
ABSTRACT
Introduction In Latin America, Peru is the most impacted country due to COVID-19 pandemic. Given the authorized nationwide use of hydroxychloroquine, azithromycin, ivermectin and dexamethasone in COVID-19 patients, we aimed to evaluate their effectiveness alone or combined to prevent 30-day mortality among COVID-19 hospitalized patients without life-threatening illness.
Methods Design. Retrospective cohort study using digital clinical records to emulate a target trial. Setting. Nationwide data of mid- and high-level complexity hospitals from the Peruvian Social Health Insurance (EsSalud) between April 1 and July 19, 2020. Participants. Patients aged 18 years with confirmed SARS-CoV-2 infection by PCR, and non-severe pneumonia at admission. Interventions. We compared five treatment groups to the standard of care treatment regimen (control group) within 48 hours of admission to hospital: hydroxychloroquine/chloroquine alone (HCQ), ivermectin alone (IVM), azithromycin alone (AZIT), HCQ + AZIT group, and IVM + AZIT group with doses recommended by the Peruvian Ministry of Health. Main outcomes measures. The primary outcome was all-cause mortality rate, the secondary outcomes were survival without ICU rate, and survival without oxygen prescription rate. Analyses were adjusted for confounding factors by inverse probability of treatment weighting. A doubly-adjustment method was done for sensitivity analysis.
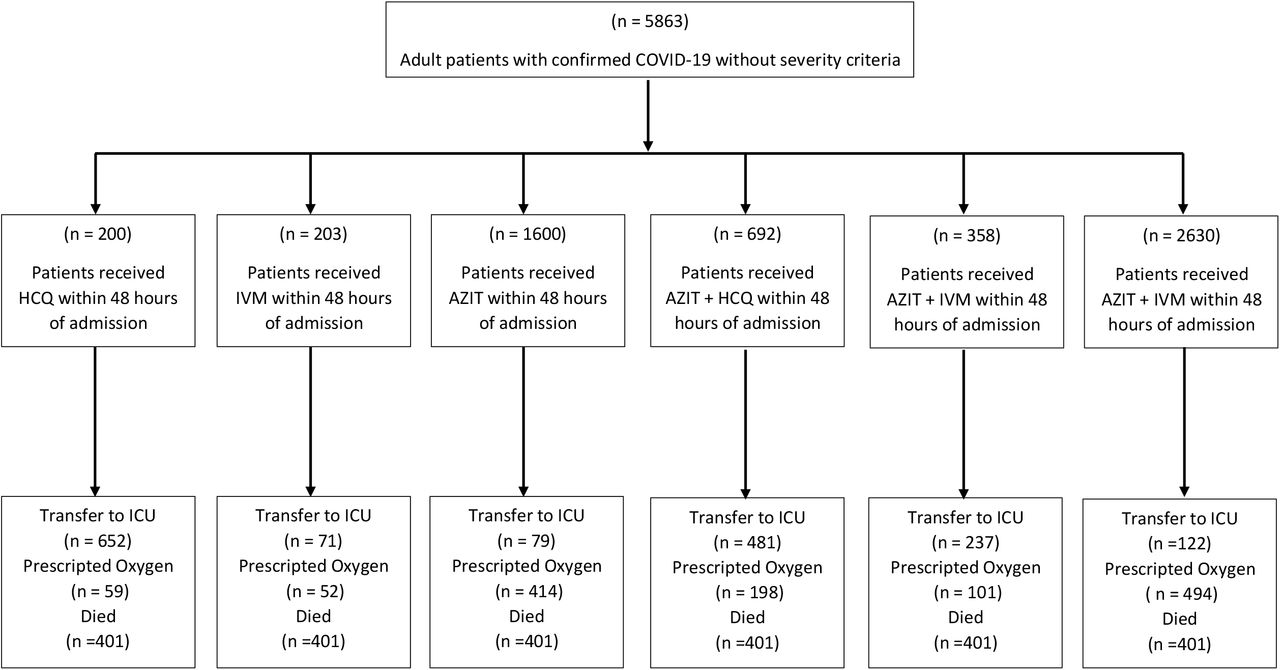
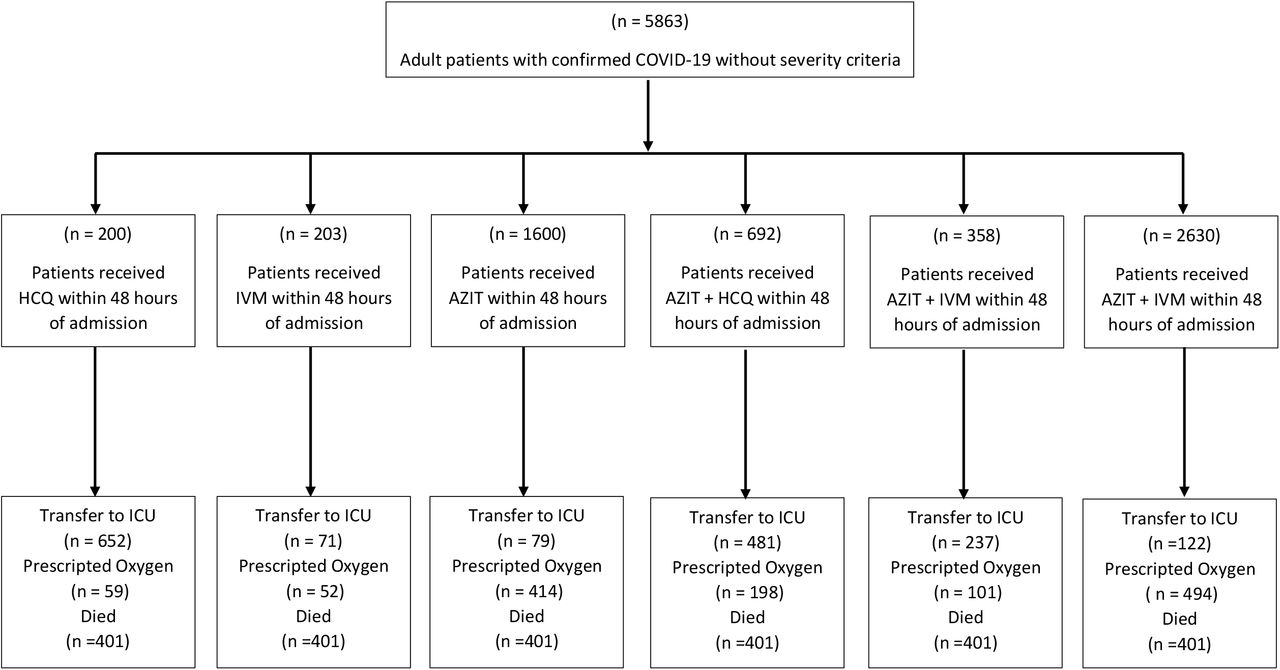
Results Among 5683 patients eligible for analysis, 200 received hydroxychloroquine or chloroquine within 48 hours of hospital admission, 203 received ivermectin, 1600 received azithromycin, 692 received hydroxychloroquine or chloroquine plus azithromycin, 358 received ivermectin plus azithromycin and 2630 received standard of care. AZIT + HCQ group was associated with 84% higher all-cause mortality hazard rate compared to standard care (wHR = 1.84, 95% CI: 1.12-3.02). Consistently, AZIT + HCQ treatment was associated with survival without transfer to ICU (wHR = 1.49, 95% CI: 1.01-2.19) and survival without oxygen prescription (wHR = 1.70, 95% CI: 1.07-2.69). HCQ treatment was associated with 77% higher all-cause mortality or oxygen prescription hazard rate compared to standard treatment (wHR = 1.77, 95% CI: 1.01-3.11). Surprisingly, we observed that IVM treatment was associated with less survival rate without transfer to ICU in the weighted analysis (wHR = 1.58, 95% CI:1.11-2.25) By last, we did not find evidence of effect on reduce all-cause mortality or increase survival rate without transfer to ICU or survival rate without oxygen prescription for AZIT group neither AZIT + IVM group in all analyses.
Conclusion The results of our target trial emulation match with previous findings of randomized clinical trials and observational studies, which showed no beneficial effects of hydroxychloroquine, ivermectin, azithromycin, or their combinations.
INTRODUCTION
The Coronavirus disease 2019 (COVID-19) imposed a major global challenge given its rapid transmission worldwide and high mortality among other causes (1, 2). To aggravate the current emergency situation, there is no specific pharmacological treatment that has proven being effective in controlling the SARS-CoV-2 infection or improving clinical outcomes (3). Traditionally, any specific drugs to treat the infection might take several years to develop. However, given the rapid spread of the COVID-19 pandemic, and with no available alternatives against the SARS-CoV-2 virus, several existing drugs were repurposed based on in vitro studies or low-quality evidence. Consequently, there has been extensive efforts on investigating the efficacy and effectiveness of several pharmacological treatments using randomized clinical trials as well as observational studies (4).
Currently, only dexamethasone has shown to reduce all-cause mortality and the need of mechanical ventilation; while remdesivir seems to reduce symptoms duration and occurrence of severe adverse events (5). On the other hand, some emergently repurposed treatments have consistently demonstrated no benefits on all-cause mortality, including hydroxychloroquine with or without azithromycin, lopinavir-ritonavir, and convalescent plasma (5). Ivermectin has only demonstrated efficacy in laboratory conditions, but not evidence has yet reported on hospitalized patients with COVID-19 (6). Most studies tested the efficacy and effectiveness in hospitalized patients to prevent all-cause mortality, serious adverse events, admission to intensive care, need of mechanical ventilation, and receipt of renal replacement therapy; however, many of these studies had limitations that render the evidence low-quality. Despite this, these drugs continue to being used in different health systems worldwide, and some of them have even been tested for pre-exposure prophylaxis among healthcare professional finding the same unsuccessful results (7).
Peru has suffered greatly with the pandemic, being the sixth country by total number of cases worldwide and the top one regarding mortality (828,169 cases and 101.94 deaths per 100,000 inhabitants respectively by 10/05/2020) (8, 9). The urgent need to address this national crisis, drove the Peruvian Ministry of Health to authorize the use of hydroxychloroquine with or without azithromycin, oral ivermectin alone or in combination with the other drugs (10, 11). Given the permitted clinical prescription in hospitalized patients, and the implementation of electronic clinical records nationwide for all COVID-19 patients treated in the Peruvian Social Security Health System, we intended to efficiently use this real-world data through target trials to make robust causal analysis emulating a randomized controlled clinical trial (12, 13). In this way, the biases traditionally associated with observational studies might be minimized, and more realistic estimates of effectiveness could be obtained (14). Moreover, we intend to use novel techniques involving machine learning algorithms to improve our propensity score models. Thus, our study aimed to evaluate the effectiveness of hydroxychloroquine, azithromycin, and ivermectin alone or combined, to prevent 30-day mortality in COVID-19 hospitalized patients but without life-threatening illness. Additionally, as secondary goals, we evaluated two composite outcomes, survival without intense care unit (ICU) transfer, and survival without oxygen prescription.
METHODS
Study design and population
We conducted a retrospective cohort study that analyzed data obtained from routine care through electronic health records (EHR) of patients hospitalized with COVID-19 in mid- and high-level complexity hospitals belonging to the Peruvian Social Security Health System (EsSalud). We attempted to emulate a target trial to obtain robust estimates of clinical effectiveness for hydroxychloroquine/chloroquine, azithromycin, ivermectin, alone or combined, on relevant clinical outcomes (12, 15). We retrieved anonymized data of COVID-19 patients, as defined by the Pan-American Health Organization (16), from the EHRs stored in the EsSalud information system central using the International Classification of Disease Tenth Revision (ICD-10) codes (17).
We included patients admitted between April 1 and July 19, 2020 with the following criteria: 18 years old or above; confirmed SARS-CoV-2 infection by PCR; clinical manifestations compatible with non-severe disease at admission (no need of oxygen, no acute respiratory failure diagnosis, no systemic inflammatory response syndrome, no sepsis or septic shock, no acute respiratory distress syndrome [ARDS], no acute pulmonary edema, no disseminated intravascular coagulation [DIC]). We excluded patients with any of these criteria: self-reported pregnancy at admission; discharge, ICU admission or death within 24 hours of admission; received other experimental drugs (tocilizumab, lopinavir-ritonavir or remdesivir) within 48 hours of admission; self-reported treatment of hydroxychloroquine for rheumatological diseases.
Treatment strategies
We compared five treatment groups to the standard of care treatment regimen, as a control group. The treatment groups were defined as follows: hydroxychloroquine/chloroquine alone (HCQ group), ivermectin alone (IVM group), azithromycin alone (AZIT group), hydroxychloroquine/chloroquine plus azithromycin (HCQ + AZIT group), and ivermectin plus azithromycin (IVM + AZIT group) at doses recommended by the Peruvian Ministry of Health (10, 11). The standard of care was defined as a treatment regimen of antipyretics, hydration, and basic supportive care, and oxygen saturation monitorization. The decision to administer one of these treatment groups depended on clinician’s own criteria guided by the Ministry of Health recommendations, which was changing over time according to updated evidence-based reviews (10, 11). Thus, there was an expected heterogeneity of administered treatment to patients across different hospitals, services, and even month of hospitalization.
We allowed a grace period of 48 hours to initiate therapy in order to assess a more realistic clinical question: what is the effectiveness of initiating therapy within 48 hours of hospitalization compared to only receiving standard care within 48 hours of hospitalization? Hence, patients who received any of the treatment regimens after 48 hours of hospitalization were assigned to the control group. Although this approach is similar to an intention-to-treat analysis, the 48 hours period of grace allow us to estimate a per protocol effect as a causal contrast of interest. As mentioned before, patients who developed any of the outcomes within 24 hours of admission were excluded. However, the patients who developed the outcome after 24 hours but before being assigned to a group during the grace period (48 hours) were still included. Because these patients could have potentially been assigned to any group, they were randomly distributed between the control and treatment groups to avoid time-dependent bias due to inappropriate exclusion or treatment assignment (12).
Start, end of follow-up and outcomes
The onset of follow-up, defined as the time zero, for each patient was the date of hospitalization. The end of the follow-up was the date of occurrence of any outcome (death, death and/or transfer to ICU, death and/or oxygen prescription), discharge, or end of follow-up by July 19, 2020. The primary outcome was all-cause mortality rate, and the secondary outcomes were survival without ICU rate, and survival without oxygen prescription rate.
Strategy for emulating random assignment
To emulate the random assignment of a target trial, we used a propensity score weighting for multivalued treatments employing a machine-learning approach to calculate balanced differences on the baseline covariates for the control and treatment groups (18, 19). Propensity scores are an estimate of the probability of receiving a certain treatment given their baseline or pre-treatment characteristics (20). Assuming positivity and no unmeasured confounder, instead of matching pairs of patients, the propensity score can be used to weight in a transformation of the values, allowing causal effect estimations (20). In order to estimate propensity scores for treatment assignment, we used generalized boosting models (GBM) (15, 21). This machine-learning algorithm iteratively fits classification trees using large and non-parsimonious number of pre-treatment covariates. This non-parametric approach improves traditional logistic regression for propensity score estimation (22) because it minimizes bias from model misspecification commonly obtained by incorrect parametric model assumptions (23) and works well with missing data (22). Furthermore, GBMs automatically determine which baseline covariates, and which of their interactions, should be included in the model. Thus, we trained iteratively 5000 classification trees as maximum, setting the following parameters: shrinkage factor of 0.01, allowing for testing and inclusion of all interactions between three and two covariates, and a bag fraction of one (24). We chose minimization of the standardized mean effect as the stop method to achieve optimal balance. To estimate the average treatment effect on treated subjects (ATET), propensity score weights (PSW) were generated using the standardized treatment assignment ratio weighting (25, 26). This method sets the PSW to 1 for control group (standard of care) and calculates the PSW for treatment groups using the odds in the reference groups (PSW = propensity score/(1-propensity score)) (26).
All the variables included in the propensity score model were selected based on expert’s opinion before the analysis. In addition, we selected pre-treatment covariates which could be confounders or prognostically relevant (18). We did not include baseline variables theoretically associated with treatment assignment, but not with outcome, to avoid power reduction and/or bias amplification (18, 27). The baseline covariates included were: age; sex; month of admission; location of the health center (Capital, North, South, Center, Rainforest); Charlson’s index at hospital admission; comorbidities known in the first 48 hours (myocardial infarct/chronic heart failure/peripheral vascular disease; chronic lung disease; mild/severe liver disease; uncomplicated/complicated diabetes mellitus; cancer, stroke/dementia/paralysis; chronic kidney disease; metabolic disease; peptic ulcer disease; HIV; and uncomplicated/complicated hypertension); emergency care before hospital admission; antibiotics (other than azithromycin) used within 48 hours of admission; previous use of angiotensin-converting enzyme inhibitors/angiotensin-II receptor antagonists; and pneumonia diagnosed within 48 hours of admission. We assessed the overlap of propensity score distributions between the control group and each treatment group to verify the common support assumption. The balance was assessed using standardized mean differences for numerical covariates, and row differences for categorical variables. In all cases, we considered a threshold of 10% as indicative of meaningful imbalance (18). During balance optimization, we remained blinded to the outcome results of the study.
Statistical analysis
We reported baseline characteristics for the control and treatment groups using weighted Kaplan-Meier survival curves, and 30-days cumulative incidence with a binomial exact 95% confidence intervals (95% CI). We estimated unweighted (uHR) and propensity score weighted hazard ratios (wHR) using Cox proportional hazards regression to assess effectiveness. In order to control any residual confounding effect, we reported wHR with double adjustment after adding all the covariates of the propensity score to the Cox model. Finally, we performed a Bonferroni adjustment of p-values and 95% CI to compare treatment groups against control.
Ethics
This study was classified with minimal risk of vulnerability for participants. In order to maintain the privacy of the patients, the data extraction was anonymized by the EsSalud’s informatics office before data manipulation or analysis. This target trial protocol was approved by EsSalud’s Institutional Review Board of COVID studies (91-SGRyGIS-DIS-IETSI-ESSALUD-2020) and was also registered in the Peruvian Health Research Projects repository (PRISA, by its acronym in Spanish) with ID EI-1243 (28).
RESULTS
Among 5683 patients eligible for analysis, 200 received hydroxychloroquine or chloroquine within 48 hours of hospital admission, 203 received ivermectin, 1600 received azithromycin, 692 received hydroxychloroquine or chloroquine plus azithromycin, 358 received ivermectin plus azithromycin and 2630 received standard of care (none of the antimicrobials mentioned) (SM Figure 1). Age ranged between 18 and 104 years old with a mean of 59.4 years old (SD = 16.3 years old) and 36.8% (n = 2091) of the participants were women. Table 1 describes the baseline characteristics of the study population.
Baseline characteristics of patients with COVID-19 assigned to one of the treatment groups (HCQ, IVM, AZIT+HCQ and AZIT+IVM) or standard care (control group)
Propensity score model development
Propensity scores showed well overlapping between treatment groups versus control group with well overlapping (>95%) in the region of common support (SM Figure 1). Before inverse probability of treatment weighting, we observed >8 of 30 baseline covariates with high disbalance (> 10% standardized mean difference). After we applied inverse probability of treatment weighting, only 1 of the 30 baseline covariates (age) had imbalance (>10% standardized mean difference) and the remain 39 baseline covariates showed weighted standardized differences below 10% (Figure 2).

Follow-up and outcomes
The median of follow-up for overall survival was 7 days (9 days for HCQ group, 8 days for IVM group, 8 days for AZIT group, 9 days for AZIT + HCQ group and 8 days for AZIT + IVM group). At final of follow-up, 1072 of 5683 (18.9%) patients had died (49 [15.3%] in HCQ group, 47 [24.5%] in IVM group, 325 [23.2%] in AZIT group, 165 [23.5%] in AZIT + HCQ group and 85 [23.5%] in AZIT + IVM group. Figure 3 shows weighted KM survival curves for the main outcome. SM Figure 2 and SM Figure 3 shows weighted KM survival curves for the secondary outcomes: survival without transfer to ICU and survival without oxygen prescription, respectively.

{kind=link}
{kind=link}
{kind=link}
In the non-weighted analyses, among the 5683 patients in the six treatment groups, the AZIT + IVM treatment was associated with 40% higher all-cause mortality hazard rate compared to standard care group (uHR = 1.40; 95% CI: 1.03-1.90). AZIT + IVQ treatment also was associated with a 39% higher mortality and/or oxygen prescription hazard rate compared with standard care (uHR = 1.39; 95% CI: 1.04-1.85). By last, IVM treatment also was associated with higher all-cause mortality hazard compared to standard care group (uHR = 1.57; 95% CI: 1.16-2.14),
After adjusting by potential confounding variables using the inverse probability weighting approach, we observed that AZIT + HCQ group was associated with 84% higher all-cause mortality hazard rate compared to standard care (wHR = 1.84, 95% CI: 1.12-3.02). Consistently, AZIT + HCQ treatment was consistently associated with the two secondary outcomes: survival without transfer to ICU (wHR = 1.49, 95% CI: 1.01-2.19) and survival without oxygen prescription (wHR = 1.70, 95% CI: 1.07-2.69). Except for survival without transfer to ICU, these results were consistent even after doing double-robust adjustment to reduce residual confounding in the sensibility analysis (see SM Table 1).
Although we found inconsistent results regarding the estimated effect of HCQ on primary and secondary outcomes, overall, we found results compatible with no effect or even a harmful effect of increasing the risk of the study outcomes. Thus, the weighted analysis showed that HCQ treatment was associated with 77% higher all-cause mortality or oxygen prescription hazard rate compared to standard treatment (wHR = 1.77, 95% CI: 1.01-3.11). The double-robust adjustment sensitivity analysis showed that HCQ treatment was associated with until 2 times higher all-mortality hazard rates (drwHR = 2.08, 95% CI: 1.12-3.86) and all-mortality or oxygen prescription hazard rate (drwHR = 2.13, 95% CI: 1.20-3.77) compared to standard care. In this sensitivity analysis, we also observed that HCQ group was also associated to higher all-cause mortality or transfer to ICU hazard rate compared to the control group (drwHR = 1.69, 95% CI: 1.04-2.76).
Surprisingly, we observed that IVM treatment was associated with less survival rate without transfer to ICU in the weighted analysis (wHR = 1.58, 95% CI:1.11-2.25) and this result persists similar in the sensibility analysis that used double robust adjustment (drwHR = 1.60, 95% CI: 1.12-2.27). By the other hand, we did not find evidence of effect on reduce all-cause mortality or increase survival rate without transfer to ICU or survival rate without oxygen prescription for AZIT group neither AZIT + IVM group in all weighted and double-adjusted weighted analyses (see Table 2).
Primary and secondary outcomes in patients with COVID-19 assigned to treatment groups or standard care (control group)
DISCUSSION
This is the first study in Latin America, a region widely impacted by the pandemic, emulating a clinical trial based on observational data comparing different drug treatments for COVID-19. Using a database based on thousands of electronic clinical records, it was possible to replicate conditions of a clinical trial for several drugs prescribed during the pandemic. The electronic clinical records were fully implemented by the Peruvian Social Health Insurance in response to the COVID-19 emergency, yielding a unique opportunity to analyze big data under real-world conditions. This study also employed novel statistical tools to emulate adequate randomization of the patients. Not only a propensity score weighting was used to balance the control and intervention groups according to the probability of having been prescribed a certain drug, but the regression itself employed generalized boosted models based on repeated decision trees. The resulting models for our main outcome, death, and two secondary outcomes, survival without ICU and survival without oxygen requirement, showed no benefit from any of the treatment arms compared with standard care. There was even a consistent increase of risk developing the outcome with the hydroxychloroquine and azithromycin combination.
Azithromycin
Our study showed no effect of azithromycin alone over mortality, survival without ICU, and survival without oxygen requirement. Few published studies have compared azithromycin alone versus standard of care free of hydroxychloroquine or ivermectin. Albani et al in Italy followed a cohort of 1403 patients either receiving azithromycin alone, HCQ alone, the combination of both, or none of them. Using propensity score weighting, they found that azithromycin alone was associated with lower mortality (OR 0.60, 95%CI 0.42-0.85) compared to no treatment. Guerin et al in France (29) compared 34 patients on azithromycin alone with no treatment, finding reduction in days to achieve clinical recovery (12.9 vs 25.8, p=0.015). On the other hand, Geleris et al (30) analyzed a large single-center cohort in NYC using propensity score matching to evaluate HCQ, but also assessed azithromycin alone vs standard of care, finding no benefit for the end point of death and/or ICU transfer (HR 1.03, 95%CI 0.81-1.31). Arshad et al (31) also evaluated azithromycin alone as a secondary aim in their multicenter, retrospective, propensity score matched observational study in USA, finding no effect (HR 1.05, 95%CI 0.68-1.62). Rodiguez-Molinero et al in Spain followed a cohort of 239 patients treated with azithromycin alone (32). They were able to match 29 patients on azithromycin alone with an equal number of controls using multiple clinical and prognosis factors. They found no difference in oxygen saturation/fraction of oxygen at 48h, and a longer time to discharge in the azithromycin group. When using the unmatched whole cohort, they found no difference in any of these outcomes. In summary, the available evidence is still contradictory and mainly based on observational designs.
Hydroxychloroquine alone
We found a slight increase of risk for death and/or oxygen requirement, but not for our primary outcome (death), or for death and/or ICU transfer. This is consistent with the systematic review published by Fiolet et al (33) including 29 articles: three RCTs, one non-randomized trial, and 25 observational studies. They included 11932 patients on the HCQ alone group, 8081 on the HCQ/azithromycin group, and 12930 on the control group. They found no association of HCQ alone with mortality with a pooled relative risk (RR) of 0.83 (95%CI 0.65-1.06) for all 17 studies and RR of 1.09 (95%CI 0.97-1.24) for the three randomized controlled trials. Among these studies, the New England Journal paper by Geleris et al (30), after using propensity score matching, found no significant association between hydroxychloroquine use and intubation or death (HR 1.04, 95%CI 0.82-1.32). Results were similar in multiple sensitivity analyses
Hydroxychloroquine / azithromycin combination
Noticeably, we found a consistent increase on the risk for the three outcomes among the patients who received the HCQ/azithromycin combination compared with standard of care. Similarly, the previously mentioned systematic review by Fiolet et al (33) found that HCQ/azithromycin was associated with an increased mortality (RR = 1.27; 95% CI 1.04-1.54) for six observational studies plus a RCT. Two other observational studies not included in the previous systematic review, found no benefit in mortality. A Brazilian randomized clinical trial, 447 patients, showed no improvement of clinical outcomes with the use of azithromycin in addition to standard of care that included hydroxychloroquine (OR 1.36, 95%CI 0.94-1.97) in patients with severe COVID-19 (34). An open-label controlled trial in Iran compared 55 patients on HCQ plus lopinavir with 56 patients who received azithromycin on top of that regimen, finding no difference in mortality (35). However, there are at least two big observational studies, which found a beneficial effect of the combination on mortality. Arshad et al in the Henry Ford Health system followed observationally 2561 patients. They found a 66% HR reduction with HCQW and 71% with the HCQ/azithromycin combination (31). Lauriola et al in Italy reported an observational study with 377 consecutive patients and measured in-hospital death. They found a reduce in-hospital mortality with the HCQ/azithromycin combination (HR 0.265, 95%CI 0.17-0.41) (36). Therefore, it is still not clear which is the real effect of the combination based on the published data; however, there is a physio-pathological plausibility that the combination increased cardiac adverse events, affecting survival negatively (37).
Ivermectin
Until the date of this manuscript, there are no published clinical trials or large observational studies analyzing the effect of ivermectin on patients hospitalized with COVID-19. We found no association of ivermectin with all-cause mortality or with death and/or oxygen requirement; however, a deleterious effect was found on death and/or ICU admission. The reason of this association is not immediately clear for us, given the no-effect on the other two outcomes. One possibility is the presence of residual confounding despite the propensity score matching and further model adjustments. We only found pre-printed observational studies evaluating the effectiveness of this drug. The largest series is the ICON study done in Florida, USA (38). They compared 173 patient on ivermectin versus 107 under usual care without employing any matching or weighting. They found less mortality in the ivermectin group (OR 0.52, 95%CI 0.29-0.96) and even greater effect on the subgroup with severe pulmonary disease (OR 0.15, 95%CI 0.05-0.47). A pilot study in Iraq compared 71 patients receiving HCQ/azithromycin with 16 patients receiving a single oral dose of ivermectin on top (39). They found no difference on mortality (2/71 vs 0/16), but less hospitalization time in days (13.2±0.9 vs 7.6±2.8, p<0.001). Finally, there is a descriptive study in Argentina with 167 patients and no control group. They evaluated a treatment protocol that includes ivermectin, and reported an overall mortality of 0.59%, lower than their country average (40). Therefore, our study is the largest series assessing the effect of ivermectin among hospitalized patients and employing an adequate comparison between groups.
Conclusion
In conclusion, this is the first clinical trial emulation done in Latin America for COVID-19, and so far, the largest performed using an appropriate method to balance groups. Different from observational studies, a clinical trial emulation allows for robust models, which minimize bias of treatment assignment, yielding reliable results. However, equilibrating control and intervention groups is no easy task, since the most common methods have disadvantages as sample size reduction (matching) or poor overlapping (weighting). The use of machine learning algorithms based on iterative decision tress offers an excellent opportunity to optimize the balance between groups, maintaining stable models. Besides, the use of large observational data provides enough power to compare different treatment arms simultaneously, does not require the logistics of a randomized clinical trial, and approximates treatment efficacy under real-world conditions.
The results of this clinical trial emulation match with previous findings of randomized clinical trials and observational studies, which showed no beneficial effects of hydroxychloroquine, ivermectin, azithromycin, or their combinations. Once assignation bias and possible confounders are controlled, the effect of the pharmacological treatments studied is not significant, implying that any effect perceived in observational studies and case series is probably due to confounding effect and selection bias. We even detected a consistent increase in death risk, as well as transfer to ICU and oxygen requirement, with the hydroxychloroquine-azithromycin combination. This association has been reported in other studies and clinical trials, corroborating a potentially harmful effect of this combination. However, we did not have an adequate registry of pharmacological side effects in our electronic database, to suggest adverse reactions as the path for mortality increases.
Data Availability
The data supporting the findings of this study are available in the IETSI EsSalud computer files, but restrictions apply to the availability of these data, which were used under the current study license and are therefore not publicly available. However, the data are available to the authors upon reasonable request and with the permission of IETSI EsSalud.
Acknowledgments
We thank Engr. Pedro Vasquez, Engr. Elard Pastor and all the team from the Gerencia Central de Tecnologías de lnformación y Comunicaciones – GCTIC for their collaboration extracting and structuring the data from the electronic medical records.
Footnotes
Financial statement: This study was funded by the Instituto de Evaluación de Tecnologías en Salud e Investigación – IETSI, EsSalud – Peru.
Conflicts of interest: The authors declare no conflicts of interest regarding the subject of this scientific article.
References



