
Abstract
In the United States, schools closed in March 2020 due to COVID-19 and have begun reopening as of August 2020, despite continuing transmission of SARS-CoV-2. To determine the impact of school reopening with varying levels of operating capacity and face-mask adherence, we used an agent-based model calibrated to and validated against multiple data types from the state of Indiana, USA. In our model, transmission can occur in schools, workplaces, community settings, and households, all of which are structured in a realistic way according to state geography and demography. Using this model, we quantified the burden of COVID-19 on K-12 students, teachers, their families, and the general population under alternative scenarios about school reopening. In our primary analysis, we considered three levels of school operating capacity (50%, 75%, and 100%) and three assumptions about face-mask adherence in schools (50%, 75%, and 100%). Under a scenario in which schools operate remotely, we projected 45,579 (95% CrI: 14,109-132,546) infections and 790 (95% CrI: 176-1680) deaths between August 24 and December 31. Reopening at 100% capacity with 50% face-mask adherence in schools resulted in a proportional increase of 42.9 (95% CrI: 41.3-44.3) times that number of infections and 9.2 (95% CrI: 8.9-9.5) times that number of deaths. In contrast, operating at 50% capacity with 100% face-mask adherence resulted in only an 11% (95% CrI: 5%-18%) increase in the number of infections compared to the scenario in which schools operate remotely. We conclude that reduced capacity and high face-mask adherence in schools substantially reduce the burden of COVID-19, both among those with direct ties to schools and across the state. As Indiana and other states proceed with school reopening, our results illustrate quantitatively the benefits of safety measures that schools are undertaking, underscoring their value for both schools and their communities.
1 Introduction
The United States has been the country most severely impacted by the COVID-19 pandemic in terms of total reported cases and deaths, with over 5.2 million cases and 167,000 deaths through August 14 [1]. This severity led to social interventions on an unprecedented scale, including restrictions on mass gatherings, bans on non-essential travel, and school closures [2, 3, 4, 5]. While such restrictions were initially successful in reducing transmission, the subsequent relaxation of restrictions on mass gatherings and movement were followed by large increases in notified cases and, more recently, deaths [1, 3, 6, 7]. The state of Indiana reported its highest daily number of cases to date (1,249) on August 6 [8].
It is within this context of intense community transmission that attention has turned to the reopening of schools for the start of the academic year in August [9, 10, 11]. During influenza epidemics, school closures have been estimated to reduce transmission community-wide [12, 13, 14]. In general, schools are seen as key drivers of the transmission of respiratory pathogens due to close contact among children at school [15, 16, 17]. However, several factors complicate the effect of school reopenings on SARS-CoV-2 transmission. In particular, children and adolescents appear less susceptible to infection and are much less likely to experience severe outcomes following infection [18, 19, 20, 21, 22, 23]. It is also still unclear what their contribution to transmission is, but several studies suggest they can play an important role [18, 24, 25, 26]. There are additional economic and social factors to consider, too, such as the economic costs of school closures for families that must then stay home from work, and the nutritional benefits of school reopening for children who rely on free and subsidized school meals [27, 28, 29].
Our objective in this study was to explore the impacts of strategies for school reopening on the burden of COVID-19 in the state of Indiana, USA. We synthesized evidence around features of COVID-19 epidemiology in children [19] in an agent-based model originally developed for pandemic influenza [30] that is equipped to translate such evidence into projections of community-wide transmission under alternative scenarios about school reopening. We focused on the role of reducing the capacity of classrooms and adherence to wearing face masks in schools, given that both physical distancing and face masks have been shown to reduce transmission of SARS-CoV-2 in community settings [31]. Our main outcome measures were changes in statewide totals of SARS-CoV-2 infections, symptomatic infections, and deaths, across different scenarios of school capacity and face-mask adherence, compared with a baseline scenario in which schools operate remotely.
2 Methods
Approach
Our approach to modeling SARS-CoV-2 transmission is based on the Framework for Reconstructing Epidemic Dynamics (FRED) model [30]. Using this model, we simulated the spread of SARS-CoV-2 in the population of Indiana, USA using a synthetic population with demographic and geographic characteristics of the population, including age, household composition, household location, and occupation [32]. We analyzed the impact of school reopening from August 24 (first day of classes in Marion County, the most populous) to December 31, 2020 in the overall population of Indiana, as well as in students, teachers, and their households. We quantified impact as the difference in the number of COVID-19 infections, symptomatic infections, and deaths, between each scenario and the baseline scenario.
Agent-based model
We chose an agent-based model for this analysis to address key issues such as heterogeneity of transmission within a population due to population density, age, occupation, and contact network. We used a synthetic population of Indiana to realistically represent characteristics of the population [32]. FRED simulates pathogen spread in a population by recreating interactions among people on a daily basis. Each human is modeled as an agent who visits a set of places defined by their activity space (houses, schools, workplaces, and neighborhood locations). Transmission can occur when an infected person visits the same location as a susceptible person on the same day, with numbers of contacts per person specific to each location type. For instance, school contacts depend not on the size of the school but on the age of the student. Every day of the week, students and teachers visit their school, and students are assigned to classrooms based on their age. Given that schools are closed during the weekends, community contact is increased by 50% [30]. For both schools and other locations, we adopted contact rates for each location type that were previously calibrated to attack rates for influenza specific to each location type [30, 33].
Once infected, each individual had latent and infectious periods drawn from distributions calibrated so that the average generation interval distribution matched estimates from Singapore (mean = 5.20, standard deviation = 1.72) [34]. The absolute risk of transmission depended on the number and location of an infected individual’s contacts and a parameter that controls SARS-CoV-2 transmissibility upon contact, which we calibrated. A proportion of the infections were asymptomatic [35]. We assumed these infections were as infectious as symptomatic infections and had identical incubation and infectious period distributions [36, 37, 26, 38]. We assumed that children were less susceptible to infection than adults, which we modeled with a logistic function calibrated to model-based estimates of this relationship by Davies et al. [19]. We assumed that severity of disease increased with age, consistent with statistical analyses performed elsewhere [39, 40, 41, 21].
Agent behavior in FRED has the potential to change over the course of an epidemic. Following the onset of symptoms, infected agents self-isolate at home according to a fixed daily rate, whereas others continue their daily activities [42, 43]. This rate was chosen so that, on average, 68% of agents will self-isolate at some point during their symptoms, where 68% is the proportion of symptomatic infections with a fever and assuming that those with a fever are likely to self-isolate. [43]. Agents can also respond to public health interventions, including school closure, shelter in place, and a combination of mask-wearing and social distancing. School closures occur on specific dates [44], resulting in students limiting their activity space to household and neighborhood locations. Shelter-in-place interventions reduce some agents’ activity spaces to their households only, whereas others continue with their daily routines. We used mobility reports from Google [45] to drive daily compliance with shelter-in-place, such that shelter-in-place compliance in our model accounts for both the effects of shelter-in-place orders and some people deciding to continue staying at home after those orders are lifted [46]. We used Google Trends data for Indiana using the terms “face mask” and “social distancing” [47] to capture temporal trends and survey data [48] to capture the magnitude of these behaviors. Our default assumption about protection afforded by face masks followed a median estimate of the adjusted odds ratio of 0.3 against SARS-CoV in a non-health care setting [49, 31]. Further details about the model are available in the Supplementary Text.
Data and outcomes
We obtained daily incidence of death from the New York Times COVID-19 database [1]. Hospitalizations and the age distribution of deaths reported in Indiana were obtained from the Indiana COVID-19 dashboard [8]. Daily numbers of tests performed in the state were available from The Covid Project [50]. We calibrated the model to daily values of deaths, hospitalizations, and test positivity through August 10 and to the age distribution of deaths cumulative through July 13 to estimate nine model parameters using a sobol design sampling algorithm [51, 52] (Supplementary Material). We validated the model by comparing its predictions of the infection attack rate overall and by age to results from two statewide serological surveys undertaken in late April and early June [53, 54].
To account for uncertainty in the calibrated parameters in our future projections, we simulated nine scenarios about school reopening with values of the model’s nine free parameters sampled from the calibrated distribution. From August 24 to December 31, we outputted numbers of daily infections, symptomatic cases, hospitalizations, and deaths, structured by age, place of infection (school, home, other), and affiliation with schools (student, teacher, none). For our analysis, we focused on infections, symptomatic infections, and deaths in the overall population and the subgroups of students, teachers, and their families.
Model scenarios
Our primary analysis focused on three scenarios for school operating capacity (50%, 75%, or 100% of students receiving in-person instruction) and three scenarios for face-mask adherence in schools (50%, 75%, or 100%). We compared each of the nine combinations of these scenarios to a scenario in which schools reopened normally (100% capacity, 0% face-mask adherence) and to a scenario in which schools operated remotely until the end of the calendar year. For each of these scenarios, we analyzed the sensitivity of the model outcomes to parameter uncertainty by calculating the partial rank correlation coefficient [55] of each calibrated parameter and two outcomes: the cumulative number of infections between August 24 and December 31, and the proportion of infections acquired in schools during that period.
In addition to our primary analysis, we considered alternative scenarios about select model parameters that we regarded as potentially important unknowns. To explore the possibility that children play a lesser role in SARS-CoV-2 transmission than our default assumptions would suggest, we considered one alternative scenario in which asymptomatic infections (which are more likely to occur among children) are half as infectious as symptomatic infections, and a second alternative scenario in which children aged 0-10 years have lower susceptibility (0.1). To explore the possibility that face masks could be either more or less protective than our default assumption would suggest, we considered scenarios that followed adjusted odds ratio estimates at the lower (0.12) and upper (0.73) ends of the 95% CrI from the study that informed our default assumption about protection afforded by face masks [49, 31].
3 Results
Our model was generally consistent with the data to which it was calibrated, capturing trends over time in daily deaths, hospitalizations, and test positivity (Fig. 1A-C), as well as greater proportions of deaths among older age groups (Fig. 1D). Some trade-offs in the model’s ability to recreate different data types were apparent, such as a recent increase in hospitalizations that the model failed to capture (Fig. 1C), likely due to the predominance of data on deaths in the likelihood. Even so, the model’s predictions reproduced the range of variability in the data, as assessed by coverage probability of its 95% posterior predictive intervals (daily deaths: 0.85; daily hospitalizations: 0.93; daily test positivity: 0.95; cumulative deaths by age: 1.0). The model was also consistent with data withheld from fitting. Across all ages, the model’s 95% posterior predictive intervals of the cumulative proportion infected through late April (median: 0.017; 95% CrI: 0.0045-0.051) and early June (median: 0.022; 95% CrI: 0.0058-0.069) spanned estimates from two state-wide serological surveys [53] (Fig. 2A). Our model’s predictions also overlapped with age-stratified estimates from those surveys (Fig. 2B), although it underpredicted infections among individuals aged 40-60 years.

Model calibration to data: A) daily incidence of death; B) proportion of deaths through July 13 in decadal age bins; C) daily incidence of hospitalization; and D) daily proportion of tests administered that are positive for SARS-CoV-2. In all panels, blue diamonds represent data. In A, C, and D, the gray line is the median, the dark shaded region the 50% posterior predictive interval, and the light shaded region the 95% posterior predictive interval.

Model comparison with data withheld from fitting. We validated the model’s predictions against data withheld from fitting on A) the cumulative proportion of the population of Indiana infected through late April and early June, and B) the cumulative proportion infected among individuals aged 12-40, 40-60, and 60+. Data are shown in navy and come from a random, statewide serological survey [53]. Model predictions are shown in gray. In A, the line and band indicate the median and 95% posterior predictive interval. In B, lines, boxes, and error bars indicate median, interquartile range, and 95% posterior predictive interval.
Calibration of the parameter that scaled the magnitude of SARS-CoV-2 importations [56, 57] in our model resulted in a median of 1.299 (95% PPI: 0.502-1.461) imported infections per day from February 1 to August 10. To ensure that the model reliably reproduced the high occurrence of deaths observed in long-term care facilities, we seeded infections into those facilities at a daily rate proportional to the prevalence of infection on that day; this calibrated proportion was 0.037 (95% PPI: 0.022-0.092). On the opposite end of the age spectrum, our calibration resulted in a median estimate of susceptibility among children of 0.346 (95% CrI: 0.311-0.506), compared to 0.834 (95% CrI: 0.652-0.946) in adults (Fig. S1). Our calibration resulted in an estimate of transmissibility (median: 0.593; 95% CrI: 0.501-0.788) that corresponded to values of R(t) during the initial phase of the epidemic in Indiana of 1.46 (95% CrI: 0.31-3.48), which represents an average of daily values across the month of February (Fig. 1A). Driven by a calibrated estimate 32.1% (95% CrI: 28.8-66.9%) on April 7 (Fig. S2A), our estimates of R(t) dropped to a low of 0.57 (95% CrI: 0.42-0.71) on April 7 and have remained below 1 since (Fig. 1A). Also impacting our estimates of R(t) is the increasing use of face masks in the community, which we estimated at 0.534 (95% CrI: 0.461-0.540) as of July 19 (Fig. S2B). Note that this estimated distribution of community face-mask adherence does not differ between scenarios and is not the same as the level of adherence in schools, which we imposed at different levels depending on the scenario.
In the event that schools reopen at full capacity and without any use of face masks, our model projects that R(t) would increase to 1.72 (95% CrI: 1.43-2.17) by mid-September (Fig. 3A). This assumes that levels of sheltering in place and face-mask adherence in the community remain at their estimated levels as of August 13 (Fig. S2B). Consistent with our model’s prediction that schools contributed appreciably to transmission early in the epidemic (median: 26.2%; 95% CrI: 21.0-27.5%), this increase in transmission is associated with an increase in the proportion of infections arising in schools upon their reopening (Fig. 3B). The sensitivity of the proportion of infections arising in schools to model parameters was highest for the inflection point of the age-susceptibility relationship, the transmissibility parameter, and the rate at which infections were imported into long-term care facilities (Fig. S6). This increase in infections arising in schools is projected to give rise to additional transmission statewide (Fig. 3C). An example of transmission chains arising from schools and spilling out into school-affiliated families and the broader community is shown in Fig. 4.

The impact of school reopening in Indiana on: A) the reproduction number, R(t), over time; B) the proportion of infections acquired in different location types over time; and C) the daily incidence of infection over time. In all panels, schools reopened on August 24. In A and C, the line represents the median, and the shaded region represents the 50% posterior predictive interval.

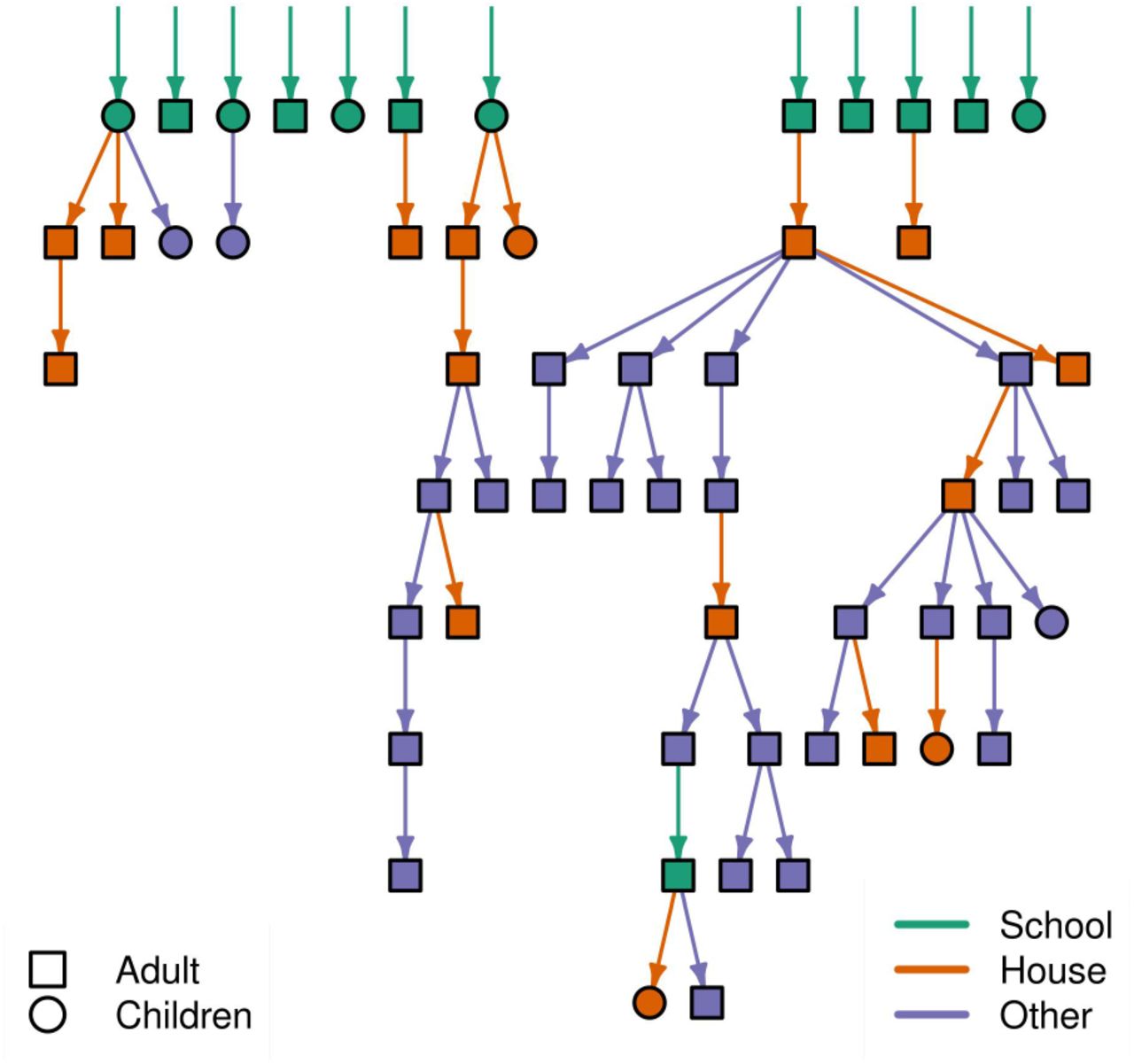
Example transmission tree of SARS-CoV-2 from one simulation of the model for Saint Joseph County, Indiana. Green shapes at the top represent agents in the model infected at school, and arrows descending from them and other shapes show transmission events in school-affiliated households (orange) and the community at large (purple) that trace back to infections originally acquired in schools. Different shapes distinguish children (circles) from adults (squares).
In the event that schools remain open throughout the semester and no other policies or behavioral responses occur, the increase in R(t) driven by reopening schools at full capacity and without the use of face masks would be projected to result in 2.57 million (95% CrI: 2.36-2.88 million) infections (Fig. 5A) and 10,246 (95% CrI: 7,862-13,794) deaths (Fig. 5B) from Indiana’s population as a whole between August 24 and December 31. At the other extreme, if schools were to go to remote instruction and all children remained at home, our model projects that R(t) would remain near current levels through the remainder of 2020 (Fig. S3A). Again, this assumes that levels of sheltering in place and face-mask adherence in the community as a whole remain at their estimated levels as of August 13. Under this scenario, transmission would continue through contacts at workplaces, within homes, and elsewhere in the community (Fig. S3B), with 45,579 (95% CrI: 14,651-132,546) infections (Fig. S3C) and 790 (95% CrI: 176-1680) deaths between August 24 and December 31.

The impact of different school reopening strategies on A) cumulative infections and B) cumulative deaths in Indiana between August 24 and December 31. Scenarios are defined by the capacity at which schools operate (x-axis) and face-mask adherence (shading). Orange lines represent projections under a scenario of school reopening at full capacity without masks (solid: median; dotted: 95% posterior predictive interval). Blue lines represent a scenario where schools operate remotely. Error bars indicate inter-quartile ranges.
Differing policies on the capacity at which schools operate in person and enforce the use of face masks have a strong influence on the projected statewide burden of COVID-19. If schools operate at 50% capacity and achieve high face-mask adherence, the number of infections and deaths that we project is similar to what we project under the scenario in which schools operate remotely (Fig. 5, Table S1). Of these two policies, projections of infections and deaths were more sensitive to the capacity at which schools operate, with the worst outcomes projected to occur when schools operate at full capacity and with low face-mask adherence. Under this scenario, cumulative infections statewide were projected to be 42.8 (95% CrI: 41.3-44.3) times greater than if schools operated remotely, and cumulative deaths statewide were projected to be 9.2 (95% CrI: 8.9-9.5) times greater (Table S1). The sensitivity of these results to model parameters was relatively high for parameters that define the age-susceptibility relationship and, in some cases, for the transmissibility and shelter-in-place compliance parameters (Fig. S5).
We also explored the sensitivity of these results to alternative assumptions about the contribution of children to SARS-CoV-2 transmission and protection afforded by face masks. Under an alternative assumption that susceptibility of children aged 0-10 years was only 0.1, we observed reductions in cumulative infections and deaths that were consistent but relatively modest compared to differences due to operating capacity and face-mask adherence (Table S10, S11). Under an alternative assumption that the relative infectiousness of asymptomatic infections was 50% that of symptomatic infections, we observed reductions in cumulative infections and deaths under high operating capacity but increases under low and medium capacity (Table S10, S11). Again though, these differences were relatively modest compared to differences due to operating capacity and face-mask adherence. Alternative assumptions about protection afforded by face masks resulted in consistent differences in cumulative infections and deaths, with lower face-mask efficacy associated with more infections and deaths (Table S12, S13). For example, under a scenario with 50% operating capacity and 100% face-mask adherence in schools, the increase in cumulative infections relative to operating remotely ranged from 7% (95% CrI: 3-11%) to 307% (95% CrI: 294-322%). Even so, the relative impacts of varying levels of operating capacity and face-mask adherence were generally similar under these alternative assumptions.
The burden of COVID-19 associated with reopening schools differed for students, teachers, and their families. Relative to a scenario with remote instruction, risk of infection and symptomatic infection was greatest for students (Fig. 6, left column), with a hundred-fold or greater increase in the risk of infection if schools operate at full capacity with moderate or low face-mask adherence (Table S2). Due to their older ages, teachers and families experienced a much higher risk of death under scenarios with high capacity and moderate or low face-mask adherence, as compared with a scenario with remote instruction (Fig. 6, center & right columns). Under a scenario with high capacity and low face-mask adherence, there was a 166-fold higher risk of death for teachers (Table S3) and a 223-fold higher risk of death for family members of students and teachers (Table S4). At the same time, the risk of death under a scenario with high capacity and low face-mask adherence was around 72% the risk of death if schools were to operate at full capacity with no masks (Tables S7 & S8).

The impact of different school reopening strategies on cumulative infections (top row), cumulative symptomatic infections (middle row), and cumulative deaths (bottom row) in Indiana between August 24 and December 31. These outcomes are presented separately for students (left column), teachers (middle column), and school-affiliated families (right column). Scenarios are defined by the capacity at which schools operate (x-axis) and face-mask adherence (shading). Orange lines represent projections under a scenario of school reopening at full capacity without masks (solid: median; dotted: 95% posterior predictive interval). Blue lines represent a scenario where schools operate remotely. Error bars indicate inter-quartile ranges.
4 Discussion
Our model provides a detailed, demographically realistic representation of SARS-CoV-2 transmission in Indiana that is consistent both with data to which it was calibrated and to data that was withheld from calibration. In contrast to models that rely on assumptions about intervention impacts or estimate them statistically [2, 58], our model makes predictions about intervention impacts based on first-principles assumptions about individual-level behavior and contact patterns. Consistent with results from other analyses [2, 58, 20], the inputs and assumptions in our model led to a prediction that schools made a considerable contribution to SARS-CoV-2 transmission in February and early March, prior to large-scale changes in behavior. Extending that, a primary result of our analysis is that schools could, once again, make a considerable contribution to SARS-CoV-2 transmission as they resume normal activity in the fall semester.
Our results indicate that operating at reduced capacity and achieving high face-mask adherence would reduce the burden of COVID-19 in schools and across the state. In the event that both interventions are pursued fully, our model projects that infections and deaths statewide would be around 10% greater than under a scenario with fully remote instruction. In the event that schools operate at full capacity, our model projects that infections and deaths statewide could be one to two orders of magnitude greater than under a scenario with fully remote instruction, especially if there is poor face-mask adherence in schools. The impacts associated with reducing capacity result from reductions in both the number of contacts within the school and the probability that an infected student would be in attendance in the first place, similar to the logic behind why smaller gatherings are associated with reduced risk of transmission [3, 59, 60]. The magnitude of our results was most sensitive to the degree of protection afforded by face masks, which remains uncertain in school and other community settings for SARS-CoV-2 [31].
Although the scenarios we considered resulted in projected impacts spanning nearly the full range between fully remote instruction and fully in-person instruction with no face masks, they are a simplification of the full range of scenarios of how schools could operate this fall. Scenarios that we did not explore include different groups of students attending in person or remotely [61], varying degrees of modularization within schools [62], and the implementation of testing-based control strategies in schools [63]. A related simplification of our statewide analysis is that the state, in reality, consists of a patchwork of policies across districts. In light of this complexity that our model does not capture, our results should be interpreted with caution in setting specific, quantitative targets for capacity or face-mask adherence. For any scenario though, our results illustrate the importance of reducing capacity and maximizing face-mask adherence to the extent possible, as do other modeling studies [61, 62, 63, 64, 65].
The burden of COVID-19 associated with reopening schools is not expected to fall evenly across the state’s population. Under scenarios with schools operating at full capacity, our model projects that hundreds of thousands of children could be infected during the fall semester. Whereas very few deaths are expected among infected children, the numbers of deaths among teachers and school-affiliated families could number in the hundreds. In comparison, the total number of deaths projected across the state is projected to be in the low thousands, meaning that adults with close ties to schools could represent a sizable fraction of deaths across the state in coming months, if schools operate at full capacity and with low face-mask adherence. Importantly, the magnitude of these projections depend further on factors outside the control of schools [2]. In the absence of school reopening, our projections assume steady, controlled levels of transmission with R(t) < 1. Changes in government policies, individual behavior, and face-mask adherence in the community all have the potential to alter this trajectory for the state as a whole, as well as its schools [2, 31, 66].
A critical assumption of our analysis is that children are capable of being infected with SARS-CoV-2 and transmitting it to others at meaningful levels. Although the burden of severe disease skews strongly towards older ages [22, 67, 8], there are other lines of evidence that support our assumption. These include a contact-tracing study that found no distinguishable difference between infectivity of children and adults [26], several studies that found no distinguishable difference in viral load between children and adults [68, 37, 36, 69], a study that observed a greater secondary attack rate among children in homes [26], and a modeling study that found no evidence that children were less infectious [70]. More direct evidence comes from COVID-19 outbreaks that have already been observed in schools, including one in a high school in Israel in which 13.2% of students and 16.6% of staff were infected in just 10 days [71]. Even more pertinent, some schools in Indiana recently reopened and have already reported cases of COVID-19 among students [72]. Our analysis offers perspective on what those initial cases could give rise to in coming months, depending on the degree to which schools choose to operate at reduced capacity and enforce face-mask adherence. Based on two alternative scenarios we explored about the potential for SARS-CoV-2 transmission among children, these lessons about the importance of operating capacity and face-mask adherence appear robust to outstanding biological uncertainties about transmission of SARS-CoV-2 by children.
There is now a growing body of evidence that school closures contributed to mitigating the first wave of the epidemic and could lead to rising case numbers if relaxed [6, 63]. Our study adds to this evidence, and suggests an even greater impact of school reopening than several other studies [65, 63, 62, 73, 61]. This is due in part to our assumption that asymptomatic and symptomatic infections contribute similarly to transmission [26, 68, 37, 36, 69], and in part to our model’s ability to capture chains of transmission within schools and extending out into the community. Our study echoes several modeling studies in emphasizing the importance of reducing school capacity to impede transmission [62, 63, 64, 65, 73]. As schools grapple with COVID-19 throughout fall 2020 and beyond, results such as these provide an important basis for motivating the adoption and sustainment of reductions in operating capacity and adherence to face-mask requirements. As we demonstrated, these actions are highly consequential for those directly linked to schools and for the communities in which they are embedded.
Data Availability
The data is publicly available
5 Acknowledgements
This work was supported by an NSF RAPID grant to TAP (DEB 2027718), an Arthur J. Schmitt Fellowship and Eck Institute for Global Health Fellowship to RJO, and a Richard and Peggy Notabaert Premier Fellowship to MP. We thank the University of Notre Dame Center for Research Computing for computing resources.
Footnotes
Updated manuscript to change the baseline assumptiono f face-mask protection from 0.15 adjusted OR to 0.3 (0.12 - 0.73) adjusted OR, based on the review of face-mask efficacy on a non-health-care setting. We also updated the assumptions to include an alternative assumption on the infectivity of asymptomatic infections to be half as infectious as symptomatic infections. In addition, we included an alternative scenario in which children aged 0-10 years have lower susceptibility.
References
- [1].↵
- [2].↵
- [3].↵
- [4].↵
- [5].↵
- [6].↵
- [7].↵
- [8].↵
- [9].↵
- [10].↵
- [11].↵
- [12].↵
- [13].↵
- [14].↵
- [15].↵
- [16].↵
- [17].↵
- [18].↵
- [19].↵
- [20].↵
- [21].↵
- [22].↵
- [23].↵
- [24].↵
- [25].↵
- [26].↵
- [27].↵
- [28].↵
- [29].↵
- [30].↵
- [31].↵
- [32].↵
- [33].↵
- [34].↵
- [35].↵
- [36].↵
- [37].↵
- [38].↵
- [39].↵
- [40].↵
- [41].↵
- [42].↵
- [43].↵
- [44].↵
- [45].↵
- [46].↵
- [47].↵
- [48].↵
- [49].↵
- [50].↵
- [51].↵
- [52].↵
- [53].↵
- [54].↵
- [55].↵
- [56].↵
- [57].↵
- [58].↵
- [59].↵
- [60].↵
- [61].↵
- [62].↵
- [63].↵
- [64].↵
- [65].↵
- [66].↵
- [67].↵
- [68].↵
- [69].↵
- [70].↵
- [71].↵
- [72].↵
- [73].↵




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}