
Abstract
Background The early stages of the COVID-19 pandemic illustrated that SARS-CoV-2, the virus that causes the disease, has the potential to spread exponentially. Therefore, as long as a substantial proportion of the population remains susceptible to infection, the potential for new epidemic waves persists even in settings with low numbers of active COVID-19 infections, unless sufficient countermeasures are in place. In this study, we examine the Australian state of New South Wales, a setting with prolonged low transmission, high mobility, non-universal mask usage, and a well-functioning test-and-trace system. We investigate how vulnerable the state would be to resurgences in COVID-19 transmission under variations in the levels of testing, tracing, and mask usage.
Methods We use a stochastic agent-based model, calibrated to the New South Wales epidemic and policy environment, to simulate possible epidemic outcomes over October 1 – December 31, 2020, under a range of assumptions about contact tracing efficacy, testing rates, and mask uptake.
Results We find that the relative impact of masks is greatest when testing and tracing rates are lower (and vice versa). With very high testing rates (90% of people with symptoms, plus 90% of people with a known history of contact with a confirmed case), we estimate that the epidemic would remain under control until at least the end of 2020, with as little as 70–110 new infections estimated over October 1 – December 31 under high mask uptake scenarios, or 340–1,400 without masks, depending on the efficacy of community contact tracing. However, across comparable levels of mask uptake and contact tracing, the number of infections over this period would be up to 6 times higher if the testing rate was 80% instead of 90%, 17 times higher if the testing rate was 65%, or more than 100 times higher with a 50% testing rate.
Conclusions Our work suggests that testing, tracing and masks can all be effective means of controlling transmission in dynamic community settings. A multifaceted strategy that combines all three, alongside continued hygiene and distancing protocols, is likely to be the most robust means of controlling community-based transmission of SARS-CoV-2.
Introduction
Across the world, governmental responses to the ongoing COVID-19 pandemic have already profoundly curtailed the spread of SARS-CoV-2, the virus that causes the disease. As the pandemic unfolded during the second half of 2020, the nature of the governmental responses also evolved. An increasing number of countries moved from an initial crisis-management phase into a new phase centred around minimising transmission risk while allowing societal and economic activities to resume (1). In this paper, we focus on three key components of this phase: masks (either mandatory or recommended in certain settings), testing, and contact tracing, whereby those known to have been in contact with a confirmed case are required to test and/or quarantine. When used in combination with physical distancing and hand hygiene measures, all three strategies allow relatively high mobility: testing and contact tracing means that only those at greatest risk of transmitting the virus need to stay home, while masks mean that people with undiagnosed infections present less of a risk to others (2–4).
Given the complexities of COVID-19 transmission, including the duration of pre-symptomatic infection (5,6), the proportion of infections that are asymptomatic (7), and the possibility of transmission via surface contact (8), maintaining control of COVID-19 has proven challenging in many jurisdictions (9–13). The often-cited success stories of Taiwan, Vietnam, Thailand, and South Korea included high mask usage, high rates of testing, and fast, effective contact tracing (14–16). The benefits of a multi-pronged approach have also been illustrated in the literature; in the UK, for example, a recent study (17) found that mandating masks in secondary schools could achieve approximately the same reduction in resurgence risk as having an 8-11% increase in symptomatic testing.
In this work, we use an agent-based model to estimate the combination of testing, community-based contact tracing, and mask usage required to maintain epidemic control in a low-transmission, high-mobility setting. The context for our study is the Australian state of New South Wales (NSW), with a population of 7.5 million and just over 4000 diagnosed cases as of September 30, 2020. Over the period from June 1 – September 30, 2020, masks were recommended by the government for the general public and made mandatory for staff in various businesses including supermarkets. Across Australia, 58% of people reported wearing masks in mid-August, including all Victorians (18); the proportion of people in NSW wearing masks has not been reported, although CCTV footage from August registered ∼30% of passengers on urban public transport wearing masks (19). At the same time, high levels of testing (∼20,000 tests/day) and rapid contact tracing were in place, with notable focus on contact tracing. The state health department (NSW Health) required all businesses to have a COVID-19 Safety Plan, and for the majority of public-facing businesses this included a requirement for customers to register their details upon entry. Upon identifying a new case, NSW Health’s contact tracers would then (a) conduct an extended interview to determine all possible venues in which transmission may have occurred, (b) place details of those venues on their website, on social media, and in newspapers, urging people who had been at the venue to self-isolate for 14 days, (c) attempt to contact all people who were registered to have been at venues within a given window of the time that the diagnosed case was known to have been there and instruct them to self-isolate for 14 days. Over the four months from June 1 – September 30, 2020 while this strategy was in place, approximately 900 new cases were identified, and only 45 (5%) of these were locally acquired and not linked to known clusters (20).
This paper builds on previous work in which we estimated the probability of epidemic rebound following a prolonged period of low, stable transmission and relatively high community mobility (21), assuming that 25% of contacts encountered in locations that require customer registration (including restaurants, cafes, bars, pubs, sports/leisure/fitness centres, arts venues, places of worship, and large events) could be traced within two weeks. However, in this study we consider a range of testing and contact tracing levels, and assess the balance between masks, testing and contact tracing as a means of controlling community-based transmission.
Methods
Transmission model
As in our previous study (21), we used an open-source agent-based model, Covasim (22), developed by the Institute for Disease Modeling with source code and documentation available at https://covasim.org. To simulate the epidemic and policy environment in New South Wales over March 1 – September 30, 2020, we include parameter changes that capture the testing, tracing, isolation, quarantine, and lockdown policies that were enacted over this time (summarised in Table S1), as well as the introduction of interstate cases in late June prior to the closure of the state border with neighbouring Victoria. We then calibrate the model by adjusting the per-contact transmission rate to fit data on the daily number of cases diagnosed, excluding cases acquired overseas or interstate, by performing an automated search for the values of the per-contact transmission risk and the number of seed infections that minimised the absolute differences between the model projections and the data (Figure 1). All data and code used in these analyses are available via Github (https://github.com/optimamodel/covid_nsw).
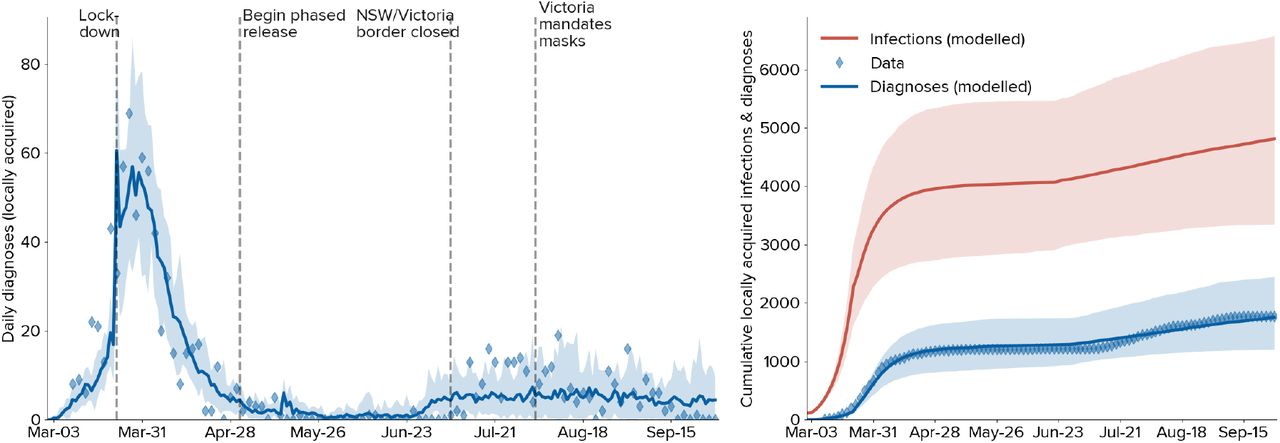
Calibration of the model to the NSW epidemic. Solid lines indicate the median model projections over 20 model runs; shaded areas indicate 95% projected intervals over different initialisations; blue diamonds indicate data on confirmed locally-acquired cases.
Model analysis
We run the model from October 1, 2020, until December 31, 2020, using a set of assumptions about future testing rates, the efficacy of contact tracing, and mask uptake. For testing rates, we distinguish between symptom-based testing and testing of asymptomatic contacts. NSW Health guidelines advise anyone with symptoms to get tested, as well as anyone identified as a contact regardless of symptoms (23). To reflect this, we use a baseline assumption that the testing rate for asymptomatic contacts is the same as for people with symptoms, and run a counterfactual set of scenarios in which it is assumed to be half the rate for those with symptoms (Table 1).
overview of the 160 scenarios (4×2×5×4) analysed over Oct 1 – Dec 31, 2020.
To model the efficacy of contact tracing, we assume that 100% of household contacts will be traced and notified on the same day that test results are communicated, and that 95% of school contacts and 90% of workplace contacts will be notified on the following day. We then consider scenarios in which 0%, 25%, 50%, 75%, or 100% of all other contacts (which we refer to as community contacts) can be traced within a week of a case notification. For each scenario, the time to trace each contact is drawn from a scaled Poisson distribution with a mean of 1 day (Figure S1). We also assume that 0%, 25%, 50%, or 75% of the population will wear masks in dynamic community settings (i.e., settings in which people interact with strangers or random groups of people), which in the model includes arts venues, large events such as concerts, festivals, sports games, public parks and other outdoor settings, public transport, and all other community settings. We run 20 simulations for each permutation of testing rates, mask usage and contact tracing efficacy.
For all simulations, we assume that masks will reduce the per-contact probability of transmission by 30%, in line with estimates from (24). We also assume that people who have been contact-traced will quarantine with 90% efficacy from their workplace, school, and community contacts. Test results are assumed to be communicated within 24 hours (25).
Results
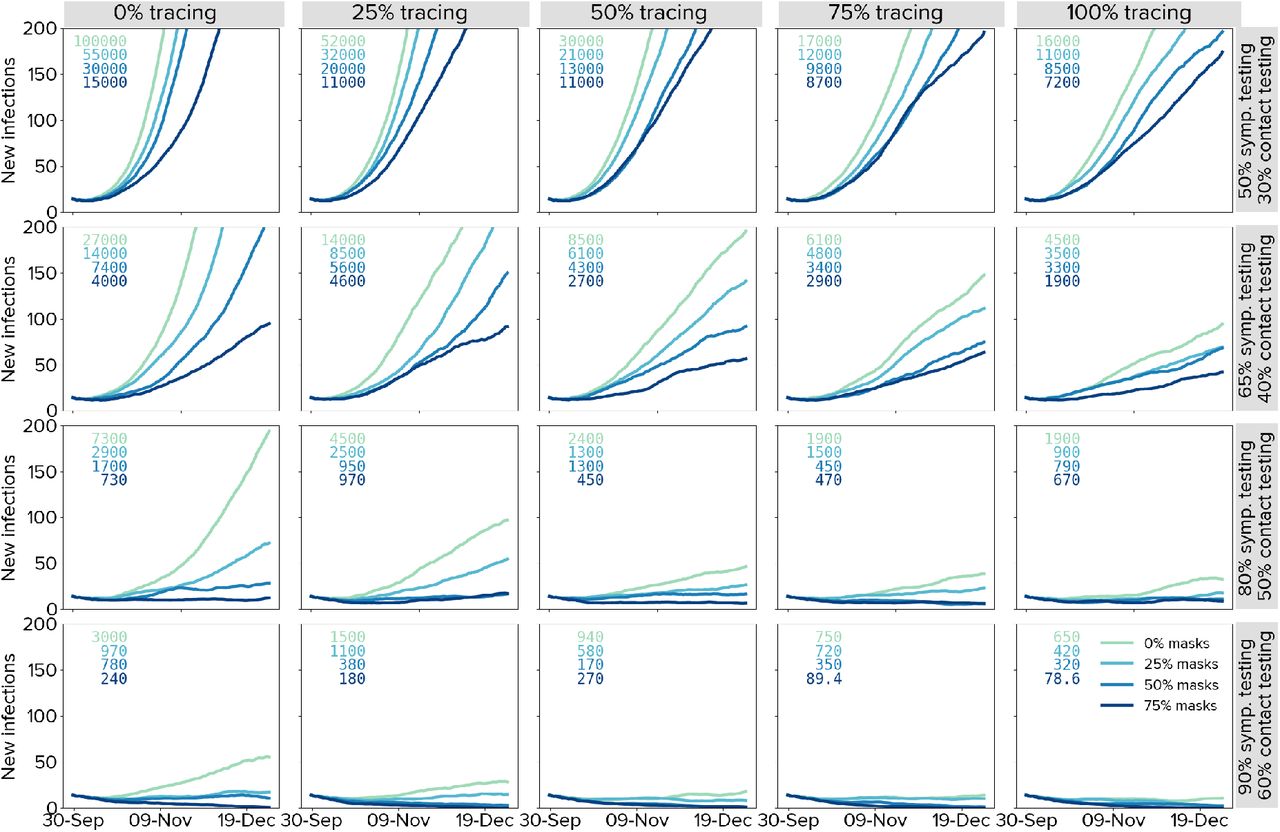
Estimates of daily new infections under each scenario are presented in Figure 2. A key finding highlighted by Figure 2 is how effective high levels of testing are in maintaining epidemic control: all strategies in which there is at least some contact tracing in place and testing rates are very high (90% of people with symptoms and 90% of asymptomatic contacts of confirmed cases) lead to a robustly controlled epidemic, with as little as 70–110 new infections estimated over October 1 – December 31 under high mask uptake scenarios, or 340–1,400 without masks, with the ranges depending on the efficacy of community contact tracing (Figure 2, bottom row). However, holding mask uptake and contact tracing constant, we estimate that the number of infections over October 1 – December 31, 2020, would be up to 6 times higher if the testing rate was 80% instead of 90%, 17 times higher if the testing rate was 65%, or more than 100 times higher with a 50% testing rate (Figure 2, third row).

Trailing 14-day average of daily new infections under different assumptions about the testing rate (rows), proportion of community contacts that can be traced within one week (columns), and mask uptake (line colours). Projections represent the median of 20 simulations. Text boxes in each panel displays the cumulative number of infections over October 1 – December 31, 2020.
A second key finding is that the lower the testing rate, the greater the impact of masks and contact tracing (and vice versa). With medium-lower testing rates of 50% or 65%, the marginal impact of both masks and contact tracing are considerable (Figure 2, top two rows). Under these scenarios, the most robust strategies consist of a combination of masks and community contact tracing. Assuming a 50% testing rate, a scenario with near-perfect tracing and no masks is approximately equivalent to a scenario with no tracing and high mask uptake. However, without community contact tracing, a reduction in mask usage from 75% to 50% would lead to a near-doubling in estimated infections (from 11,500 to 21,800), whereas even moderate levels of community contact tracing (25% traceable within a week) would increase the robustness of the response to lower mask usage (with 9,260 infections estimated under 75% mask usage and 13,700 under 50% mask usage). Similarly, masks strengthen the resilience of the epidemic outcome to decreases in contact tracing efficacy: without masks, a reduction in community contact tracing from 100% to 75% would lead to a 40% increase in total infections, whereas it would have no impact if 75% of the population were wearing masks.
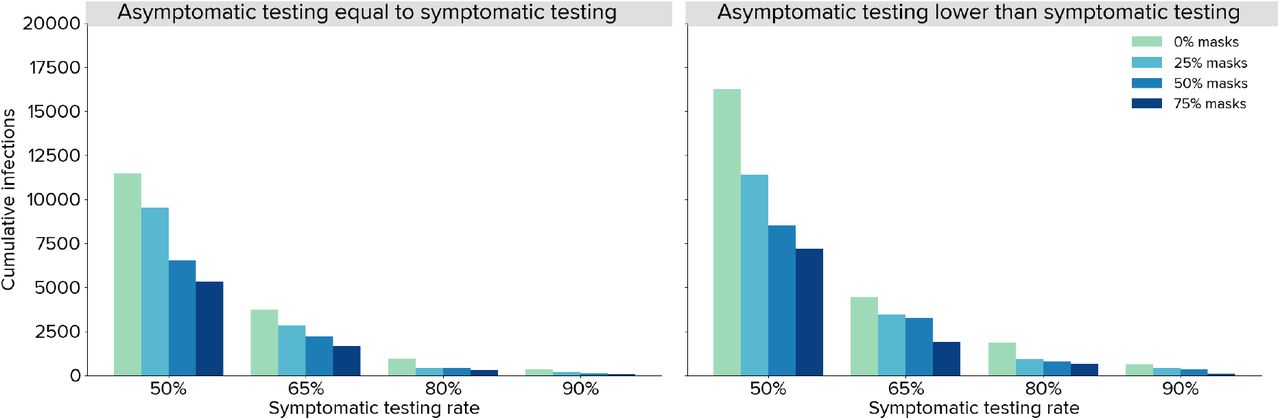
If asymptomatic contacts only test at half the rate of people with symptoms, we estimate a more severe epidemic over the last quarter of 2020. In Figure 3 we highlight a particular set of scenarios corresponding to the most optimistic contact tracing assumptions, in which all community contacts are assumed to be traced within one week, with a mean time to trace of one day (the full set of scenarios are summarised in Figure S2). Within this set of scenarios, the total number of infections is estimated to be around 50% higher if asymptomatic contacts test at a lower rate than people with symptoms (averaged across all levels of mask usage).
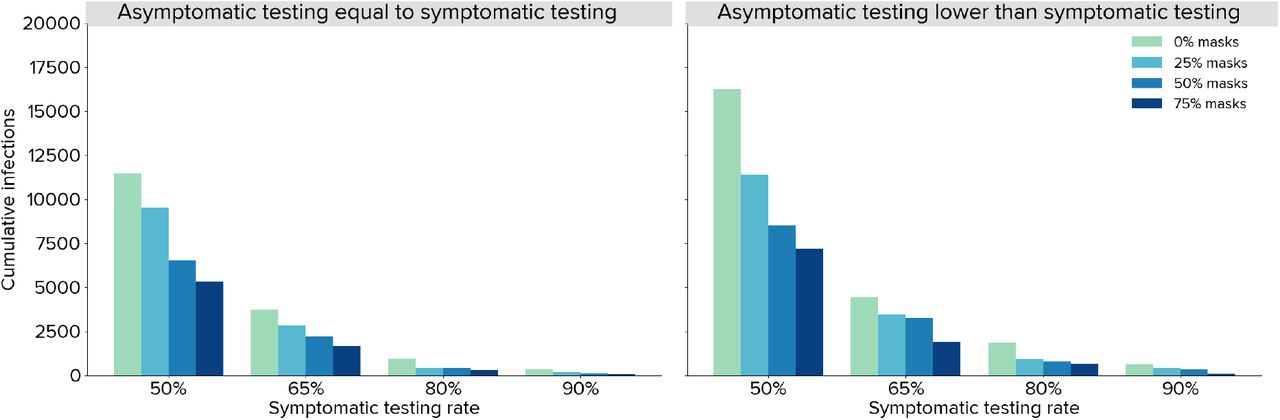
Estimated total infections over October 1 – December 31, 2020 under different assumptions about testing rates and mask uptake, assuming all community contacts can be traced within a week with a mean time to trace of 1 day. Projections represent the median of 20 simulations.
Discussion
In this work we present estimates illustrating the extent to which masks, community testing, and community contact tracing can reduce the spread of SARS-CoV-2 in New South Wales, Australia. We found that the relative impact of masks is greatest when testing and tracing rates are lower (and vice versa). With very high testing rates (90% of people with symptoms, plus 90% of people with a known history of contact with a confirmed case), we estimate that the epidemic in New South Wales would remain under control until at least the end of 2020, provided that fast and effective contact tracing is in place. If testing rates are lower, we estimate that mask use can play an important role in reducing the potential for epidemic resurgence.
Of the interventions considered, this study suggests that maintaining high levels of symptomatic testing, contact tracing, and testing of contacts is the most important. Longer term, there may be challenges associated with maintaining high levels of testing, mask use, and contact tracing. If daily case numbers remain low and the perceived threat of COVID-19 declines, community fatigue may influence testing behaviours, particularly for mild cases of COVID-19. There may also be a decline in mask use. Individuals may become less compliant with sign-in procedures, and venues may also become less vigilant in enforcing these procedures. This study suggests that having high levels of any two of mask use, testing and contact tracing can partly mitigate the need for the third; however practical challenges mean that this is unlikely to occur, and a more multifaceted approach of aiming for high coverage of all three and ending up with moderate coverage of all three may be an effective and more robust strategy.
Although various efforts have been made to synthesise the ever-expanding body of research regarding the efficacy of different interventions, each country’s epidemic has distinct characteristics, and there are very few standardised, globally-applicable guidelines on what constitutes a best-practice public health strategy. As a result, jurisdictions have taken diverse approaches in terms of which interventions to prioritise, from a list that includes physical distancing, travel restrictions, wearing of masks or face coverings, isolation and/or testing of those with COVID-like symptoms, isolation of those who test positive, and tracing the contacts of confirmed cases for testing and/or quarantining. Although it may not always be articulated as such, numerous trade-offs are being made between different policy options in an attempt to allow the highest degree of societal activity commensurate with epidemic control. In New South Wales, mask use has been encouraged in particular settings since July, but not mandated; at the same time, there has been a strong focus on contact tracing. The results from this work suggest that the prioritisation of contact tracing may mitigate the relative importance of masks to some extent, but that this relies on continued high levels of community testing.
There are several limitations to this study. Firstly, the mathematical model that we use requires data on various aspects of SARS-CoV-2 transmission and prevention that are still not known exactly, including the effects of masks on preventing individual transmission and the proportion of infections that are asymptomatic. Whilst we have used the best available data and sampled from appropriate distributions where possible, this represents a source of uncertainty in all mathematical models of COVID-19. Secondly, we have constructed sets of scenarios that examine various combinations of parameters on mask uptake, contact tracing, testing of people with symptoms, and asymptomatic contact testing, but there are many more parameters that determine the dynamics of transmission, including the stringency of border control measures, people’s adherence to quarantine and isolation policies, and the effect of ongoing distancing policies. Changes to any of these policies would affect the results presented here in ways that are not straightforward to predict or extrapolate. Third, we have not considered any outbreak risk associated with newly seeded cases in the community that may arise from international or interstate arrivals. Finally, the model used here does not contain a geospatial component, and we have not considered heterogeneities in incidence, behaviour, or contact patterns across different parts of the state in these analyses. This could be relevant for questions around mask uptake, as uptake of masks is generally higher in more densely populated areas, so using a state-wide average for the proportion of the population wearing masks may underestimate their impact, especially since >90% of infections in NSW to date have occurred in the Sydney metropolitan area.
Conclusions
Our work suggests that testing, tracing and masks can be effective means of controlling transmission in dynamic community settings, and higher compliance with one can offset lower compliance with the other to some extent. However, pursuing a strategy that combines aggressive testing, high mask usage, and effective contact tracing, alongside continued hygiene and distancing protocols, is likely to be the most robust means of controlling community-based transmission of SARS-CoV-2.
Data Availability
All code and data analysed during this study are available in https://github.com/optimamodel/covid_nsw
Supplementary materials
Declarations
Competing interests statement
The authors declare that they have no competing interests.
Data sharing statement
All code and data analysed during this study are available in https://github.com/optimamodel/covid_nsw.
Funding
Australian NHMRC. RA, MH, and NS provide guidance to the Victorian Government’s COVID-19 response.
Authors’ contributions
RMS wrote the manuscript and produced the results. The model parameters and calibration were agreed upon by RMS, RA, NS, and RG. The scenarios and analyses were agreed upon by NS, MH, and RMS. CK, RMS, RA, DM, and DJK led development of the model (along with numerous other contributors listed below).
Supplementary materials

Assumed distribution of times required to find community contacts.
Effects of policies on transmission risk in New South Wales

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trailing 14-day average of daily new infections under different assumptions about the testing rate (rows), proportion of community contacts that can be traced within one week (columns), and mask uptake (line colours). Projections represent the median of 20 simulations. Text boxes in each panel displays the cumulative number of infections over October 1 – December 31, 2020.
Acknowledgements
We thank all contributors to the Covasim model, including at the Institute for Disease Modeling, including Brittany Hagedorn, Katherine Rosenfeld, Prashanth Selvaraj, Rafael Nunez, Gregory Hart, Carrie Bennette, Marita Zimmermann, Assaf Oron, Dennis Chao, Michael Famulare, Lauren George; at GitHub, including Michal Jastrzebski, Will Fitzgerald, Cory Gwin, Julian Nadeau, Hamel Husain, Rasmus Wriedt Larsen, Aditya Sharad, and Oege de Moor; at Microsoft, including William Chen, Scott Ayers, and Rolf Harms; and at the Burnet Institute, including Anna Palmer, Dominic Delport, and Sherrie Kelly. This work benefited from a useful discussion with James Wood, Deborah Cromer, and John Kaldor of the University of NSW, Australia.
References
Supplementary references
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.



