
Abstract
Importance Knowing the transmissibility of asymptomatic infections and risk of infection from household and community exposures is critical to SARS-CoV-2 control. Limited previous evidence is based primarily on virologic testing, which disproportionately misses mild and asymptomatic infections. Serologic measures are more likely to capture all previously infected individuals.
Objective Estimate the risk of SARS-CoV-2 infection from household and community exposures, and identify key risk factors for transmission and infection.
Design Household serosurvey and transmission model.
Setting Population-based serosurvey in Geneva, Switzerland
Participants 4,524 household members five years and older from 2,267 households enrolled April-June 2020.
Exposures SARS-CoV-2 infected (seropositive) household members and background risk of community transmission.
Main outcomes and measures Past SARS-CoV-2 infection confirmed through anti-SARS-CoV-2 IgG antibodies by ELISA. Chain-binomial models based on the number of infections within households were used to estimate extra-household infection risk by demographics and reported extra-household contacts, and infection risk from exposure to an infected household member by demographics and infector’s symptoms. Infections attributable to exposure to different types of infectious individuals were estimated.
Results The chance of being infected by a single SARS-CoV-2 infected household member was 17.2% (95%CrI 13.6-21.5%) compared to a cumulative extra-household infection risk of 5.1% (95%CrI 4.5-5.8%). Infection risk from an infected household member increased with age, from 7.5% (95%CrI 1.3-20.3%) among 5-9 years to 30.2% (95%CrI 14.3-48.2%) among those ≥65 years. Working-age adults (20-49 years) had the highest extra-household infection risk. Seropositive household members not reporting symptoms had 74.8% lower odds (95%CrI 43.8-90.3%) of infecting another household member compared to those reporting symptoms, accounting for 19.6% (95%CrI 12.9-24.5%) of all household infections.
Conclusions and Relevance The risk of infection from exposure to a single infected household member was four-times that of extra-household exposures over the first wave of the pandemic. Young children had a lower risk from infection from household members. Asymptomatic infections are far less likely to transmit than symptomatic ones but do cause infections. While the small households in Geneva limit the contribution of household spread, household transmission likely plays a greater role in other settings.
Background
Household-centered studies provide an enumerable set of individuals known to be exposed to an infectious person, hence, they have played an important role for estimating key transmission properties of SARS-CoV-2. However, most published studies of SARS-CoV-2 household transmission rely on clinical disease (COVID-19), and/or PCR-based viral detection to identify infected individuals.1 Due to the narrow time window after exposure in which RT-PCR can be highly sensitive,2 case ascertainment based on virologic testing may miss infections, especially those that are mild or asymptomatic.3 This can lead to important biases and limit what can be studied, including underestimates of the importance of sub-clinical infections and household secondary attack rates.3
Serologic studies provide an alternative tool for understanding SARS-CoV-2 transmission. Serological tests remain sensitive to detecting past infections well beyond the period when the virus is detectable 4, thereby providing a way to measure whether individuals have ever been infected.
Virologic and serologic studies have provided important insights into SARS-CoV-2 transmission. These include estimates of the household secondary attack rate (e.g., 17% in a recent meta-analysis1) and evidence of reduced infection rates among young children.1,5,6 However a number of critical gaps in the evidence remain, including the relative role of transmission between household members compared to transmission in the community, the infectiousness of asymptomatic individuals and the effect of age on susceptibility to infection and infectiousness.
To help fill these gaps, we apply household transmission models to data from a household-based population serosurvey of 4,534 people from 2,267 households in Geneva, Switzerland. We provide a serology-based assessment of transmission between intra- and extra-household contacts, illuminate risk factors for infection and transmission and measure the importance of asymptomatic transmission. By doing so, we provide important evidence for guiding the COVID-19 pandemic response.
Methods
Study design, participants, and procedures
The SEROCoV-POP study is a population-based survey of former participants of an annual survey of individuals 20-74 years old representative of the population of Geneva (Canton), Switzerland. The full survey protocol is available online and a detailed description of the design and initial seroprevalence results were previously published.7
The SEROCoV-POP study invited all 10,587 participants of the previous annual surveys with a valid email address to participate in the study through email. Participants were invited to bring all members of their household aged 5 years and older to join the study. After providing informed written consent, participants either filled out a questionnaire online, in the days before their visit, or on site at the time of their visit. The questionnaire included questions about participants’ demographics, household composition, symptoms since January 2020, details on the frequency of extra-household contacts and reduction in social interaction since the start of pandemic. Only participants 14 years and older were asked about their frequency of extra-household contacts and change in behavior pre- and post-pandemic. We defined symptom presentation a priori as having reported any of: cough, fever, shortness of breath, or loss of smell or taste between January 2020 and 2 weeks before blood draw, with the upper limit imposed due to the low sensitivity of antibody tests during this time window. We collected peripheral venous blood from each consenting participant. The study was approved by the Cantonal Research Ethics Commission of Geneva, Switzerland (CER16-363).
Laboratory analysis
We assessed anti-SARS-CoV-2 IgG antibodies in each participant using an ELISA (Euroimmun; Lübeck, Germany #EI 2606-9601 G) targeting the S1 domain of the spike protein of SARS-CoV-2; sera diluted 1:101 were processed on a EuroLabWorkstation ELISA (Euroimmun). An in-house validation study found that the manufacturer’s recommended cutoff for positivity (1.1) had a sensitivity of 93% and a specificity of 99%.8 In our primary analyses we defined seropositivity based on the cutoff recommended by the manufacturer and explored a higher cut-off of 1.5 (>1.5) in sensitivity analyses to increase specificity.8 As the presence of antibodies has been shown to be a reliable marker of recent infection, we use the term ‘infected’ to refer to a seropositive individual.
Statistical analyses
We fit chain binomial transmission models to estimate two primary quantities; the probability of extra-household infection over the course of the first epidemic wave (referred to also as ‘community infections’) and the probability of being infected from a single infected household member over the course of his/her infectious period (referred to as ‘household exposures’).9 When fitting these models we consider all possible sequences of viral introductions to each household and subsequent transmission events within the household. For example, in a household with 2 seropositive individuals, both could have been infected outside of the household, or one could have been infected outside and then infected one other person within the household. We adapted models to estimate the within household and extra-household transmission risk according to the characteristics of potential infectees (i.e., age and sex) and, for within-household risk, those of the potential infectors (i.e, symptoms and/or age). We simulate the proportion of infections attributable to extra-household and within household exposures.
We built a series of 9 models including different combinations of individual-level characteristics (e.g., age, sex, self-reported contacts, symptoms) and compared their fit using the widely applicable information criterion (WAIC).10 We implemented the models in the Stan probabilistic programming language and used the rstan package (version 2.21.0) to sample from the posterior distribution and analyse outputs.11 We used weakly informative priors on all parameters to be normally distributed on the logit scale with mean of 0 and standard error of 1.5. We ran four chains of 1,000 iterations each with 250 warm-up iterations and assessed convergence visually and using the Gelman-Rubin Convergence Statistic (R-hat).12 All estimates are means of the posterior samples with the 2.5th and 97.5th percentiles of this distribution reported as the 95% credible interval. Full model and inference details are provided in the supplement and code needed to reproduce analyses are available at https://github.com/HopkinsIDD/serocovpop-households.
Results
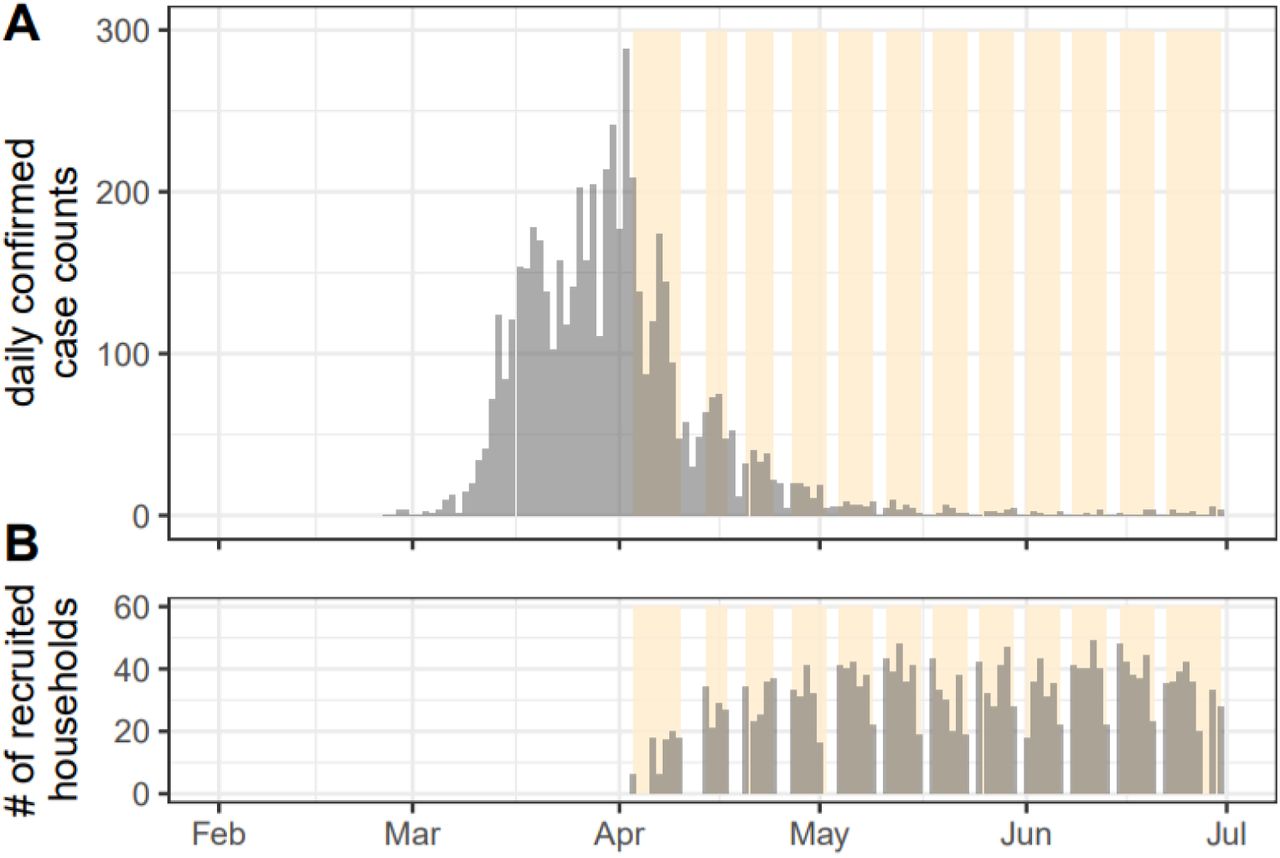
Between April 3th and June 30th, 8,344 individuals coming from 4,393 households were successfully enrolled in the SEROCoV-POP study (Figure 1).7 In 2,627 of these households, all members of the household were eligible, available, and provided a blood sample. The majority of these households were either one (37.9%, n=860) or two (39.2%, n=889) person households (Figure S1). The median household size in our study (2.0, interquartile range [IQR]=1,2) was similar to the general population in Geneva canton (median=2.0, IQR=1,3).13

Epidemic curve and recruitment period of household serosurvey. (A) daily confirmed COVID-19 cases reported in Geneva up to July 1st, 2020. (B) Daily number of recruited households over the 12-week study period. First detected case in Geneva canton was reported on February 26th and the epidemic lasted about two months. Yellow bands indicate time periods of enrollment for each week. This includes all 4,438 households enrolled in the SEROCoV-POP study, not restricted to the complete households used in these analyses for which serostatus of all household members were available
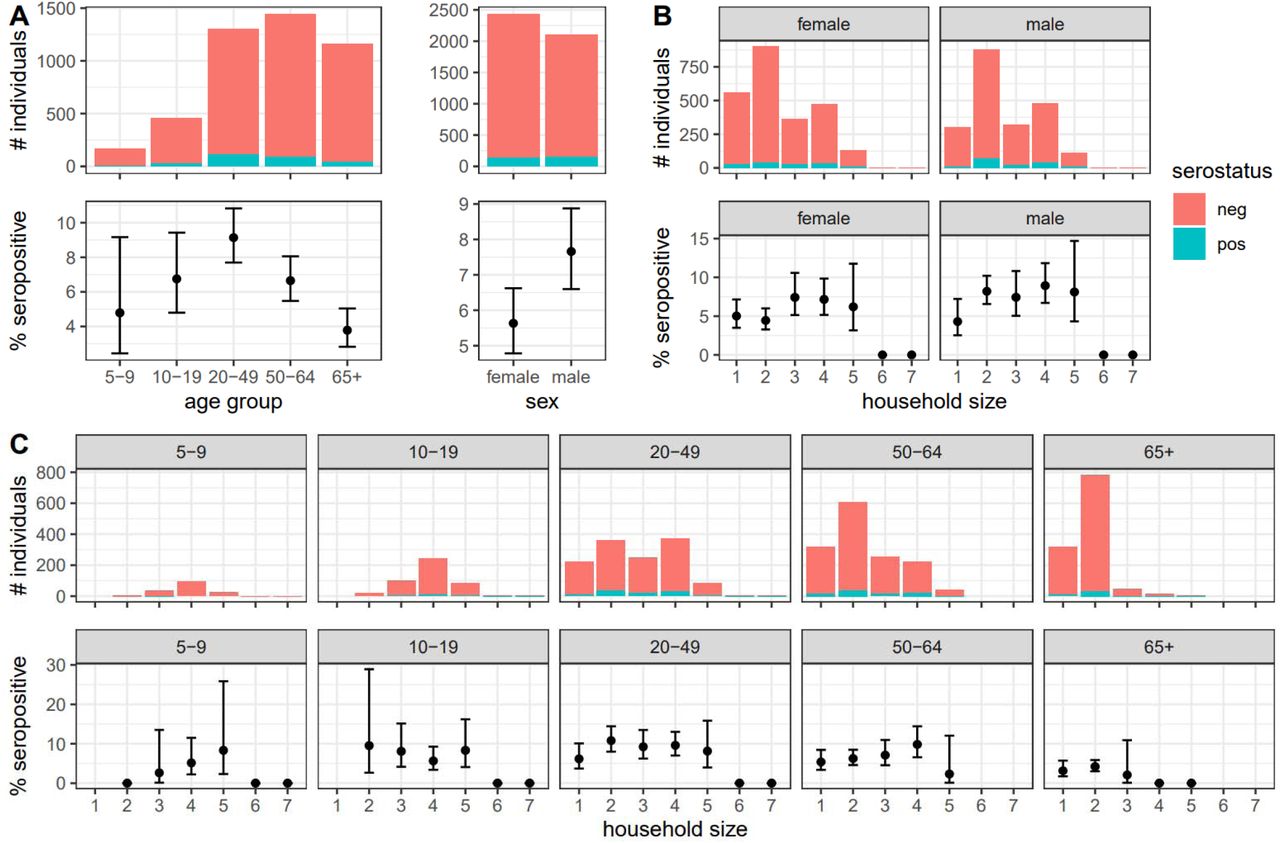
The median age of the 4,534 household members in our study was 53 years (IQR=34,65), and 53.6% were female. Compared with the general canton population, our study sample included more individuals 50 years and older and fewer 20-49 year olds. Individuals in older age groups were more likely to live in smaller households: 94.6% (1,100/1,163) of people who were 65 years and older lived alone or in two-person households versus 44.5% (588/1,302) of those 20-49 years old (Table 1).
Number of recruited and seropositive individuals by age-group, sex and household size of the households they reside in.
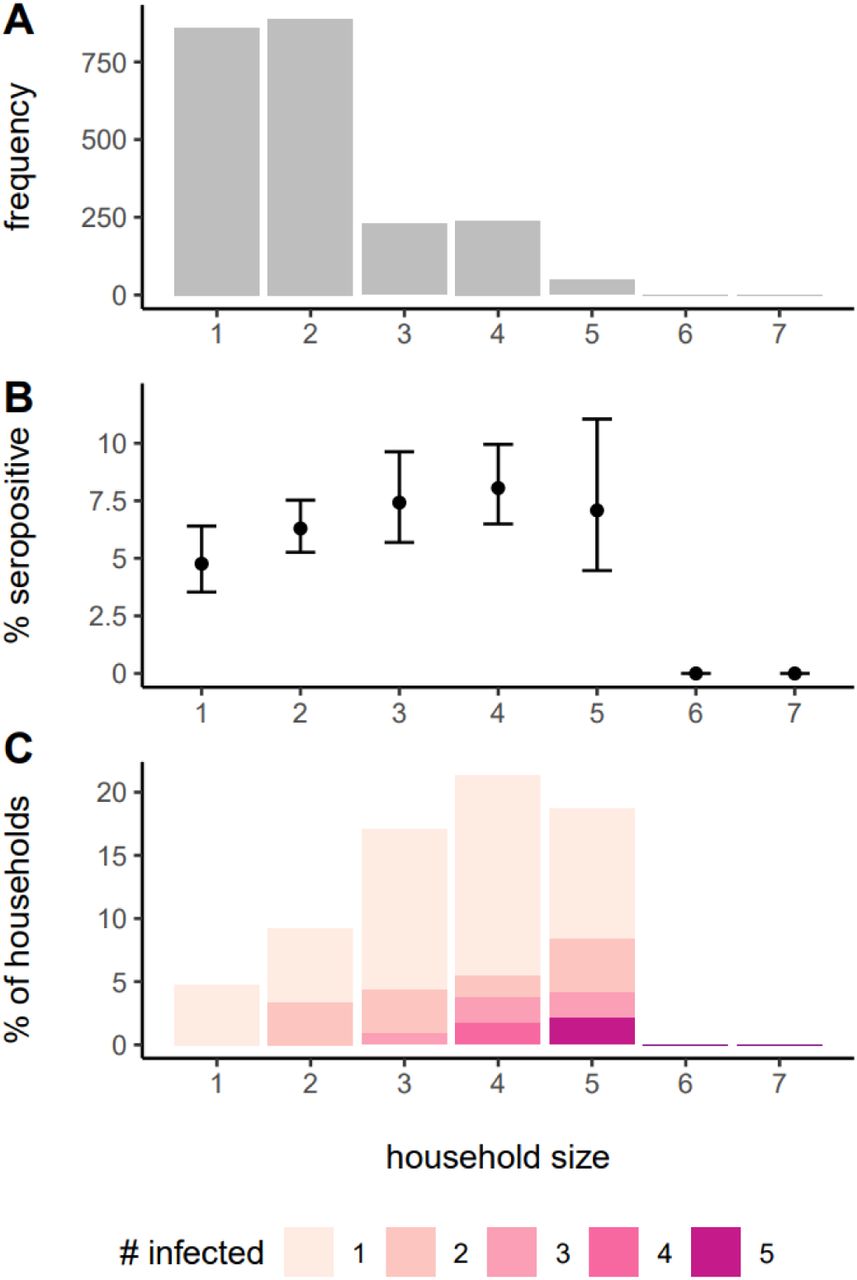
Overall, 6.6% (298/4,534) of individuals tested positive for SARS-CoV-2 anti-S1 IgG antibodies by ELISA. Of the 2,267 households included in the analyses, 222 (9.8%) had at least one seropositive household member. The proportion of households with seropositive members increased from 4.8% (41/860) in households of size one, to 17.0%(39/229) in households of size three, and was relatively constant in larger households (Figure S1, Table 1, Figure S2). Symptoms consistent with COVID-19 were reported by 70.6% (209/298) of seropositive individuals although this was significantly lower in young children (37.5%, 3/8).
From the start of the epidemic in Geneva (first case reported on February 26, 2020) through the time of the serosurvey, the cumulative risk of infection from extra-household exposures was 5.1% (95% Credible Interval [CrI] 4.5-5.8%). The probability of being infected from a single infected household member was 17.2% (95% CrI 13.6-21.5%, Figure 2). For transmission between household members, the risk being infected increased with age, from 7.5% (95%CrI 1.3-20.3%) among 5-9 year olds to 30.2% (95%CrI 14.3-48.2%) among those 65 and older, with little difference among those 10-64 years olds (Figure 2). In contrast, the extra-household infection risk was the highest among working age adults, particularly 20-49 years olds (7.4%, 95%CrI 5.9-9.0%, Figure 2, Table S4). Models allowing for differential risk of transmission by the age of the infector were not well supported by the data and included no significant differences between ages (Table S2).

Median probability of (A) extra-housheold infection over the duration of the outbreak and (B) infection from a single infected household member by age group and sex of the susceptibles. Bars represent 95% credible intervals. Probabilities of being infected by sex and age group of the exposed individuals are estimated by a model only including age and sex of the exposed individuals (model 2, orange/green bars; see Table S2). The probabilities of being infected by the age group of the exposed individuals combining males and females (left four grey bars on both panels) are estimated with an age-only model (model 1). The overall probabilities of being infected (rightmost grey bar on both panels) are estimated with the null model (model 0).
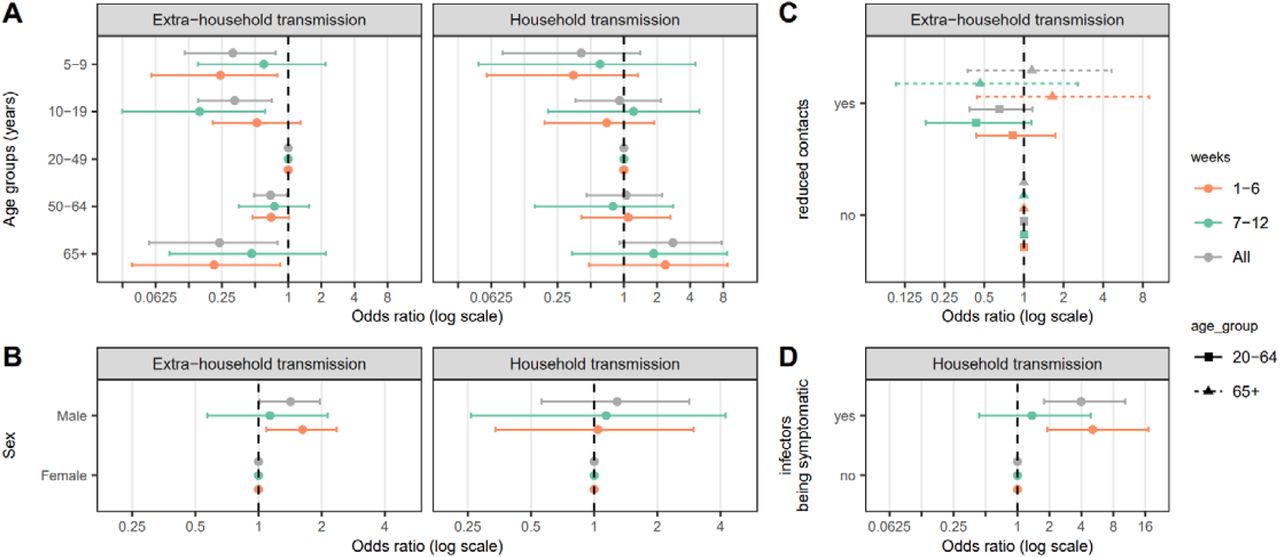
Across age-groups, males were more likely to be infected outside the household (OR=1.4, 95%CrI 1.0-2.0) and had a higher chance of being infected from a household exposure (OR=1.3, 95%CrI 0.56-2.8), though there is substantial uncertainty in the latter estimate (Figure 3 & Table S2).

Relative susceptibility to extra-household infection and infection from a single infected household member by individual characteristics of the exposed individuals, A) age group, B) sex, C) self-reported reduction in social interaction since the start of the pandemic and D) potential infectors’ symptom status. Odds ratios and confidence intervals, shown on the log-scale, are estimates from model 5 (See Table S2).
Seropositive household members not reporting symptoms had 0.25 times the odds (OR=0.25, 95%CrI: 0.10-0.56) of infecting another household member compared to those reporting symptoms consistent with COVID-19 (Figure 3).
We found some evidence that those aged 20-64 who reported reducing extra-household contacts during the pandemic had a reduced odds of extra-household infection (OR=0.66, 95%CrI 0.39-1.2). However, no similar reduction in the odds of infection was seen in those aged 65 or older and data were not available for younger individuals (Figure 3, Figure S4).
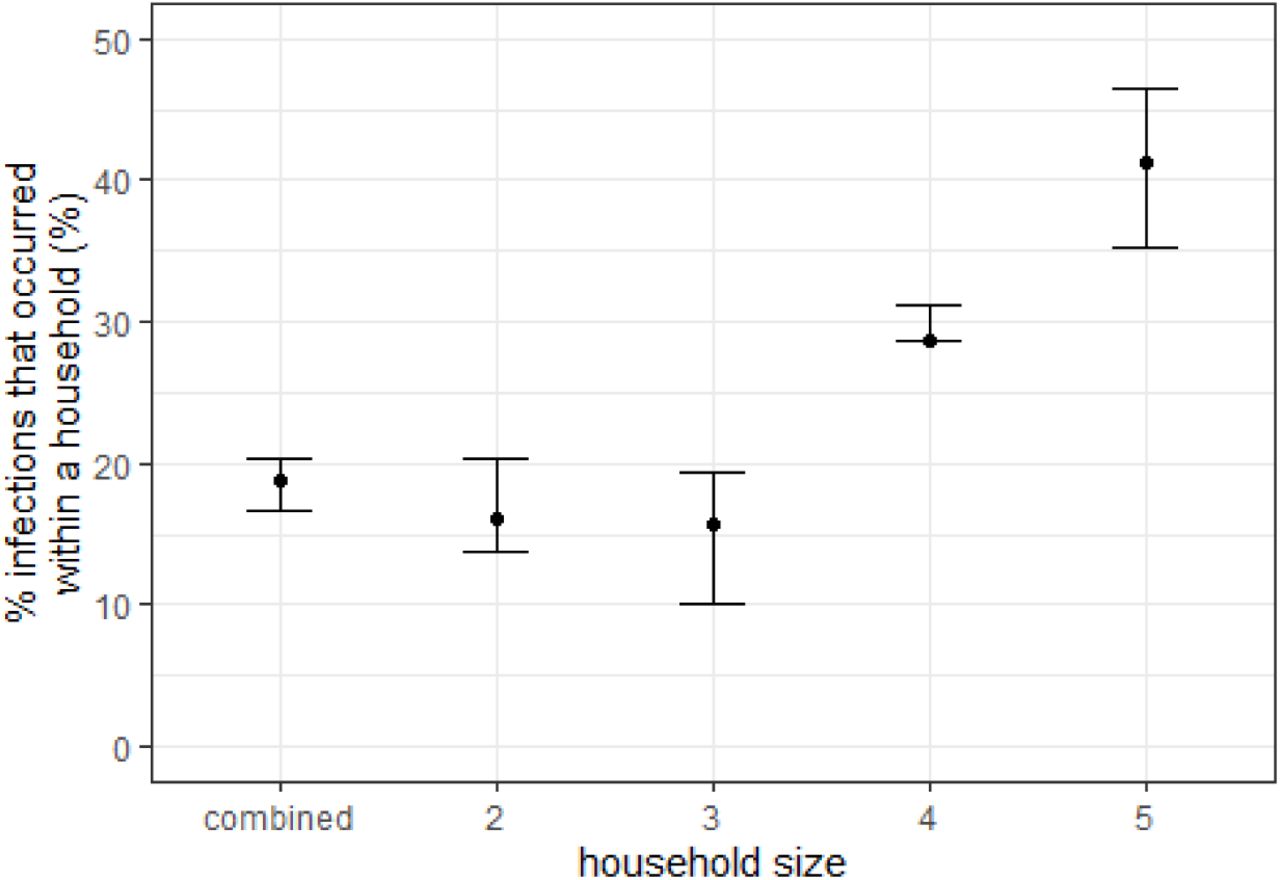
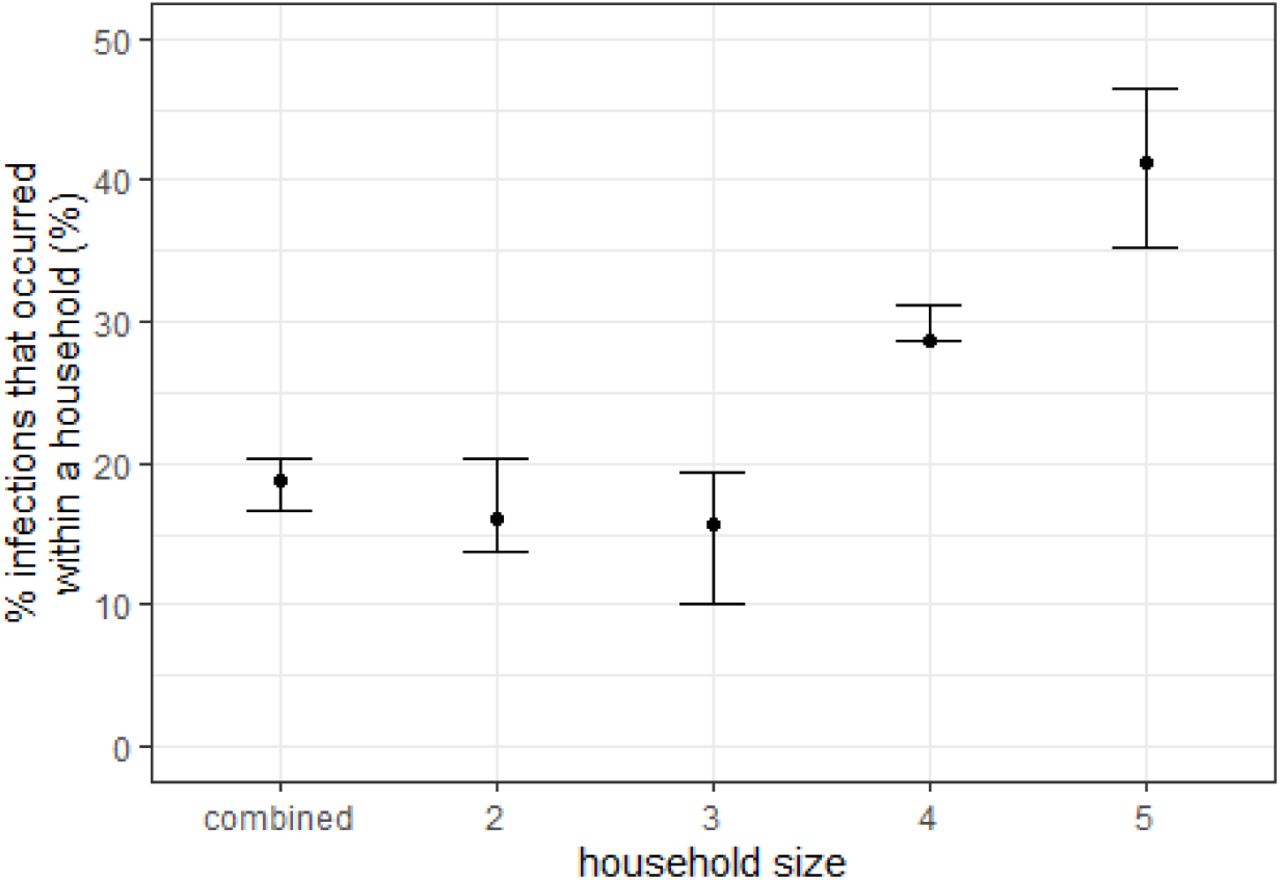
Using posterior distributions of parameters, we simulated the source of infection for all individuals in the study. We estimate that 18.8% (95%CrI 16.7-20.4) of all infections occurred in the household, with the proportion of infections attributable to household transmission increasing with household size (Figure S6). In households with two individuals, 16.1% (95%CrI 13.7-20.4) of infections were between household members, with this increasing to 41.2% (95%CrI 35.3-46.5) in households of five people (Table S3). Of within-household infections, we estimate 19.6% (95%CrI 12.9-24.5) were due to individuals not reporting symptoms consistent with COVID-19.
Here we focus on the results of the best fitting models, but across the nine candidate models considered (Table S2), infection risk estimates were qualitatively and quantitatively consistent with the primary findings. Similarly, we explored the sensitivity of our results to the ELISA seropositivity cutoff and found no qualitative differences in results (Figure S3).
Discussion
The results presented here appropriately place symptomatic household transmission of SARS-CoV-2 in the context of community risk and asymptomatic spread. We show an approximate 1 in 5 risk of being infected by a single SARS-CoV-2 infected household member. This contrasts with a 1 in 20 chance of being infected in the community over most of the first epidemic wave in Geneva, a period of roughly 2 months. However, despite the high risk of transmission from an infected household member, households are mostly small in this high-income urban setting, limiting opportunities for onward transmission. Thus, less than 20% of cases could be attributed to transmission between household members. While asymptomatic individuals appear to be significantly less infectious, they cannot be dismissed as inconsequential to disease spread, and are responsible for one-fifth of within-household transmission. Our results further illustrate the dual roles of biology and social behavior in shaping age-specific infection patterns, with the age signature of risk within households indicative of low susceptibility in the very young, and elevated susceptibility in the old; while extra-household risk seems more driven by behavior, with working age adults being at the highest risk.
As with many previous studies of SARS-CoV-2 transmission among household members and other close contacts, we find reduced risk of infection from household exposures among young children, and elevated risk of infection among those 65 or older.1 However, it is important to note that we only find this reduced risk among the youngest children in our study (5-9 year olds), while 10-19 year olds have a similar risk profile to working age adults. This is consistent with the hypothesis that young children may be biologically less susceptible to SARS-CoV-2 infection, though social and behavioral factors cannot be ruled out.
When we turn our attention to extra-household infections social factors seem to dominate risk, and both young children and older adults are at reduced risk of infection compared to working age adults. As children have returned to schools in Geneva, the social factors driving this pattern have likely changed significantly and we may see children become a more significant source of extra-household infections, despite their apparently lower susceptibility to infection. The risk that infected young children pose to their household members is unclear, we did not find any significant relationship between age of infector and probability of transmission (nor did including these terms improve model fit), but children are less often symptomatic and we did find a strong relationship between symptoms and transmission.
It has long been thought that asymptomatic individuals are less likely to transmit than symptomatic ones, though studies have recovered similar concentrations of viral RNA from naso-pharyngeal samples from these two groups.14 By using serological data, we were able to show that those not reporting symptoms have one-quarter the odds of transmitting within households as symptomatic ones; and ultimately caused about one-fifth of household infections. We have no direct evidence for the role of asymptomatics in community spread, but it is likely they may play an even larger role there as symptomatic individuals are more likely to stay home or take extra precautions to reduce exposures when sick.
Our study has a number of important limitations. Symptoms were self-reported and, given that the times of infection are unknown, they may not necessarily have been a result of the SARS-CoV-2 infection. Further, we looked at only a narrow range of symptoms to increase specificity, which left out more general symptoms (e.g., nausea, diarrhea) which may have been SARS-CoV-2 related. We detected only eight seropositive children under the age of 10, leading to large uncertainty in age-specific risk estimates for this group. While validation data of the Euroimmun ELISA from across the world have confirmed its high specificity and sensitivity for detecting recent infections,8,15,16 most data are from adults, and it is possible that performance in young children may be different.
Although most of the participants in the study were recruited after the epidemic peak, it is possible that we did not fully capture all infections in each household due to insufficient time to mount a detectable response or due to waning of responses. However, when conducting stratified analyses including households recruited early and late, we found few qualitative differences in the primary results (Figure S4). Furthermore, this study captures infections that occurred during the first wave of the pandemic in Geneva, a unique period of time when workplaces and schools were largely closed and peoples’ social contacts were greatly reduced. In future phases of this pandemic, we may expect differences in our estimates of the proportion of transmission that occurs between household members. Given the increasing importance of household transmission with increasing household size (Figure S6), and the relatively small household sizes in Geneva, we believe our estimates of the proportion of infections attributable to household transmission is lower than it would be in much of the world.
Our study highlights how biological and social factors combine to shape the risk of SARS-CoV-2 infection. While we expect some differences across settings, we believe that the trend in infection risk by age and increased transmissibility of symptomatic individuals are fundamental attributes of this pandemic. These differences have important implications for guiding patient care and public health policy. For example, increased susceptibility of the oldest individuals suggests that rapid and aggressive measures are needed to protect them as soon as there is any possibility that SARS-CoV-2 was introduced into their living environment. At the population level, quantifying the infectiousness of asymptomatics can help us understand the extent the pandemic is driven by asymptomatic infections. Continued serological monitoring of diverse populations with detailed analyses like those presented here are critical to the continued evidence-based response to this pandemic.
Data Availability
Code to reproduce analyses will be posted on github (https://github.com/HopkinsIDD/serocovpop-households) and data will be made available upon request to the corresponding author.
Author Contributions
Drs Azman and Stringhini had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Drs Azman and Lessler have contributed equally.
Concept and design
Bi, Lessler, Stringhini, Azman
Acquisition, analysis, or interpretation of data
Bi, Lessler, Eckerle, Lauer, Kaiser, Vuilleumier, Cummings, Flahult, Petrovic, Gessous, Stringhini, Azman
Drafting of the manuscript
Bi, Lessler, Stringhini, Azman
Critical revision of the manuscript for important intellectual content
Bi, Lessler, Eckerle, Lauer, Kaiser, Vuilleumier, Cummings, Flahult, Petrovic, Gessous, Stringhini, Azman
Statistical analysis
Bi, Lessler, Lauer, Azman
Obtained funding
Stringhini, Gessous
Administrative, technical, or material support
Stringhini, Gessous,Petrovic, Kaiser, Vuilleumier
Supervision
Azman, Lessler, Stringhini, Kaiser
Funding/Support
This study grants from Swiss Federal Office of Public Health, Swiss School of Public Health (Corona Immunitas research program), Fondation de Bienfaisance du Groupe Pictet, Fondation Ancrage, Fondation Privée des Hôpitaux Universitaires de Genève, and Center for Emerging Viral Diseases.
Role of the Funder/Sponsor
The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Supplemental material

Frequency of households of different sizes in the study (A), proportion seropositive by household size (B) and distribution of the number of seropositive people in household by size (C).

Study population by age group, sex, and household size. A) Number of individuals and seropositivity rate by age group, and by sex. B) Number of individuals and seropositivity rate by household size and sex. C) Number of individuals and seropositivity rate by household size and age group. Bar plots show the number of individuals in each group. Those tested seropositive and seronegative were colored in red and green respectively. The interval plots show seropositivity rate and 95% confidence interval in each group. Data that correspond to this figure are shown in Table 1.

Relative susceptibility to seropositivity analyzed using different definitions of seropositivity. In the main analysis, all samples with an optical density to cutoff ratio ≥1.1 were classified as being seropositive. In the sensitivity analysis, all samples with an optical density to cutoff >1.5 were classified as being seropositive. An odds ratio greater than 1 indicates infection is more likely to occur in this group compared to the reference group. The reference group for the age-specific and sex-specific odds ratio are 20-49 years old and female, respectively. The reference group for symptom status of potential infectors was infectors being asymptomatic. The reference group for self-reported reduction in social interaction since the start of the outbreak was no reduction, and relative susceptibility was estimated by those 20-64 years old and those 65 years old and over separately.
Relative susceptibility to seropositivity in the first and second half of the study period. First of the study period (first 6 weeks) spans from April 3rd to May 16th, and the second half (last 6 weeks) spans from May 18th to June 30th. An odds ratio greater than 1 indicates infection is more likely to occur in this group compared to the reference group. The reference group for the age-specific and sex-specific odds ratio are 20-49 years old and female, respectively. The reference group for symptom status of potential infectors was infectors being asymptomatic. The reference group for self-reported reduction in social interaction since the start of the outbreak was no reduction and was estimated for those 20-64 years old and those 65 years old and over separately.

Median probability of (A) extra-housheold infection over the duration of the outbreak and (B) infection from a single infected household member by age group and sex of the susceptibles. Bars represent 95% credible intervals.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportion of infections that occurred within a household of various household size (median and 95% credible intervals).
Household composition over the study period.
Model performance and estimated parameters of the adapted chain binomial models that incorporate key individual-level factors (e.g., age, sex, reduced extra-household exposure, extra-household contact frequency of the exposed individuals and symptom status of the potential infectors) that may be associated with susceptibility to infection from extra-household sources and by a single infected houseohld member. Odds ratio over 1 indicates higher susceptibility to infection.
Attributable fraction of extra-household infections, within household infections by symptomatics, and within household infections by asymptomatics.
Probability of infection from extra-household exposures and a single infected household member by age group and sex of the exposed individuals. Graphic representation of the results is shown in Figure 3.
Supplemental Text: Technical summary
1. Chain binomial model description and main assumptions
We built a series of models to estimate two quantities: 1) infection risk from extra-household sources and 2) infection risk from a single infected household member. These models are based on adapted versions of chain binomial models [7] that we fit to the final size of infections within households.
The model assumes that 1) each household member can be infected either from within a household or from extra-household sources, 2) household members mix at random within a household and can infect one another, and 3) all household members were initially susceptible to infection to SARS-CoV-2, and that infection to SAR-CoV-2 confers immunity to reinfection for the duration of the study period. In addition, we assume our serological survey fully captures all infections in a household.
We consider all possible sequences of viral introductions to each household and subsequent transmission events within the household. For example, in a household with 2 seropositive individuals, both could have been infected outside of the household, or one could have been infected outside and then infected one other person within the household. For each possible sequence of viral introduction and subsequent transmission events within the household, we assign generation of infections for each household member (i.e., generation for household member i). So, people infected from outside the household are assigned to generation 0, those they infect to generation 1, those generation 1 infects to generation 2, and so on. Uninfected individuals are assigned an implicit generation of infinity. We augment the data and denote each assignment for all members for household h as H Hh,k, where k denotes one possible sequence of viral introduction and subsequent transmission events within the household.
We define the probability of a household member i escaping infection from a single infectious household member j to be and the probability of individual i escaping infection from the community (i.e., outside the household) over the course of epidemic to be. We define the probability of household member i having an infection generation of as:
 where the first three terms,
where the first three terms,
 represent the probability of household member i escaping infection from extra-household sources and other infected household members up to generation, and
represent the probability of household member i escaping infection from extra-household sources and other infected household members up to generation, and
 denotes the probability of household member i being infected by any infected household member in generation.
denotes the probability of household member i being infected by any infected household member in generation.
We estimate as a function of an exposed individual’s characteristics (i.e., age and sex) and the infectors’ characteristics (i.e, symptoms and/or age).

Similarly, we estimate B, the probability of escaping infection from sources outside of household members since the start of the epidemic, as a function of an exposed individual’s characteristics (age and sex) in addition to two variables capturing self-reported behviours related to social contacts: the reduction in social interactions since the start of the pandemic, and the frequency of extra-household social contacts during the pandemic.

2. Inference
The likelihood of each generation assignment is:

And the likelihood of observing the final infection state (i.e., household attack rate) of a household h is then:

We set weakly informative priors on all parameters to be normally distributed on the logit scale with mean of 0 and standard error of 1.5. We ran four chains of 1,000 iterations each with 250 warm-up iterations and assessed convergence visually and using the Gelman-Rubin Convergence Statistic (R-hat).
3. Simulation of Infectors
We simulate the source of infection for all individuals in the study. We first draw one sequence of viral introductions and subsequent within-household transmission events (H Hh,k) from all k possible sequences for each household with seropositive individuals. We assume number of successful draws from each sequence (Y) follows categorical distribution,
 with Pr(H Hh,k) being the probability of each of the k sequences being drawn.
with Pr(H Hh,k) being the probability of each of the k sequences being drawn.
Next, for each individual, i, infected by a household member, we draw from this person’s potential infectors. We assume number of successful draws from each potential infector within the household (Z) follows categorical distribution,
 with 1 − Qi,j being the probability of a household member, i, being infected by an infected household member j.
with 1 − Qi,j being the probability of a household member, i, being infected by an infected household member j.
SEROCoV-POP STUDY TEAM
Silvia Stringhini1, 2, 3, Idris Guessous1, 2, Andrew S. Azman1,4,5, Hélène Baysson2, Prune Collombet1,2, David De Ridder2, Paola d’Ippolito1, Matilde D’asaro-Aglieri Rinella1, Yaron Dibner1, Nacira El Merjani1, Natalie Francioli1, Marion Frangville2, Kailing Marcus1, Chantal Martinez1, Natacha Noel1, Francesco Pennacchio1, Javier Perez-Saez4,5, Dusan Petrovic1,3, Attilio Picazio1, Alborz Pishkenari1, Giovanni Piumatti1,8, Jane Portier1, Caroline Pugin1, Barinjaka Rakotomiaramanana1, Aude Richard1,4, Lilas Salzmann-Bellard1, Stephanie Schrempft1, Maria-Eugenia Zaballa1, Zoé Waldmann2, Ania Wisniak4, Alioucha Davidovic2, Joséphine Duc2, Julie Guérin2, Fanny Lombard2, Manon Will2, Antoine Flahault1,2,4, Isabelle Arm Vernez9, Olivia Keiser4, Loan Mattera17, Magdalena Schellongova2, Laurent Kaiser2,6,9,14, Isabella Eckerle 2,6,9, Pierre Lescuyer6, Benjamin Meyer2, 13, Géraldine Poulain6, Nicolas Vuilleumier2,6, Sabine Yerly6,9, François Chappuis1,2, Sylvie Welker1, Delphine Courvoisier1, Laurent Gétaz1,2, Mayssam Nehme1, Febronio Pardo22, Guillemette Violot23, Samia Hurst7, Philippe Matute1, Jean-Michel Maugey22, Didier Pittet 12, Arnaud G. L’Huillier2,10, Klara M. Posfay-Barbe2,10, Jean-François Pradeau22, Michel Tacchino22, Didier Trono11
1. Division of Primary Care, Geneva University Hospitals, Geneva, Switzerland
2. Faculty of Medicine, University of Geneva, Geneva, Switzerland
3. University Centre for General Medicine and Public Health, University of Lausanne, Lausanne, Switzerland
4. Institute of Global Health, Faculty of Medicine, University of Geneva, Geneva, Switzerland
5. Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, USA
6. Division of Laboratory Medicine, Geneva University Hospitals, Geneva, Switzerland
7. Institut Ethique, Histoire, Humanités, University of Geneva, Geneva, Switzerland
8. Faculty of BioMedicine, Università della Svizzera italiana, Lugano, Switzerland
9. Geneva Center for Emerging Viral Diseases and Laboratory of Virology, Geneva University Hospitals, Geneva, Switzerland
10. Division of General Pediatrics, Geneva University Hospitals, Geneva, Switzerland
11. School of Life Sciences, Ecole Polytechnique Fédérale de Lausanne (EPFL), Lausanne, Switzerland
12. Infection Prevention and Control program and World Health Organization (WHO) Collaborating Centre on Patient Safety, Geneva University Hospitals, Geneva, Switzerland
13. Centre for Vaccinology, Department of Pathology and Immunology, University of Geneva, Geneva, Switzerland
14. Division of Infectious Diseases, Geneva University Hospitals, Geneva, Switzerland
15. Division of Diagnostics, Geneva University Hospitals, Geneva, Switzerland
16. Division of Women, Children and Adolescents, Geneva University Hospitals, Geneva, Switzerland
17. Campus Biotech, Geneva, Switzerland
18. Education Structure, University of Geneva, Geneva, Switzerland
19. Institute of Social and Preventive Medicine, Bern, Switzerland
20. Deutsches Primatenzentrum (DPZ), Göttingen University, Göttingen, Germany
21. Human Resources Department, Geneva University Hospitals, Geneva, Switzerland
22. Information Systems Division, Geneva University Hospitals, Geneva, Switzerland
23. Division of Communication, Geneva University Hospitals, Geneva, Switzerland
References



