
Summary
Objective to review the evidence from studies comparing SARS-CoV-2 culture, the best indicator of current infection and infectiousness with the results of reverse transcriptase polymerase chain reaction (RT-PCR).
Methods We searched LitCovid, medRxiv, Google Scholar and the WHO Covid-19 database for Covid-19 using the terms ‘viral culture’ or ‘viral replication’ and associated synonyms up to 10 September 2020. We carried out citation matching and included studies reporting attempts to culture or observe SARS-CoV-2 matching with cutoffs for RT-PCR positivity. One reviewer extracted data for each study and a second reviewer checked end edited the extraction and summarised the narratively by sample: fecal, respiratory, environment or mixed.
Where necessary we wrote to corresponding authors of the included or background papers for additional information. We assessed quality using a modified QUADAS 2 risk of bias tool.
This review is part of an Open Evidence Review on Transmission Dynamics of COVID-19. Summaries of the included studies and the protocol (v1) are available at: https://www.cebm.net/evidence-synthesis/transmission-dynamics-of-covid-19/. Searches are updated every 2 weeks. This is the fourth version of this review that was first published on the 4th of August and updated on the 21t of August
Results We included 29 studies reporting culturing or observing tissue invasion by SARS-CoV in sputum, naso or oropharyngeal, urine, stool, blood and environmental samples from patients diagnosed with Covid-19. The data are suggestive of a relation between the time from collection of a specimen to test, cycle threshold and symptom severity. The quality of the studies was moderate with lack of standardised reporting.
Twelve studies reported that Ct values were significantly lower and log copies higher in samples producing live virus culture. Five studies reported no growth in samples based on a Ct cut-off value. These values ranged from CT > 24 for no growth to Ct ≥ 34. Two studies report a strong relationship between Ct value and ability to recover infectious virus and that the odds of live virus culture reduced by 33% for every one unit increase in Ct. A cut-off RT-PCR Ct > 30 was associated with non-infectious samples. One study that analysed the NSP, N and E gene fragments of the PCR result reported different cut-off thresholds depending on the gene fragment analysed. The duration of RNA shedding detected by PCR was far longer compared to detection of live culture. Six out of eight studies reported RNA shedding for longer than 14 days. Yet, infectivity declines after day 8 even among cases with ongoing high viral loads. A very small proportion of people re-testing positive after hospital discharge or with high Ct are likely to be infectious.
Conclusion Prospective routine testing of reference and culture specimens are necessary for each country involved in the pandemic to establish the usefulness and reliability of PCR for Covid-19 and its relation to patients’ factors. Infectivity is related to the date of onset of symptoms and cycle threshold level.
A binary Yes/No approach to the interpretation RT-PCR unvalidated against viral culture will result in false positives with possible segregation of large numbers of people who are no longer infectious and hence not a threat to public health.
Introduction
The ability to make decisions on the prevention and management of COVID-19 infections rests on our capacity to identify those who are infected and infectious. In the absence of predictive clinical signs or symptoms1, the most widely used means of detection is molecular testing using Reverse Transcriptase quantitative Polymerase Chain Reaction (RT-qPCR)2,3.
The test amplifies genomic sequences identified in samples. As it is capable of generating observable signals from small samples, it is very sensitive. Amplification of genomic sequence is measured in cycle thresholds (Ct). There appears to be a correlation between Ct values from respiratory samples, symptom onset to test (STT) date and positive viral culture. The lower the Ct value and the shorter the STT, the higher the infectivity potential4.
Whether probing for sequences or whole genomes5, in the diagnosis of Covid-19 a positive RT-qPCR cannot tell you whether the person is infectious or when the infection began, nor the provenance of the genetic material. Very early in the COVID-19 outbreak it was recognised that cycle threshold values may be a proxy for quantitative measure of viral load, but correlation with clinical progress and transmissibility was not yet known6. A positive result indicates that a person has come into contact with the genomic sequence or some other viral antigen at some time in the past. However, presence of viral genome on its own is not sufficient proof of infectivity and caution is needed when evaluating the infectivity of specimens simply based on the detection of viral nucleic acids5. In addition, viral genomic material can be still be present weeks after infectious viral clearance.7 Like all tests, RT-qPCR requires validation against a gold standard. In this case isolation of a whole virion (as opposed to fragments) and proof that the isolate is capable of replicating its progeny in culture cells is the closest we are likely to get to a gold standard.8 The inability of PCR to distinguish between the shedding of live virus or of viral debris, means that is cannot measure a person’s viral load (or quantity of virus present in a person’s excreta).
Our Open Evidence Review of transmission modalities of SARS CoV-2 identified a low number of studies which have attempted viral culture. There are objective difficulties in doing such cultures such as the requirement for a level III laboratory, avoidance of contamination, time and the quality of the specimens as well as financial availability of reagents and culture media to rule out the presence of other pathogens.
As viral culture represents the best indicator of infection and infectiousness, we set out to review the evidence on viral culture compared to PCR, and report the results of those studies attempting viral culture regardless of source (specimen type) of the sample tested.
Methods
We searched four main databases: LitCovid, medRxiv, Google Scholar and the WHO Covid-19 database for Covid-19 using the terms ‘viral culture’ or ‘viral replication’ and associated synonyms. Searches were last updated on 10 September 2020. Searches are conducted on a per calendar month basis and for databases which do not support such date granularity, the date of publication is approximated. For articles that looked particularly relevant, citation matching was undertaken and relevant results were identified.
We included studies reporting attempts to culture SARS-CoV-2 and those which also estimated the infectiousness of the isolates or observed tissue invasion by SARS CoV-2. One reviewer extracted data for each study and a second review checked end edited the extraction. We tabulated the data and summarised data narratively by mode of sample: fecal, respiratory, environment or mixed.
Where necessary we wrote to corresponding authors of the included or background papers for additional information. We assessed quality using a modified QUADAS 2 risk of bias tool. We simplified the tool as the included studies were not designed as primary diagnostic accuracy studies.9
This review is part of an Open Evidence Review on Transmission Dynamics of COVID-19. Summaries of the included studies and the protocol (v1) are available at: https://www.cebm.net/evidence-synthesis/transmission-dynamics-of-covid-19/. Searches are updated every 2 weeks.
This is the fourth update of this review with the addition of four studies identified in the two weeks since the last update.
Results
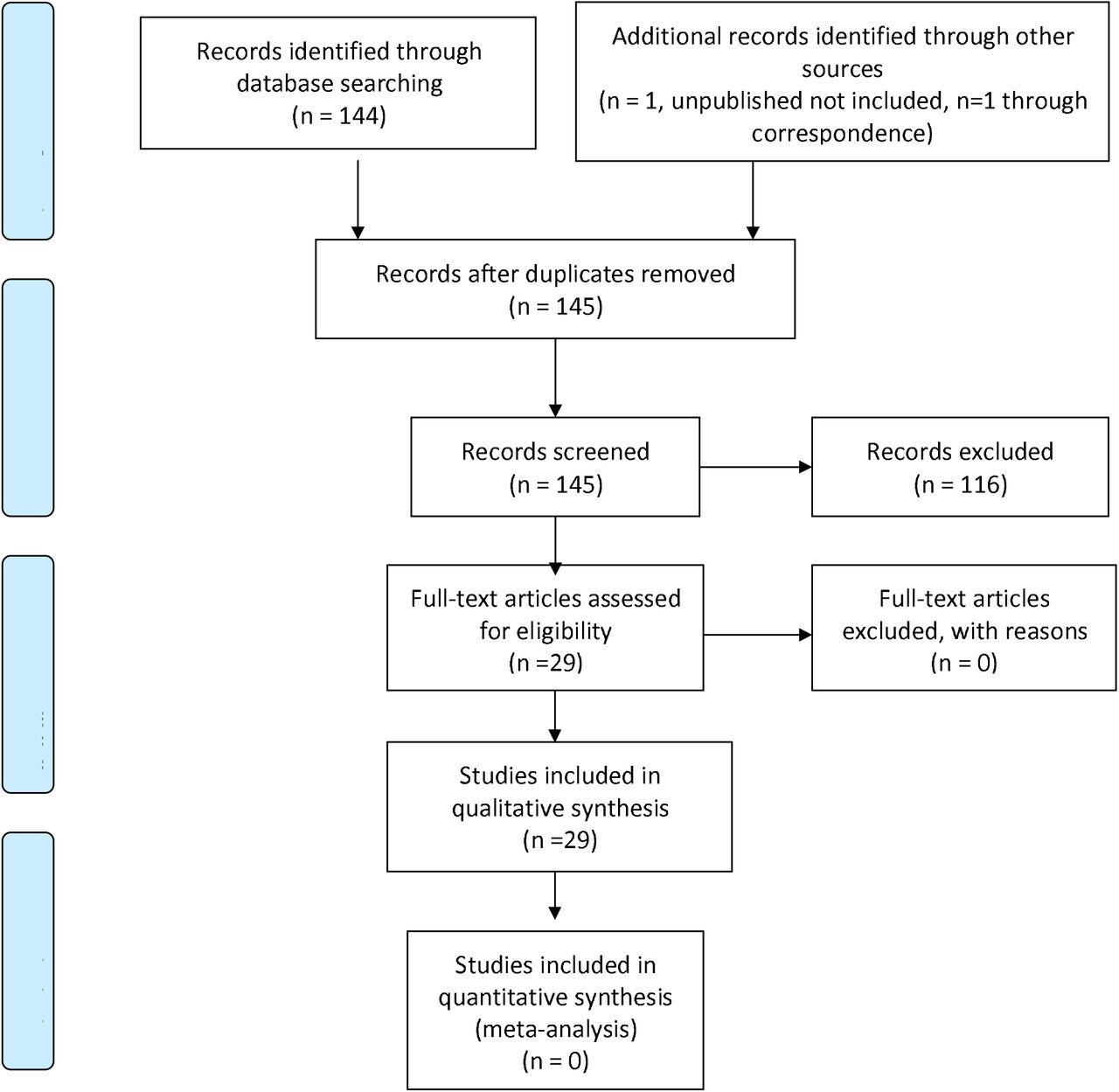
We identified 145 articles of possible interest and after screening full texts included 29 (see PRISMA10 flow chart - Figure 1). We identified one unpublished study which was not included as no permission to do so was given by the authors. The salient characteristics of each included study are shown in Table 1.

{kind=link}
Characteristics of included studies. Key: STT = symptom onset to test date.
All included studies were case series of moderate quality (Table 2. Quality of included studies). We could not identify a protocol for any of the studies. All the included studies had been either published or were available as preprints. All had been made public in 2020. We received five responses from authors regarding clarifying information (see Acknowledgments).
Quality of included studies
Studies using fecal samples
Nine studies assessed viral viability from fecal samples which were positive for SARS-CoV-2 based on RT-PCR result 11-13,14-19. One study reported infecting ferrets with stool supernatant11, two reported visual growth in tissue12,20 and five reported achieving viral replication13-16. One laboratory study21 found that SARS-CoV-2 infected human small intestinal organoids.
Studies using respiratory samples
Sixteen studies on respiratory samples reported achieving viral isolation4,22,11,23,24,14,15,16,25-28,19,29-31. One study assessed 90 nasopharyngeal samples and cultured 26 of the samples, and positive cultures were only observed up to day eight post symptom onset; 4 another study obtained 31 cultures from 46 nasopharyngeal and oropharyngeal samples; 23 while 183 nasopharyngeal and sputum samples produced 124 cases in which a cytopathic effect was observed although the denominator of samples taken was unclear 32. Another study in health care workers in UK hospitals isolated one SARS Cov-2 from nineteen specimens in a situation of low viral circulation.27
Two more studies reported a clear correlation between symptoms onset, date of sampling, Ct and likelihood of viral culture. 25,26
L’Huillier and colleagues28 sampled nasopharyngeal swabs in 638 patients aged less than 16 years in a Geneva Hospital: 23 (3.6%) tested positive for SARS CoV-2 - median age of 12 years and 12 (52% were culture positive). The Ct was around 28 for the children whose samples grew viable viruses. Gniazdowski 29 probably assessed 161 nasopharyngeal specimens. A positive culture was associated with Ct values of 18.8 ± 3.4. Infectious viral shedding occurred in specimens (a Ct ≥ 23 yielded 8.5% of virus isolates).
Basile and colleagues 30 found a culture positivity rate of 24%, which was significantly more likely to be positive in ICU patients compared with other inpatients or outpatients.
A report by the Korean Centres for Disease Control failed to grow live viruses from 108 respiratory samples 33 from “re-positives” i.e. people who had tested positive after previously testing negative33
Ladhani 31 and colleagues reported a successful culture rate of out 31 of 86 RT-PCR positive nasopharyngeal samples from six nursing home in London.
The largest number of positive culture came from the La Scola group publications32 with 1941 positive cultures from 3790 samples.
Studies using environmental samples
Two possible positive cultures were obtained from 95 environmental samples in one study that assessed the aerosol and surface transmission potential of SARS-CoV-2 34. Zhou and colleagues reported on samples taken from seven areas of a large London hospital. Despite apparent extensive air and surface contamination of the hospital environment, no infectious samples were grown35. For air samples, 2/31 (6.4%) were positive and 12/31 (39%) suspect for SARS-CoV-2 RNA but no virus was cultured. Similarly, 91 of 218 surface samples were suspect (42%) or 23 positive (11%) for SARS-CoV-2 RNA but no virus was cultured. The authors noted that a cut-off RT-PCR Ct > 30 was associated with non-infectious specimens.
Ahn and colleagues36 failed to grow live virus from an unspecified number of air samples in isolation rooms of patients with severe Covid-19 but were able to grow virus from swabs of hand rails, and the external surfaces of intubation cannulae.
Mixed sources
Some of the studies labelled as mixed source samples are also reported in individual provenance breakdown in this text because of lack of clarity of the text.
Eight studies reported viral culture from mixed sources. Using 60 samples from 50 cases of Covid-19, viral culture was achieved from 12 oropharyngeal, nine nasopharyngeal and two sputum samples5. Jeong et al 11 who reported isolation live virus from a stool sample also reported that from of an unreported number of nasopharyngeal, oropharyngeal, saliva, sputum and stool samples, one viral culture was achieved: ferrets inoculated with these samples became infected; SARS-CoV-2 was isolated from the nasal washes of the two urine-treated ferrets and one stool-treated ferret11. An unreported number of samples from saliva, nasal swabs, urine, blood and stool collected from nine Covid-19 patients produced positive cultures and a possible specimen stool culture14. One study showed that from nine nasopharyngeal, oropharyngeal, stool, serum and urine samples, all nine were culturable, including two from non-hospitalised Covid-19 patients15.
Yao and colleagues cultured viable viral isolates from seven sputum samples, three stool samples and one nasopharyngeal sample of 11 patient aged 4 months to 71 years, indicating that the SARS-CoV-2 is capable of replicating in stool samples as well as sputum and the nasopharynx.16 All samples had been taken within 5 days of symptom onset. The authors also report a relationship between viral load (copy thresholds) and cytopathic effect observed in infected culture cells.37
Kim and colleagues reported no viral growth from and unclear number of serum, usirne and stool samples despite collection very soon after admission17. Lu and colleagues also reported no viral growth, however their specimens were from 87 cases tested “re-positive”.18
Young and colleagues 19 from Singapore had 21 positive cultures from 19 hospitalised patients in Singapore. No virus was isolated from samples with a Ct value >30, or when the sample was collected >14 days after symptoms onset. All positive cultures came from naso-pharyngeal samples, none of the 24 urine or 35 stool samples exhibited viral growth
Blood cultures
In one study by Andersson38 et al 20 RT-PCR positive serum samples were selected at random from a Covid-19 sample bank, representing samples from 12 individual patients (four individuals were represented at two timepoints), collected at 3 to 20 days following onset of symptoms. None of the 20 serum samples produced a viral culture
Post mortem study
One study on alveolar samples from 68 elderly deceased gre iable virus from 6 out 6 different samples, in one case on day 26 from symptom onset.39
Duration of viral shedding
Nine studies report on the duration of viral shedding as assessed by PCR for SARS-CoV-2 RNA4,11,20,13,14,15,13,25,40. The minimum duration of RNA shedding detected by PCR was seven days reported in Bullard, the maximum duration of shedding was 35 days after symptom onset in Qian. Seven out of eight studies reported RNA shedding for longer than 14 days (see Table 3).
Duration of viral shedding in the included studies.
Young et al19 reported that 91% of patients had ceased viral shedding by day 20 from symptom onset.
Duration of live viral culture detection
The duration of live viral culture detection was much shorter than viral shedding. Wölfel et al 14reported that virus could not be isolated from samples taken after day 8 even among cases with ongoing high viral loads of approximately 105 RNA copies/mL.
Bullard et al similarly reported that SARS-CoV-2 Vero cell infectivity of respiratory samples from SARS-CoV-2 positive individuals was only observed for RT-PCR Ct < 24 and symptom onset to test of < 8 days4.
Singanayagam and colleagues 25 reported the median duration of virus shedding as measured by viral culture was 4 days (Inter Quartile Range: 1 to 8)25.
The relationship between RT-PCR results and viral culture of SARS-CoV-2
Fifteen studies attempted to quantify the relationship between cycle threshold (Ct) and likelihood of culturing live virus4,5,12,32,13,15,14,16,25,26,27,28-31. Table 4 shows that nine studies analysed the relationship between Ct values and live viral culture4,5,32,25,27,29,30,31,19 and three quantified the mean log copies of detected virus and live culture5,26,28. All reported that Ct were significantly lower and log copies were significantly higher in those with live virus culture. Five studies reported no growth in samples based on a Ct cut-off value4,5,27.19,31 These values for no growth ranged from CT > 244 to Ct ≥ 3531.
Relationship of PCR Cycle threshold and Log10 copies to Positive Viral Culture
Singanayagam et al 22 reported the estimated probability of recovery of virus from samples with Ct < 35 was 8.3% (95% CI: 2.8%-18.4%). All donors above the Ct threshold of 35 (n=5) with live culture were symptomatic.
The study in London nursing homes by Ladhani and colleagues found no correlation between Ct values with presence or absence of symptoms in either residents or staff31, although nearly 50%of both categories were asymptomatic.
Huang and colleagues5 analysed the NSP, N and E gene fragments of the PCR result, which reported different cut-off thresholds depending on the gene fragment analysed5. No growth was found for the NSP 12 fragment at Ct > 31.47, whereas the value was higher for the N gene fragment at >35.2.
Bullard et al 4 reported a reduction in the odds ratio for culturing live virus of 0.64 for every one unit increase in Ct (95%CI 0.49 to 0.84, p<0.001). Similar to Bullard and colleagues, Singanayagam 22 reported a strong relationship between Ct value and ability to recover infectious virus: estimated OR of recovering infectious virus decreased by 0.67 for each unit increase in Ct value (95% CI: 0.58-0.77). This value is very close to that of other empirical studies (an increased Ct of 0.58 per day since symptoms started)41
Young et al19 reported no viral isolation from samples where the Ct value was >30, or when the sample was collected >14 days after symptoms onset.
Discussion
Society is attempting to interrupt transmission of SARS-CoV-2 by identifying and isolating those who are sick and those who are infectious. As there are no Covid-19-specific mass treatments or preventive measures, such a strategy relies on our capability to identify infected and infectious persons with a reasonable amount of certainty to avoid isolation of those who pose little threat to the public health. An increasing body of evidence shows that such identification cannot be accurately achieved through the simplistic division of those who test positive and who do not, on the basis of the results of RT-PCR. The sensitivity and specificity of RT-PCR needs comparing to the gold standard of infectiousness: the capacity to grow live virus from a specimen.
Some of the authors of the studies in our review have attempted and successfully achieved culture of SARS-CoV-2 in the laboratory, using a range of respiratory, fecal or environmentally collected samples. However the simplistic dichotomous division into positive/negative is insufficient to accurately identify infectiousness as detection of viral RNA cannot support an inference of contagiousness42. The evidence shows that there is a positive relationship between lower cycle count threshold, likelihood of positive viral culture43 and date of symptom onset. Nowhere can this be seen as clearly as in the two studies assessing the infectiousness of “re-positives”, i.e. those COVID-19 cases who had been discharged from hospital after testing negative repeatedly and then testing positive after discharge: Lu 202018, Korean CDC33.
In a very tightly designed and argued study Lu and colleagues tested four hypotheses for the origin of “re-positives”18. After discarding the first two (re-infection and latency) on the basis of their evidence, they reached the conclusions that the most plausible explanations were either contamination of the sample by extraneous material or identification in the sample of minute and irrelevant particles of SARS-CoV-2 debris representing virus long neutralised by the immune system.
Both explanations fit the facts, the others do not. It is very likely that a huge expansion in testing capability requires training protocols and precautions to avoid poor laboratory practice which are simply not possible in the restricted times of a pandemic. We equally know that weak positives (those with high Ct) are unlikely to be infectious, as a whole live virus is the prime requirement for transmission, not the fragments identified by PCR.
The purpose of viral testing is to assess the relation of the micro-organism and hazard to humans, i.e. its clinical impact on the individual providing the sample for primary care and the risk of transmission to others for public health. PCR on its own is unable to provide such answers. When interpreting the results of RT-PCR it is important to take into consideration the clinical picture, the cycle threshold value, the number of days from symptom onset to test (STT) and the specimen donor’s age 44,42,43. Several of our included studies assessed the relationship of these variables and there appears to be a time window during which shedding is at its highest with low cycle threshold and higher possibility of culturing a live virus, with viral load and probability of growing live virus of SARS-CoV2 peaking much sooner than that of SARS CoV-1 or MERS-CoV42. We propose that further work should be done on this with the aim of constructing a calibrating algorithm for PCR which are likely to detect infectious patients. PCR should be continuously calibrated against a reference culture in Vero cells in which cytopathic effect has been observed4. Confirmation of visual identification using methods, such as an immunofluorescence assay may also be relevant for some virus types8. Henderson and colleagues have called for a multicenter study of all currently manufactured SARS-CoV-2 nucleic acid amplification tests to correlate the cycle threshold values on each platform for patients who have positive and negative viral cultures. Calibration of assays could then be done to estimate virus viability from the cycle threshold with some certainty.45
Ascertainment of infectiousness is all the more important as there is good evidence of viral RNA persistence across a whole range of different viral RNA disease with little or no infectivity in the post infectious phase on MERS46, measles 47, other coronoviridae48, HCV and a variety of animal RNA viruses48. In one COVID-19 (former) case this persisted until day 78 from symptoms onset with a very high Ct 41 but no culture growth, showing its lack of infectiousness.
We are unsure whether SARS CoV-2 methods of cell culture have been standardised. Systems can vary depending upon the selection of the cell lines; the collection, transport, and handling of and the maintenance of viable and healthy inoculated cells49. We therefore recommend that standard methods for culture should be urgently developed and external quality assessment schemes be extended to to all laboratories offering testing for SARS CoV2.50. If identification of viral infectivity relies on visual inspection of cytopathogenic effect, then a reference culture of cells must also be developed to test recognition against infected cells. Viral culture may not be appropriate for routine daily results, but specialized laboratories should rely on their own ability to use viruses as controls, perform complete investigations when needed, and store representative clinical strains whenever possible49. In the absence of culture, ferret inoculation of specimen washings and antibody titres could also be used. It may be impossible to produce a universal Cycle threshold value as this may change with circumstances (e.g. hospital, community, cluster and symptom level), laboratory methods51 and the current evidence base is thin.
We suggest the WHO produce a protocol to standardise the use and interpretation of PCR and routine use of culture or animal model to continuously calibrate PCR testing, coordinated by designated Biosafety Level III laboratory facilities with inward directional airflow52. Further studies with standardised methods51 and reporting are needed to establish the magnitude and reliability of this association.
The results of our review are similar to those of the scoping review by Byrne and colleagues on infectivity periods53 and those of the living review by Cevick and colleagues42. Although the inclusion criteria are narrower than ours, the authors reviewed 79 studies on the dynamics, load and shedding for SARS CoV-1, MERS and SARS CoV-2 from symptoms onset. They conclude that although SARS-CoV-2 RNA shedding in respiratory (up to 83 days) and stool (35 days) can be prolonged, duration of viable virus is relatively shortlived (up to a maximum of 8 days from symptoms onset). Results that are consistent with Bullard et al who found no growth in samples with a cycle threshold greater than 24 or when symptom onset was greater than 8 days, and Wolfel et al14 who reported that virus could not be isolated from samples taken after day 8 even among cases with ongoing high viral loads.
The review by Rhee and colleagues also reaches conclusion similar to ours.43
The evidence is increasingly pointing to the probability of culturing live virus being related to the amount of viral RNA in the sample and, therefore, inversely related to the cycle threshold. Thus, blanket detection of viral RNA cannot be used to infer infectiousness. Length of excretion is also linked to age, male gender and possibly use of steroids and severity of illness.
The limits of our review are the low number of studies of relatively poor quality with lack of standardised reporting and lack of gold testing for each country involved in the pandemic. We plan to keep updating this review with emerging evidence.
Conclusion
The current data are suggestive of a relation between the time from collection of a specimen to test, copy threshold, and symptom severity, but the quality of the studies limits drawing firm conclusions. We recommend that a uniform international standard for reporting of comparative SARS-CoV-2 culture with index test studies be produced. Particular attention should be paid to the relationship between the results of testing, clinical conditions and the characteristics of the source patients, description of flow of specimens and testing methods. Extensive training of operators and avoidance of contamination should take place on the basis of fixed and internationally recognised protocols. Defining cut off levels predictive of infectivity should be feasible and necessary for diagnosing viral respiratory infections using molecular tests54.
We will contact the corresponding authors of the 11 studies correlating Ct with likelihood of culture to assess whether it is possible to aggregate data and determine a firm correlation to aid decision making.
Funding
The review was partly funded by NIHR Evidence Synthesis Working Group project 380 and supported by the Maria and David Willets foundation.
Disclaimer
The article has not been peer-reviewed. The views expressed in this commentary represent the views of the authors and not necessarily those of the host institution, the NHS, the NIHR, or the Department of Health and Social Care. The views are not a substitute for professional medical advice. It will be regularly updated see the evidence explorer at https://www.cebm.net/evidence-synthesis/transmission-dynamics-of-covid-19/ for regular updates to the evidence summaries and briefs.
Data Availability
All data included in the review are from publications or preprints. All extractions sheets with direct links to the source paper are available from https://www.cebm.net/evidence-synthesis/transmission-dynamics-of-covid-19/
Authors
Tom Jefferson is a Senior Associate Tutor and Honorary Research Fellow, Centre for Evidence-Based Medicine, University of Oxford. Disclosure statement is here
Elizabeth Spencer is Epidemiology and Evidence Synthesis Researcher at the Centre for Evidence-Based Medicine. (Bio and disclosure statement here)
Jon Brassey is the Director of Trip Database Ltd, Lead for Knowledge Mobilisation at Public Health Wales (NHS) and an Associate Editor at the BMJ Evidence-Based Medicine.
Carl Heneghan is Professor of Evidence-Based Medicine, Director of the Centre for Evidence-Based Medicine and Director of Studies for the Evidence-Based Health Care Programme. (Full bio and disclosure statement here)
This work is licensed under a Creative Commons Attribution-Noncommercial 4.0 International License.
Acknowledgments
Drs Susan Amirian, Siyuan Ding, Long Rong and Sravanthi Parasato and Bernard La Scola provided additional information for this brief. Dr Maryanne DeMasi helped with reference identification.
Footnotes
3 new studies have been added to the review, identified from a 20th of August 2020 searches update 6 new studies have been added to the review, identified from a 31st of August 2020 searches update 5 new studies have been added to the review, identified from a 10th of September 2020 searches update
References




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
1
Community Reviews
0
Automated Services
55
Blogs/Media
Author Videos