
ABSTRACT
{kind=link}
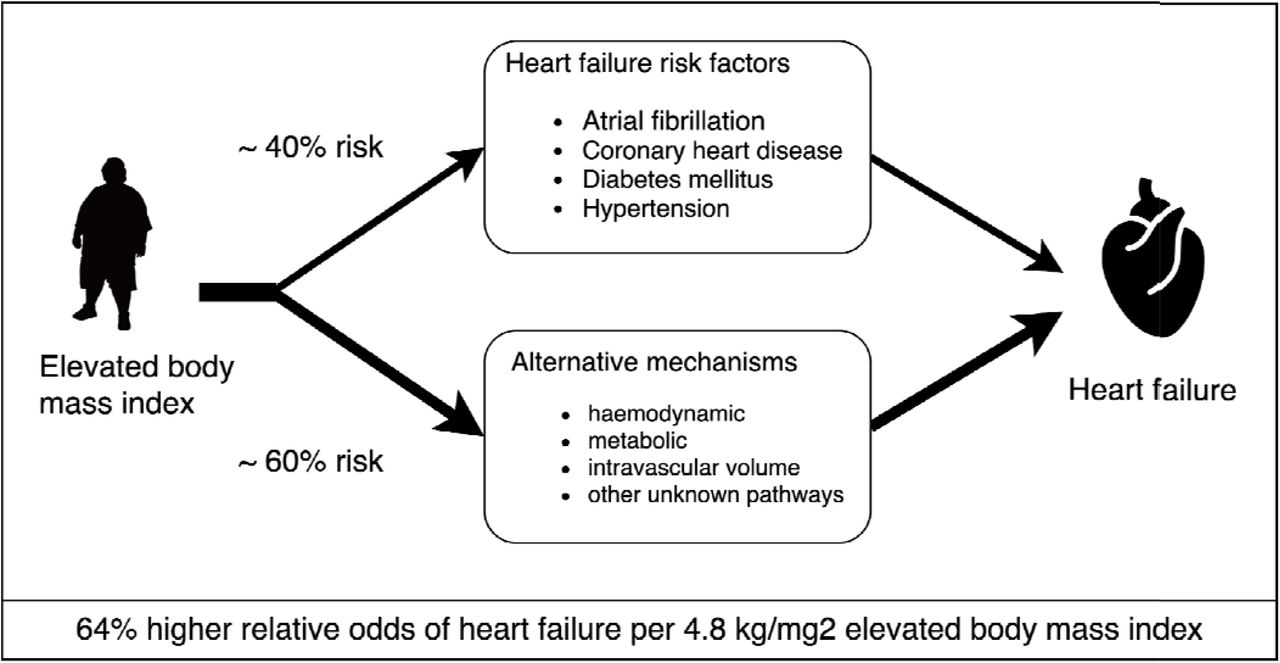
Aims Elevated body mass index (BMI) is a known risk factor for heart failure (HF), however, the underlying mechanisms are incompletely understood. The aim of this study was to investigate the role of common HF risk factors as potential mediators.
Methods and Results Electronic health record data from primary care, hospital admissions and death registrations in England were used to perform an observational analysis. Data for 1.5 million individuals aged ≥18 years, with BMI measurements and free from heart failure at baseline, were included between 1998 and 2016. Cox models were used to estimate the association between BMI and HF with and without adjustment for atrial fibrillation (AF), diabetes mellitus (DM), coronary heart disease (CHD), and hypertension (HTN). Univariable and multivariable two-sample Mendelian randomisation was performed to estimate causal effects.
Among non-underweight individuals, BMI was positively associated with HF with a 1-SD (∼ 4.8kg/m2) higher BMI associated with a hazard ratio (HR) of 1.31 (1.30, 1.32). Genetically predicted BMI yielded a causal odds ratio (OR) of 1.64 per 4.8 kg/m2 BMI (1.58, 1.70) which attenuated by 41% (to OR of 1.38 (95% CI 1.31-1.45), when simultaneously accounting for AF, DM, CHD and SBP.
Conclusion About 40% of the excess risk of HF due to adiposity is driven by SBP, AF, DM and CHD. These findings highlight the importance of the prevention and treatment of excess adiposity and downstream HF risk factors to prevent HF, even in people in whom the above risk factors are well managed.
One-sentence summary This study of the role of excess adiposity as a risk factor for HF, including an observational analysis of measured BMI 1.5 million individuals and multivariable MR analysis of genetically elevated BMI, provides evidence that adiposity is causally associated with HF, with approximately 40% of the effect being mediated by conventional risk pathways.
Competing Interest Statement
Dr Holmes has collaborated with Boehringer Ingelheim in research and in adherence to the University of Oxfords Clinical Trial Service Unit and Epidemiological Studies Unit (CSTU) staff policy, did not accept personal honoraria or other payments from pharmaceutical companies.
Funding Statement
This work was funded, in part, by grants from the National Institute for Health Research, University College London Hospitals Biomedical Research Centre and BigData@Heart Consortium funded by the Innovative Medicines Initiative-2 Joint Undertaking under grant agreement No. 116074. Dr Lumbers is supported by a UK Research and Innovation Rutherford Fellowship hosted by Health Data Research UK (MR/S003754/1. Dr Katsoulis is funded by the British Heart Foundation (grant: FS/18/5/33319). Dr Holmes works in a unit that receives funding from the UK Medical Research Council and is supported by a British Heart Foundation Intermediate Clinical Research Fellowship (FS/18/23/33512) and the National Institute for Health Research Oxford Biomedical Research Centre
Author Declarations
I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained.
Yes
The details of the IRB/oversight body that provided approval or exemption for the research described are given below:
ISAC approval: 18_010
All necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived.
Yes
I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance).
Yes
I have followed all appropriate research reporting guidelines and uploaded the relevant EQUATOR Network research reporting checklist(s) and other pertinent material as supplementary files, if applicable.
Yes
Data Availability
Data is not available



