs, the mechanisms remain unclear although severe hypoxaemia, inflammatory activation and hypercoagulability may be contributory. (47-51) Chronic pulmonary disease and asthma, while reported in other studies to have increased risk for mortality, was not shown to be a significant factor in this study, possibly due to the over-reporting of mild or unconfirmed/undiagnosed disease in this cohort (13, 52). Restrictions imposed to curb the pandemic may have resulted in decreased utilisation of services for the prevention and treatment of NCDs. (12) Race as a potential proxy for poverty has been shown in other studies is an additional risk factor for higher in-hospital mortality.(17, 35, 53, 54)
The case fatality ratio (CFR) of 18% observed among hospitalised patients in our analysis was lower than that reported in studies in Europe (24-32%) and South America (23-43%) but was higher than the CFR of 13% reported in the Democratic Republic of Congo with a small sample size. (15-17) The lower CFR could be explained by the relatively younger population structure in South Africa. Observed variation in CFRs at different times of the epidemic and between provinces and health sectors may be a result of population demographics, varying population levels of COVID-19 infection, levels of comorbidities in different areas, changes in admission practices, the severity of illness in admitted cases, availability of treatment options, limited access to care, higher numbers of admissions overwhelming services and health services’ effectiveness,.(55, 56)
The DATCOV national hospital surveillance system for COVID-19 also provided valuable insights into the epidemic trajectory. The systematically collected data on hospitalised cases show that the epidemic peaked in July and since then cases have decreased despite progressive opening of the restrictions. A recent report from the Western Cape Province indicated high seroprevalence in some communities, suggesting that amongst other factors, possible population level immunity may be playing a role on the reductions seen. (57)
Strengths and Limitations
The main strengths of the DATCOV hospital surveillance system are the large numbers of hospital admissions reported, that it is representative across all provinces and the public and private health sector in South Africa, and that it provides real-time data.
The limitations of this surveillance are representation bias as DATCOV did not initially include all public hospitals with COVID-19 admissions and therefore may have a bias towards the private sector of South Africa. The Department of Health decided in mid-July to implement this surveillance system across all hospitals, and DATCOV will soon be a fully representative surveillance system. Furthermore, DATCOV only reports hospital-based admissions and deaths and therefore does not include deaths occurring outside hospitals. Non-COVID-19 deaths were reported following medical panel review, however it is possible that some deaths were misclassified.
Data quality in a surveillance system is dependent on the information submitted by healthcare institutions. We used multiple imputation to address missing data; however, the validity of the imputed data relies on the assumption that data were missing at random. Fields with the highest proportion of incomplete data include race and comorbidities. HIV prevalence among hospitalised cases was less than community HIV prevalence because of higher reporting of data by the private sector; however, HIV prevalence among hospitalised individuals in the public sector aged 20 to 59 years was similar to population HIV prevalence in this age group (Table S2). The level of control of NCDs such as diabetes, using objective measures like HbA1C, was not consistently reported. Other data have shown that individuals with poorly controlled NCD were at greater risk for mortality. (13, 34)
Conclusions and policy implications
South Africa is experiencing a large COVID-19 epidemic. DATCOV provides information on the trends and risk factors associated with COVID-19 mortality in South Africa. It also addresses a knowledge gap in LMIC, allowing for analysis of COVID-19 epidemiology in a country with a younger population, unique disease profile with epidemics of both infectious (HIV and TB) and non-communicable chronic diseases, and an overburdened public health system. The availability of reliable surveillance data allows a better understanding of the epidemiology of COVID-19 in South Africa, to monitor the COVID-19 epidemic and to respond with adequate control measures. When local transmission is widespread and testing strategies change, hospital admission or mortality surveillance systems provide a more reliable picture of the epidemic progression than overall confirmed case numbers. (58)
Given the high prevalence of HIV and TB in South Africa and the demonstration of modest increases in COVID-19 mortality for individuals with these diseases, expected COVID-19 mortality may be better predicted. The lack of statistical evidence of interaction between NCDs and HIV in a large cohort of COVID-19 patients suggest no or minimal synergistic effect of these conditions on COVID-19 associated-mortality; however, this finding requires further investigation in different settings. The increased CFR in certain provinces, in the public sector and in later months of the epidemic require further interrogation for resources and support to be directed where they are found to be required, ahead of a possible resurgence of cases.
Data Availability
All data is available through the National Institute for Communicable Diseases by permission to the corresponding author.
Conflicts of interest
The authors declare that there are no conflicts of interest.
Role of the funding source
DATCOV is funded by the National Institute for Communicable Diseases (NICD) and the South African National Government. No additional funding was obtained towards the completion of this analysis and the development of this manuscript.
Contributorship
DS, SG, WJ contributed to literature search. WJ, MM, CC contributed to study design, data collection. WJ contributed to data analysis, and creation of tables and figures. WJ, CC, TK, SW, LB contributed to data interpretation and writing. WJ drafted the manuscript and all other authors contributed scientific inputs equally to drafts of the manuscript. WJ,MM verified the underlying data.
Acknowledgements
We acknowledge the significant contributions to the DATCOV program and this manuscript by Drs Stefano Tempia and Pelagia Murangandi of the U.S. CDC South Africa, on secondment to the NICD.
The authors wish to acknowledge the support and contribution from the following organisations: NICD, the National Department of Health, the nine provincial departments of health, the Hospital Association of Southern Africa (HASA), the private hospital groups and public sector hospitals who submitted data to DATCOV. Health professionals submitted data and are acknowledged. A full list of DATCOV surveillance participants is provided in Appendix. The authors would also wish to acknowledge the DATCOV team, Rebone Kai, Simphiwe Dyasi, Tracy Arendse, Beverley Cowper, Kholofelo Skhosana, Felicia Malomane, Monwabisi Blom, Akhona Mzoneli, Salaminah Mhlanga, Bracha Chiger, Busisiwe Ali, Siphamandla Mzobe, Linamandla Qekeleshe, Caroline Magongwa, Caroline Mudara, Lovelyn Nnaji, Richard Welch, Noel Mfongeh, Christo Greyling, David Spade, Winrie Kruger, Supriya Soorju and Ryan Hudson; and the ComUnity team, Gareth Jane, David Prosser and George Ulloa.
References



