
Abstract
Background Global vaccine development efforts have been accelerated in response to the devastating COVID-19 pandemic. We evaluated the impact of a 2-dose COVID-19 vaccination campaign on reducing incidence, hospitalizations, and deaths in the United States (US).
Methods We developed an agent-based model of SARS-CoV-2 transmission and parameterized it with US demographics and age-specific COVID-19 outcomes. Healthcare workers and high-risk individuals were prioritized for vaccination, while children under 18 years of age were not vaccinated. We considered a vaccine efficacy of 90% against infection following 2 doses administered 28 days apart achieving 40% vaccine coverage of the overall population. We specified 10% pre-existing population immunity for the base-case scenario and calibrated to an effective reproduction number of 1.5, accounting for current COVID-19 interventions in the US.
Results Vaccination reduced the overall attack rate to 1.6% (95% CI: 1.3% - 1.8%) from 7.1% (95% CI: 6.3% - 7.9%) across the same period without vaccination. The highest relative reduction (83-90%) was observed among individuals aged 65 and older. Vaccination markedly reduced adverse outcomes, with non-ICU, ICU hospitalizations, and deaths decreasing by 85.2% (95% CI: 82.3% - 87.6%), 85.3% (95% CI: 82.3% - 87.8%), and 87.8% (95% CI: 85.1% - 90.1%), respectively.
Conclusions Our results indicate that vaccination can have a substantial impact on reducing disease transmission and adverse clinical outcomes. However, with uptake of 40% or less in the population, vaccination is unlikely to completely eliminate the need for non-pharmaceutical interventions.
Key points Vaccination with 90% vaccine efficacy could substantially mitigate future attack rates, hospitalizations, and deaths, even if only adults are vaccinated. Current non-pharmaceutical interventions remain an important part of outbreak response as vaccines become available and distributed over time.
Introduction
Despite unprecedented movement restrictions, social distancing measures, and stay-at-home orders enacted in many countries [1–4], the COVID-19 pandemic has caused devastating morbidity and mortality. However, the vast majority of the global population remains susceptible to COVID-19, highlighting the need for an effective vaccine.
To mitigate the mounting burden of COVID-19, vaccine development has occurred at an unprecedented pace [5]. As of November 18, 2020, Phase III clinical trials for 12 candidates are underway and some have reported early efficacy results [6]. Other candidates have advanced to phase I and II trials, with over 80 additional candidates in preclinical development [5–8]. The imminent arrival of COVID-19 vaccines compels an urgent need to understand the potential population-level impact of vaccination on COVID-19 transmission and disease outcomes.
The target product profile (TPP) developed by the World Health Organization (WHO) specifies 70% as a preferred population-based efficacy for a COVID-19 vaccine, with a minimum 50% point estimate [9]. Likewise, the Food and Drug Administration (FDA) specifies a primary efficacy of 50% with a lower bound of 30% [10]. Encouragingly, preliminary results from two phase III clinical trials (Pfizer, Moderna) indicate efficacy of over 90% against symptomatic infection [11,12], exceeding the TTP and FDA target range. However, efficacy results do not directly translate to population-level impact. Vaccination programs will roll out over several months, and vaccine delivery will occur over weeks to months as vaccines are manufactured at scale. To project the impact of vaccination and roll-out during the outbreaks, we developed an age-structured transmission model, taking into account comorbidities and demographics of the United States (US) [13–16].
We explored a strategy where healthcare workers and high-risk individuals, including those with comorbidities associated with severe COVID-19 [13–15] and individuals older than 50 years of age, were prioritized for vaccination. This prioritization relies on the evidence that COVID-19 patients with pre-existing health conditions, including diabetes and hypertension, are 2-4 times more likely to develop severe disease than those without comorbidities [17–19]. Moreover, severity of symptoms and risk of death increase precipitously with age [20,21]. Additional vaccines were allocated according to the age-dependent distribution of vaccines against seasonal influenza in the US for individuals aged 18 years and older until population coverage reached 40% [22]. Pre-existing immunity or contemporaneous infection with COVID-19 was not a factor in vaccine allocation. For sensitivity analyses, we assessed vaccine impact at various vaccine coverages and levels of population immunity accrued prior to vaccine availability.
Methods
Model structure
We extended a previously developed agent-based COVID-19 transmission model to include vaccination [23]. The model encapsulates the natural history of COVID-19 with classes of individuals including: susceptible; vaccinated; latently infected (not yet infectious); asymptomatic (and infectious); pre-symptomatic (and infectious); symptomatic with either mild or severe/critical illness; recovered; and dead (Figure 1). We stratified the population into 6 age groups of 0-4, 5-19, 20-49, 50-64, 65-79, and 80+ years based on US demographics [16], in addition to the age-specific prevalence of comorbidities (Appendix, Table A1) [15,24]. The number of daily contacts for each individual was sampled from a negative-binomial distribution [25] with age-dependent mean and standard deviation (Appendix, Tables A2). These contacts were then distributed across age groups using an empirically-determined contact network [25].

Schematic model diagram for infection and natural history of disease.
Disease dynamics
Disease transmission was implemented probabilistically for contacts between susceptible and infectious individuals in asymptomatic, pre-symptomatic, or symptomatic stages of the disease. Based on the number of secondary cases generated during each stage of the disease [26], infectivity of asymptomatic, mild symptomatic, and severe symptomatic stages were parameterized to be 11%, 44%, and 89%, relative to the pre-symptomatic stage [26,27]. Disease-specific parameters were sampled for each individual from their associated distributions and ranges. If infection occurred, the incubation period was sampled from a Gamma distribution with a mean of 5.2 days [28]. A proportion of infected individuals develop symptoms after a highly infectious pre-symptomatic stage prior to the onset of symptoms [29]. The duration of the pre-symptomatic stage was sampled from a Gamma distribution with a mean of 2.3 days [27,29]. The infectious period following the onset of symptoms was sampled from a Gamma distribution with a mean of 3.2 days [30]. Symptomatic cases had an age-dependent probability of developing mild or severe/critical illness. The remaining proportion of infected individuals were asymptomatic after the latent period until recovery, with an infectious period that was sampled from a Gamma distribution with a mean of 5 days [30,31]. We assumed that recovery from a primary infection provided adequate immunity for the remainder of the simulation, preventing re-infection. A summary of model parameterization is provided in Table 1.
Description of model parameters and their estimates.
Infection outcomes
In the model, symptomatic cases with mild illness recover without the need for hospitalization, but hospital and intensive care unit (ICU) admissions were included for severely/critically ill patients. It was also specified that severely ill individuals who were not hospitalized practice self-isolation immediately upon symptom onset, with the age-dependent daily number of contacts based on a matrix derived from a representative sample population during COVID-19 lockdown [32]. Non-ICU and ICU admissions of patients were parameterized based on age-stratified COVID-19 hospitalization data, and the presence of comorbidities [13,14]. For those who were hospitalized, time from symptom onset to admission was sampled in the range of 2-5 days [23,33]. The lengths of non-ICU and ICU stays were sampled from Gamma distributions with means of 12.4 and 14.4 days, respectively [34,35].
Vaccination
We implemented a two-dose vaccination campaign achieving 40% population coverage of the entire population. Vaccines were prioritized to the following groups sequentially: (i) healthcare workers, individuals with comorbidities, and those aged 65 and older (i.e., protection cohort); and (ii) individuals aged 18-64 (i.e., disruption minimization cohort) [36]. We assumed that 70% coverage was the maximum achievable in any age group. Pre-existing immunity as a result of a primary infection with COVID-19 was not a factor in the vaccination of individuals. The age-specific coverage resulting from this prioritization was 38% of those 18-19 years old, 46% of those 20-49 years old, 49% of those 50-64 years old, and 70% of those 65+ years old. We specified an accelerated roll-out in which 80 individuals per 10,000 population would be vaccinated per day, with a 6-day immunization schedule per week. This rate corresponds to ∼15.7 million vaccine doses per week for approximately 15 weeks.
We included a 28-day interval between the first and second vaccine doses. We considered a vaccine efficacy (Ve) of 90% against infection following a 2-dose schedule under ideal conditions for healthy individuals [11,12]. We implemented a 14-day interval after the first vaccine dose to reach half of Ve. The protection equivalent to Ve was reached one week after the second dose. Vaccine efficacy was implemented as a reduction in the probability of transmission when a vaccinated individual encountered an infectious individual. This efficacy was reduced to Vp = (1-q)Ve in vaccinated individuals with comorbidities or in persons older than 65 years of age, where q was sampled uniformly from the 10%-50% range for each individual. This parameterization was based on observed reductions in influenza vaccine effectiveness among frail and comorbid individuals [37,38]. We also assumed that vaccine-induced immunity reduces the risk of developing severe illness by the same factor of Vp =(1-q)Ve if infection occurs post-vaccination, thereby affecting hospitalization rates. The immunity conferred by vaccination or infection was assumed to last longer than one year (i.e., the simulation timelines).
Model scenarios
In the base-case scenario, we assumed a 10% level of pre-existing immunity in the population at the onset of simulations, corresponding to estimates provided in recent seroprevalence studies [39,40]. In scenario analysis, 5% pre-existing immunity was considered to represent regions that have not yet been substantially affected by COVID-19 outbreaks, and alternatively 20% pre-existing immunity was used to represent the expectation that immunity will continue to accrue prior to vaccine availability. To accurately capture the age distribution of population immunity, the model was simulated in the absence of vaccination in an entirely susceptible population. Then, the infection rates in different age groups were derived when the overall attack rate reached 5%, 10%, and 20%, and the corresponding distributions were used as the starting population for the vaccination model (Appendix, Table A3).
Model implementation
Model calibration was performed using an effective reproduction number of 1.5 to account for the effect of current COVID-19 interventions in the US [41]. Simulations were seeded with one initial case in the latent stage in a population of 10,000 individuals (a scalable size in agent-based modelling), and the results averaged over 1000 independent Monte-Carlo realizations, which was sufficient for stabilization. Confidence intervals were obtained using the bias-corrected-and-accelerated bootstrap method. The model was implemented in Julia language and is available at: https://github.com/thomasvilches/covid_vac.
Results
The transmission probability per contact was calibrated to an effective reproduction number Re=1.5 [41]. For the base-case scenario of 10% pre-existing immunity, and with self-isolation of infected individuals following symptom onset, the attack rate was projected to be 7.1% (95% CI: 6.3% - 7.9%) in the absence of a vaccine.
Attack rate
Vaccination substantially mitigated the attack rate across all age groups, with a mean overall attack rate of 1.6% (95% CI: 1.3% - 1.8%) (Figure 2). The vaccination program would avert 556 (95% CI: 477 - 641) infections per 10,000 people (Figure 3).The attack rate was most substantially reduced among individuals aged 65+, by 83-90% (Figure 2). Although no children under 18 years of age were vaccinated, the attack rate among those under 20 years old reduced by at least 50%, largely driven by indirect protection. Sensitivity analyses indicated that more infections would be averted if the population had lower pre-existing immunity (Figure 2,3).

Overall and age-specific relative reduction of mean attack rates with vaccination, as compared to the outbreak scenario in the absence of vaccination, with 5% (blue), 10% (red), and 20% (green) levels of pre-existing immunity.
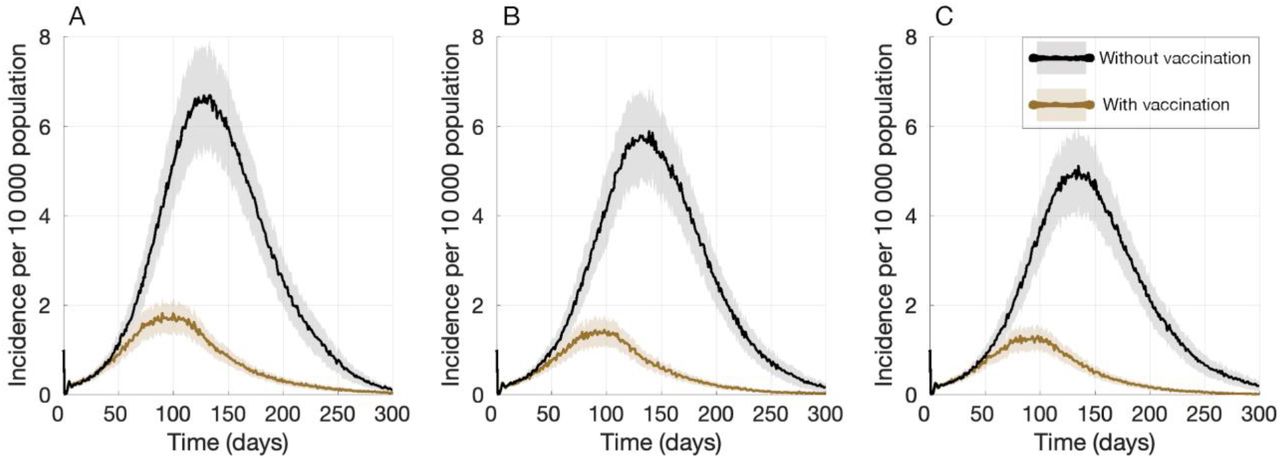
Projected daily incidence of COVID-19 per 10,000 population with 5% (A), 10% (B), and 20% (C) levels of pre-existing immunity.
Hospitalizations and Deaths
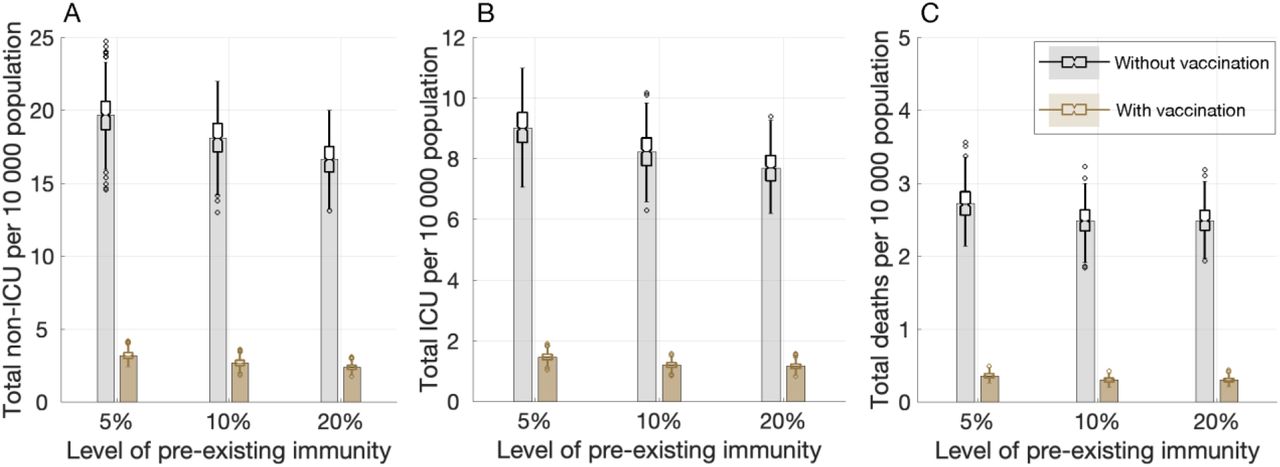
In the absence of vaccination, and with 10% pre-existing immunity, total non-ICU and ICU hospitalizations were projected to be 18 (95% CI: 16.2 - 20.3) and 8.3 (95% CI: 7.3 - 9.3) per 10,000 population, respectively, with 2.5 (95% CI: 2.2 - 2.8) deaths per 10,000 population (Figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Projected daily number of non-ICU hospitalizations (A), ICU hospitalizations (B), and deaths (C) with 5%, 10%, and 20% levels of pre-existing immunity.
Vaccination markedly reduced hospitalizations and deaths (Figure 4). Non-ICU hospitalizations, ICU hospitalizations, and deaths would be reduced by 85.2% (95% CI: 82.3% - 87.6%), 85.3% (95% CI: 82.3% - 87.8%), and 87.8% (95% CI: 85.1% - 90.1%), respectively. We projected that vaccination would lead to similar reductions in hospitalizations and deaths across different levels of pre-existing immunity (Figure 4) (Appendix, Tables A5-A7).
We further simulated health outcomes under 20% vaccine coverage. Under the base-case scenario of 10% pre-existing immunity, Non-ICU hospitalizations, ICU hospitalizations, and deaths would be reduced by 60% (95% CI: 53.3% - 66.5%), 62% (95% CI: 53.3% - 67.7%), and 64.2% (95% CI: 57.9% - 70.3%), respectively. (Appendix, Figure A1-A3).
Discussion
COVID-19 outbreaks have caused significant global morbidity and mortality, in addition to undermining the economic and social well-being of individuals and communities. Despite this devastating toll, the majority of the population remains susceptible to SARS-CoV-2 infection [42]. Thus, vaccine development has been a high priority. The scale and speed of vaccine development efforts have been unprecedented, and it is now likely that highly protective vaccines will be distributed by the start of 2021. This study shows that vaccines with 90% efficacy could substantially mitigate future attack rates, hospitalizations, and deaths, even if only adults are vaccinated.
Our findings should be interpreted within study assumptions and limitations. First, our model vaccinated a large proportion of high-risk individuals, including 90% of healthcare workers and 57% of comorbid individuals. Although this coverage may be difficult to achieve in a short term [43], strategic public health campaigns and transparent communication regarding vaccine safety may be able to improve uptake. Second, we assumed that the protective efficacy of a vaccine would be reduced by 10%-50% in comorbid and elderly individuals, similar to observations for influenza vaccines [37]. The validity of this assumption can only be established once efficacy trial results in these populations are reported. If the performance of a COVID-19 vaccine was not eroded by age or frailty, vaccine impact would be even greater than we projected. Third, we assumed that all vaccinated individuals received both doses. If substantial drop-out occurs after the first dose, vaccines could be used more quickly for the general population, and the short-term effect of drop-outs may be minor. Finally, the model did not explicitly simulate other mitigation measures (e.g., social distancing, mask-wearing, testing, and contact tracing); however, we calibrated the model to current estimates of the effective reproduction number to account for compliance with such measures in the US.
Given the limited population-level immunity to COVID-19 [39], vaccination remains a key preventive measure to reduce disease burden and mitigate future outbreaks. Our study suggests that a vaccine could have a substantial impact on reducing infection, hospitalizations, and deaths, especially among vulnerable individuals with comorbidities and risk factors associated with severe COVID-19. Our findings corroborate the proposed framework by the Committee on Equitable Allocation of Vaccine for the Novel Coronavirus [36], highlighting that their proposed targeted vaccination strategy can effectively mitigate disease burden and the societal impact of COVID-19. We also find that, even with the rapid roll-out simulated here, several months may be elapsed before control of COVID-19 at the population level. Moreover, this impact may be achieved in the context of continued public health efforts, and is not possible without diligent attention to the other aspects of infectious disease control such as masking, testing, contact-tracing, and isolation of infected cases. If the arrival of vaccination programs is accompanied by widespread relaxation of other measures, much higher coverage will be necessary with a significantly higher distribution capacity. Nevertheless, our results are an encouraging signal of the power and promise of vaccines against COVID-19.
Competing Interests
Dr. Joanne M. Langley reports that her institution has received funding for research studies from Sanofi Pasteur, GlaxoSmithKline, Merck, Janssen and Pfizer. Dr. Joanne M. Langley also holds the CIHR-GSK Chair in Pediatric Vaccinology at Dalhousie University. Dr. Neuzil’s research center received funding for research studies from Pfizer. Other authors declare no competing interests.
Funding
Canadian Institutes of Health Research [OV4 – 170643, COVID-19 Rapid Research]; São Paulo Research Foundation [18/24811-1]; the National Institutes of Health [1RO1AI151176-01; 1K01AI141576-01], and the National Science Foundation [RAPID 2027755; CCF-1918784].
Reproducibility Statement
The computational system and parameters are available under an open source license at https://github.com/thomasvilches/covid_vac.
References



