
Abstract
To reduce the transmission of SARS-CoV-2 most countries closed schools, despite uncertainty if school closures are an effective containment measure. At the onset of the pandemic, Swedish upper secondary schools moved to online instruction while lower secondary school remained open. This allows for a comparison of parents and teachers differently exposed to open and closed schools, but otherwise facing similar conditions. Leveraging rich Swedish register data, we connect all students and teachers in Sweden to their families and study the impact of moving to online instruction on the incidence of SARS-CoV-2 and COVID-19. We find that among parents, exposure to open rather than closed schools resulted in a small increase in PCR-confirmed infections [OR 1.15; CI95 1.03–1.27]. Among lower secondary teachers the infection rate doubled relative to upper secondary teachers [OR 2.01; CI95 1.52–2.67]. This spilled over to the partners of lower secondary teachers who had a higher infection rate than their upper secondary counterparts [OR 1.30; CI95 1.00–1.68]. When analyzing COVID-19 diagnoses from healthcare visits and the incidence of severe health outcomes, results are similar for teachers but somewhat weaker for parents and teachers’ partners. The results for parents indicate that keeping lower secondary schools open had minor consequences for the transmission of SARS-CoV-2 in society. The results for teachers suggest that measures to protect teachers could be considered.
1. Introduction
In the effort to contain the spread of SARS-CoV-2 most countries closed schools during the ongoing pandemic. An estimated 1.3 billion students in 195 countries were affected by school closures in mid-April 2020 (UNESCO, 2020). These closures are likely to have a negative impact on student learning and well-being, especially for students from disadvantaged backgrounds (Dorn, Hancock, Sarakatsannis & Viruleg, 2020; Guessoum et al., 2020). School closures also affect labor supply, not least among healthcare workers, hence reducing healthcare capacity (Bayham & Fenichel, 2020). While the costs associated with school closures are high, modelling studies question their effectiveness in reducing the transmission of SARS-CoV-2 and direct evidence is largely missing (Viner et al., 2020). The absence of direct evidence is because school closures were usually implemented early, universally, and in close proximity to a raft of non-pharmaceutical interventions (NPIs) that have been documented and modelled to bring about large reductions in the basic reproduction number (Hsiang et al., 2020; Kraemer et al., 2020; Pan et al., 2020; Tian et al., 2020; Maier & Brockmann, 2020; Auger et al., 2020). This renders it difficult, if not impossible, to disentangle the effects of each specific intervention.
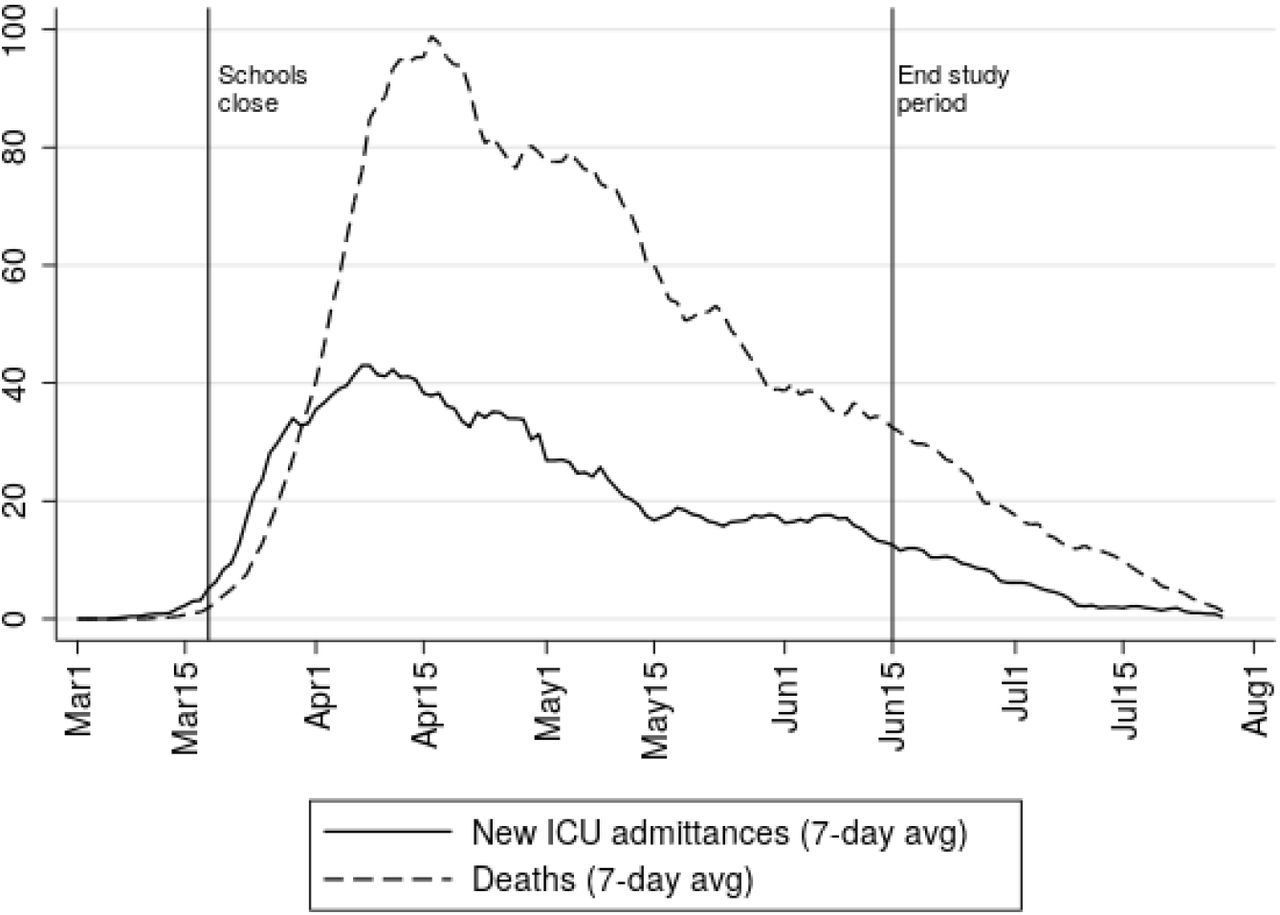
Sweden was an exception to the norm of universal school closures. On March 18, 2020, one week after the first reported death from COVID-19, upper secondary schools moved to online instruction while schools for younger students remained open until the end of the school year in mid-June. While other NPIs were also implemented (Public Health Agency of Sweden, 2020c), this partial school closure allows for a comparison of individuals and households who were differently exposed to open and closed schools, but otherwise faced similar conditions throughout the period of widespread contagion illustrated in Figure 1. In this study, we link detailed register data from Statistics Sweden on the entire Swedish population to all PCR (Polymerase Chain Reaction)-identified cases of SARS-CoV-2 reported to the Swedish Public Health Agency and COVID-19 cases requiring medical treatment reported to the National Board of Health and Welfare between the time of school closure to the end of the school year. To study the broad impact of school closures on the transmission of the virus, we estimate differences in infection rates between parents exposed to lower and upper secondary students. We further analyze differences in infection rates between lower and upper secondary teachers as well as their household partners.

COVID-19 deaths and ICU admissions. 7-day averages of deaths and ICU admissions. Solid vertical lines mark the start of school closure and the end of the period of analysis. Data from the Public Health Agency (Public Health Agency of Sweden, 2020a).
For school closures to affect the transmission they must affect behavior and contact patterns. While absenteeism among lower secondary students increased during the spring, student absences were not dramatically higher that usual (see online supplement). The impact of school closures on the transmission of SARS-CoV-2 further depends on how the virus spreads between students, from students to adults, and among adults in school and at home. Current reviews of the evidence suggest that while children and adolescents do get infected, they usually develop mild or no symptoms (ECDC, 2020). The susceptibility to infection appears to be lower among the young, but there is some uncertainty regarding this as a large number of cases probably go undetected. Children and adolescents with mild or no symptoms may still carry and spread the infection, but the evidence available indicates that infectiousness, just as the severity of symptoms, is increasing in age. Outbreaks have been reported in connection to school openings and overnight summer camps (Stein-Zamir et al., 2020; Szablewski, 2020), but transmission within schools prior to their closure at the onset of the pandemic appears to have been limited (Heavey, Casey, Kelly, Kelly & McDarby, 2020; Macartney et al., 2020). A general caveat concerning the available evidence is that most studies on the susceptibility and infectiousness of children and adolescents have been conducted when schools were closed and other NPIs were in place.
Differences between groups can be attributed to school closures if the groups are behaviorally and biologically similar in all other respects that affect the probability to get infected and tested. As lower secondary school (school years 7–9, typical age 14–16) is compulsory and attendance to upper secondary school (school years 10–12, typical age 17–19) is close to universal, the main selection concern regards the age of parents and students. Parental characteristics (age, sex, income, occupation, region of origin and of residence) are controlled for, but the susceptibility and infectiousness are likely to increase in student age and general behavior may differ between younger and older students. We therefore focus our attention to parents exposed to students in the final year of lower secondary and first year of upper secondary school. The main concern regarding differences between upper and lower secondary teachers and their partners refers to partner characteristics that, as for parents, are adjusted for. Given these restrictions and adjustments, the estimated differences can plausibly be attributed to the exposure to open and closed schools and the study thus offers credible direct evidence on the impact of school closures on the SARS-CoV-2 pandemic.
Models predict that school closures can be effective if they actually reduce the number of contacts, the basic reproduction number is low (R0<2), and the attack rate is higher in children than in adults (Jackson, Mangtani, Hawker, Olowokure & Vynnycky, 2014). The basic reproduction number for SARS-CoV-2 is above 2 (C.-C. Lai, Shih, Ko, Tang & Hsueh, 2020) and the attack rate in students is likely to be low relative to adults (ECDC, 2020). The theoretical prior is therefore that the impact of school closures on the transmission of SARS-CoV-2 among parents is low (Viner et al., 2020). For teachers and their partners, a more substantive impact can be expected. Teachers at open schools were not only exposed to students but also to other adults, both at work and during their commute. Upper secondary teachers, on the other hand, partly worked from school, but a substantive fraction did their teaching from home (see online supplement).
2. Results
We estimate differences in infections among parents, teachers, and teachers’ partners who were differently exposed to lower (open) and upper (online) secondary schools using linear probability models (OLS) and logistic regressions. Descriptive statistics are shown in Table 2. The preferred outcome is PCR-confirmed SARS-CoV-2 which has the highest incidence (8.75 cases/1000 among lower and upper secondary parents and 4.69/1000 among teachers). If we exclude healthcare workers who were targeted for testing, the incidence drops to 5.50/1000 among parents. One potential drawback of this outcome is that unbiased results rely on compared groups having equal propensity to get tested. In particular, it could be that those directly or indirectly exposed to open schools were more prone to get tested which would exaggerate the impact of school closures. The risk of such bias is alleviated by the limited testing capacity that forced testing to be targeted towards those with severe symptoms and care workers throughout most of the relevant period (see online supporting information). However, we also analyze COVID-19 diagnoses from healthcare visits which is less likely to suffer from bias due to behavioral differences. Healthcare coverage in Sweden is universal and fees for doctor or hospital visits are low, assuring individuals in need of care will seek care. This is particularly true for hospitalizations since admittance to hospital is determined strictly on medical grounds. As receiving a COVID-19 diagnosis is a less frequent event (4.22/1000 among parents; 2.60/1000 among teachers) these estimations have lower statistical power. Low incidence is an even larger problem for severe cases (hospitalization or deaths) which has an incidence of 2.36/1000 among parents and 1.59/1000 among teachers. Nevertheless, results for severe cases reported in the online supporting information are similar to those found for healthcare.
The data covers the entire relevant Swedish population and contains all reported cases as well as detailed information on covariates (see Materials and Methods and the online supporting information for details). Upper secondary schools moved online on March 18. Allowing for an incubation period from infection to symptoms of about a week (Lauer et al., 2020), the cut-off date is set to March 25 for teachers and April 1 for parents and teachers’ partners. The school year ends during the second week of June and the end date is therefore set to June 15 for PCR tests and June 30 for diagnoses through healthcare contacts.
Parental school exposure is defined by the school year that the youngest child in the household attends. In order to attribute estimated differences to school closures, households must be similar in all aspects that affects the likelihood of getting infected or tested, except for their exposure to open and closed schools. By narrowing the comparison to parents with the youngest child in the final year of lower secondary (Year 9) and first year of upper secondary school (Year 10), we reduce the risk of introducing biases due to confounding factors. Figure 2 shows the estimated odds ratios for PCR-confirmed SARS-CoV-2 parents from logistic regressions for where we adjust for age, sex, occupation, educational attainment, income, regions of residence and of origin (see Method and Materials). Results for parents by school years 7–12 show there is a tendency to a positive age gradient, potentially indicating a higher parental risk of infection when exposed to older children. The most relevant comparison is therefore between school years 9 and 10 (reference category) for which we in Table 1 estimate an odds ratio of 1.15 [CI95 1.03–1.27].

SARS-CoV-2 odds ratios for parents by school year of the youngest child in the household. Odds ratios estimated using logistic regression. The reference category is school year 10 and 95% confidence intervals are indicated.
Corresponding results using OLS are shown in Table 1 which also includes results for COVID-19 diagnoses from healthcare contacts. The estimates indicate that parental exposure to open schools results in 1.09 (se. 0.42) additional SARS-CoV-2 cases per 1000 individuals and 0.08 (se. 0.28) additional COVID-19 diagnoses per 1000. The odds ratio for COVID-19 diagnoses is 1.03 [CI95 0.88–1.19]. The results for COVID-19 diagnoses are not only significantly indistinguishable from zero, but also statistically indistinguishable from the estimates for PCR-confirmed SARS-CoV-2. Thus, we can not rule out that there are similar size effect on the probability to get a COVID-19 diagnoses when visiting a doctor or being admitted to hospital as the probability of a positive PCR tests. The same applies to the estimates for severe cases shown in the online supporting information [OR 0.99; CI95 0.82–1.21].
Next, we analyze differences between lower and upper secondary teachers and their partners. Upper secondary teachers constitute a relevant counterfactual to the work situation that lower secondary teachers had been in if their schools had moved to online instruction. The groups are also similar with respect to educational attainment and geographic dispersion. As there may still be differences in the household composition between the groups, we — in addition to the controls used for parents — adjust for the occupation and educational attainment of teachers’ partners, the number of children in separate age groups linked to the household, and whether or not the teacher is single. Table 1 shows that the likelihood of a positive PCR test was twice as high for lower secondary than for upper secondary teachers [OR 2.01; CI95 1.52–2.67]. Table 1 also shows the corresponding OLS estimate of 2.81 additional cases/1000 (se 0.59). The table further shows an estimate of identical magnitude for COVID-19 diagnoses [OR 2.01; CI95 1.45-2.79], indicating that the PCR results are not due to biased testing. Table S1 in the online supplement shows an estimate for severe cases of similar magnitude [OR 2.15; CI95 1.41-3.28].
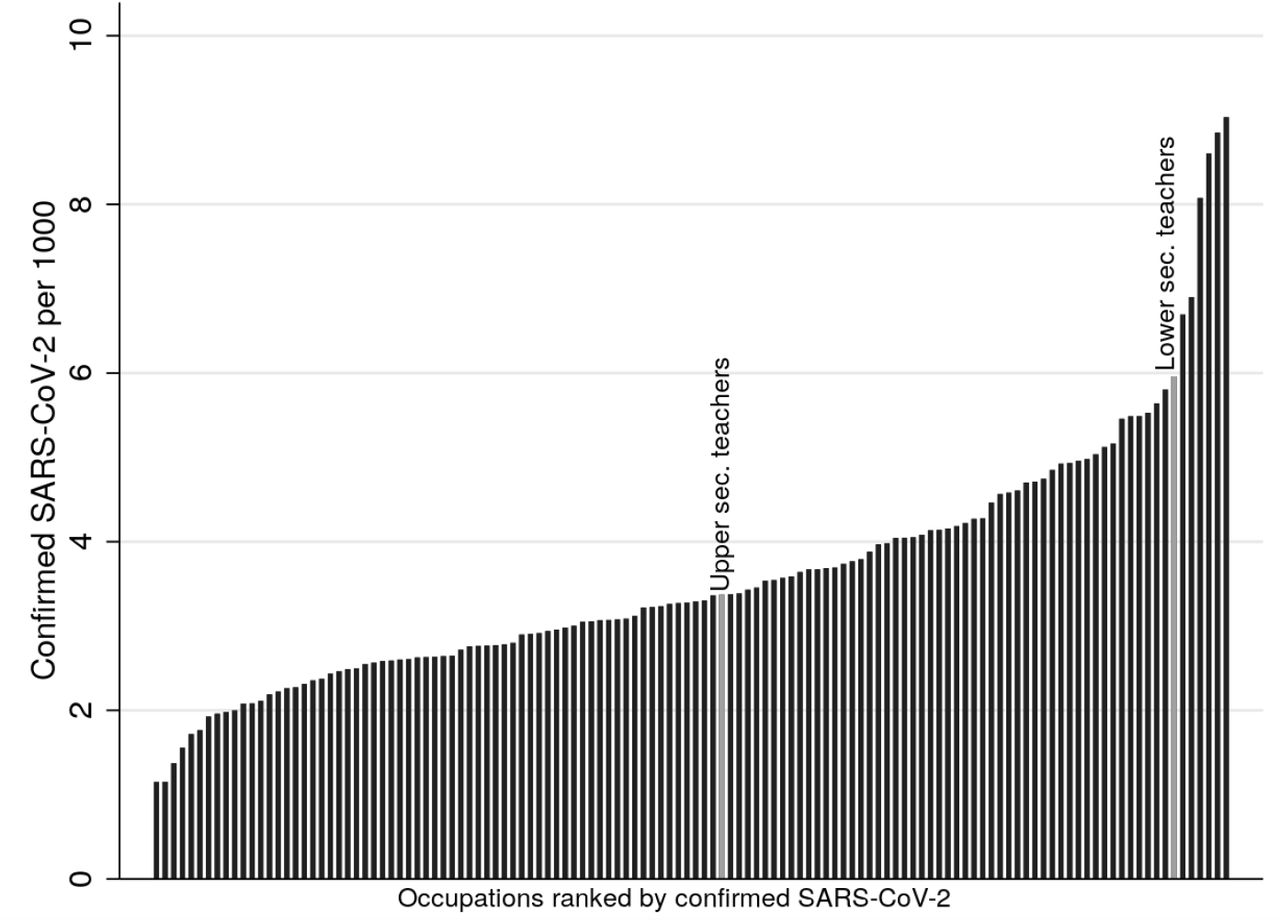
In order to gauge the magnitude of the estimated effects for teachers, Figure 3 shows the incidence of detected SARS-CoV-2 in 122 three-digit occupations with at least 1000 employees in ages 25–65 (healthcare workers excluded). Upper secondary teachers in our sample are at the median while lower secondary teachers constitute the 7th most affected occupation. Taxi drivers are the at the top of the distribution while driving instructors have the same level of infections as lower secondary teachers. As another comparison, Table 2 shows that the incidence of SARS-CoV-2 is similar among lower secondary teachers (5.91/1000) and the parents to the students that they teach (5.33/1000, excluding healthcare workers). This is also the case for COVID-19 diagnoses and more severe health outcomes.

SARS-CoV-2 across occupations. Incidence (cases per 1000) of detected SARS-CoV-2 by 3-digit occupational codes (SSYK2012) until June 15, 2020. Ages 25–65, only occupations with at least 1000 employees reported. Values for the upper and lower secondary teachers in our sample indicated.
The higher incidence of infections among lower secondary teachers spilled over to their partners who have a higher incidence of positive PCR tests than their upper secondary counterparts [OR 1.30; CI95 1.00–1.68]. This is evidence of within household transmission from teachers to their partners. However, the estimates for COVID-19 diagnoses for teachers’ partners are not statistically distinguishable from zero [OR 1.04; CI95 0.71–1.52] and the same applies for severe cases [OR 1.09; CI95 0.62–1.92]. The relatively imprecise estimates for these outcomes also renders them statistically indistinguishable from the estimates for PCR-confirmed SARS-CoV-2.
We check the robustness of the main results in several ways. First, media searches reveal that some lower secondary schools closed spontaneously and preemptively, albeit usually for a brief period in time (see the online supplement). As privately run independent schools were over-represented in this group, we exclude individuals connected to such schools. This results in marginally larger estimates for parents and teachers’ partners, and marginally smaller estimates for teachers. Second, schools were allowed to let small groups of students return to school to complete practical assignments and such practices may have been more common among vocational students. We therefore exclude parents connected to students in vocational upper secondary programs. This makes the groups exposed to open and closed schools substantially less comparable and it leads to a reduction in the point estimate (from 1.09 to 0.79 cases/1000) and an increase in the standard error. Third, rather than controlling for employment in the healthcare sectors, we drop teacher households where the partner is a healthcare employee. As expected, the results remain unchanged. Fourth, we derive a slightly different measure of parental exposure to lower secondary schools and use a more restrictive population of parents but the results remain unchanged. These results can be found in Tables S2 and S3 in the online supplement.
How school closures affect the transmission of the virus depend on how they reduce contact between those potentially infected. This may differ depending on contextual factors and we analyze two types of heterogeneity. First, we allow the estimates for exposure to lower secondary schools to differ by population density in the district of residence. Second, we let them vary by the regional rate of infections prior to school closure. The results presented in Table S4 in the online supplement reveal interaction terms with large standard errors not allowing a clear interpretation.
3. Discussion
On March 18, 2020, upper secondary schools in Sweden moved to online instruction while lower secondary schools continued instruction as normal. This partial school closure provides a rare opportunity to study the impact on the transmission of SARS-CoV-2 during a period of widespread contagion. The impact of school closures on the transmission of the virus in society is best captured by the results for parents. We find that parental exposure to open rather than closed schools is associated with a somewhat higher rate of PCR-confirmed SARS-CoV-2 infections [OR 1.15; CI95 1.03–1.27]. The association is, if anything, weaker for COVID-19 diagnoses from healthcare visits [OR 1.03; CI95 0.88–1.19] and severe cases that include hospitalizations and deaths [OR 0.99; CI95 0.82–1.21]. The positive association for PCR-confirmed cases could partly reflect other behavioral differences between house-holds with slightly younger and older children, but if treated as a causal the estimates indicate that a hypothetical closure of lower secondary schools in Sweden would have resulted in 341 fewer detected cases among the 312 575 parents in our sample. This can be related to 2679 detected cases in this group until mid-June (1666 cases when excluding healthcare workers). Due to the sample restrictions made, the actual number of parents exposed to lower secondary schools is higher and if we extrapolate to a total of 450 000 exposed parents, the estimates suggest 491 fewer detected cases. This can be related to the country total of 53 482 detected cases until mid-June (35 556 excluding healthcare workers). The relatively low impact of school closures on the transmission of the virus cannot be attributed to particularly harsh precautionary measures within the schools that remained open. Rather, the measures recommended (Public Health Agency of Sweden, 2020b) are best described as mild in an international comparison (Guthrie et al., 2020). In particular, there were no imposed class size reductions and no recommendations concerning the use of face masks. Face masks are also rarely used in Sweden (YouGov, 2020).
Teachers were more severely affected by the decision to keep lower secondary schools open. We estimate a PCR-confirmed infection rate twice as high among lower secondary teachers relative to teachers at upper secondary level [OR 2.01; CI95 1.52–2.67]. This is fully consistent with the results for COVID-19 diagnoses from healthcare visits [OR 2.01; CI95 1.45–2.79] and severe cases [OR 2.15; CI95 1.41–3.28]. When excluding healthcare workers, a comparison of SARS-CoV-2 infection rates across 122 occupations shows that while upper secondary teachers are at the median, the lower secondary teachers in our sample constitute the 7th most affected group. Other occupations with high infection rates (e.g. taxi drivers, driving instructors, social assistants, therapists, police officers) tend to have close interactions at work. This suggests that infections occur at school, but we cannot determine to what extent the effects are due to infections from students to teachers or if they reflect interactions between adults at school or during the commute. Increased infections among lower secondary teachers spill over to their partners who have a higher PCR-confirmed infection rate than their upper secondary counterparts [OR 1.30; CI95 1.00–1.68]. As for parents, the estimates are lower for COVID-19 diagnoses [OR 1.04; CI95 0.71–1.52] and severe cases [OR 1.09; CI95 0.62–1.92] among teachers’ partners. These estimates are relatively imprecise.
According to our estimates, 149 fewer cases of SARS-CoV-2 had been detected among lower secondary teachers and their partners if lower secondary schools had closed. To this we can add the estimated 491 fewer cases among parents. Most transmission is within households so even if 640 fewer detected cases is a lower bound, this can be seen as relatively low compared to the country total. Based on an age-specific case fatality rate (CFR) of 1.1% (see Table S5 in the online supplement), this corresponds to approximately 7 fewer deaths, 5.5 among parents and 1.6 among teachers and their partners. This counterfactual inference regarding mortality is highly uncertain, however, and in our sample we count a total of 24 COVID-19 related deaths at the lower secondary level (22 parents, 1 teacher, 1 partner). The corresponding number at the upper secondary level is 35 (all parents). As for severe health outcomes, we find 79 such cases (including one death) among the 39 446 lower secondary teachers in our sample. According to our estimates, this number had been down to 46 if lower secondary schools had been closed.
School closure is a costly measure with potential long-run detrimental effects for students. The results presented are broadly in line with theoretical work indicating that closing the schools is not a particularly effective way to contain SARS-CoV-2 (Viner et al., 2020), at least not when facing as high a level of contagion as Sweden did during the spring of 2020. Regardless of the limited overall impact on the virus transmission, keeping lower secondary schools open had a quite substantial impact on teachers. This should be taken into account and precautionary measures could be considered. It should, however, be noted that the incidence of SARS-CoV-2 and COVID-19 among lower secondary teachers is on par with the incidence among the parents of the students they teach.
Finally, it should be mentioned that we do not study the impact of school closures on students. Because of age related differences in access to testing (see online supplement), the severity of symptoms, risk behavior and patterns of socialization, results for students based on PCR-testing are likely to be biased and difficult to interpret. The rate of severe cases among children and adolescents is also too low to render a statistical analysis meaningful; 87 such cases are recorded among the 1.23 million students in compulsory school age (7–16) and 71 among the 339 000 youths in ages 17–19 that comprise the bulk of upper secondary students. It can also noted there were zero COVID-19 related deaths in age groups 2–19 recorded in Sweden until late July. There might be other health implications among students, but analyzing these are beyond the scope of this study.
4. Materials and methods
We construct estimation samples for parents, teachers and their partners using registers held by Statistics Sweden. Through the Multi-Generation register (MGR) and Longitudinal integrated database for health insurance and labor market studies (LISA) we identify all parents with children in relevant ages in their households. Children are assigned to school year, schools and upper secondary programs using the Student Register as per October 15, 2019. We sample all parents in Sweden and their partners living in households with the youngest child in lower or upper secondary school. We also include parents with a biological or adopted child who do not live in the same household but in the same region. Information on detailed place of residence as of December 31, 2019, is available for all individuals in Sweden in the Register of the Total Population (RTB). The sample of teachers includes all teachers working at the lower or upper secondary levels in the Teacher Register and refers to the status of the teacher in the fall of 2019. Their partners are identified using the household identifier in LISA. See the online supporting information for further details on the estimation samples. Information on the covariates: disposable income, educational attainment and occupation are available in LISA. Occupations are reported according to the Swedish Standard Classification of Occupations (SSYK 2012) which is based on the international classification (ISCO-08). There are 46 occupation categories on the 2-digit level.
Information on positive PCR tests of SARS-CoV-2 is from the Swedish Public Health Agency. Up until late July there were 75/ 933 reported cases of SARS-CoV-2, out of which test dates are missing for 2506 cases. As majority of the cases without test date are reported outside the main period of analysis, they are discarded. Personal identifiers are available for all cases, making it possible to link the test results to register data. Information on COVID-19 diagnoses until June 30 from the Inpatient-and Outpatient register is available from the National Board of Health and Welfare and on deaths from the Cause of Death register held by Statistic Sweden. By June 30, 2020, 33 596 individuals had been diagnosed with COVID-19 (ICD 10 codes U07.1 or U07.2) either in the Patient registers or the Cause of Death register.
Table 2 reports descriptive statistics for parents, teachers and teachers’ partners, starting with the incidence of positive PCR tests of SARS-CoV-2 as of June 15. Since healthcare workers were prioritized for testing, we also present the incidence among parents and teachers’ partners excluding those working in healthcare separately. Healthcare workers are excluded by dropping those with occupational codes 15, 22, 32 and 53 (SSYK2012). The table further shows the incidence of positive PCR test prior to the cut-off date chosen to reflect the infection rate prior to the move to online instruction at the upper secondary level (March 25 for teachers, April 1 for parents and partners). The table next displays the incidence of COVID-19 diagnoses from healthcare visits and the incidence severe cases as of June 30. Finally it displays the number of COVID-19 related deaths in each sample as of July 25 and the number of individuals in each group.
We use ordinary least squares (OLS) and logistic regressions to empirically analyze if SARS-CoV-2 infection can be attributed to being exposed to open or closed schools. We estimate the following OLS regression model for the three populations: parents, teachers and teachers’ partners:

The outcome yi is an indicator variable for a positive SARS-CoV-2 PCR test or being diagnosed with COVID-19 by a doctor in outpatient care or at a hospital. yi, prior is an indicator for SARS-Cov-2/COVID-19 before the cut-off date (March 25 for teachers, April 1 for parents and partners). Open is an indicator variable taking the value (1) if individual i is exposed to (open) lower secondary schools. Parents with the youngest child in lower secondary school is defined as exposed and parents with the youngest child in upper secondary school is defined as unexposed. Lower secondary teachers and their partners are defined as exposed and their upper secondary counterparts as unexposed. X is vector of individual and household characteristics. When estimating the model for teachers the vector includes: 20 indicators for age categories, sex, 7 indicators for categories of educational attainment, 46 indicators of categories of partners’ occupation, 12 region indicators of country of origin for those not born in Sweden, log of household income, 290 indicators of municipality of residence and household exposure to the number of children in age groups 2–6, 7–16, 17–19, and 20+ who reside in the same region as the teacher. The municipality fixed effects are exchanged for 21 region fixed effects when estimating the logistic model. The equivalent vector of variables is used for teachers’ partners, with the exception of own occupation instead of partner occupation. The vector of controls for parents include a similar set of variables as for teachers: age categories, sex, municipality of residence, educational attainment, occupational categories (own and partners’), region of origin for those not born in Sweden, the log of disposable family income and indicators for missing data on any of these variables. Standard errors are clustered at the school level when estimating the model for teachers and teachers’ partners and at the household level when studying parents.
Data Availability
The data used for the analysis have been obtained by combining several administrative registers collected and held by three government agencies: Statistics Sweden, The National Board of Health and Welfare and The Public Health Authority. Access to these data sets is restricted by national regulations, but any researcher wishing to replicate our results can apply for access through these agencies. Since the study involves sensitive individual level data, getting access to the data also requires approval from an Ethics Board.
Supplementary information for
S1. Context
Compulsory schools were kept open for instruction, but to reduce transmission the following precautionary measures were recommended (Public Health Agency of Sweden, 2020b): enhanced facilities for hand washing and disinfection; posters encouraging hand washing; increased distance in classrooms and dining halls, if possible; avoidance of large gatherings, as far as possible; minimize activities like open houses and parental meetings; increased outdoor activities, if possible; avoidance of close contacts between staff and students and between students; enhanced cleaning of heavily exposed areas and keyboards/tablets. Compared to school opening policies in other countries, the precautionary measures in Sweden are best described as mild (Guthrie et al., 2020). In particular, there were no imposed reductions of class size and no recommendations concerning the use of face masks.
On March 18, upper secondary schools and institutions of higher education moved to online instruction. Upper secondary schools thus closed for normal instructions just as the number of deaths and ICU admissions began to increase (see Figure 1 in the main text). Although upper secondary school moved to online teaching, some teachers were still teaching online from the school premises. According to a survey conducted by a large teachers’ union during the last week of April and first week of May, 21 percent taught from the school, 46 percent partly from home, and 33 percent only from home (National Union of Teachers, 2020). As expected, compulsory school teachers mainly taught from school; merely 2 percent of the teachers in compulsory schools had been partly teaching online from home and 1 percent had only been teaching from home. There have also been media reports of substantial student absenteeism in compulsory schools. Again there are no official reports but according to the same survey, 18 percent of compulsory students were absent on a typical day. In a survey of 27 compulsory schools conducted by the National Board of Education during late April, 7 schools reported that absenteeism among compulsory school students was about normal, 13 that there was an increase in absenteeism of between 20 and 50 percent, and 7 stated an increase of more than 50 percent (Swedish National Agency for Education, 2020b). Based on these surveys, we draw the conclusion that student absenteeism at the lower secondary level was not dramatically high, even though there are local exceptions.
S2. Data and sample restrictions
The sample of parents is constructed as follows. We define household adults who are exposed to their own children (biological or adopted) or a new partner’s children from a previous relationship as parents. For separated parents, we use the household identifier in LISA to identify any current partner. This enables us to identify new couples who are either married or have common children. Households consisting of unmarried cohabitant couples without common children cannot be identified and will be categorized as single households. The study population consists of parents who have children in school years 7–12 in the household, or biological children in these school years living in the same region. Because parents are less likely to interact regularly with children living at a distance, only children residing in the same region are considered in the analysis. There are 21 regions in Sweden and they are thus relatively large geographical areas. There were recommendations against leaving the region of residence during most of the spring 2020.
We sort parents by the age of the youngest child connected to the parents in the household or through biological links. Parents are considered exposed to lower secondary schools if their youngest child is enrolled in school years 7–9. Unexposed parents are defined by their youngest child being enrolled in upper secondary school. In the analysis we will focus on parents with the youngest child in school years 9 and 10 since they are likely to be the most similar in all other aspects, except for parents with their youngest child in the 9th school year being exposed to an open school. This analysis population consists of 205 844 adults.
The teacher sample consists of teachers working in lower and upper secondary schools according to the Teacher Register. Teachers with children born in 2019 are excluded as they are likely to be on parental leave during the spring of 2020. We also exclude those recorded as being on leave of absence during the fall of 2019. The final sample consists of 72 946 teachers. For the sample of teachers’ partners, we connect partners to teachers using the household identifier from LISA. This enables us to identify partners who are either married to or have common children with the teacher. The resulting sample consists of 47 384 partners.
Our main outcome variable is positive PCR test reported to the Public Health Agency but we also analyse the incidence of COVID-19 diagnoses from healthcare visits and severe cases of COVID-19 (hospitalizations and deaths) reported to the National Board of Health and Welfare. The first case of SARS-CoV-2 in Sweden was reported on 31 January, 2020, and the disease was classified as a danger to public health and to society on the following day (Public Health Agency of Sweden, 2020a). Among other things, this classification means that all documented cases of active infection have to be reported to the Public Health Agency. Testing capacity was slow to expand and from March 13 (week 11), testing was directed towards healthcare employees and individuals with symptoms of COVID-19 in need of healthcare. As can be seen in Fig. S1, testing increased substantially from early June (week 23). Healthcare is the responsibility of Sweden’s 21 healthcare regions as is testing for SARS-CoV-2. Thus, there are regional differences in testing capacity as well as rules and recommendation regarding testing. Some regions have recommended not to test children under 16 (for example Västra GÖtaland and Uppsala) and some have not had any age restrictions (for example Skåne). The number of detected cases does therefore not well reflect the actual rate of infections and the rate of positive tests remained high throughout June (week 27). By June 15, a total of 383 000 PCR tests had been performed (3800 per 100 000 inhabitants) (Public Health Agency of Sweden, 2020d).
S3. Robustness tests
As discussed in the main text, a concern is that the propensity to get tested for SARS-CoV-2 is affected by being connected to open and closed schools, regardless of health status. This is less of a concern for COVID-19 diagnoses made by the healthcare sector, especially severe cases which requires hospital care or cause death. As a robustness test we report results for severe cases defined as admittance to hospital or death due to COVID-19. The estimates presented in Table S1 are similar to those found for healthcare diagnoses that are presented in the main text.
Despite school closures not being imposed by the government, some lower secondary schools spontaneously moved to online instruction. Thus, some lower secondary school may be classified as having on-site instruction when they in fact conducted the teaching online. No official records on such closures exist but based on searches in media archives, they were rare and usually short-lived. There are approximately 1500 lower secondary schools in Sweden and we find 40 media reported closures. Out of these, 11 were reactions to cases among students or staff while 29 were proactive. Privately managed independent schools (26 percent of all lower secondary schools) are vastly over-represented in reports on such proactive closures (22 cases). See details on media searches in the next section. To explore this we re-estimate the OLS model excluding individuals with their youngest child exposed to independent lower secondary schools. We find that this only marginally affects the results for teachers and their partners (Table S2) but increases the estimates somewhat for parents (Table S3).
We investigate if the estimated effects on teachers and teacher’s partners are due to lower secondary teachers being more exposed to the healthcare sector through the teacher’s partners occupation. This should be adjusted with the indicators for occupational categories included in the model. However, to further explore whether this is a concern we exclude teachers whose partners work in healthcare (occupational codes 15, 22, 32 and 53) and re-estimate the model. This change does not have any significant effect on the estimates (Table S2).
At the upper secondary level, schools were allowed to let small groups of students complete practical elements of education and assignments, provided that schools deemed that this could be done safely (Swedish National Agency for Education, 2020a)). This mainly concerned students at vocational programs since practical skills taught at vocational programs are difficult to teach online. Students at vocational programs were also generally allowed to continue apprenticeships, provided that this was practically feasible. We investigate whether this affects our results by excluding parents with the youngest child exposed to upper secondary vocational programs. The estimates reported in Table S3 show a small decrease in the estimates relative to the baseline.
Finally, we estimate the main model using an alternative measure of exposure to lower secondary school for parents. Instead of defining a parent as exposed if they have the youngest child in school year 9 and not exposed if they have the youngest child in school year 10, we define a parent as exposed if they have a child in the household, or a biological or adopted child residing in the same region, in lower secondary school. We remove families with children not in secondary school. Since we want to compare parents with lower secondary children to parents with children of a similar age we control for having a child in school year 11 and 12. Thus, the estimate presented in the last column of Table S3 shows the effect of being exposed to a child in lower secondary school compared to being exposed to a child in upper secondary school year 10. The effect is of similar magnitude as in the main specification.
S4. Heterogeneity analysis
The expected impact of school closures on virus transmission depends mainly on the magnitude of contact reduction. Two factors that may be of importance for the effect is population density and how widely spread the virus was prior to schools closing. A study of US districts show that transmission of SARS-CoV-2 increases with population density (Korevaar et al., 2020). This suggests that when people live close, each person interact with more people and hence are more likely to transmit the virus. The consequences for the effectiveness of school closures is, however, unclear. On the one hand, school closures may have a larger impact in densely populated areas if isolation lead to larger reductions of the number of contacts. On the other hand, if a larger share of the interactions take place outside of school in densely populated areas, the expected effect should be smaller. To investigate this matter we implement a heterogeneity analysis by district population density, categorizing districts with a population density above the 75th percentile as high density districts.
Timing of the interventions has been shown to be important for the effectiveness of NPIs (S. Lai et al., 2020). This suggests a larger impact of closing school when the spread within society is low. Therefore we investigate whether the impact of school closures depends on the spread of the virus prior to schools were closed. Regions with above the populated weighted median spread of 12 cases per 100 000 are categorized as high spread regions, i.e. the regions (cases per 100 000 in parenthesis): Stockholm (20), Uppsala (16), ÖstergÖtland (16), Skåne (16), SÖrmland (13) and JÖnkÖping (12).
The econometric model is modified by adding interaction terms between indicators for high population density, respective high initial contagion, and exposure to lower secondary school as well as interactions with all control variables except for the municipality indicators. The results from the analysis is reported in Table S4. As the estimated standard errors are large, it is not possible to draw any clear conclusions. The interaction effect with high population density is negative or close to zero in all models but the estimates are not statistically significant. The interaction with initial level of contagion is also not statistically significant in any model.
S5. Media searches
In order to get information on spontaneous closures of lower secondary schools, media searches were conducted using the service Mediearkivet/Retriver and on Sveriges Radio’s site (public service radio with substantial local presence). Search terms were permutations of “school closure” (skolstängning/skola stängd), “distance education” (distansundervisning), “online education” (onlineundervisning), “corona” and “covid”. Results for individual schools were followed by web searches to find more information on each particular case. Spontaneous closures were recorded as proactive if they did not occur as a result of cases detected at the school and reactive otherwise. Provided that information is available, a closure is labelled as brief if the duration was less than a week.
In total, reports on 40 closures were found (27 among privately managed independent schools). 29 of these were proactive (22 among independent schools) while 11 were reactive (5 among independent schools). Spontaneous closures thus appear to have been rare and independent schools are vastly over-represented among those that closed proactively. Two of the reactive closures were on advice from the local disease protection officer and they both occurred late in the school year (June 6 and 8). Information on the duration was usually not available, but of the 18 reports from which the duration can be judged, 12 were brief. Several of the closures were also partial, meaning that school days were cut short, rolling schedules introduced, or that instruction partially moved online. Details on each specific report are available from the authors.
S6. Cases, deaths and the case fatality rate
To extrapolate the expected effect of school closure on the number of deaths in Sweden we derive the case fatality ratio (CFR) for different age groups. CFR is calculated by dividing the number of deaths with the number of cases and hence crucially depend on the testing regime. Table S5 shows the incidence of detected SARS-CoV-2 in different age groups until June 15, 2020, and the number of deaths among these cases reported until July 25. The numbers are shown both including and excluding healthcare workers, for which testing was more accessible. The CFR increases with age, except for the higher value for the youngest age group due to one dead child. This child was younger than one years old and thus not directly exposed to schools. The average age among teachers is 48, their partners 49 and parents 50 years old. Based on the CFR distribution in Table S5 we calculate the expected effect on mortality among lower secondary parents using a CFR of 1.1 percent.

Tests and cases per week. Weekly number of PCR tests and positive cases. Vertical lines indicate weeks 14 and 24, the approximate period of analysis. Data from the Public Health Agency (Public Health Agency of Sweden, 2020d).
Footnotes
↵* Vlachos: Stockholm University. E-mail: jonas.vlachos{at}ne.su.se.
↵† Hertegård: Uppsala University. E-mail: edvin.hertegard{at}nek.uu.se.
↵‡ Svaleryd: Uppsala University. E-mail: helena.svaleryd{at}nek.uu.se. This project was approved by the Swedish Ethical Approval Board (Etikprövingsnämnden) on May 19, 2020 (decision number 2020-02323). The data on PCR tests was first made available on July 28, 2020. Due to reporting errors, the PCR data was updated on October 2, 2020. Data on healthcare outcomes was received on September 24, 2020. We are grateful for financial support from Handelsbankens forskningssiftelser, and for comments by Jonas Björk, Lena Edlund, Jens Engleson, Tove Fall, Erik Grönqvist, Emily Oster, Oskar Nordström Skans and David Strömberg. Data is available from Statistics Sweden, the Public Health Agency, and the National Board of Health and Welfare following an ethical review.




{kind=link}
{kind=link}
{kind=link}
{kind=link}