
Abstract
Background Changes in the prevalence of mental health problems among smokers due to the COVID-19 pandemic in England have important implications for existing health inequalities. This study examined the prevalence of psychological distress among smokers following the onset of the pandemic compared with previous years.
Methods Cross-sectional data were used from a representative survey of smokers (18+) in England (n = 2,927) during four months (April to July) in 2016, 2017 and 2020. Adjusted logistic regressions estimated the associations between past-month psychological distress across two time periods (2016/17 and 2020), and age. Weighted proportions, chi-squared statistics and stratified logistic regression models were used to compare the distributions of minimal, moderate and severe distress, respectively, within socio-demographic and smoking characteristic categories in 2016/17 and 2020.
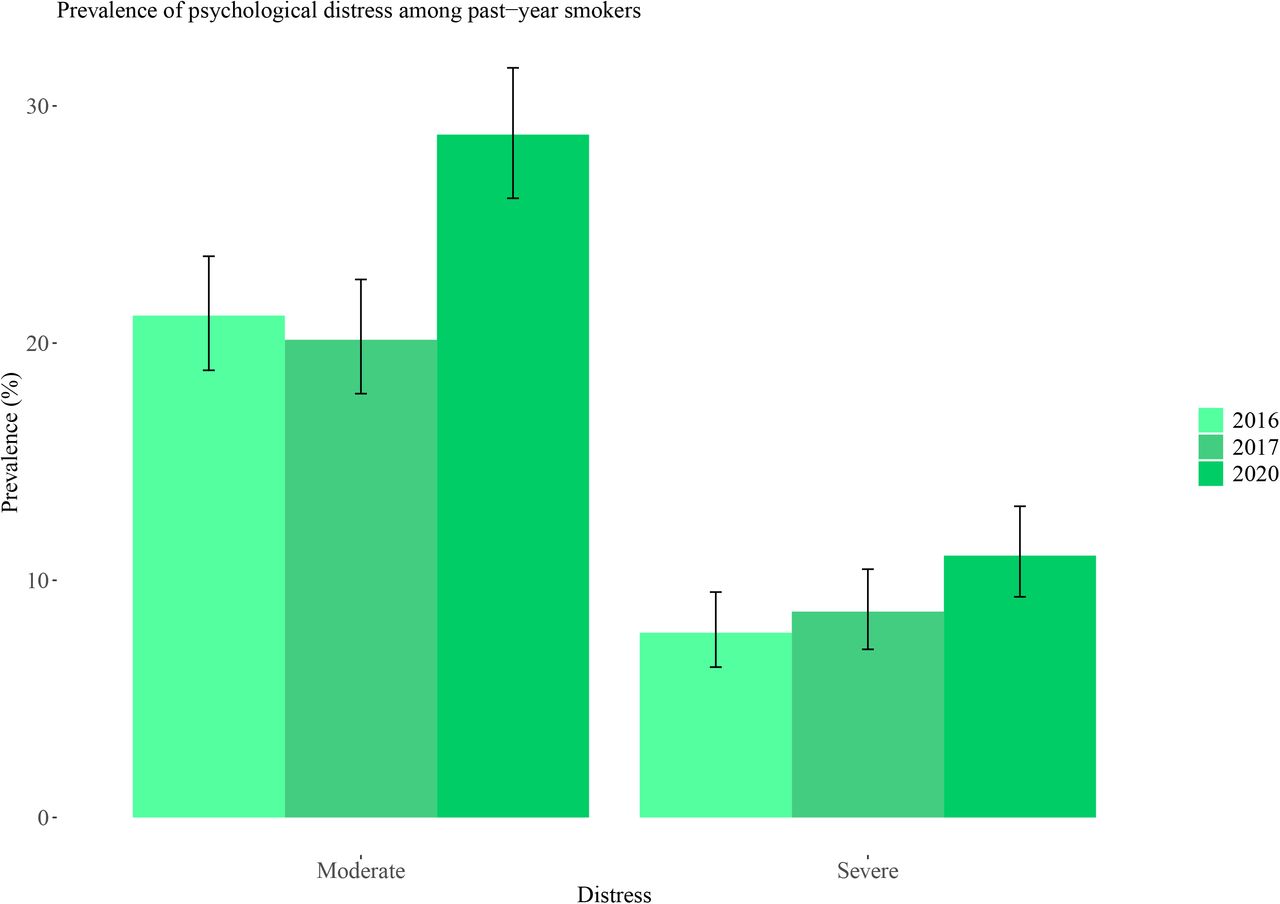
Results The prevalence of moderate and severe distress among past-year smokers was higher in 2020 (moderate: 28.79%, 95%CI 26.11-31.60; OR=2.08, 95%CI 1.34-3.25; severe: 11.04%, 9.30-13.12; OR=2.16, 1.13-4.07) than in 2016/17 (moderate: 20.66%, 19.02-22.43; severe: 8.23%, 7.16-9.47). While there was no overall evidence of an interaction between time period and age, young (16-24 years) and middle-age groups (45-54 years) may have experienced greater increases in moderate and older age groups (65+ years) in severe distress from 2016/17 to 2020. There were also increases in 2020 of moderate distress among those from more disadvantaged social grades and of both moderate and severe distress among women and those with low cigarette addiction.
Conclusions Between April-July 2016/17 and April-July 2020 in England there were increases in both moderate and severe distress among smokers. The distribution of distress differed between 2016/17 and 2020 and represents a widening of established inequalities, with increases in distress among socio-economically disadvantaged groups, women and diverging age groups.
What this paper adds
Surveys in the UK indicate that there has been a deterioration in mental health of the general population since the onset of the COVID-19 pandemic.
Smoking is strongly associated with poor mental health, and a deterioration in mental health among smokers has potentially damaging consequences for existing health inequalities in the UK.
Our findings using data from a large population-based sample of adults in England show that between 2016/17 and 2020 there were increases in moderate and severe psychological distress among smokers.
INTRODUCTION
Between 2014 and 2015 the prevalence of adult smoking in England was estimated to be 16.4%.1 Across the same period smoking prevalence was higher among those with anxiety or depression (28.0%), a long-term mental health condition (34.0%) and serious mental illness (40.5%).1 Those with a mental health condition are more likely to be more dependent smokers and to have greater difficulty in remaining abstinent after quitting, despite greater desire to quit compared with the general population.2 These differences in smoking may account for up to two thirds of the inequality in life expectancy between those living with and without a mental health condition.3 This study aimed to examine the prevalence of distress among smokers following the onset of the COVID-19 pandemic in England compared with previous years.
Serious psychological distress is defined as mental health problems that are associated with impairment in social or occupational functioning and require treatment.4 Psychological distress is more common among smokers and is negatively associated with quit success and abstinence.5,6 The relationship between smoking and distress may be explained by common risk factors related to socio-economic position7, but research also suggests potential bidirectionality8. Individuals may be motivated to smoke to alleviate symptoms of distress, and there is evidence that smoking may itself directly increase the risk of distress.9,10
Between 2016-2017 in England, 24.3% and 9.7% of past-year smokers indicated moderate and serious past-month distress, respectively.11 Also, those with an indication of a mental health problem were more dependent on cigarettes but more likely to be motivated and have recently attempted to quit.
The COVID-19 pandemic and resulting government ‘lockdown’ measures were associated with a deterioration of mental health in the UK compared with pre-COVID-19 trends, with specific burden among women and young adults.12,13–15 Research has suggested that following the March 2020 government restrictions, smokers were more likely to try and quit, and rates of smoking cessation were higher.16 However, a deterioration in mental health among smokers may negatively impact quitting behaviour given that smokers with distress have been found to be less likely to quit and remain abstinent.5,6
Our previous research has highlighted an age gradient in distress among smokers, with younger groups reporting higher levels of distress compared with older age groups.11 However, considering the sharp positive age gradient in the risk of death from COVID-1917, deterioration in mental health during the pandemic may be more pronounced among older age groups.
An increase in the prevalence of distress among smokers during the COVID-19 pandemic in England could potentially widen existing health inequalities. Monitoring levels of distress among smokers is important to highlight unmet need for mental health and smoking cessation support in general and also during current and potential future respiratory disease epidemics. Using Smoking Toolkit Study (STS) data the aims of this study were to i) examine the prevalence of psychological distress among past-year smokers during April-July 2020 compared with the same monthly time period (April-July) in 2016-2017 (the previous time distress was assessed in the STS) and ii) examine the distribution of distress within sociodemographic and smoking characteristic categories of past-year smokers during April-July 2020 and April-July 2016-2017.
METHODS
Study design
Data were drawn from the Smoking Toolkit Study (STS), a monthly repeated cross-sectional survey of a representative sample of adults in England.18 The dataset for the primary analysis consisted of four months of STS data from April to July in each of the years 2016, 2017 and 2020. Respondents were age 18 years or older.
The STS uses a hybrid of random location and quota sampling to select a new sample of approximately 1,700 adults each month. Locations are randomly selected from around 170,000 output areas in England stratified by geodemographic characteristics. Interviews are performed with one household member until quotas based on factors influencing the probability of being at home (e.g. gender, age, working status) are fulfilled. Comparisons with other national surveys show that the STS recruits a representative sample of the population in England.18 Data are usually collected monthly through face-to-face computer assisted interviews. However, due to the COVID-19 pandemic, from March 2020 data were collected via telephone only. Diagnostic analyses have suggested it is reasonable to compare data from before and after the lockdown, despite the change in data collection method.16
Ethical approval for the STS is granted by the UCL Ethics Committee (ID 0498/001; ID: 2808/005). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline were used in the design and reporting of this study.19
Dependent variables, independent variables and covariates
The primary outcome of this study was the prevalence of psychological distress among past-year smokers. This was derived using the following measures.
Mental health (Past-month psychological distress)
Past-month distress was measured using the K6 community screening measure of non-specific psychological distress.20,21 The measure has ‘substantial’ concordance with independent clinical ratings of serious mental illness.21 Participants were asked:
“During the past 30 days, about how often, if at all, did you feel… nervous; hopeless; restless or fidgety; so depressed that nothing could cheer you up; that everything was an effort; worthless?”
The answer options were presented in a randomised order and for each the respondent indicated one of the following: “All of the time (scored 4); Most of the time (3); Some of the time (2); A little of the time (1); None of the time (0)”
A sum score with a possible range from 0 to 24 was calculated. Based on previous research scores of 13 and higher were categorised as serious distress, scores between 5-12 as moderate and less than 5 as no/minimal distress.22
Smoking status
Smoking status was ascertained using responses to the following question:
“Which of the following best applies to you?”
Those who responded with “I smoke cigarettes (including hand rolled) every day” and “I smoke cigarettes (including hand rolled), but not every day” were categorised as current cigarette smokers.
Those who responded with “I smoke cigarettes (including hand rolled) every day”, “I smoke cigarettes (including hand rolled), but not every day” and “I have stopped smoking completely in the last year” were categorised as past-year smokers.
Those indicating that they do not smoke cigarettes, but do smoke tobacco of some kind (e.g. Pipe, cigar or shisha) were excluded from the analysis (n=138) because they do not include measures of dependence that are measured for cigarette.
Smoking and quitting behaviour
Cigarette addiction
Cigarette addiction was measured using the heaviness of smoking index (HSI).23 This HSI uses two questions from the Fagerström Test for Cigarette Dependence: time to first cigarette in the morning after waking and the number of cigarettes smoked per day. Those with a score >4 are considered to have high addiction, and those with <4 considered to have low/moderate addiction.
Motivation to stop smoking
Motivation to stop smoking was assessed using the Motivation To Stop Scale24, a single-item measure with seven response options representing increasing motivation to quit. Responses were collapsed into two variables reflecting high vs. low or no motivation to stop smoking.24
Quit attempts
Quit attempts in the past month was measured among past year smokers using the question “How many serious attempts to stop smoking have you made in the last 12 months?”, and if one or more attempts were reported: “How long ago did your most recent serious quit attempt start?”.
We distinguished those who attempted to quit up to 1 month ago versus those who made no quit attempt or attempted to quit more than 1 month before the interview but were not successful.
Socio-demographic characteristics
The socio-demographic variables age (categories 16-24, 25-34, 35-44, 45-54, 55-64, and ≥65 years), sex (categories women vs other), occupation-based social grade (AB (higher and intermediate managerial, administrative and professional), C1 (supervisory, clerical and junior managerial, administrative and professional), C2 (skilled manual workers), D (semi□skilled and unskilled manual workers) and E (state pensioners, casual and lowest□grade workers, unemployed)), region of England (government office region including nine categories: North East, North West, Yorkshire and the Humber, East Midlands, West Midlands, East of England, London, South East, South West), and the presence of children in the household were measured.
Time period
The variable for time period included four months of data (April-July) each from the years 2016, 2017 and 2020. In this study, data from 2016 and 2017 were collapsed together to form a new variable reflecting April-July 2016-2017. These time periods were chosen because questions related to mental health outcomes were not included in the surveys during 2018 and 2019, and were only re-added from April 2020. The comparison of the same four month time period in 2020 and 2016-2017 sought to account for potential seasonality in mental health disorders.25,26
Sample selection
Overall, 19,960 (unweighted) adults aged 18+ were surveyed. Of these, 3,640 past-year (current and recent ex) smokers were asked the mental health questions. Those who exclusively smoked cigars and pipes (n = 138), did not complete the mental health questions or selected ‘I don’t know’ or ‘prefer not to say’ in response to any of them (n = 399), or had missing data on any of the other variables included in the present analysis were excluded. This left a final unweighted sample size for analysis of 2,972 past-year smokers of which 2,418 were current smokers.
Statistical analysis
To address our first aim, weighted proportions (95% CIs) were used to describe the prevalence of past-month moderate and severe distress, respectively, during the period of April-July 2020, and April-July 2016-2017 among past-year smokers.
We constructed separate logistic regression models to assess changes in moderate and severe distress, respectively, among smokers (past-year and current) between the two time periods (April-July 2020 vs April-July 2016-2017 as referent) and age (six categories with 16-24 as referent) and the interaction terms.
All associations are reported as odds ratios (ORs) with 95% confidence intervals (adjusted for sex, social grade and region). The inclusion of the time period*age interaction allowed us to examine psychological distress at different levels of age, which is of interest given the strong age gradient in risk of death from COVID-19.17
To address our second aim, we: i) calculated weighted proportions and chi-square statistics to compare the distribution of moderate and severe distress, respectively, within socio-demographic (age, sex, social grade, whether there were children in the house) and smoking characteristics (cigarette addiction, quit attempts and motivation to stop smoking) of past-year smokers during April-July 2020 and April-July 2016-2017; and ii) constructed a series of stratified logistic regression models to examine any changes within these socio-demographic and smoking characteristic sub-groups between April-July 2016-2017 (referent) and April-July 2020. All associations are reported as odds ratios (ORs) with 95% confidence intervals (adjusted for age, social grade, sex and region except where the covariate was the variable of interest).
Analysis was carried out in R version 3.6.0 in September 2020. A 2-sided P□<□.05 was considered statistically significant. The analysis plan was pre-registered online at https://osf.io/eh6sk/.
Sensitivity analysis
The same analyses reported for the primary analysis was conducted but comparing April-July 2020 with all months in 2016-2017.
Unregistered post-hoc analyses
We conducted further logistic regression models to explore changes in moderate and severe distress among recent ex-smokers (quit within the past year) between the two time periods (April-July 2020 vs April-July 2016-2017 as referent) and age (six categories with 16-24 as referent). We calculated Bayes factors (BF) for non-significant associations to explore whether they provided evidence for no effect (BF < 1/3) when compared to the alternative hypothesis or indicated data insensitivity (BF ≥ 1/3 and < 3).27 The alternative hypothesis was modelled using a half-normal distribution centred on zero, with a standard deviation equal to the expected effect size.
In 2016-2017 mental health data was only collected among current and recent ex-smokers. From April 2020 all respondents were asked questions about their mental health, allowing us to examine levels of distress across all categories of smoking status. Analysing distress according to smoking status contextualises the findings among smokers against those who have never smoked or have been abstinent for a long time. Further analyses were run exploring differences in the prevalence distress between April-July 2020 according to smoking status. The results are presented as weighted proportions (with 95% CIs). Logistic regression was used to estimate the association between distress and smoking status (four categories: Smoker, Stopped in the past year, Stopped >1 year ago and Never Smoker (referent)).
RESULTS
A weighted total of 3,211 past-year smokers (mean (SD) age = 43.26 (17.11) years; 48.08% women) completed the STS survey between April-July in 2016 (n = 1,106), 2017 (n = 1,066) and 2020 (n = 1,039). Among the overall sample 748 (23.29%) reported moderate distress, and 293 (9.12%) reported severe distress. See Table 1 for an overview of the sample characteristics. Weighted prevalence statistics for moderate and severe distress among past-year smokers in 2016, 2017 and 2020 are shown in Figure 1.

{kind=link}
Changes in distress between 2016-2017 and 2020
Past-year smokers
Past-year smokers in 2020 had twice the odds of moderate and severe distress, respectively, compared with 2016-2017 (Table 2). An age gradient was apparent, with older age groups less likely to report moderate or severe distress, respectively, compared with those aged 16-24. There was no evidence of an interaction between time period and age.
Associations between i) moderate (vs none) and ii) severe psychological distress (vs none) and time period of survey (April-July 2020 vs April-July 2016-2017) among past-year and current smokers in England
A sensitivity analysis using the entire two-year period of 2016 and 2017 as a comparator time period produced similar results to the main analysis. (Supplementary Table s1).
Current smokers
Similarly, current smokers in 2020 had twice the odds of moderate distress compared with 2016-2017 (Table 2). An age gradient was also apparent among current smokers, with older age groups less likely to report moderate or severe distress, respectively, compared with those aged 16-24. There was no evidence of an interaction between time period and age.
Recent ex-smokers
Among the much smaller group of recent ex-smokers (n=277) there were no significant associations between moderate or severe psychological distress, respectively, in 2020 compared with 2016-2017 (Supplementary Table s2). Based on observed increases in mental health problems pre and post COVID-19 among the general population in the UK28, exploratory expected effect sizes (ORs) were set to 1.1, 1.5 and 1.9 respectively. The calculation of Bayes factors under all of these contexts indicated that the data were insensitive to detect these effects (Supplementary Table s3).
Prevalence of psychological distress according to smoking status between April-July 2020
There were greater levels of both moderate and severe distress among smokers, recent and >1year ex-smokers compared with never smokers (Supplementary Figure s1 and Table s4).
The distribution of distress within sociodemographic and smoking characteristics of past-year smokers in 2016-2017 and 2020
Moderate distress
The prevalence of moderate distress was higher in 2020 compared with 2016-2017 among: those aged 16-24 and 45-54, women, those in more disadvantaged social grades, those with and without children in the house, and among those with low cigarette addiction (Table 3). No differences were apparent among those who had tried to quit within the past month or among current smokers with high motivation to quit.
Changes in the sociodemographic profile of i) no/minimal, ii) moderate and iii) severe distress in 2016/2017 and 2020.
Severe distress
The prevalence of severe distress was higher in 2020 compared with 2016-2017 among: those aged 65+, women, and among those with low cigarette addiction (Table 3). There were no apparent differences in the prevalence of distress according to high cigarette addiction, recent quit attempts or motivation to stop smoking.
DISCUSSION
Between April-July 2016/17 and April-July 2020 in England there were increases in moderate and severe distress, respectively, among both past-year and current smokers. Older age groups were less likely to report symptoms compared with younger groups, but there was no interaction between age and time period. Within socio-demographic categories, moderate distress was greater in 2020 among those aged 16-24 and 45-54 years, women, those from more disadvantaged social grades, those with and without children at home and those with low cigarette addiction. Severe distress was greater in 2020 among those aged 65+, women and among those with low cigarette addiction.
The increase in levels of both moderate and severe distress among smokers is likely caused by the ongoing COVID-19 pandemic and associated stay-at-home restrictions that have affected work and social life in England.29 Moreover, while mental health has deteriorated in the overall population as a result of COVID-1912, our analysis using exclusively April-July 2020 data highlighted that smokers specifically continue to display elevated levels of distress compared with non-smokers. Together these findings have concerning implications for existing smoking-related health inequalities considering the strong and potentially bi-directional associations between smoking and mental illness.8
Older smokers were less likely to report distress compared with younger groups.11 These findings re-emphasise the need to address higher prevalence of poor mental health among younger smokers.12,30,31 We hypothesised that there may be an interaction between age-group and year with older smokers experiencing greater distress in 2020 due to the age gradient in deaths from COVID-19 and the known risks of smoking. This was not borne out in the primary analysis, but there were signals of age-group differences in our stratified socio-demographic analyses discussed below.
Compared with 2016/17 the distribution of moderate distress in 2020 differed within certain sociodemographic characteristics, with higher prevalence in those aged 16-24 and 45-54, women, those from more disadvantaged social grades and in both those with and without children in the home. The distribution of severe distress was broadly similar across the two time periods, with the exceptions of higher prevalence in 2020 within women and those aged 65+. These demographic profiles of distress have important implications for existing inequalities and support other findings that the impacts of COVID-19 on worsening mental health have not been felt equally across society, but specifically among women and the more socioeconomically disadvantaged.12 However, the reported significance of these stratified socio-demographic analyses within age specifically (given the absence of interaction effects described above), but also other characteristics should be treated with caution and viewed descriptively.
Regarding smoking and quitting behaviour, our results indicate that between 2016/17 and 2020 there have been no changes in the prevalence of high cigarette addiction among those with moderate or severe distress, respectively. There were, however, increases in the prevalence of low addiction. Whether this phenomenon is unique to 2020 or represents a sustained change in the mental health population (as has been observed in the general population of smokers in England32) will be monitored going forward. The prevalence of past month quit attempts or motivation to stop smoking (among current smokers) did not change between 2016/17 and 2020 within any category of psychological distress. This is consistent with recently published findings in the general population showing that COVID-19 triggered only a minority of quit attempts in England.33,34
Recent YouGov data in England has suggested that those with existing mental health problems may have been more likely to have quit successfully during the pandemic.35 However, robust analyses of this unexpected finding is needed. Moreover, the same YouGov data has suggested that smokers with poor mental health who did quit during the pandemic are smoking more and are less likely to quit as a result of COVID-19.
Findings from this study have implications for policy and practice. The levels of distress among disadvantaged social grades and women, and the persistence of poor mental health among younger smokers is concerning given that the prevalence of mental illness 2016/17 was already thought to be greater in these demographics than in previous years.36 It is important that support for smoking cessation is available to those with mental health problems during the pandemic and in its aftermath. Mental health practitioners should continue to monitor the smoking status of their patients, and offer referral to local authority stop smoking services where they can receive effective support for smoking cessation.37 Specific attention should be considered for smokers aged 65+ at this time, who are generally more dependent on cigarettes38 and from our analyses appear to have greater distress than in previous years. Advice on effective harm reduction alternatives such as electronic cigarettes should also be considered.39,40 In addition, clear public health messaging about the immediate health benefits of smoking cessation is necessary to counter the uncertainty that has emerged related to some evidence that smokers appear to be at reduced risk of SARS-Cov-2 infection.41
To our knowledge this study is the first to analyse psychological distress among smokers using data before and during the COVID-19 pandemic. However, it is limited by the use of cross-sectional survey data where smoking status is self-reported. Moreover, we did not have mental health data in 2018, 2019 and the first three months of 2020. While it is likely that some of the increase in mental health problems in 2020 reflect a continuation of a secular trend going back to 200836, data from the opinions and lifestyle survey collected between 2018 to date highlight a clear deterioration in wellbeing among smokers following the onset of the pandemic in England.42
Future research should continue to monitor changes in distress among smokers throughout the ongoing pandemic and its aftermath. Greater understanding about the direction(s) of the relationship between smoking and mental illness will also help inform the best approach for reducing smoking levels in this vulnerable group.
In conclusion, comparing April-July 2016/17 with April-July 2020 in England there were increases in moderate and severe distress among smokers. Continued support and messaging for smoking cessation among those with poor mental health is ever more important during the ongoing COVID-19 pandemic and in its aftermath.
Data Availability
Pre-registered analysis plan and statistical code are available at https://osf.io/eh6sk/
Funding and acknowledgements
We are grateful to Cancer Research UK and the UK Prevention Research Partnership for funding the study. Authors are members of the UK Prevention Research Partnership, an initiative funded by UK Research and Innovation Councils, the Department of Health and Social Care (England), and the UK devolved administrations and leading health research charities.
Statement of competing interests
Authors are members of the UK Prevention Research Partnership, an initiative funded by UK Research and Innovation Councils, the Department of Health and Social Care (England), and the UK devolved administrations and leading health research charities. JB reports receiving grants from Cancer Research UK during the conduct of the study and receiving unrestricted research funding from pharmaceutical companies who manufacture smoking cessation medications to study smoking cessation outside the submitted work. LS reports receiving honoraria for talks, receiving an unrestricted research grant and travel expenses to attend meetings and workshops by pharmaceutical companies that make smoking cessation products (Pfizer and Johnson & Johnson), and acting as a paid reviewer for grant-awarding bodies and as a paid consultant for health care companies. LK, LB, GM and MH have no competing interests to declare.
References



