
Abstract
Abnormally phosphorylated tau, an indicator of Alzheimer’s disease, begins to accumulate in the first decades of life in the locus coeruleus (LC), the primary source of cortical norepinephrine. Ensuing dysfunction in noradrenergic neuromodulation is hypothesized to contribute to Alzheimer’s progression. However, research into the role of the LC has been impeded by a lack of effective ways of assessing it in vivo. Advances in high-resolution brainstem magnetic resonance imaging (MRI) hold potential to investigate the association of locus coeruleus integrity and Alzheimer’s-related neuropathological markers in vivo.
Leveraging a meta-analytical approach, we first synthesized LC localizations and dimensions across previously published studies to improve the reliability and validity of MR-based locus coeruleus detection. Next, we applied this refined volume of interest to determine whether MR-indexed LC integrity can serve as a marker for noradrenergic degeneration in early-onset Alzheimer’s disease. Eighteen participants (34.7±10.1 years; 9♀) with or known to be at-risk for mutations in genes associated with autosomal-dominant Alzheimer’s disease (ADAD) were investigated. Genotyping confirmed mutations in seven participants (PSEN1, n = 6; APP, n = 1), of which four were symptomatic. Participants underwent 3T-MRI, flortaucipir positron emission tomography (PET), and cognitive testing. LC MRI intensity, a non-invasive proxy for neuronal density, was semi-automatically extracted from high-resolution brainstem scans across the rostrocaudal extent of the nucleus.
Relative to healthy controls, symptomatic participants showed lower LC intensity. This effect was pronounced in rostral segments of the nucleus that project to the mediotemporal lobe and other memory-relevant areas. Among carriers of ADAD-causing mutations, closer proximity to the mutation-specific median age of dementia diagnosis was associated with lower LC intensity. Leveraging a multivariate statistical approach, we revealed a pattern of LC-related tau pathology in occipito-temporo-parietal brain regions. Finally, higher locus intensity was closely linked to memory performance across a variety of neuropsychological tests.
Our finding of diminished MR-indexed LC integrity in autosomal-dominant Alzheimer’s disease suggest a role of the noradrenergic system in this neurodegenerative disease.
Introduction
Alzheimer’s disease (AD) is presently an incurable neurodegenerative disease leading to dementia with the number of worldwide cases predicted to triple over the next thirty years (Alzheimer’s Disease International, 2019; Canter, Penney, & Tsai, 2016; World Health Organization, 2004). Post-mortem studies indicate that abnormally phosphorylated tau, an indicator of AD, begins to appear early in life in the locus coeruleus (LC), the primary source of cortical norepinephrine (Braak, Thal, Ghebremedhin, & Del Tredici, 2011; Ehrenberg et al., 2017; Poe et al., 2020; Stratmann et al., 2016; Theofilas, Dunlop, Heinsen, & Grinberg, 2015). With increasing age, abnormal tau appears in a characteristic topographical sequence in noradrenergic projection targets like the mediotemporal lobe (referred to as Braak stages, a classification system of the progression of tau spread; Braak et al., 2011; Chalermpalanupap, Weinshenker, & Rorabaugh, 2017; Stratmann et al., 2016). An animal model indicates that injecting hyperphosphorylated human tau into the rodent LC leads to its slow spread to other brainstem nuclei and eventually to cortical regions (Ghosh et al., 2019).
Notably, tau deposition is strongly linked to both neural and cognitive decline in Alzheimer’s (Hanseeuw et al., 2019; Jagust, 2018; La Joie et al., 2020). Tau burden in the LC increases linearly with the progression of Braak stages while noradrenergic neurons first decrease in size and then degenerate (Ehrenberg et al., 2017; Kelly et al., 2017; Theofilas et al., 2017). Accordingly, a meta-analysis of twenty-four post-mortem investigations revealed substantive cell loss in the LC of Alzheimer’s patients relative to controls (mean d = 2.28; 95 % CI = 2.06–2.51; Lyness, Zarow, & Chui, 2003), with reduced neuron counts evident already at prodromal stages of the disease (Arendt, Brückner, Morawski, Jäger, & Gertz, 2015; Kelly et al., 2017). Topographically, noradrenergic neurodegeneration is most pronounced in rostral and middle segments of the nucleus that project to the hippocampus and other memory-relevant areas (Ehrenberg et al., 2017; Lyness et al., 2003). LC degeneration, however, does not only constitute a consequence of Alzheimer’s pathology but also contributes to its disease development (Marien, Colpaert, & Rosenquist, 2004; Mather & Harley, 2016; Satoh & Iijima, 2019; Weinshenker, 2018). Studies with genetically modified animals indicate that abnormally phosphorylated tau in the LC leads to dysfunctional noradrenergic neuromodulation in memory-relevant brain areas (Ghosh et al., 2019; Rorabaugh et al., 2017; Weinshenker, 2018) and that tau pathology and LC degeneration synergistically aggravate neural and behavioral deterioration (Chalermpalanupap et al., 2018; also see Jacobs, Riphagen, Ramakers, & Verhey, 2019). Specifically, experimentally decreased norepinephrine levels have been associated with increased tau and amyloid-β deposition, another hallmark of AD (Chalermpalanupap et al., 2018; Heneka et al., 2010). Insights into the role of noradrenergic neurodegeneration in the progression of AD are thus of high clinical significance (Grinberg & Heinsen, 2017), yet in-vivo human data is missing.
Studies in humans have long been impeded by methodological challenges in non-invasive assessments of the LC due to its small size and its location deep within the brainstem (for discussions, see Astafiev, Snyder, Shulman, & Corbetta, 2010; Keren, Lozar, Harris, Morgan, & Eckert, 2009). Advances in high-resolution brainstem magnetic resonance imaging (MRI) may help the field overcome these hurdles (Betts, Kirilina, et al., 2019; Liu et al., 2017). Over the last fifteen years, several MRI sequences have been developed that reveal the LC as a hyperintense cluster of voxels bordering the fourth ventricle (e.g., Betts, Cardenas-Blanco, Kanowski, Jessen, & Düzel, 2017; Nakane, Nihashi, Kawai, & Naganawa, 2008; Priovoulos et al., 2017; Sasaki et al., 2006). Keren and colleagues (2015) validated a MR-based LC imaging sequence by first scanning human post-mortem samples at ultra-high field strength and afterwards performing histological analyses of the same samples. They demonstrated that the hyperintensities observed on MRI scans closely co-localize with noradrenergic cells as identified by tyrosine hydroxylase (the rate-limiting enzyme of catecholamine synthesis) staining, opening the door for non-invasive LC assessments (Keren et al., 2015; also see Cassidy et al., 2019 for a postmortem validation in dopaminergic structures and Betts, Kirilina, et al., 2019 for a discussion of potential contrast mechanisms).
Probing the utility of LC MRI to detect pathology-related changes in the noradrenergic system in vivo, several studies compared patients diagnosed with AD to healthy controls (Betts, Cardenas-Blanco, et al., 2019; Dordevic et al., 2017; Miyoshi et al., 2013; Takahashi et al., 2015). In general agreement with earlier post-mortem investigations (Lyness et al., 2003), the majority of studies observed lower LC MRI intensity, a proxy for the density of noradrenergic cells (Keren et al., 2015), in the patient groups (but see Miyoshi et al., 2013).
However, all of these studies investigated the by far most common, late-onset type of AD (>65 years; LOAD). LOAD is considered a heterogeneous, age-related disease that encompasses not only tau and amyloid pathology but also the aggregation of other proteins such as α-synuclein and cerebro-vascular influences (Jagust, 2018; Van Cauwenberghe, Van Broeckhoven, & Sleegers, 2016). Given that large lifespan studies suggest spatially confined age differences in LC integrity in healthy older adults (Dahl et al., 2019; Liu et al., 2019), unambiguously distinguishing disease-from age-related changes on this basis is challenging (Lindenberger, von Oertzen, Ghisletta, & Hertzog, 2011). Focusing instead on forms of AD that begin early in life allows the possibility of distinguishing age-from disease-related changes (cf. Jacobs, Becker, et al., 2019).
Autosomal dominant Alzheimer’s (ADAD) is a rare inherited disease caused by mutations in genes associated with the generation or accumulation of amyloid-β (Bertram, Lill, & Tanzi, 2010; Tanzi & Bertram, 2005; Van Cauwenberghe et al., 2016). In contrast to LOAD, it constitutes a relatively “pure” tau and amyloid pathology in which cerebrovascular- or other age-related neuropathological changes are absent (Jagust, 2018). In ADAD, symptoms develop early in life with a relatively predictable age at onset (Ryman et al., 2014), thus providing a unique window into the pathogenesis of Alzheimer’s (Bateman et al., 2012; Ringman, 2005). Whether or not there is MR-identifiable LC degeneration also in patients diagnosed with Alzheimer’s dementia early in life is still an open question. Importantly, answering this question could help shed light on whether LC involvement is a core feature of AD or whether it should be considered more indicative of a non-Alzheimer’s process generally associated with aging, such as the process outlined in the “primary age-related tauopathy” framework (Crary et al., 2014).
While previous post-mortem research suggests a topographical pattern of noradrenergic neurodegeneration within the LC in LOAD (Ehrenberg et al., 2017; Lyness et al., 2003), most current in-vivo (MRI) studies lack the spatial specificity to draw comparable conclusions. That is, they report disease-related differences in MR-indexed LC integrity (Dordevic et al., 2017; Takahashi et al., 2015) without exploring potential topographical patterns therein, precluding direct comparisons (but see Betts, Cardenas-Blanco, et al., 2019). Investigations in healthy participants successfully applied LC MRI to map the spatial extent of the central noradrenergic nucleus in standard space (Betts et al., 2017; Dahl et al., 2019; Keren et al., 2009; Liu et al., 2019; Tona et al., 2017; Ye et al., 2020), paving the way for topographical cross-study comparisons. However, estimates of locus coeruleus’ dimensions and localizations show a sizeable variance across publications (range of agreement: 48–94 %; cf. Dahl et al., 2019; Liu et al., 2019; Ye et al., 2020; or even 1–40 % using a different methodology, Mäki-Marttunen & Espeseth, 2020). Such lack of consensus considerably limits the replicability of findings and impedes scientific progress.
Thus, the present study pursued two main goals: First, we aimed at improving the reliability and validity of MR-based LC detection. Leveraging a meta-analytical approach, we aggregated across previously published maps of the LC (Betts et al., 2017; Dahl et al., 2019; Keren et al., 2009; Liu et al., 2019; Tona et al., 2017; Ye et al., 2020) to derive a biologically plausible volume of interest (meta mask) that shows high agreement across investigations. Second, we aimed at determining whether MR-indexed LC integrity can serve as marker for noradrenergic degeneration in early-onset Alzheimer’s disease. To this end, we applied the newly generated meta mask to an independent clinical sample to semi-automatically extract MR-indexed LC integrity across the rostrocaudal extent of the nucleus (cf. Dahl et al., 2019). We specifically focused on a sample of participants with or known to be at-risk for rare mutations in genes causing ADAD (Goate et al., 1991; Murrell et al., 2006; Yescas et al., 2006). We hypothesized that middle to rostral MR-indexed LC integrity would be lower in symptomatic participants relative to healthy matched controls, corroborating earlier post-mortem findings (in LOAD; Lyness et al., 2003). Moreover, we predicted LC integrity would be associated with cortical tau burden (Chalermpalanupap et al., 2018), as assessed using positron emission tomography (PET), and attention and memory performance (Dahl et al., 2019; Liu et al., 2020).
Methods
Aggregating across published locus coeruleus maps to derive a high confidence meta mask
Previous mapping studies used a variety of LC-sensitive MRI sequences (Turbo Spin Echo [TSE; Dahl et al., 2019; Keren et al., 2009; Tona et al., 2017]; Magnetization Transfer [MT; Liu et al., 2019; Ye et al., 2020]; Fast Low Angle Shot [FLASH; Betts et al., 2017]) at different field strength (7 Tesla: Ye et al., 2020; 3 Tesla: all other studies) to visualize the nucleus. Most investigations were conducted across younger and older adults or even within lifespan samples (but see Tona et al., 2017 and Ye et al., 2020 for studies in younger and older adults, respectively). After data collection, individual brainstem scans were transformed into a group or standard space in which a manual (Betts et al., 2017; Liu et al., 2019; Tona et al., 2017) or semi-automatic (Dahl et al., 2019; Keren et al., 2009; Ye et al., 2020) approach was taken to segment the LC from surrounding tissue. While some earlier reports (Dahl et al., 2019; Liu et al., 2019; Ye et al., 2020) include a comparison of a subset of the published masks, to date there is no systematic evaluation of their agreement. More importantly, no previous study attempted to resolve the apparent disagreement in LC dimensions and localizations across publications.
In keeping with earlier analyses (Dahl et al., 2019; Liu et al., 2019; Ye et al., 2020), the LC masks noted in Table 1 were used for cross-study comparisons. Before relating different masks to one-another, all volumes were binarized and moved to a common space (MNI-ICBM 152 linear space, 0.5 mm resolution), if necessary. In standard space, first an unthresholded aggregate mask was generated using the following formula:
Locus coeruleus masks included in comparisons
 Whereby n denotes the number of masks included in the analyses (n = 6) and v denotes the value for a given voxel (either zero [non-LC tissue] or one [LC]). That is, at every voxel the individual binarized masks were averaged, resulting in an aggregate mask (LCaggregate; see Figure 1). The generated volume, LCaggregate, showed a value range between 0 and 1 (complete agreement that a voxel does not/does belong to the LC, respectively) in steps of
Whereby n denotes the number of masks included in the analyses (n = 6) and v denotes the value for a given voxel (either zero [non-LC tissue] or one [LC]). That is, at every voxel the individual binarized masks were averaged, resulting in an aggregate mask (LCaggregate; see Figure 1). The generated volume, LCaggregate, showed a value range between 0 and 1 (complete agreement that a voxel does not/does belong to the LC, respectively) in steps of  . Please note that we decided against weighing the contribution of the individual masks to the LCaggregate by sample size as two masks (Dahl et al., 2019; Liu et al., 2019) account for more than 80 % of the total number of participants (see Table 1). Hence, the aggregate would be strongly biased in favor of a subset of masks that are themselves highly spatially congruent (agreement 94%; Liu et al., 2019).
. Please note that we decided against weighing the contribution of the individual masks to the LCaggregate by sample size as two masks (Dahl et al., 2019; Liu et al., 2019) account for more than 80 % of the total number of participants (see Table 1). Hence, the aggregate would be strongly biased in favor of a subset of masks that are themselves highly spatially congruent (agreement 94%; Liu et al., 2019).
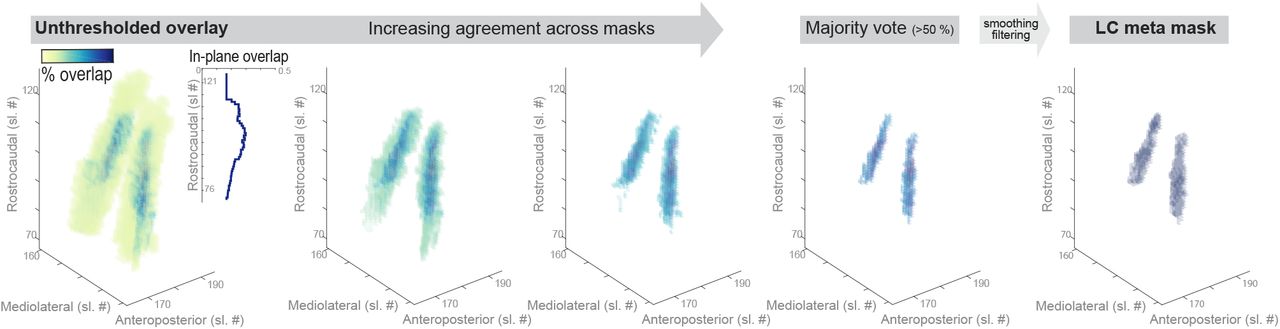
Aggregating across published locus coeruleus (LC) maps yields high confidence meta mask. Left. Unthresholded voxel-by-voxel average across published LC masks. Areas with voxels that are consistently judged to belong to the LC are shown in dark blue while low agreement areas are shown in yellow. Inlay. Agreement across masks (averaged across voxels in-plane) is lowest in most rostral and caudal regions. Middle. Pruning low agreement areas isolates a core of high confidence voxels. Right. Smoothing and filtering the thresholded overlay yields a biologically plausible LC volume of interest (rostrocaudal extent of 14 mm; volume of 74 mm3 [592 voxels]), well corresponding to earlier post-mortem reports (Fernandes et al., 2012). Sl. #, slice number in MNI 152 lin (0.5 mm) space; The LC meta mask is available for download via: osf.io/sf2ky/).
In a second step, the aggregate mask was pruned by removing low-agreement voxels until a majority vote was achieved. That is, only areas with agreement values > 50% were retained (i.e. more than  masks voted for a voxel to belong to the LC). Essentially, the described mask generation process is comparable to label fusion with majority voting (Rohlfing, Brandt, Menzel, & Maurer, 2004; Sabuncu, Yeo, Van Leemput, Fischl, & Golland, 2010; Wang et al., 2013).
masks voted for a voxel to belong to the LC). Essentially, the described mask generation process is comparable to label fusion with majority voting (Rohlfing, Brandt, Menzel, & Maurer, 2004; Sabuncu, Yeo, Van Leemput, Fischl, & Golland, 2010; Wang et al., 2013).
Finally, to obtain a biologically more plausible volume, the pruned aggregate mask was smoothed with a 0.1 mm full width at half maximum (FWHM) kernel using SPM12 (Penny, Friston, Ashburner, Kiebel, & Nichols, 2007) in Matlab (The MathWorks Inc., Natick, MA, USA). Voxels exceeding a threshold of 0.05 were considered part of the LC in the meta mask (LCmetaMask; see Figure 1). The resulting mask had a rostrocaudal extent of 14 mm and a volume of 74 mm3 (592 voxels), corresponding well with previous post-mortem findings (Fernandes, Regala, Correia, & Gonçalves-Ferreira, 2012; Tona et al., 2017). We share the generated meta mask with the scientific community via osf.io/sf2ky/
Evaluation of previously published locus coeruleus masks
Once a high-agreement volume of interest (LCmetaMask) was established, published locus coeruleus masks were compared regarding their specificity and sensitivity. That is, we evaluated (1) how many voxels of a given mask fell within the LCmetaMask relative to the total number of voxels in that mask and (2) how many voxels of the LCmetaMask were included in each mask (relative to the total number of voxels in the LCmetaMask). The mean of the quality metrics (specificity, sensitivity) was taken as indicator for the accuracy of a mask.
Application of locus coeruleus meta mask to an independent clinical sample Study design and participants
To determine whether the LCmetaMask can detect clinically significant differences in LC integrity, eighteen participants with or known to be at-risk for mutations in genes associated with ADAD were investigated (34.7 ± 10.1 years [mean ± standard deviation]; 9♀; see Table 2). Data were acquired as part of an ongoing study employing the Human Connectome Protocol (HCP) in ADAD (NIH U01AG051218, PI: Ringman; see adrc.usc.edu/scientists-researchers/ for more details). Genotyping confirmed mutations in seven of the eighteen participants (Presenilin-1 protein gene [PSEN1], n = 6; Amyloid-β Precursor Protein gene [APP], n = 1; Goate et al., 1991; Murrell et al., 2006; Yescas et al., 2006), of which four were symptomatic (see Table 2). Participants underwent 3 T MRI, flortaucipir PET, and cognitive testing. LC MR-intensity, a non-invasive proxy for neuronal density (Keren et al., 2015), was semi-automatically extracted from high-resolution brainstem scans (Dahl et al., 2019). LC ratios—that is, a ratio of peak LC intensity standardized to a pontine reference (Betts, Kirilina, et al., 2019; Liu et al., 2017)—were computed across the rostrocaudal extent of the nucleus. Standard uptake value ratios (SUVR) were calculated from partial volume corrected flortaucipir PET data using cerebellar gray matter as the reference based on the PETSurfer tool from FreeSurfer (Greve et al., 2014). SUVR images were mapped to the cortical surface which was parcellated into 36 regions of interest (Desikan et al., 2006). Univariate associations between LC ratios, clinical variables, cognitive status, and tau burden were evaluated using non-parametric Wilcoxon rank sum tests (also called Mann-Whitney U-tests) and bootstrapped Spearman’s correlations. The multivariate pattern between LC ratios, cortical tau burden and cognitive decline was evaluated using a partial least squares correlation (see below; Krishnan, Williams, McIntosh, & Abdi, 2011; McIntosh & Lobaugh, 2004).
Descriptive statistics for subgroups
While the ADAD HCP study also includes a limited number of cases with or at risk for late-onset Alzheimer’s (LOAD; with available LC MR-data: n = 7, [4 symptomatic]; 69.6 ± 8.3 years [mean ± standard deviation]), due to the small sample size and different age distribution in combination with reports of age differences in locus coeruleus ratios (Betts et al., 2017; Dahl et al., 2019; Liu et al., 2019; Shibata et al., 2006) we excluded these from further analyses.
Assessment of imaging data
Structural MRI data were collected employing a 3 T Siemens Prisma scanner with a 32-channel head coil following a Human Connectome Project imaging approach (HCP; cf. humanconnectome.org/). Only those sequences used in the current analyses are described below.
A three-dimensional (3D) T1-weighted magnetization prepared gradient-echo (MPRAGE) sequence with a duration of 6:38 min and the following parameters was applied: repetition time (TR) = 2400 ms; echo time (TE) = 2.22 ms; inversion time (TI) = 1000 ms; flip angle = 8°; bandwidth = 220 Hz/Px; dimensions = 208 × 300 × 320; isometric voxel size = 0.8 mm3. Based on this whole-brain (MPRAGE) sequence, a high-resolution, two-dimensional (2D) T1-weighted TSE sequence was aligned perpendicularly to the plane of the brainstem. Acquisition of the TSE sequence took 1:53 min, and the following parameters were used: TR = 750 ms; TE = 10 ms; flip angle = 120°; bandwidth = 285 Hz/Px; dimensions = 512 × 512 × 11; anisometric voxel size = 0.43 × 0.43 × 3.5 mm3 (mimicking the elongated shape of the locus coeruleus). Each TSE scan consisted of eleven axial slices.
PET data were collected using a 3 T Siemens Prisma scanner within the period of 90– 120 min after the injection of the compound 18F-AV-1451 (total dose: 344 MBq). Low dose computerized tomography (CT) scans were acquired prior to the PET scans for attenuation correction. The dynamic PET scans included six frames of five-minute duration, with the dimensions of 168 × 168 × 56 and a voxel size of 1.5 × 1.5 × 4 mm3. The six dynamic scans were rigidly aligned to the first one and averaged to create a static image for SUVR-based analysis.
Semi-automatic locus coeruleus intensity assessment using meta mask
Leveraging the generated LCmetaMask (see above), locus coeruleus intensity was semi-automatically extracted using a previously validated pipeline (Dahl et al., 2019; also see Ye et al., 2020 for a comparable approach). In short, individual whole brain and brainstem scans were iteratively aligned across participants using a template-based procedure implemented in Advanced Normalization Tools (version 2.1; ANTs; Avants et al., 2011; Avants, Tustison, & Song, 2009), and subsequently transformed to standard space (MNI-ICBM 152 linear, 0.5 mm; see Dahl et al., 2019 for a step-by-step description of the standardization). In standard space, individual brainstem scans were masked using the high-confidence LCmetaMask to remove non-LC tissue (using SPM12 in Matlab). To allow inter-subject comparisons of LC data, a normalization of the arbitrarily scaled MR-intensity values is required (Betts, Kirilina, et al., 2019). Thus, brainstem scans were additionally masked using a reference volume of interest positioned in the central pontine white matter, as previously suggested (Ye et al., 2020; dimensions: 4 × 4 mm in plane, following the LCmetaMask with a constant distance of 8.5 mm [y-dimension] along the rostrocaudal axis; see Figure 3). Within the masked brainstem scans, we then fully automatically searched for voxels of brightest intensity in the LC and reference regions. Next, individual, spatially-resolved LC intensity ratios were computed for each slice using the following formula (Dahl et al., 2019; Liu et al., 2017):

LC-related hyperintensity is accurately captured by meta mask. Upper row. Axial and coronal view of brainstem template overlaid on standard MNI brain. Inlays. The area surrounding the fourth ventricle is depicted with (1) a greyscale colormap and (2) a black-to-white-to-red colormap to highlight hyperintense areas. (3) LC-related hyperintensities closely overlap with the LC meta mask (blue overlay; white overlay, pontine reference region). Lower row. 3-D representation of (a) the LC meta mask, (b) above-average intensity voxels, and (c) their overlap from a front and back view. Sl. #, slice number in MNI 152 linear (0.5 mm) space; LC, locus coeruleus. Right hemisphere is plotted on the left.
 Where max(LC) denotes the peak intensity for a given slice in the LC volume of interest and max(Ref) indicates the peak intensity in the reference region. After extraction, ratios of the left and right hemisphere were averaged for further analyses to obtain more stable intensity estimates. Finally, the peak ratio across the rostrocaudal LC extent was calculated as proxy for overall locus coeruleus integrity.
Where max(LC) denotes the peak intensity for a given slice in the LC volume of interest and max(Ref) indicates the peak intensity in the reference region. After extraction, ratios of the left and right hemisphere were averaged for further analyses to obtain more stable intensity estimates. Finally, the peak ratio across the rostrocaudal LC extent was calculated as proxy for overall locus coeruleus integrity.
Assessment of cortical tau burden
To evaluate the association of MR-indexed LC integrity to hallmarks of Alzheimer’s disease, we calculated cortical tau burden from flortaucipir PET data.
First, each participant’s whole brain MR data (MPRAGE) was preprocessed using a HCP pipeline (version 3.27; Makropoulos et al., 2018). Next, the cortical surface was reconstructed and parcellated into thirty-six anatomical regions of interest using Freesurfer 6.0 (Dale, Fischl, & Sereno, 1999; Desikan et al., 2006). Flortaucipir PET images were then co-registered within participants to whole brain (MPRAGE) native space. The Muller-Gartner (MG) method was used for partial volume correction of the PET data, as implemented in PETSurfer (Greve et al., 2016). Standard uptake value ratios (SUVR) were calculated using cerebellar gray matter as reference region. Finally, partial-volume corrected SUVR images were mapped to the cortical surface and parcellated into thirty-six regions of interest (Desikan et al., 2006). For further analyses, each region’s SUVR data were averaged across hemispheres to obtain more stable estimates of cortical tau burden. Tau PET data were not available for two subjects.
Association of locus coeruleus intensity and cortical tau burden
We employed a multivariate statistical approach to assess the relation between MR-indexed locus coeruleus integrity and tau pathology across the cortex. Specifically, using a Partial Least Squares Correlation (PLSC; Krishnan et al., 2011; McIntosh & Lobaugh, 2004) we estimated a latent tau pathology profile that is maximally related to LC integrity (cf. Keresztes et al., 2017; Muehlroth et al., 2020).
First, a between-person Pearson’s correlation matrix (R) was computed between the overall LC ratios (i.e., a vector YLC with nParticipants × 1 [overall intensity ratios]) and the tau SUVR data (i.e., a matrix XTau with nParticipants × 36 [regions of interest]). This correlation matrix (RLC,Tau = YLCTXTau) was then decomposed into three matrices using a singular value decomposition (SVD; SVD(RLC,Tau) = USVT). Whereby U refers to a left singular vector of LC weights, VT denotes a right singular matrix of regional tau weights, and S is a diagonal matrix of singular values. Based on this matrix decomposition, a single latent variable was extracted. The latent variable optimally expresses (in a least squares sense) the pattern of interindividual differences in regional tau burden that shares the largest amount of variance with interindividual differences in overall LC intensity ratios. The statistical strength of the extracted pattern (i.e., the latent variable) was evaluated using a permutation test (by randomly re-ordering the observations in XTau while leaving YLC unchanged and re-calculating the SVD; nPermutations = 10,000). Subsequently, the reliability of the contribution (i.e., weights [VT]) of individual cortical regions, that is, the columns in XTau, to this latent variable was determined using a bootstrapping procedure (nBootraps = 10,000). A ratio of the region-specific weights (VT) and their corresponding bootstrapped standard errors provided bootstrap ratios (BSR) that can be interpreted akin to Z-scores. Finally, multiplying participants’ regional pattern of tau pathology (XTau) with each regions’ contribution to the latent variable (i.e., its weight, VT) yielded a summary measure, reflecting participants’ LC-related tau pathology.
Cognitive assessments
Participants completed a series of standardized neuropsychological tests to assess potential attention and memory deficits. The cognitive assessment included widely used screening instruments for mild cognitive impairment and dementia (the Montreal Cognitive Assessment [MoCA, Nasreddine et al., 2005]; the Cognitive Abilities Screening Instrument [CASI; Teng et al., 1994], and the Washington University Clinical Dementia Rating Scale [CDR; measure: sum of boxes; cf. O’Bryant et al., 2008]). In addition, attention (Digit-Symbol-Substitution Test [DSST; Wechsler, 1981]; Digit Span [measure: backward report; Wechsler, 1997], Trail Making Test [measure: part B; Tombaugh, 2004]) and memory performance were assessed (the Spanish English Verbal Learning Test [SEVLT; measures: average performance over learning trials and delayed recall; González, Mungas, & Haan, 2002], a learning and memory test akin to the Rey Auditory Verbal Learning Test [RAVLT] in which Spanish and English versions were simultaneously developed; Benson Complex Figure Test [measure: delayed recall; cf. Possin, Laluz, Alcantar, Miller, & Kramer, 2011]; and the Craft Story Test [delayed recall; Craft et al., 1996]). When available, for further analyses individual test scores were transformed to Z-scores using published normative data.
A partial least squares correlation (PLSC; Krishnan et al., 2011; McIntosh & Lobaugh, 2004) was applied to capture the multivariate association between MR-indexed LC integrity and cognitive performance, using the same methods as described above.
Data availability
The here described LC meta mask as well as pontine reference mask is available for download on an Open Science Framework repository (osf.io/sf2ky/). All sources for previously published masks are listed in Table 1. For access to raw imaging and clinical data, please refer to the HCP (https://nda.nih.gov/ccf).
Results
Aggregating across published locus coeruleus maps yields high confidence meta mask
Previously published masks of the LC (Betts et al., 2017; Dahl et al., 2019; Keren et al., 2009; Liu et al., 2019; Tona et al., 2017; Ye et al., 2020) were averaged voxel-per-voxel to generate an unthresholded overlay (LCaggregate). The LCaggregate demonstrated a core of voxels that, across publications, were consistently judged to belong to the LC (see dark-blue areas in Figure 1), surrounded by a cloud of ambiguous, low-agreement voxels (see yellow areas in Figure 1). Topographically, consensus was lowest in most rostral and caudal areas (see inlay in Figure 1).
Pruning low-agreement voxels yielded a high-confidence LC volume of interest (LCmetaMask; available for download via: osf.io/sf2ky/) that matches the dimensions reported in post-mortem investigations (Fernandes et al., 2012) and allows assessment of the accuracy of previously published masks.
Accuracy of previously published locus coeruleus masks
Once a high-confidence LC volume of interest (LCmetaMask) was generated, published masks were evaluated regarding their specificity and sensitivity. That is, we assessed (1) how many voxels judged by a given mask as belonging to the locus coeruleus were part of the LCmetaMask, and (2) what percentage of the LCmetaMask was included in each individual mask. The mean across specificity and sensitivity was taken as accuracy measure to rank the masks (see Figure 2).

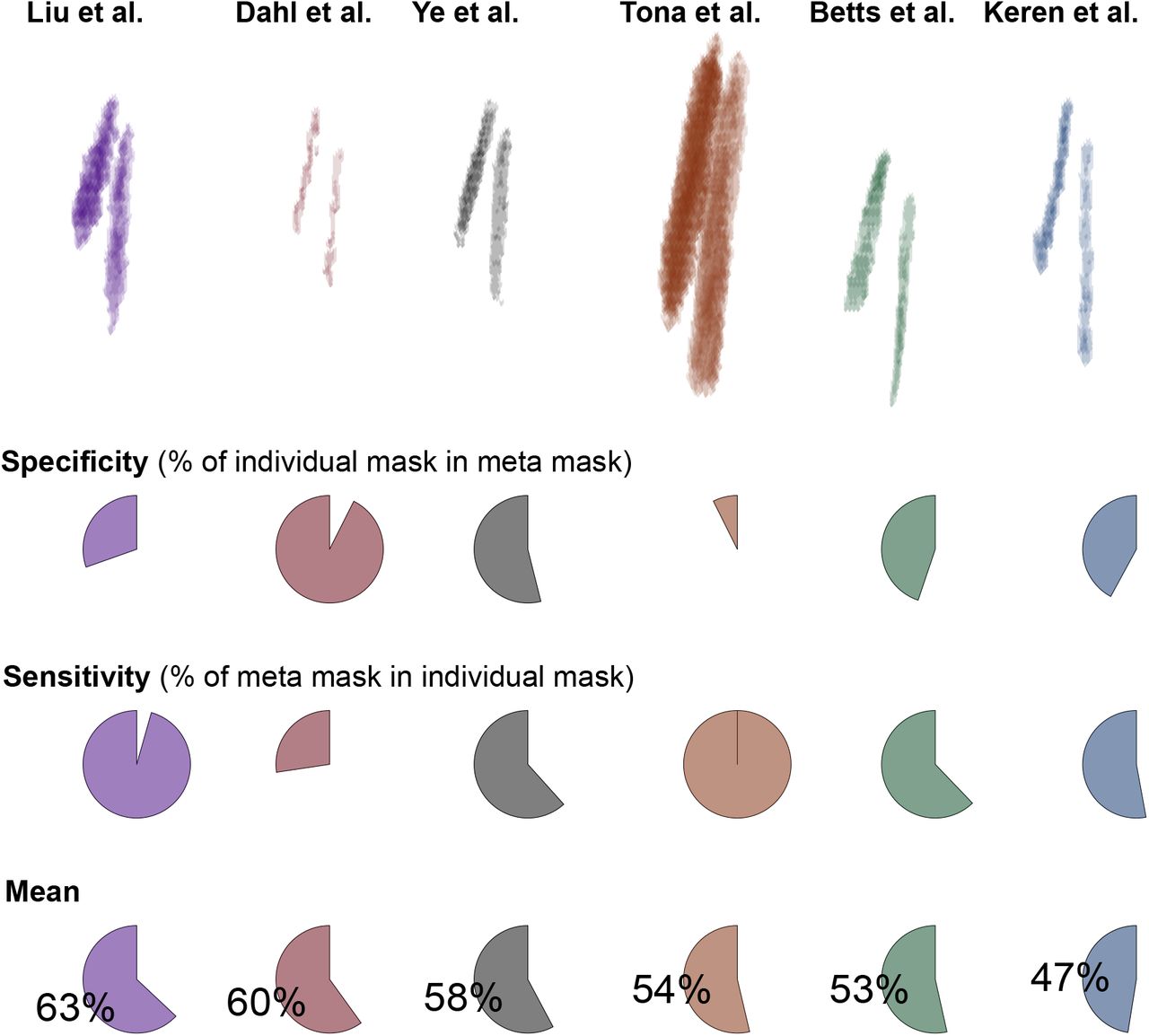
Accuracy of previously published locus coeruleus (LC) masks. Binarized masks in standard space (MNI 152, lin; top row) are ranked based on their accuracy (mean across specificity and sensitivity). Specificity expresses the percentage of a given mask that is included in the LCmetaMask whereas sensitivity denotes the percentage of the LCmetaMask that is part of each mask. For access to the individual masks, please refer to Table 1. Note that the relative position of the individual masks (top row) corresponds to their position in MNI 152 linear space; x/y/z axes are not displayed for clarity.
The masks that were computed based on the largest samples (cf. Table 1; Dahl et al., 2019; Liu et al., 2019) demonstrated the highest accuracy. Concerning specificity and sensitivity, the two masks appeared almost as mirror images. That is, the volume of interest published by Liu and colleagues evinced a high sensitivity at the cost of a relatively lower specificity (i.e., it included also non-LC voxels), while the situation was reversed for the mask by Dahl and colleagues (in line with it mapping peak LC coordinates; Dahl et al., 2019). Notably, the two masks themselves show a high agreement (94 %; Liu et al., 2019). Ye and colleagues tested a smaller sample, albeit with a higher field strength (7 T) to generate their volume of interest which appears to strike a balance between sensitivity and specificity. None of the tested masks, however, exceeded an accuracy rating of  , indicating that, by aggregating across publications, the LCmetaMask forms a volume of interest that conveys valuable information (i.e., is not redundant with previous masks).
, indicating that, by aggregating across publications, the LCmetaMask forms a volume of interest that conveys valuable information (i.e., is not redundant with previous masks).
Locus coeruleus meta mask captures high intensity voxels in independent clinical sample
We aligned and pooled across brainstem scans of participants with or known to be at-risk for mutations in genes associated with ADAD (cf. Dahl et al., 2019). On the group level, we observed a cluster of hyperintense voxels bordering the lateral floor of the fourth ventricle (Betts, Kirilina, et al., 2019). This LC-related hyperintensity was accurately captured by the LCmetaMask while excluding more medial, non-LC related high intensity voxels (see Figure 3). Taken together, this indicates that the LCmetaMask can be applied to independent datasets to reliably extract MR-indexed integrity across the rostrocaudal axis.
Lower MR-indexed locus coeruleus integrity in autosomal-dominant Alzheimer’s disease
Comparing LC intensity ratios—an in-vivo proxy for the integrity for the structure (Keren et al., 2015)—across cognitively normal and symptomatic participants, we observed reliably lower intensity in the patient group (Wilcoxon rank sum test, Z = –2.177; p = 0.03; see Figure 4). This difference was most pronounced in middle–rostral segments of the nucleus that project to the mediotemporal lobe (Wilcoxon rank sum test of group differences in rostral vs. caudal segment; Z = –2.816; p = 0.005; see Figure 4). Among carriers of ADAD-causing mutations, closer proximity to the mutation-specific median age of dementia diagnosis— termed adjusted age—was associated with lower LC ratios (mean correlation coefficient across 1,000,000 bootstraps: rho = –0.726; p = 0.047; see Figure 4). Taken together, corroborating earlier post-mortem work (in LOAD; Lyness et al., 2003), we observed lower MR-indexed LC integrity in middle–rostral segments of the nucleus, potentially indicating noradrenergic neurodegeneration.

Lower LC intensity ratios in autosomal-dominant Alzheimer’s disease (ADAD). a. Symptomatic participants show lower overall LC intensity ratios relative to cognitively normal controls (Z = –2.177; p = 0.03). b. Group differences are most pronounced in middle– rostral segments of the LC (plotted on the y-axis; Z = –2.816; p = 0.005; shaded areas indicate ± 1 standard error of the mean [SEM]). c. Closer proximity to the mutation-specific median age of dementia diagnosis (adjusted age) is associated with lower overall LC ratios (mean correlation coefficient across 1,000,000 bootstraps: rho = –0.726; p = 0.047). LC, locus coeruleus; Cog. normal, cognitively unimpaired participants.
MR-indexed locus coeruleus integrity is associated with cortical tau burden
Previous animal research suggests that noradrenergic neurodegeneration may exacerbate neural decline and contribute to Alzheimer’s pathogenesis (Chalermpalanupap et al., 2018; Rorabaugh et al., 2017). Thus, we next tested whether LC intensity would be associated with cortical tau burden, a hallmark of AD.
Across cortical regions (Desikan et al., 2006), symptomatic participants demonstrated higher flortaucipir SUVR (see Figure 5). Importantly, leveraging a multivariate statistical approach (partial least squares correlation [PLSC]; Krishnan et al., 2011), we revealed a topographical pattern of LC-related tau pathology (p = 0.037; see Figure 5). That is, we extracted a latent variable (latent PLS score) that optimally captures the multivariate association between participants’ LC intensity and regional tau burden (r = 0.54; lower LC intensity was associated with higher flortaucipir SUVR). Especially tau pathology in occipito-temporo-parietal regions contributed to this latent variable, as indicated by reliable bootstrap ratios (BSR; < –3; see Figure 5; BSR can be interpreted akin to Z-values; please note that we opted for a conservative threshold [–3] due to the large number of cortical ROI). In sum, in line with research in genetically modified animals (Chalermpalanupap et al., 2018; Rorabaugh et al., 2017), we observed a prominent association between in-vivo proxies of LC integrity and tau pathology.

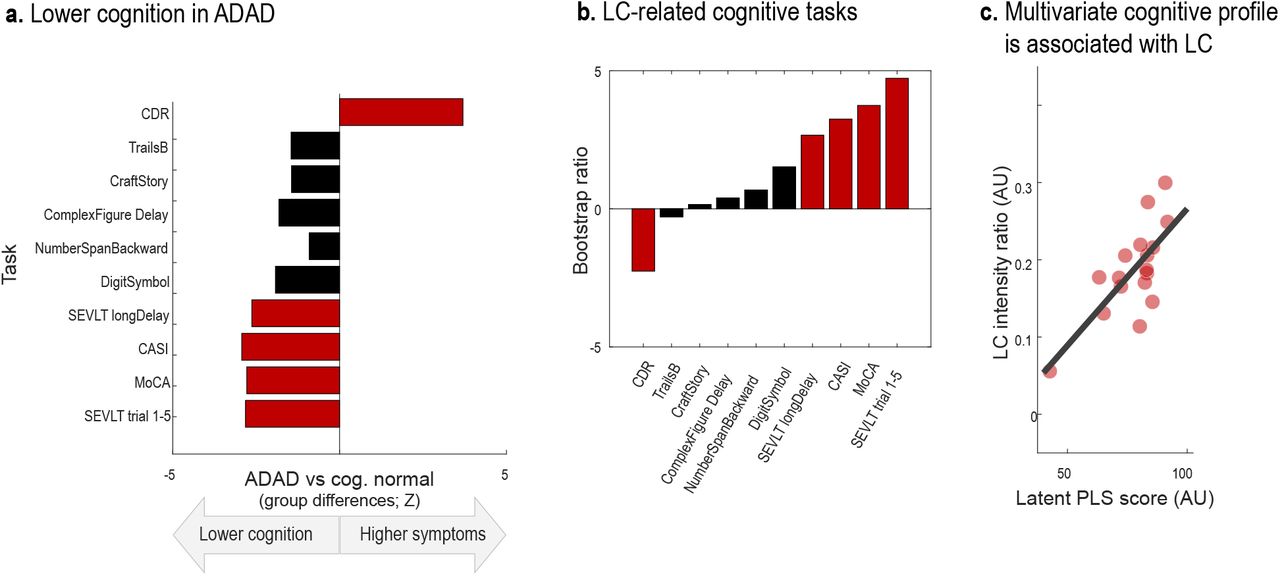
Lower LC intensity is associated with tau burden in posterior brain regions. a. Symptomatic participants show higher flortaucipir standardized uptake value ratios (SUVR) across most cortical regions relative to cognitively normal controls (missing PET data for two participants [dark blue bars]). b. Contribution of individual cortical regions of interest to a partial least squares (PLS) latent variable indexing LC-related tau pathology (Bootstrap ratios < –3 are considered reliable). c. Scatter plot depicting the relation between latent PLS scores and LC intensity (p = 0.037; r = 0.54). LC, locus coeruleus; ADAD, autosomal-dominant Alzheimer’s disease.
MR-indexed locus coeruleus integrity is associated with cognitive deficits
Finally, we set out to test the behavioral relevance of our in-vivo proxy of LC integrity. Norepinephrine release from the LC is strongly implicated in the modulation of attentional and mnemonic processing (Berridge & Waterhouse, 2003; Dahl, Mather, Sander, & Werkle-Bergner, 2020; Lee et al., 2018; Sara, 2009). Accordingly, recent imaging studies reported positive associations between LC intensity and cognition in healthy aging (Dahl et al., 2019; Hämmerer et al., 2018; Liu et al., 2020). However, whether this relation extends to ADAD of young onset is currently unknown.
Across a range of cognitive tasks, we detected worse cognitive abilities and higher dementia symptoms in the ADAD group relative to controls (see Figure 6). Reliable group differences (Wilcoxon rank sum test; Z < –1.96 | Z > 1.96) were observed for screening instruments for mild cognitive impairment and dementia (the Montreal Cognitive Assessment [MoCA, Nasreddine et al., 2005]; the Cognitive Abilities Screening Instrument [CASI; Teng et al., 1994], and the Washington University Clinical Dementia Rating Scale [CDR; measure: sum of boxes; cf. O’Bryant et al., 2008]). In addition, symptomatic participants performed significantly worse on the Spanish English Verbal Learning Test (SEVLT; measures: average performance over learning trials and delayed recall; González, Mungas, & Haan, 2002), in line with reports of verbal learning tests to convey information about participants’ current and future cognitive status (Albert, Moss, Tanzi, & Jones, 2001; Belleville, Fouquet, Hudon, Zomahoun, & Croteau, 2017; Moradi, Hallikainen, Hänninen, & Tohka, 2017; Schoenberg et al., 2006).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lower LC intensity is associated with cognitive deficits. a. Symptomatic participants show lower cognitive performance as indicated from screening instruments for mild cognitive impairment and dementia (Clinical Dementia Rating Scale [CDR]; Cognitive Abilities Screening Instrument [CASI]; Montreal Cognitive Assessment [MoCA]) as well as the Spanish English Verbal learning task (SEVLT). b. Contribution of individual neuropsychological tests to a partial least squares (PLS) latent variable indexing LC-related cognitive deficits (Bootstrap ratios < –1.96 and > 1.96 are considered reliable). c. Scatter plot depicting the relation between latent PLS scores and LC intensity (p = 0.016; r = 0.728). LC, locus coeruleus; ADAD, autosomal-dominant Alzheimer’s disease. For references to the cognitive tasks, please refer to the main text.
We applied a partial least squares correlation (PLSC) to isolate the pattern of cognitive impairment reliably linked to MR-indexed LC integrity. Our analyses isolated a single latent variable (p = 0.016) that optimally expresses the multivariate association between participants’ LC intensity and cognitive performance (r = 0.728). All cognitive tasks that were sensitive to distinguish symptomatic from cognitively normal participants contributed reliably to this latent variable (bootstrap ratios [BSR]< –1.96 | BSR > 1.96; see Figure 6). To conclude, across a range of neuropsychological tests, higher MR-indexed LC integrity was observed in participants with unimpaired cognitive performance.
Discussion
Animal and post-mortem research indicates that the brain’s noradrenergic system plays a central role in the pathogenesis of Alzheimer’s disease (Braak et al., 2011; Weinshenker, 2018). In vivo investigations, however, have long been hindered by challenges in reliable non-invasive LC assessments (Astafiev et al., 2010; Keren et al., 2009). While initial intriguing in vivo studies in late-onset Alzheimer’s are underway (LOAD; e.g., Betts, Cardenas-Blanco, et al., 2019; Jessen et al., 2018), unequivocally distinguishing age-from disease-related LC alterations is difficult on this basis (Dahl et al., 2019; Liu et al., 2019). Focusing instead on types of dementia developing earlier in life may provide a unique window into the mechanisms driving Alzheimer’s development (ADAD; Bateman et al., 2012; Jacobs, Becker, et al., 2019; Ringman, 2005).
Leveraging a meta-analytical approach, we first synthesized LC localizations and dimensions across previously published studies to improve the reliability and validity of MR-based LC detection. In a second step, we applied this newly generated volume of interest to determine whether MR-indexed LC integrity can serve as marker for noradrenergic degeneration in ADAD.
Our analyses isolated a cluster of high-confidence voxels that (1) is consistently identified as LC across published studies and (2) corresponds well to post-mortem reports (Fernandes et al., 2012). Next, exploiting this refined spatial characterization we semi-automatically extracted intensity data in an independent sample of participants with or known to be at-risk for mutations in genes associated with ADAD. We revealed lower MR-indexed LC integrity in symptomatic mutation carriers. Group differences were most pronounced in middle to rostral segments of the LC (Ehrenberg et al., 2017; Lyness et al., 2003) and scaled with proximity to the mutation-specific median age of dementia diagnosis (Ryman et al., 2014). Beyond that, lower overall LC intensity was linked to higher tau burden in posterior brain regions (Chalermpalanupap et al., 2018) and worse cognitive performance across several neuropsychological tests (Dahl et al., 2019; Liu et al., 2020). Taken together, our finding of diminished LC integrity in ADAD suggests a prominent role of the noradrenergic system in this neurodegenerative disease.
Aggregating across published locus coeruleus maps yields high confidence meta mask
Imaging of small brainstem structures that are not visible using conventional MR sequences is notoriously challenging (for discussions, see Astafiev et al., 2010; Keren et al., 2009) and warrants a close alignment of individual scans (for recommendations, see Betts, Kirilina, et al., 2019; Liu et al., 2017). Here we used Advanced Normalization Tools (ANTs; Avants et al., 2011, 2009) for brainstem normalization. ANTs is becoming increasingly recognized as a powerful tool for accurate coregistrations – it has won several internationally recognized medical image processing challenges (e.g., Klein et al., 2009; for a full list see github.com/ANTsX/ANTs) and was used in all of the currently best ranked LC mapping studies (3/3, [relative to 1/3 of the remaining studies]; Dahl et al., 2019; Liu et al., 2019; Ye et al., 2020).
Besides normalization, LC mapping studies employing larger sample sizes and a higher MR-field strength evinced a higher accuracy, as indicated by spatial congruence with the meta mask (Dahl et al., 2019; Liu et al., 2019; Ye et al., 2020). We hope that by sharing an unbiased, biologically-plausible LC volume of interest that is based on more than 1,000 participants and all commonly used sequence types (FSE, MT, FLASH; see Table 1) we assist future functional and structural imaging studies in classifying brainstem effects (this LC meta mask is available for download via osf.io/sf2ky/).
Lower MR-indexed locus coeruleus integrity in autosomal-dominant Alzheimer’s disease
Applying the newly generated LC meta mask to an independent clinical sample, we demonstrate its utility for accurately extracting intensity information across the rostrocaudal extent of the nucleus. We observed lower middle–rostral LC intensity in symptomatic carriers of ADAD-causing mutations. This finding is consistent with post-mortem reports of substantial noradrenergic neurodegeneration in LOAD (Lyness et al., 2003). Some previous post-mortem studies in ADAD also noted disproportionate depigmentation and neuronal loss in the LC (Janssen et al., 2000; Snider et al., 2005). In vivo imaging studies are in general agreement with the histological findings and indicate lower LC contrast in LOAD patients (Betts, Cardenas-Blanco, et al., 2019; Dordevic et al., 2017; Takahashi et al., 2015). To date there is only a single imaging study focusing on early-onset Alzheimer’s (ADAD; Jacobs, Becker, et al., 2019), albeit in non-symptomatic mutation carriers (i.e., at a preclinical stage). Our observation that LC intensity scaled with proximity of dementia onset (adjusted age) across non-symptomatic and symptomatic mutation carriers matches a negative age association in mutation carriers reported by Jacobs and colleagues (2019) and might indicate a progressive deterioration. Based on post-mortem validations of LC MRI (Keren et al., 2015; Cassidy et al., 2019) and decreased cell counts in Alzheimer’s (Lyness et al., 2003), we interpret our observations as indicative of noradrenergic neurodegeneration in ADAD.
MR-indexed locus coeruleus integrity is associated with cortical tau burden
Leveraging a multivariate statistical approach, we further revealed a pattern of LC-related tau pathology that was most pronounced in posterior brain regions (cf. Jacobs, Becker, et al., 2019). This observation supports the notion that loss of noradrenergic neurons may exacerbate the severity of other Alzheimer’s hallmarks, like tau pathology (Chalermpalanupap et al., 2018). The LC is one of the first brain regions in which aberrant tau can be detected already at relatively early ages (i.e., the first decades of life; Braak et al., 2011). The accumulation of abnormal tau has been hypothesized to shift noradrenergic cells to a mode of hyperactivity which in turn promotes tau release and spread along LC’ widespread axonal pathways (Chalermpalanupap et al., 2017; Weinshenker, 2018). While tau gradually propagates through cortical regions (categorized as Braak stages), noradrenergic neurons first shrink in size and then degenerate (Ehrenberg et al., 2017; Kelly et al., 2017; Theofilas et al., 2017). The frank decline of noradrenergic cells is preceded by a period of dysfunctional neurotransmission in LC’s terminal regions like the mediotemporal lobe (Weinshenker, 2018). Thus, the negative association between in vivo proxies for LC integrity and tau burden may signify a more advanced Alzheimer’s disease stage including noradrenergic neurodegeneration and wide-spread tau pathology.
MR-indexed locus coeruleus integrity is associated with cognitive deficits
Finally, we found evidence for an association between MR-indexed LC integrity and cognitive performance across several neuropsychological tests. Noradrenergic neuromodulation has been implicated in a range of cognitive functions, prominently including attention and memory (Berridge & Waterhouse, 2003; Bouret & Sara, 2005; Corbetta, Patel, & Shulman, 2008; Mather, Clewett, Sakaki, & Harley, 2016; Sara, 2009). In particular, mediated via β-adrenoceptors, norepinephrine release promotes long-term-potentiation in the hippocampus—a key determinant of synaptic plasticity and memory (O’Dell, Connor, Guglietta, & Nguyen, 2015). Recent optogenetic research moreover indicates a causal role of LC activity in memory acquisition and consolidation, potentially supported by co-release of dopamine (Duszkiewicz, McNamara, Takeuchi, & Genzel, 2019; Takeuchi et al., 2016; Uematsu et al., 2017; Wagatsuma et al., 2018). Consistent with these observations in animals, recent in vivo human research demonstrated an association between MR-indexed LC integrity and memory performance in healthy aging (Dahl et al., 2019; Hämmerer et al., 2018; Liu et al., 2020). Extending evidence from healthy populations, we here confirm the behavioral relevance of MR-indexed LC integrity in tracking cognitive decline in a clinical sample. Neuropsychological tests that proved sensitive to distinguish patients from controls were reliably linked to LC integrity (González et al., 2002; Nasreddine et al., 2005; O’Bryant et al., 2008; Teng et al., 1994). In line with reports indicating verbal learning tests as effective early markers of Alzheimer’s pathology (Albert et al., 2001; Belleville et al., 2017; Moradi et al., 2017; Schoenberg et al., 2006), verbal learning and memory showed the closest link to LC integrity (cf. Dahl et al., 2019, for analogous results in later life). Taken together, our findings suggest that noradrenergic neurotransmission supports memory performance whereas dysfunctions therein are associated with Alzheimer’s related cognitive decline.
Limitations and conclusions
Some limitations should be noted. First, the contrast mechanisms underlying LC-MRI constitute an active area of research (for a discussion, see Betts, Kirilina, et al., 2019) and future studies may help determine what precise physiological processes are reflected in MR-contrast differences. Second, as a cross-sectional observational study, it is not possible to conclude a causative relationship between loss of LC integrity and cognitive symptoms and deposition of abnormal tau in persons with ADAD. Finally, with a prevalence of about 5 cases per 100,000 persons at risk, ADAD is a rare disease (Campion et al., 1999) accounting for less than 1 % of all Alzheimer’s cases (Bateman et al., 2011). All but one ADAD mutation carriers in the current study had the same mutation in PSEN1 (A431E) which has specific features (e.g. co-occurring spastic paraparesis and possibly atypical posterior-predominant tau deposition) that may limit generalizability of the current findings. While providing insights into the pathogenesis of Alzheimer’s largely disentangled from factors associated with aging, the presented findings need to be corroborated by longitudinal evidence in larger samples (Lindenberger et al., 2011).
In conclusion, we applied a meta-analytical approach to advance the reliability and validity of MR-based LC detection. Using non-invasive in vivo proxies, we revealed lower LC integrity in symptomatic carriers of ADAD-causing mutations. Moreover, LC integrity was strongly associated with cortical tau pathology and memory decline. In summary, this suggests a prominent role of the noradrenergic system in Alzheimer’s disease (Mather & Harley, 2016; Weinshenker, 2018).
Data Availability
The here described LC meta mask as well as pontine reference mask is available for download on an Open Science Framework repository (osf.io/sf2ky/). All sources for previously published masks are listed in Table 1. For access to raw imaging and clinical data, please refer to the HCP (https://nda.nih.gov/ccf).
Footnotes
Conflict of interest statement: The authors declare no competing financial interests.
Authors note: MJD is recipient of a stipend from the GA. Lienert-Foundation and was supported by a stipend from the Davis School of Gerontology, University of Southern California. MM’s work was supported by an Alexander von Humboldt fellowship, a Max Planck Sabbatical Award, and by National Institutes of Health (NIH) grant R01AG025340. MW-B received support from the German Research Foundation (DFG, WE 4269/5-1) and the Jacobs Foundation (Early Career Research Fellowship 2017–2019). BLK was supported by a NIH grant F32AG057162. YS was supported by NIH grants RF1AG064584 and RF1AG056573. JMR was supported by NIH grants U01AG051218, R01AG062007, and P30AG066530
References



