
Abstract
People with HIV have higher rates of certain comorbidities, particularly cardiovascular disease and some malignancies, than people without HIV. As somatic mutations associated with age-related clonal haematopoiesis (CH) are linked to similar comorbidities in the general population, we hypothesized that CH may be more prevalent in people with HIV. To address this issue, we established a prospective cohort study recruiting 220 HIV-positive and 226 HIV-negative participants aged 55 years or older in Australia. Demographic characteristics, clinical data and peripheral blood were collected to assess for the presence of CH mutations and identify potential risk factors for and clinical sequelae of CH. Investigators testing for CH were blinded to participants’ HIV status. In total, 132 CH mutations were identified in 99 (22.2%) of 446 participants. CH was more prevalent in HIV-positive participants than HIV-negative participants (27.7% vs. 16.8%, p =0.006), overall and across all age groups. HIV infection was associated with an increased odds of having CH (adjusted odds ratio 2.10, 95% confidence interval 1.30-3.38, p=0.002). The most common genes mutated were DNMT3A (48.5%), TET2 (20.5%) and ASXL1 (11.4%). CH and HIV infection were independently associated with increases in blood parameters and biomarkers associated with inflammation. These data suggest a selective advantage for the emergence of CH in the context of chronic infection and inflammation related to HIV infection.
Introduction
As effective and well tolerated modern antiretroviral therapy (ART) regimens are becoming widely available in many settings, people with HIV who receive optimal ART are living longer1,2 with life expectancies approaching those of people without HIV3-5. However, HIV infection remains associated with an increased prevalence of comorbidities4,6 such as cardiovascular disease6-8 and non-AIDS defining malignancies7,9. While the reasons for this are not clear, increased comorbidities are found even in people with HIV who are virologically suppressed on ART10,11, suggesting additional factors such as inflammation and immune activation11-13, adverse effects of ART14,15, immunodeficiency9,16,17, and altered coagulation18,19 are playing a role. In addition, traditional risk factors such as smoking20 and alcohol use21 as well as exposure to oncogenic viruses22 also contribute to the increased prevalence of comorbidities in people with HIV.
Clonal haematopoiesis (CH) is characterised by the over production of blood cells derived from a single haematopoietic stem cell (HSC) harbouring somatic mutation(s) that confer a selective clonal advantage. In recent years, large studies in the general population have shown that CH increases with age and is associated with the development of haematologic malignancies, cardiovascular disease, stroke, and all-cause mortality23-27. While the pathophysiology of clonal dominance in CH is still largely unexplained, a number of studies have suggested an important interplay between CH and inflammation28-30. Despite the established causal relationship between chronic viral infections and chronic immunoinflammation, the consequence of a sustained virally-mediated underlying inflammatory state on the prevalence of CH remains unknown. Given the increased incidence of cardiovascular disease and malignancies in people with HIV and the established link between CH and cardiovascular and malignant outcomes in the general population, we sought to evaluate the prevalence of CH among persons with HIV.
The Age-Related Clonal haematopoiesis in an HIV Evaluation cohort (ARCHIVE) study was established to study genomic factors associated with ageing and the development of comorbidities among men and women with and without HIV over the age of 55 years. Our objectives in the ARCHIVE cohort were to: 1) compare the prevalence and type of somatic mutations in people with and without HIV; 2) explore socio-demographic and clinical characteristics among all participants, and characteristics of HIV infection among HIV-positive participants, in order to identify risk factors for the development of CH mutations; and 3) explore clinical outcomes including inflammatory biomarker profiles and medical comorbidities among people with and without somatic mutations, stratified by HIV status.
Methods
Study Design and Population
The detailed ARCHIVE study protocol is included as a supplementary appendix. In brief, the study enrolled participants over the age of 55 years from five high HIV-case load primary care practices and one tertiary hospital (a designated HIV care centre) in Sydney, Australia, and one high HIV-case load primary care practice and two tertiary hospitals (both designated HIV care centres) in Melbourne, Australia. HIV-negative participants were required to have a negative HIV test within 12 months of enrollment.
After providing written informed consent, participants provided a whole blood sample for full blood examination, inflammatory biomarker testing (Supplementary Table S1) and for CH testing. Relevant data were obtained from participants’ medical records including: age, gender, sexual orientation, most recent vital signs, results of routine standard of care blood tests (Supplementary Table S1), medical diagnoses, and use of pre-exposure prophylaxis (PrEP) among HIV-negative participants. For participants with HIV, date of HIV diagnosis, date of initiation of ART, lowest CD4 count on record, most recent CD4 count and HIV viral load, prior exposure to stavudine and zidovudine, which are known to cause myelosuppression31, and current ART regimen were also recorded. All participants were asked to self-complete a questionnaire on their ancestry, physical health / frailty, use of tobacco, alcohol and recreational drugs, and household income. BMI was calculated using height and weight reported from the enrolling clinical site, and was categorised using ranges published by the Centers for Disease Control and Prevention32. Data on sexual orientation was obtained by asking the enrolling clinical site to report whether the participant is sexually active with men, women or both. Sexual orientation categorised as men who have sex with men (MSM) was defined as male participants who were reported by the clinical site as having sex with either men only or both men and women.
Testing for Mutations Associated with Clonal Haematopoiesis
Investigators completing the testing for CH were blinded to participants’ HIV status. DNA was obtained from whole blood from enrolled participants. Screening for clonal haematopoiesis was performed at the Peter MacCallum Cancer Centre using a bespoke targeted deep sequencing (TS) amplicon panel designed across 55 genes recurrently mutated in haematological malignancies33 (Supplementary Methods). Target specific amplification was then performed using the Fluidigm Access Array™ system. Identification of clonal haematopoiesis mutations through variant calling and curation was performed using an in-house pipeline34 as outlined in the Supplementary Methods.
Statistical Considerations
Sample Size Calculation
We assumed that 10% of our HIV-negative participants would have somatic mutations associated with clonal haematopoiesis, which is consistent with published studies in the literature reporting a range of 6-10% in older adults23-25. Testing 220 HIV-positive and 220 HIV-negative participants gave 80% power to detect an increase to 20% prevalence of mutations among HIV-positive participants compared to the background mutation rate of 10% among HIV-negative participants.
Statistical Analysis
Conventional descriptive statistics were used to compare characteristics across HIV-positive and HIV-negative participants; p-values for comparisons were generated using the chi-square test. The primary outcome of interest was the presence of any somatic mutation associated with clonal haematopoiesis. We used logistic regression to calculate the unadjusted and adjusted odds ratios (OR) and 95% confidence interval (CI) for the risk of CH among HIV-positive participants, compared with HIV-negative participants. We adjusted a priori for age, gender and whether the participant had ever smoked, which are factors that have been reported to be associated with clonal haematopoiesis in the general population23-25 and with HIV infection (smoking and gender). We also adjusted for MSM status, which was found to differ slightly across HIV status in our study population.
In exploratory secondary analyses we looked for associations between HIV specific risk factors and CH using logistic regression. We also explored associations between our explanatory variables of interest (HIV infection and presence of CH) and clinical outcomes including elevations of: 1) inflammatory markers, 2) blood cell counts and characteristics and 3) select clinical comorbidities, including cardiovascular disease, malignancies and specifically, haematologic malignancies. Multivariable linear and logistic regression methods, adjusting a priori for age, gender, and history of ever smoking, were used to evaluate the relationship between HIV and CH and our continuous and dichotomous clinical outcomes, respectively. All continuous outcomes underwent natural log (ln) transformation. No adjustments were made to significance levels or confidence intervals for multiple comparisons. The data analysis for this paper was generated using SAS software, Version 9.4 of the SAS System for Windows (Copyright © 2019 SAS Institute Inc., Cary, NC, USA).
Human Subjects
The research protocol, consent form, and associated documents were approved by the relevant Human Research Ethics Committees in both the states of New South Wales and Victoria, Australia, where participants were enrolled. All study participants gave written informed consent to participate in the study.
Results
Study participant characteristics
A total of 461 patients were consented and 446 participants (220 HIV-positive and 226 HIV-negative) were included in the final analysis (Figure 1). Overall, HIV-positive and HIV-negative participants were similar in terms of demographic and clinical characteristics (Table 1, Supplementary Table 1). Among all participants, the median age (IQR) was 63 (59-69) years and 96.2% were male. Among the 390 (97.1%) with available data on sexual orientation from the enrolling clinical site, more HIV-positive participants were reported to be MSM than HIV-negative participants (93.1% and 87.1%, respectively). Of the 446 participants included, 397 (89.0%) completed the on-line questionnaire, including 191 (86.8%) with HIV and 206 (91.2%) without HIV. Half (50.6%) of respondents who completed the questionnaire reported ever using tobacco, though only 11.6% reported currently smoking. The majority (77.5%) of participants reported currently drinking alcohol.
Demographic and clinical characteristics of study participants, overall and by HIV status

1a. Participant enrolment and inclusion in the final analysis
1b. Study analysis design
Vital signs at the time of enrolment, clinical laboratory results available from the medical record, and study pathology results were consistent with a generally healthy study population, although 19.5% of participants were obese, defined as a body mass index ≥30 (Table 1, Supplementary Table 1). Almost all participants (97.5%) were reported by the enrolling clinical site to have at least one medical condition, excluding HIV infection (Table 1 and Supplementary Table 1). The majority (64.8%) had cardiovascular comorbidities, with hypertension (38.3%) and hyperlipidaemia (37.7%) being the most common. Twenty-four percent of participants had a history of malignancy with the majority (61.1%) being skin cancers. HIV-positive participants had a higher prevalence of several medical comorbidities, compared to HIV-negative participants (Supplementary Table 1). HIV-positive participants were found to have lower LDL, and higher triglycerides, creatinine, haemoglobin, lymphocyte count, mean corpuscular volume, interleukin-6 (IL-6), and Cystatin C, than HIV-negative participants (Supplementary Table 1).
Among the 216 HIV-positive participants with available data on date of HIV diagnosis, the median (IQR) number of years from diagnosis to enrolment was 24 (15-31) (Supplementary Table 2). Of the 217 participants with available data on CD4 nadir, 34.6% had a CD4 nadir under 200 cells/mm3. Seventeen percent had a previous AIDS-defining condition; the most common were Pneumocystis jiroveci pneumonia (6.8%), oral candidiasis (5.9%), and Kaposi’s sarcoma (4.1%) (Supplementary Table 1). Most HIV-positive participants (69.6%) had a current CD4 count of ≥ 500 cells/mm3, 95.5% had a current HIV viral load less than 40 copies/mL, and 99.6% were currently taking ART. Of the 211 with available historical ART data, 19.0% initiated ART prior to 1996, when “highly active” ART became widely used in Australia, 41.7% initiated ART from 1996-2005, and 39.3% initiated ART since 2006 when modern ART regimens became available. The median (IQR) number of years since starting ART was 17 (9-21) and 38.4% had been taking ART for 20 years or more.
Multivariable regression analysis of associations between the presence of at least one CH mutation, HIV status, age, gender, and history of ever smoking and clinical outcomes including blood cell counts, inflammatory markers, and comorbidities
Table 2a. Inflammatory markers and FBE (linear regression)
D-dimer and comorbidities1 (logistic regression)
Identification of clonal haematopoiesis mutations
We identified a higher prevalence of CH among HIV-positive participants compared with HIV-negative participants. Overall, CH associated mutations were identified in 99 (22.2%) of all 446 study participants: 61 (27.7%) of the 220 HIV-positive participants and 38 (16.8%) of the 226 HIV-negative participants (p=0.006). The increased prevalence of CH in the HIV-positive cohort was seen across all age groups but was greatest in those over 75 years of age (Figure 2a).

Figure 2a. Proportion of participants with any mutation, by age group and HIV status
Figure 2b. Gene mutations in each participant (N=99 with any mutation; left panel) and proportion of mutations in each gene, by HIV status (right panel)
Figure 2c. Proportion of participants with 0, 1, 2, 3 and 4 mutations, by HIV status
Figure 2d. Variant allele fraction (ln-transformed) over increasing age, by HIV status
A total of 132 CH mutations were identified in the 99 participants; 81 (61.4%) in HIV-positive participants compared with 51 (38.6%) in HIV-negative participants (p =0.002). The majority occurred in three of the main genes identified in other studies of CH in the general population23- 25: DNMT3A (48.5%), TET2 (20.5%) and ASXL1 (11.4%). HIV-positive participants had a higher proportion of mutations in all of these genes, particularly ASXL1, compared with HIV-negative participants (Figure 2b). Overall, missense mutations were the most frequent mutation type (40.2%), although a higher proportion of truncating mutations was observed than previously reported23,24, which included frameshift (34.9%), stop-gained (15.9%), and splice site mutations (6.9%) (Figure 2b, Supplementary Table S3). Further data on mutation characteristics can be found in Supplementary Table S3 and a full list of all identified mutations associated with clonal haematopoiesis can be found in Supplementary Table S4.
More HIV-positive participants had greater than one pathogenic CH mutation detected compared to HIV-negative participants (7.3% vs 4.9%, respectively, p=0.29) (Figure 2c). In addition, the ln-transformed variant allele fractions (VAF) of the identified mutations increased with age at a greater rate among HIV-positive participants, compared with HIV-negative participants (p-value for interaction=0.01, Figure 2d); however, there was no difference in the median (IQR) VAF by HIV status (4.7 [2.6-8.6] in HIV-positive participants vs. 4.0 [2.4-8.4] in HIV-negative participants; p=0.59).
Of the 226 HIV-negative participants, 26.6% had taken PrEP to prevent HIV acquisition and of those, 50% were taking PrEP at the time of enrolment. Of the 96.7% who had available data on what PrEP agent was used, all had used tenofovir/emtricitabine. Among HIV-negative participants, there was no difference in exposure to PrEP among those with and without CH: 26.1% of HIV-negative participants without CH had ever used PrEP vs. 11 (29.0%) of those with one or more CH mutation (p=0.71).
Association between HIV infection and the presence of clonal haematopoiesis mutations
The odds of having at least one CH mutation among HIV-positive participants compared with HIV-negative participants was 2.10 (confidence interval [CI] 1.30-3.38), p=0.002, when adjusted for age, gender, sexual orientation and history of smoking (Figure 3). In addition to fitting linear age in the model, we examined a quadratic term for age but found no statistical significance (p=0.59) We performed a sensitivity analysis of the association between HIV infection and CH by conducting four sub-analyses (mutations with VAF>2%, DNMT3A/TET2/ASXL1 mutations, male participants, and MSM participants) and found no significant differences in our results (Supplementary Tables S5. A-D). Due to the large difference seen across HIV status in ASXL1 mutations and the association between ASXL1 and smoking35, we performed a sensitivity analysis excluding participants with ASXL1 mutations and did not find any significant differences in our results (data not shown).
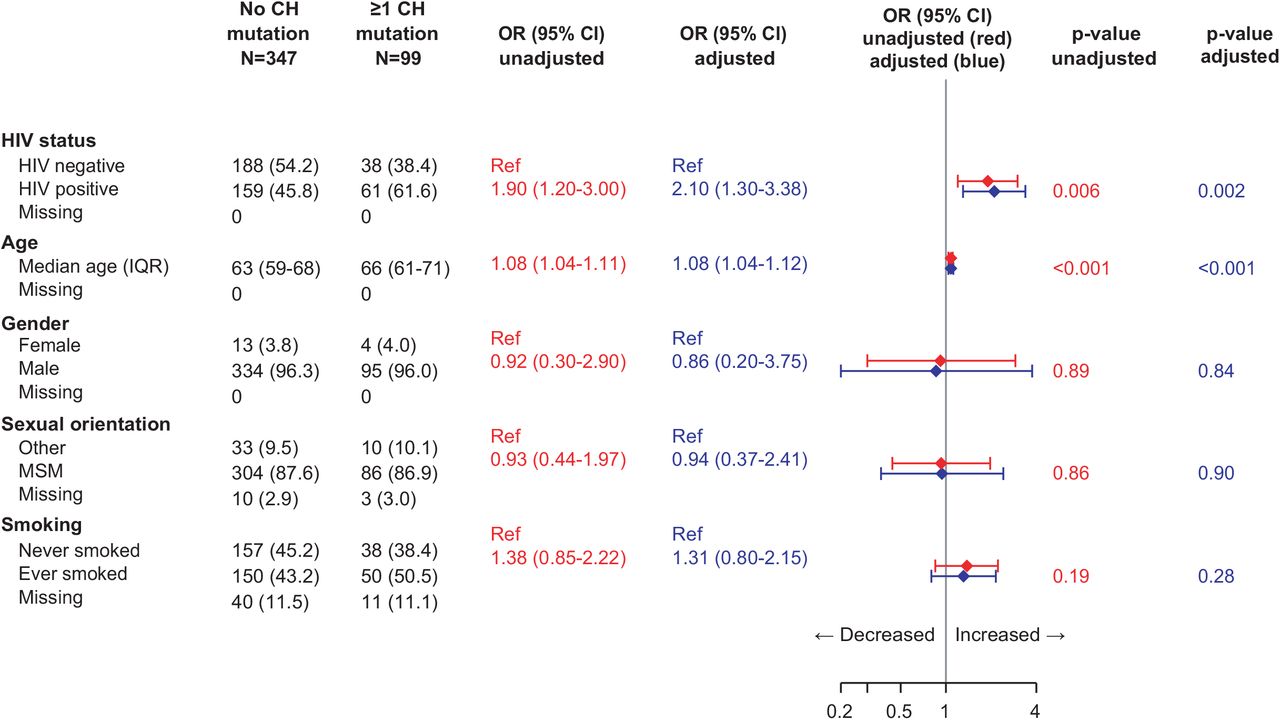
Adjusted and unadjusted estimates for the association between CH mutation and HIV status, age, gender, sexual orientation and smoking
As more HIV-positive participants were enrolled from hospital clinics than HIV-negative participants (64 [29.1%] vs. 11 [4.9%], respectively; p=<0.001), we explored whether this led to a selection bias for more unwell and possibly older, HIV-positive participants, which may have influenced our results towards finding a difference in CH by HIV status. We found no difference in the proportion of participants with and without CH that were enrolled at tertiary care sites (56 [16.1%] vs. 19 [19.2%], respectively; p=0.47) and no difference in the median age of participants enrolled at GP vs. tertiary care sites (median IQR 63 [59-69] vs. 66 [60-69]; p=0.15). In addition, we found no significant difference in the association between HIV and CH shown in Figure 3 when we adjusted for tertiary care vs. GP site in our multivariable model (data not shown).
We explored other factors that might increase the risk of CH in our study population, including ancestry, body mass index, duration and quantity of smoking exposure, alcohol use, recreational and injection drug use, and annual household income, but did not identify any statistically significant covariates (data not shown). Among HIV-positive participants, we did not identify any HIV-specific characteristics that were associated with having an increased risk of CH on univariate analysis (Supplementary Table S6). We also explored whether VAF (averaged within individuals) was correlated with years of HIV infection but did not find a significant correlation (Supplementary Figure 1).
Association between clonal haematopoiesis and clinical outcomes
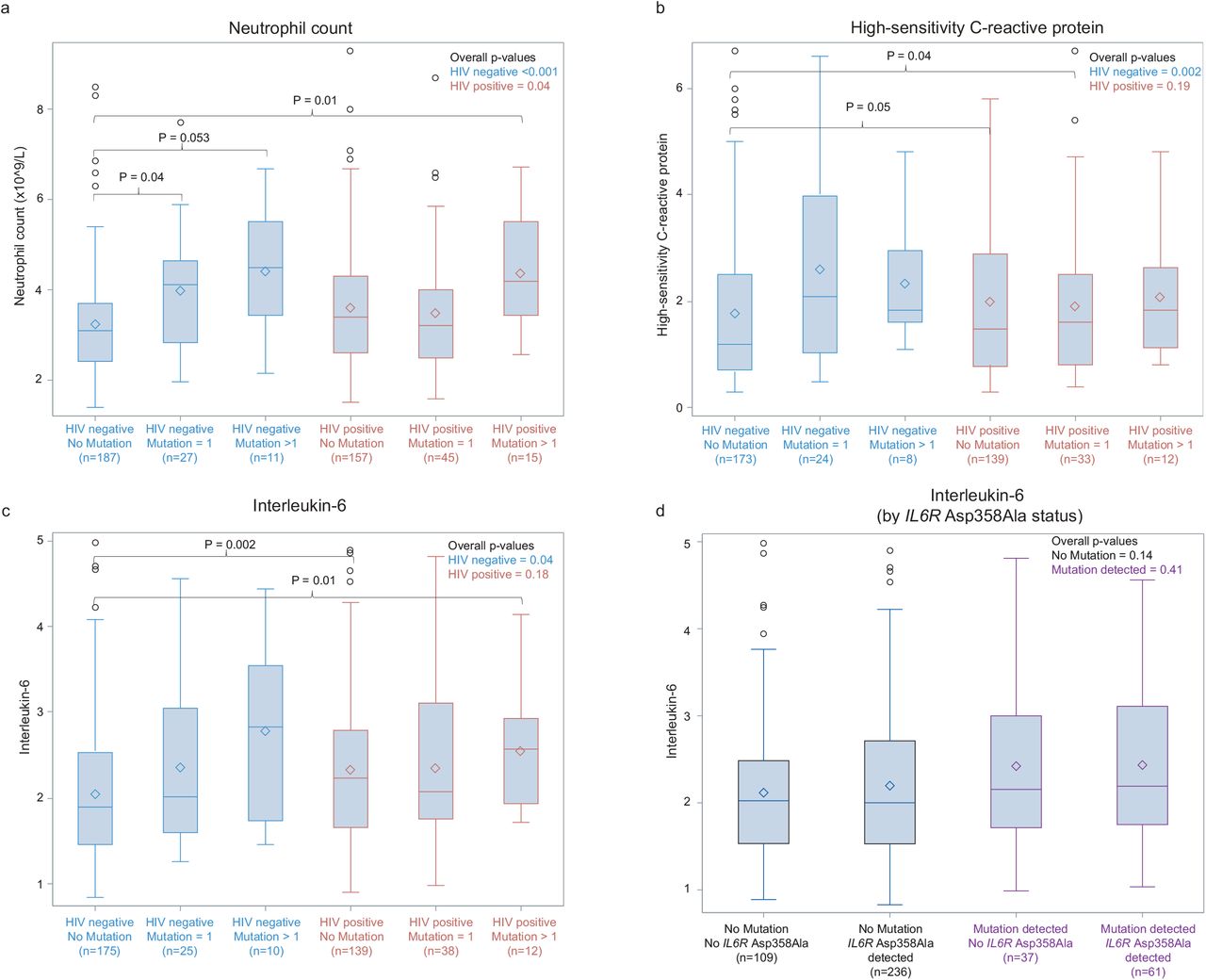
We evaluated clinical outcomes associated with both HIV infection and CH, including blood cell counts and characteristics, inflammatory markers, and select clinical comorbidities. Overall, compared to HIV-negative participants, HIV-positive participants had elevated blood parameters associated with chronic inflammation, including neutrophil count, CRP, and IL-6 (Figure 4 Panels A-C and Supplementary Figure 2 Panels A-C), even in the absence of CH. In the presence of CH, both HIV-negative and HIV-positive participants had increased levels of inflammatory biomarkers. The higher baseline levels seen in HIV-positive participants were increased even further in those with more than one CH mutation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overall p-values comparing trends within subgroups (figure inset) were generated using the Kruskal-Wallis test. P-values across specific groups comparing median values (brackets) were generated using post-hoc pairwise two-sided multiple comparison analysis using the Dwass, Steel, Critchlow-Fligner Method.
Panel A. Neutrophil count by HIV status and presence of 0, 1 and >1 CH mutation
Panel B. High-sensitivity C-reactive protein* by HIV status and presence of 0, 1 and >1 CH mutation
Panel C. Interleukin-6* by HIV status and presence of 0, 1 and >1 CH mutation
Panel D. Interleukin-6* by IL6R p. Asp358Ala status and presence or absence of CH mutations
*Outliers have been removed for box plot presentation only; p-values were calculated including outliers. Outliers were defined as values greater than 1.5 times the IQR above the third quartile.
Interleukin-6 receptor polymorphism (IL6R p. Asp358Ala)
Recent data suggest that the common hypomorphic variant of the IL-6 receptor (IL6R p. Asp358Ala) potentially negates the increased risk of cardiovascular disease observed in patients with CH36. We found within our cohort that there was no significant difference in the prevalence of the IL6 receptor polymorphism by HIV status (62.7% among HIV-positive vs. 70.8% among HIV-negative participants, p=0.07) or across the presence of CH (61.6% among participants with CH vs. 68.3% among participants without CH, p=0.21). We also found that the increased levels of serum IL-6 noted in individuals with CH and patients with HIV infection without CH could not be explained by expression of the IL6R p. Asp358Ala variant (Figure 4 Panel D, Supplementary Figure 2 Panel D).
We also conducted a multivariable regression analysis of the association between the presence of CH, HIV status, and clinical outcomes including FBE characteristics, inflammatory markers and medical comorbidities, adjusting for age, gender and history of smoking, which are known confounders of our clinical outcomes (Table 2). The presence of at least one CH mutation and HIV infection were independently associated with a statistically significant increase (p<0.05) in several blood parameters associated with chronic inflammation (Table 2). However, there were little differences found in other blood count parameters including haemoglobin, platelets or red cell distribution width.
Discussion
In this cohort of HIV-positive and HIV-negative Australian adults over the age of 55, HIV infection was associated with more than twice the odds of having CH, and this association was independent of previously reported risk factors for CH such as smoking, gender and age. Both HIV infection and the presence of CH were independently associated with increases in several parameters associated with inflammation even when adjusting for known risk factors.
We found that the increased prevalence of CH in HIV-positive individuals was most marked in older age groups. Although these individuals had higher numbers of DNMT3A and TET2 mutations, the greatest difference across HIV status occurred in pathogenic mutations in ASXL1 (Figure 2b). Notably, ASXL1 and DNMT3A mutations have been identified to be more frequent in myelodysplastic syndrome (MDS) patients with HIV and are associated with a poorer prognosis37. Whilst MDS remains an incurable disease in the absence of an allogeneic transplantation, the impending emergence of well tolerated novel disease modifying therapies38-40 may argue for better surveillance and early diagnosis in older HIV-positive patients with CH.
Raised inflammatory markers, which are well-documented in HIV infection, have recently been implicated in the pathogenesis of CH28-30,41. Increasing experimental evidence has also highlighted the fact that repeated or sustained exposure to inflammatory stimuli are toxic to normal HSCs ultimately leading to their depletion and bone marrow failure42-44. Remarkably, in the context of sustained chronic inflammation, HSCs with mutations in CH genes such as TET2 have a major competitive advantage45,46. Unlike normal HSCs, TET2 mutant HSCs show reduced apoptosis and enhanced activity in response to inflammatory cytokines, particularly IL645,46. Consistent with our findings, IL-6 is known to be increased in HIV-positive individuals even in those who are virologically-suppressed on highly effective ART regimens19,47. Taken together, these findings raise the prospect that the underlying chronic inflammatory state seen in HIV infection provides the ideal milieu for clonal dominance of HSC with CH mutations and may account for the increased risk of CH seen in HIV-positive individuals. It is also possible that the immunodeficiency associated with acute HIV infection and / or the chronic inflammation and immune activation associated with long-term HIV infection may lead to impaired immune surveillance and reduced clearance of clonal populations of HSC in people with HIV further contributing to the higher prevalence of CH.
Whilst these are the first prospective data from a carefully conducted clinical study designed specifically to investigate the prevalence of CH in people with and without HIV, we note with interest that a recent pre-print describing a retrospective analysis of sequencing data from disparate cohorts, including some individuals with HIV, have confirmed our findings providing independent validation of our study48.
Notably, our cohort only enrolled people over 55 years of age who were predominantly male and MSM in a health system that provides universal access to standard of care antiretrovirals. Further clinical studies in larger and more diverse populations including younger individuals, women with HIV and those who have not had sufficient access to ART are needed to evaluate HIV-specific risk factors for CH. These insights may inform future trial interventions to guide the management of CH in people with HIV.
Data Availability
The data that support the findings of this study are available from the corresponding authors upon reasonable request.
Funding Statement
The Kirby Institute receives funding from the Australian Government Department of Health and Ageing. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Australian Government.
We thank the following funders for fellowship and grant support: NHMRC Investigator Grant (#1196749 - M.A.D), Cancer Council Victoria Dunlop Fellowship (M.A.D), Howard Hughes Medical Institute international research scholarship (M.A.D), NHMRC Investigator Grant (#1196755 - S.J.D), CSL Centenary fellowship (S.J.D), NHMRC Post-Graduate Scholarship (N.J.D.), NHMRC Fellowship (#1110067 – M.N.P), Cancer Institute of NSW Future Research Leader Fellowship (#15-1-01, M.N.P), NHMRC/MRFF Investigator Grant (#1195030 – P.Y.), Snowdome Foundation/Maddie Riewoldt’s vision (P.Y.), Dr George Klempfner, Mrs Yolanda Klempfner AO (P.Y.), and Gilead (P.Y), NHMRC Project Grant (#1128984 to S.J.D and M.A.D), NHMRC Program Grant (#1213110).
Financial Disclosures
M.A.D. has been a member of advisory boards for CTX CRC, Storm Therapeutics, Celgene and Cambridge Epigenetix. S.J.D has been a member of advisory boards for Astra Zeneca. The S.J.D. lab has received funding from CTx CRC and Genentech. The M.A.D. lab received research funding from CTx CRC. N.J.D. has received research support from Gilead Sciences Australia. D.E.S. has received research support and consultancy fees from: Gilead Sciences Australia, Janssen pharmaceuticals, Merck and Co, Sydney, Australia. J.H.’s institution has received reimbursement for her involvement in Advisory Boards for Gilead Sciences, Merch, Sharp & Dohme Australia and ViiV Healthcare. M.B. has received support for medical advisory boards, lecturing and attendance at scientific conferences from Gilead Sciences, ViiV Healthcare and Abbvie and his institution has received research support from Gilead Sciences, ViiV Healthcare, GSK, Abbvie, MSD, Amgen, and Eli Lilly.
Acknowledgements
The authors would like to thank all of the patients that participated in this study. We also acknowledge the following clinical site study coordinators: Trina Vincent, Holdsworth House Medical Practice; Ricardo Rosario, East Sydney Doctors; Helen Lau, Prahran Market Clinic; Florence Bascombe, St Vincent’s Hospital Sydney; Denise Smith, Albion Centre; Sally Price, Alfred Hospital; Jessica O’Brien, Monash Health; Hooi Theng Lynn Tan, Taylor Square Private Clinic; Brett Sinclair, Department of Sexual Health Medicine, Sydney Local Health District.
Statistical analyses were completed by N.J.D and P.Y
References



