
Abstract
Background Most Bluetooth-based exposure notification apps use three binary classifications to recommend quarantine following SARS-CoV-2 exposure: a window of infectiousness in the transmitter, ≥15 minutes duration, and Bluetooth attenuation below a threshold. However, Bluetooth attenuation is not a reliable measure of distance, and infection risk is not a binary function of distance, nor duration, nor timing.
Methods We model uncertainty in the shape and orientation of an exhaled virus-containing plume and in inhalation parameters, and measure uncertainty in distance as a function of Bluetooth attenuation. We calculate expected dose by combining this with estimated infectiousness based on timing relative to symptom onset. We calibrate an exponential dose-response curve on the basis of the infection probabilities of household contacts. The conditional probability of current or future infectiousness, conditioned on how long post-exposure an exposed individual has been free of symptoms, decreases during quarantine, with shape determined by the distribution of incubation periods, proportion of asymptomatic cases, and distribution of asymptomatic shedding durations. It can be adjusted for negative test results using Bayes Theorem.
Findings We capture a 10-fold range of risk using 6 infectiousness values, 11-fold range using 3 Bluetooth attenuation bins, ~6-fold range from exposure duration given the 30 minute duration cap imposed by the Google/Apple v1.1, and ~11-fold between the beginning and end of 14 day quarantine. Imposing a consistent risk threshold for the probability of infection can recommend quarantine with weaker Bluetooth signal, even when not recommended for the entirety of the infectious period.
Interpretation The Covid-Watch app is currently programmed either to use a threshold on initial infection risk to determine 14-day quarantine onset, or on the conditional probability of current and future infectiousness conditions to determine both quarantine and duration. Either threshold can be set by public health authorities.
Funding University of Arizona
Research in Context Evidence before this study
Epidemiological models suggest a benefit from smartphone-based automatic notification of exposure to Covid-19 infected individuals. Google and Apple have rolled out a privacy-preserving API with which apps can offer such notifications based on the degree of Bluetooth attenuation of a signal issued by an infected individual, its duration, and its timing relative to symptom onset in and test date for that infected individual. Apps deployed so far have focused on approximating close contact definitions of 15 minutes and a given distance such as 1 meter or 2 meters. However, Bluetooth attenuation is not a reliable measure of distance, and infection risk is not a binary function of distance, nor duration, nor timing.
Added value of this study We integrate all sources of information (including our own new experiments on the relationship between distance and Bluetooth attenuation) to provide a measure of infection risk that is as accurate as possible given the data on exposure that is available to an app based on the Google/Apple system. We also provide a method to calculate the probability of current or future infectiousness, which is a function not only of initial infection risk, but also of the number of symptom-free days since exposure, and any negative test results.
Implications of all available evidence
Our risk scoring system can guide quarantine recommendations in exposure notification apps, targeting them to individuals who are the most likely to be infected. It can also recommend release from quarantine on the day that the probability of current or future infectiousness falls below a threshold, leading to different quarantine durations for different individuals.
Background
Manual contact tracing followed by quarantine of known contacts is a critical method for containing or mitigating the spread of communicable diseases. It is, however, extremely resource and time-intensive and relies on case recall of contacts. New technologies can supplement this approach.1 Manual contact tracing can be effective for COVID-192-4, however, a significant challenge is the extremely short window of time between an infected individual presenting for testing and the contacts that they infected beginning to shed infectious virus.5,6 Automatic exposure notification approaches based on Bluetooth proximity have the potential to achieve many of the benefits of contact tracing, while also providing more rapid notification, greater privacy7,8, more objective recall of contacts including those whose identity is unknown to the case, and greater scalability.5,9 The two approaches of contact tracing and exposure notifications are complementary and may directly interact e.g. when those receiving digital exposure notifications are referred to human contact tracers for the information and support needed for quarantine adherence and further investigation.10
Apps have access to data on timing, duration, and Bluetooth attenuation. Determining the threshold for entering quarantine based on probability of infection should yield better results than from combining three binary thresholds for duration, distance, and the infectious period of the transmitter. A threshold for exiting quarantine based on the conditional probability of current or future infectiousness could also be used. Both would help optimize the reduction in disease transmission per day of quarantine recommended.
Here we lay out a framework for doing so using the decentralized protocol of the Google/Apple Exposure Notification (GAEN) Application Programming Interface (API). When a user reports positive infection status, the GAEN v1.1 framework (Figure 1) allows apps to assign a “Transmission Risk Level” to each day that they might have been shedding, and to communicate this level to the receiver’s phone via a Temporary Exposure Key (TEK). On the receiver’s device, the GAEN framework records Bluetooth attenuation as a rough estimate of distance, and the duration of exposure.

Assessment of the probability of infection following a single exposure. The calibration work is reported in this manuscript, and the procedures on the Transmitter’s and Receiver’s phones are part of the Covid Watch app.
The risk of infection depends on viral dose,11 which in turn depends on the shedding rate of the infected individual, and on the duration and distance of the interaction. As days go by without onset of symptoms, the probability of future infectiousness decreases, because the probability is conditioned on lack of symptoms for an increasing stretch of time. We parameterize calculations of both probabilities using both past literature and new experiments and illustrate what different risk thresholds imply for quarantine recommendations. We are piloting and evaluating the Covid Watch app using portions of this scheme on the campus of the University of Arizona.
Methods
The overall approach to calculating infection risk is summarized in Figure 1. Parameter values and their descriptions and sources are summarized in Supplementary Table 1 for calculations performed by the app and in Supplementary Table 2 for parameters we used during calibration.
The GAEN v1.1 framework records exposure durations only up to 30 minutes, in order to protect anonymity of COVID-positive patients by limiting the risk that users will be able guess the source of their exposure, while still meeting contact definitions that invoke minimum exposure duration of 15 minutes. Durations can be recorded separately within three bins of attenuation, thus allowing a total of 90 minutes if the attenuation varies in the necessary manner over the exposure. We calculate a weighted sum of the three durations, using the weights to capture the differences in expected dose (number of inhaled particles over an exposure time). Note that GAEN v1.5 lifts the duration cap but restricts our ability to record levels of infectiousness. We focus here on GAEN v1.1, but our scheme can be adapted for later versions.
We measured Bluetooth attenuation under GAEN v1.1 for a range of distances, phones, and scenarios of possible signal interference with the potential to affect the attenuation – distance relationship (Supplementary Materials Section 1).12 We rebalanced this dataset to form a pseudo dataset that is more representative of the distribution of barriers and scenarios in the real world (Supplementary Materials Section 1).
From this pseudo dataset, we first sample a datapoint that falls within the attenuation bin in question. If this is a zero-risk barrier scenario, we assign an infection risk of 0. Otherwise, we record the distance ρ in meters. Note that our method is not based on mapping thresholds in distance to thresholds in Bluetooth attenuation, but instead on resampling from the probability distribution of distance as a function of attenuation.
We feed this distance into a microbial exposure model that estimates the airborne spread of viral particles from an emitter’s mouth following a Gaussian plume formation, and their subsequent inhalation by contacts (Supplementary Materials Sections 2 and 3). We use a Monte Carlo approach to sample angle, exhalation rate of the transmitter, cross-section of the transmitter’s open mouth, and inhalation rate of the exposed individual, to obtain a mean dose/time for that attenuation bin. For distances ≤ 1 meter, we assume face to face interactions, consistent with distances measured for “interpersonal” interactions.13 We choose thresholds between attenuation bins, and relative risks for time spent in each bin (Supplementary Materials Section 4).
We use an exponential dose-response curve, which is derived from the assumption that each host is susceptible and that each virus has an independent probability of survival and subsequent initialization of infection.11 In our case, this probability k, multiplied by a constant C to convert from arbitrary units to number of viruses, sets the parameter λ = kC in the equation
 where expected dose D comes from a shedding rate multiplied by a weighted sum of time spent within 3 attenuation ranges. An exponential dose-response curve is superior to the approximate beta-Poisson for some other viruses (http://qmrawiki.org/content/recommended-best-fit-parameters, accessed 09/07/2020). These viruses include adenovirus, enterovirus, poliovirus, and SARS-CoV-1.
where expected dose D comes from a shedding rate multiplied by a weighted sum of time spent within 3 attenuation ranges. An exponential dose-response curve is superior to the approximate beta-Poisson for some other viruses (http://qmrawiki.org/content/recommended-best-fit-parameters, accessed 09/07/2020). These viruses include adenovirus, enterovirus, poliovirus, and SARS-CoV-1.
Our weighted sum of durations and our estimates of shedding rates S in the Results are both in arbitrary units. We therefore fit λ to obtain infection probabilities that are compatible with household spread. Asymptomatic infection and low test sensitivity can both deflate estimated household infection risks, while indirect chains of infection via a third household member can inflate them. A meta-analysis by Curmei et al.14 attempted to correct for these complications and estimated a secondary attack rate of household contacts of 30%. We assumed exposure is equivalent to 8 hours with the maximum shedding rate in the lowest attenuation and calculated λ for this dose that would result in a 30% infection risk.
Our scheme can be used either to 1) set a threshold on the initial probability of infection to trigger 14-day quarantine, or 2) set a threshold for the probability of current or future infectiousness to determine both who should quarantine and for how long. Our method for calculating the probability of current or future infectiousness, conditioned on lack of symptoms so far and incorporating the possibility of asymptomatic infection, is described in Supplementary Materials Section 5. The parameters used are summarized in Table 1. This method can be extended to inform the timing of testing and the effect of a negative test result on a recommended duration of quarantine (Supplementary Materials Section 6). Note that strictly speaking when using this latter threshold, our “quarantine” recommendations are, through their treatment of the possibility of undiagnosed asymptomatic infection, a combination of quarantine and isolation.
Our scheme, by expressing exposures in terms of probabilities of infection and infectiousness, naturally lends itself to combining risks over multiple exposures (Supplementary Materials Section 7).
Results
Our Gaussian plume model of microbial exposure produces the relationship between distance and infection risk shown in Figure 2. Training on both this and our distance-attenuation measurements (as summarized in Methods), we chose the 3 attenuation bins of ≤ 50dB (close range), 50-70dB (medium range), and >70 dB (far range), with weights 2.15, 0.79, and 0.19, respectively. Using these weights, we calibrate λ = 3.50 × 10-6 (see Methods) to obtain an infection probability of 0.30 for household contacts. Note that the best way to calibrate both weights and λ would be after the app is rolled out, with manual contact tracers compiling exposure characteristics and relating them to the rate of subsequent infection. While Eq. 5 calculates the function of an expectation rather than an expectation of a function, treating variance in dose amounts to using an “effective” value of λ (Supplementary Materials Section 8).

Expected dose and corresponding probability of infection for a 30-minute exposure, estimated using our Monte Carlo procedure as a function of distance from an infected individual. The discontinuity at 1 meter indicates our assumption that this distance threshold indicates face-to-face interaction. Faded points show doses and infection risks that would be estimated if a face-to-face or non-face-to-face interaction assumption were consistent across distances. The bolded points indicate what we assumed in our framework. Note that Bluetooth information likely contains more risk information regarding whether an interaction was face-to-face than it does about risk as a function of the distance at which either a face-to-face or a non-face-to-face interaction takes place. The WHO close contact definition invoking 1 meter also invokes face-to-face interaction.15 The same is true, only with 2 meters, for European guidance (available at https://www.ecdc.europa.eu/en/covid-19-contact-tracing-public-health-management, accessed on 7/1/2020).16 The Centers for Disease Control and Prevention (CDC)’s definition departs from this in omitting reference to face-to-face when referring to interactions occurring within 6 feet (available at https://www.cdc.gov/coronavirus/2019-ncov/php/public-health-recommendations.html, accessed on 7/1/2020).17
Bluetooth attenuation thus only distinguishes a 2.7-fold difference in dose and hence risk between close and medium range, and only 11-fold between close and far range. In contrast, informed both by TCID50 data18 and by epidemiological evidence19, we assign a 10-fold higher risk to exposures to individuals during peak shedding than during the margins of the infectious period (Supplementary Materials Section 9, illustrated in Figure 3A). The magnitude of shedding (transmission risk value) has received less attention than attenuation and exposure duration and is not to our knowledge widely used by other GAEN apps.

Examples of quarantine recommendations using a threshold for infection risk (B) vs. for current or future infectiousness (C). Shaded cells indicate that a 30-minute interaction is insufficient to trigger quarantine. A) Transmission risk levels 1-6 are used to capture the 10-fold range of relative infectiousness on different days as a function of timing relative to symptom onset. Evidence from both transmission pairs and TCID50 measurements is reviewed in the Supplementary Materials Section 9. B) The minimum length interaction needed to trigger 14-day quarantine is a function both of Bluetooth signal attenuation and of Transmission Risk Level. Approaches that neglect the latter correspond to a single row of 15 minutes, and potentially a second row of 30 minutes. C) Number of quarantine days recommended following a 30-minute interaction.
Apps can measure duration far more accurately than distance, but the GAEN v1.1 duration cap of 30 minutes, combined with the use of 5 minute or similar windows, mean that only ~6-fold differences in the risk from low-attenuation exposures are captured in this way, or up to 8.6-fold when stochastic variation in attenuation over time also shows up at lower attenuations, or much longer in GAEN v1.5 where there is no cap on duration.
The relatively low predictive power of Bluetooth attenuation gives rise to diagonal patterns in the quarantine recommendations in Figure 3B. These diagonal patterns mean that quarantine will sometimes be recommended following prolonged exposure to a high shedder, even if the interaction took place at well beyond the estimated 2 m. distance. However, these exposures are not risk-free either, in particular if taking place in an indoor environment, especially in cases with heavy breathing, such as exercise environments20 or choir rehearsals,21 where aerosols may mix throughout the room and also deposit on surfaces. The diagonal pattern reflects the compelling evidence that exposure timing and duration also significantly contribute to infection risk. We therefore sometimes recommend quarantine recommendation even when Bluetooth attenuation, which is a poor proxy for distance, is not low. However, Bluetooth attenuation is nevertheless critical to concluding that an interaction occurred at all.
So far, we have estimated the probability of infection from an exposure. Each day that passes without symptoms provides more information to make infection less likely, and eventually also to increase the probability that shedding from an asymptomatic infection has ended. To calculate the probability of current or future infectiousness on a subsequent day, conditional on no symptoms until that day, we apply a discount factor based both on time elapsed without symptoms and also any negative test results (Supplementary Materials Sections 5 and 6). We multiply the probability of infection from an exposure by this discount factor to determine the remaining risk of infectiousness from a given exposure.
Traditional quarantine guidelines are binary (either 14 days from date of last exposure, or no quarantine required). However, a consistent approach to risk, combined with a desire to impose quarantine days in the most efficient manner possible to combat disease spread, suggests that individuals should quarantine for longer following a higher-risk exposure (Figure 4A) (although see Supplementary Materials Section 5 for a caveat with very high doses). This approach calculates the number of days post-interaction that would be needed to drop below a given threshold of probability of current or future infectiousness. Exposure scenarios of 30 minutes are illustrated in Figure 3C.

Applying a consistent risk tolerance for current or future infectiousness causes quarantine duration to be a function of initial risk, of the tolerated degree of risk, of the fraction of infections that are assumed to be asymptomatic, and of any negative test results. A) Initial infection risk is 1.12% following 15 minutes of close contact with an individual around the time of symptom onset. With a 20% asymptomatic fraction, a 14-day quarantine is recommended under a 0.13% risk threshold, but only a 7-day quarantine under a 0.5% threshold. Following a lower risk exposure with 0.2% infection risk, quarantine would be 5 days with the stricter threshold, and there would be no quarantine with the less strict. B) Quarantine must be longer to mitigate a high likelihood of asymptomatic infection in the exposed individual. C) A negative test result, shown here as taking place on Day 5, can shorten quarantine, in particular mitigating the risk of asymptomatic infection. We apply Bayes theorem with 70% sensitivity and 100% specificity. Note that widespread availability of testing would allow much stricter risk thresholds to be used. Day 0 is included in the total quarantine times.
We used a 0.13% threshold in Figure 3C, because it recommends a 14-day quarantine for 15 minutes in close range with a high shedder. Such an interaction has a 1.12% infection risk, which falls below a 0.13% probability of current or future infectiousness after 14 days of quarantine during which no symptoms appear. Note that this initial infection risk is broadly compatible with the attack rate reported in Taiwan (1.0%, 95% CI: 0.6-1.6%) for those interacting with infected individuals in the first 5 days of symptom onset,22 which is similar to the 1.9% attack rate (95% CI 1.8%-2.0%) reported in South Korea.23
Current advice treats the larger risk of longer exposure the same, making a 0.13% threshold more conservative because it is calculated to generate a 14-day quarantine for a minimal duration of exposure. However, this is offset by our assuming maximal shedding in calculating this benchmark example. In other words, while this threshold approximates the risk tolerance of current advice, the details of who is recommended for quarantine and for how long will be different in our quantification of total risk than it would be if we were to combine independent binary thresholds for infectious period of transmitters, duration of exposure, and distance to produce a quarantine duration of uniform length. This leads to more consistent treatment of risk to yield the greatest benefit in terms of transmission prevented per day of quarantine recommended. Shorter quarantines might significantly reduce the harms imposed by quarantine,24 and increase compliance25 (although see McVernon et al26). Quarantining for 14 days post-exposure may be exceptionally challenging for essential workers, individuals without sick leave, or those who would endure significant financial hardship due to lost income.
The assumed fraction of asymptomatic infections affects the discounting of risk. The symptomatic fraction is discounted according to the distribution of incubation periods from exposure to symptom onset, while releasing the asymptomatic fraction from quarantine is not safe until not only onset, but also shedding is over (Supplementary Materials Section 5). Our calculations so far assume that 20% of infections are asymptomatic. If we instead assume that 50% infections are asymptomatic, e.g. in a young age group, even a 15-minute contact registered as low attenuation and with peak shedding in the transmitter would require a 16-day quarantine to meet a 0.13% threshold (Figure 4B). However, if an individual were to test negative during their quarantine, their conditional probability of current or future infectiousness would drop, shortening their quarantine to 13 days for a test with 70% sensitivity (Figure 4C).
Discussion
Here we quantify relative risk of infection using experiments to inform the noisy distance-attenuation relationship, and Monte Carlo simulations to inform both this and other sources of variability and uncertainty that affect risk. We roughly calibrate relative infection risk to absolute probability of infection based on limited information from the infection probability of household contacts.
Errors in calibration are likely but will generally not affect the rank order of risks. For example, adjusting the risk threshold of 0.13% for quarantine will have similar effects to adjusting the value of A. Knowledge of absolute vs. relative risk does have some effect once some saturation in risk begins to occur, little of which will occur unless much longer durations are recorded.
With 20% cases being asymptomatic and no testing, the risk of current or future infectiousness falls ~11 -fold over the first 14 days of quarantine. Under GAEN v1.5, risk will sometimes differ more between two individuals entering quarantine than when comparing the same individual before vs. after a 14-day quarantine. For this reason, our scheme could recommend quarantines longer than 14 days. Variation in quarantine length is to be expected – if total risk is scored consistently, some quarantines will be longer and others shorter, in order for residual infection probability, conditional on time elapsed without symptoms, to fall below a threshold.
The Covid Watch app is currently programmed either to use a threshold on infection risk to determine 14-day quarantine onset, or on risk of current and future infectiousness to determine both quarantine and duration. Either threshold can be set by public health authorities flexibly in the light of external factors such as level of community transmission, jurisdictional comfort with uncertainty related to digital exposure notifications, and current public health science and recommendations. Communities that have achieved containment might choose to set a stricter threshold, testing individuals once or twice to lower their risk following each negative test.
Communities with high prevalence might raise the threshold if it seems likely that the number of quarantine recommendations being issued by the app will cause it to fall out of use. Note that the maximum possible initial infection risk in our v1.1 scheme is 3.23%; relaxing the 30-minute cap on durations, while maintaining infectiousness information, would be necessary in order to get resolution among higher risks. The effects of this problem are partly ameliorated by using the variable quarantine duration approach (Figure 3C). When a threshold is set well below the probability that a randomly chosen member of the population is currently infected, it should be recognized that individuals agreeing to download and comply with the recommendations of the app are implicitly agreeing to adhere to higher standards than those implied by the current absence of a general stay-at-home order. At the time of writing (September 5), the rate of current infection is ~1% in Arizona.27
When the infection risk of the average person in the population is high, we believe that the best solutions are population-level restrictions and closures. Under these circumstances, a GAEN app might still have utility for essential workers. However, a GAEN app could be an inferior but still useful option should the political will for population-level restrictions not exist.
As the conditional probability of current or future infectiousness (conditioned on the exposed individual being asymptomatic) falls throughout their quarantine period, messaging can also change. E.g., during the initial high risk days, users might be offered concrete resources such as grocery delivery, or the option to quarantine in a specialized facility in order to protect other household members, before transitioning to self-quarantine once risks falls. Even with self-quarantine, an app might identify the days on which staying home is the highest priority (I.e. days where the potential infectivity may be highest). Messaging considerations are discussed in Supplementary Material Section 10.
We caution that our derived relationship between Bluetooth attenuation and infection risk is extremely approximate and model-dependent. We have more confidence in our settings of Transmission Risk Levels for symptomatic cases, but very little for asymptomatic cases. These parameters need to be calibrated with real world data on app users who report their app-recorded exposures to manual contact tracing efforts, who then track which users go on to test positive, and who are therefore able to mine the data to quantify the quantitative relationship between exposure details (duration, attenuation, Transmission Risk Level) and probability of infection. Transfer of this data to manual contact tracers’ contact management databases is critical to improve the targeting of quarantine recommendations to those at highest risk of being infected, which will make most efficient use of each day of quarantine recommended to reduce transmission.
Short of this, more quantitative data on infectivity would be extremely valuable. Our determination of shedding duration partly relies on the prospective sampling of all individuals in a skilled nursing facility28, where many patients subsequently got sick. Daily samples during similar outbreaks could be used to quantify how shedding varies both among individuals and as a function of time relative to symptom onset. TCID50 data would be ideal, but even Ct values can be valuable for this purpose. However, the fact that the settings we originally chose based on infectivity data agreed with later and improved epidemiological approaches19,29 is encouraging.
Without extended durations, our default calibrations will not recommend quarantine (Figure 3B) or extended quarantine (Figure 3C) for lower Transmission Risks. However, with the duration cap lifted in a GAEN v1.5 or later, 43 minutes in the ≤50 dB range, 1.92 hours in the 50-70 dB range, or 7.93 hours in the >70 dB range with an individual of transmission risk level 2 would be required. However, GAEN v1.5 does not quantify infectiousness, and GAEN v1.6 re-introduces only two levels of infectiousness. Limited durations and infectiousness information have been driven by privacy concerns, but this must be weighed against the significant ethical considerations in favor of efficient allocation of quarantine.30 In Supplementary Section 10, we suggest an alternative method to preserve anonymity, which is to conceal all exposure details from the user’s view. When using variable quarantine duration, this also effectively conceals the date of exposure.
Our framework can be used not only to guide recommendations for who should quarantine and for how long, but also to allocate associated resources including quarantine facilities, grocery delivery and other social support, and priority for access to scarce tests. Both manual contact tracing and digital exposure notification require rapid testing to be effective. Given limited tests, targeting those at highest risk of infection will do the most good in finding new positive cases who are early enough in the course of infection for these approaches to stem transmission the most.
Data Availability
Supplementary Data Table 1 provides the alpha test data used to calibrate our weights.
Code Availability
Code and necessary data are accessible under a Creative Commons license at https://github.com/awilson12/risk_scoring
Competing Interests
JIP, ZS, MX, SH, TW, and JM are members of Covid Watch, a 501 (c)(3) non-profit developing open source code software for exposure notifications. The organization is also involved in providing commercial solutions around the technology.
Author Contributions
JM conceived the overall risk scoring approach and oversaw all aspects of the project. AMW, PIB, and JM designed the Gaussian plume component, and AMW implemented it. JM and AMW reviewed the literature to choose Transmission Risk Levels. JM designed and implemented the variable quarantine approach. MX and JMc designed and managed the alpha testing. JIP preprocessed and cleaned the alpha test data. YC and YJS designed and performed people traffic simulations to inform a realistic distribution of distances. NA implemented the rebalancing procedure to reflect that distribution, and performed sampling to choose weights. AMW and JM calibrated the dose-response curve and NA explored its sensitivity to variance in dose. JIP, ZS, SH, and TW designed and implemented the core components of the Covid Watch app used in the alpha testing. JIP modified the app to obtain high resolution attenuation data. ZS provided up-to-date guidance about what is possible under GAEN, and checked calculations. PIB and KCE provided input on all public health aspects of the research. AMW and JM wrote the first draft of the manuscript, followed by significant input from PIB and KCE.
Supplemental Materials for
Parameter values used by app to calculate risk
Parameter values used by us to calibrate parameter values in Table 1
1.0 Experiments on Distance-Attenuation Relationship
Using a developer version of the Covid Watch app, we called the API multiple times with different attenuation thresholds in order to achieve resolution of 3dB in the 30dB-99dB range. The API appears to round up durations to 5-minute increments, each with its own attenuation value; we consider each of these to be a datapoint. Our tests were all short, e.g. a 12-minute test would yield 3 datapoints.
There were 7 testers and 14 phones, representing a variety of models, all of iPhones – handset type and orientation can affect signal.14 49 measurements were taken with specific phone orientations, while for the remaining 986 the devices were side-by-side and facing upwards if not otherwise specified by the barrier type (e.g. pocket). 203, 222, 199, 374, 17, 20 measurements were at 0.5m., 1m., 1.5m., 2m., 3m., and 5m., respectively. We also used the 28, 28, 29, 27, and 16 zero-risk barrier measurements at 0.5m., 1m., 1.5m., 2m., and “N/A”, respectively. Note that improvements made in GAEN v1.5 are expected to improve our ability to estimate distance as a function of attenuation. While useful, we note that new experimental data would be required for recalibration. The imbalanced nature of the collected data, with few long distance measurements and no Android measurements, reflects the fact that the decision was made to recommence once v1.5 was available, whose calibration will be both qualitatively and quantitatively different.
1163 out of the total 1558 datapoints were used for attenuation weight and attenuation threshold setting, with exclusions of data described in Figure S1. The 1163 non-excluded datapoints are supplied in Supplementary Dataset 1. Of the included 1035 attenuation measures that involved infection risk, 747 did not include a deliberate barrier, while 288 includes barriers such as pockets, backpacks, nearby laptop, and human body. 925 measures were taken inside homes, 49 were taken inside an elevator, and 61 outside.

Attenuation data cleaning
*A few attenuation values were implausibly low, always representing one such increment per device per series of attenuation values corresponding to a single test. We believe this is because these testers used the dropdown menu to turn off Bluetooth rather than going to Settings, and this only disables existing Bluetooth connections, causing an anomalously strong signal to be recorded during the period in which the test was being set up. We manually annotated these, totaling 144 datapoints, and excluded them from further analysis, yielding 1414 datapoints.
**Distance is not needed for the 128 datapoints taken in the presence of a risk-blocking barrier (e.g. closed car doors or walls), so points marking “N/A” for distance were not excluded for any of these.
To rebalance the distance measurements, we created a pseudo-dataset with different multiples of the data collected at each of the distances. To inform the desired distribution of distances, we analyzed the time-weighted pairwise distance in traffic flow simulations of a classroom.15 These indicate a roughly uniform distribution over possible distances, with a reduction in close contact due to attempts to adhere to social distancing rules. Since close contact might be more common in other settings, and distances beyond 5m. can also register Bluetooth signal, we made 5, 5, 6, 3, 132, and 168 copies of the non-zero-risk data at distances of 0.5m., 1m., 1.5m., 2m., 3m., and 5m, respectively, yielding a data ratio of 1015: 1100: 1194: 1122: 2244: 3360 (as a rough approximation of a target ratio of 1:1:1:1:2:3) prior to the sampling described below. To this, we added 4 copies of the zero-risk barrier measurements, so that they made up 4.85% of the total pseudo-dataset.
Our calibration code holds shedding rate and exposure duration constant at 50 arbitrary units/m3 and 30 minutes, in order to isolate the effect of distance on differences in dose between attenuation buckets.
2.0 Estimation of Exposure Concentrations
It is well-acknowledged that both distance from an infected individual and duration of “close proximity interactions”16 are important parameters in estimating the probability of infection of those exposed.17-20 However, there is little quantitative information about the relationship between distance and risk of infection. Chu et al. (2020)18 quantified risk in terms of answers to binary survey questions about whether the respondent came within distance X of an infected person. They found that the value of the threshold distance X in the survey question predicts the degree to which the answer predicts risk, but this relationship cannot easily be converted into one between actual distance and risk.
For this reason, we instead model the dose inhaled at different distances. Exhaled breath is a likely source of infection.21,22 Accordingly, we model a Gaussian plume23 of virus-containing aerosols originating from the emitter’s face at (0,0,0). The x axis represents the direction that the transmitter is facing and breathing toward with breath velocity U (m/s). Diffusion causes spread away from y=0 or z=0. The viral concentration is then


 where Q is virus emitted per second and is equal to the product of shedding rate, S, (in arbitrary units proportional to copies/m3) and an exhalation rate, X, (taken from measured inhalation rates in m3/s), yielding arbitrary units proportional to copies per second being generated (eq 1.1). We sample our exhalation rates from a normal distribution of inhalation rates with a mean and standard deviation of 16.3 and 4.15 m3/day, respectively. These were informed by the 16-21 year old range from Table 6-1 in the Exposure Factors Handbook (2011).10 To avoid negative exhalation rates, this distribution was left-truncated at 9 m3/day, the smallest fifth percentile of inhalation rates for males and females in age ranges overlapping with the 16-21 year old range.10 The velocity of breath U (m/s) was determined by dividing the exhalation rate (m3/s) by the cross-sectional area of an open mouth A (m2), which is the area over which air is assumed to be exhaled at the plume source. The cross-sectional area was informed by a uniform distribution with minimum and maximum cross-sectional areas measured for an open mouth with a “large bite” configuration, ranging from 23 to 59 cm2.11 Note that for a steady-state plume assuming a continuous output of virus, the effects of the exhalation rate (volume of air per second) on amount of virus emitted, and on the velocity with which they disperse, cancel out. For an abrupt exhalation such as a cough, rather than steady state, a higher exhalation rate would affect viral airborne concentration.
where Q is virus emitted per second and is equal to the product of shedding rate, S, (in arbitrary units proportional to copies/m3) and an exhalation rate, X, (taken from measured inhalation rates in m3/s), yielding arbitrary units proportional to copies per second being generated (eq 1.1). We sample our exhalation rates from a normal distribution of inhalation rates with a mean and standard deviation of 16.3 and 4.15 m3/day, respectively. These were informed by the 16-21 year old range from Table 6-1 in the Exposure Factors Handbook (2011).10 To avoid negative exhalation rates, this distribution was left-truncated at 9 m3/day, the smallest fifth percentile of inhalation rates for males and females in age ranges overlapping with the 16-21 year old range.10 The velocity of breath U (m/s) was determined by dividing the exhalation rate (m3/s) by the cross-sectional area of an open mouth A (m2), which is the area over which air is assumed to be exhaled at the plume source. The cross-sectional area was informed by a uniform distribution with minimum and maximum cross-sectional areas measured for an open mouth with a “large bite” configuration, ranging from 23 to 59 cm2.11 Note that for a steady-state plume assuming a continuous output of virus, the effects of the exhalation rate (volume of air per second) on amount of virus emitted, and on the velocity with which they disperse, cancel out. For an abrupt exhalation such as a cough, rather than steady state, a higher exhalation rate would affect viral airborne concentration.
For interactions ≤ 1m, we assumed two people interacting are directly in front of each other along the x-axis (φ = π /2, θ=0). For interactions beyond the close range (>1m), we sample θ from a uniform 360 degrees (min=0, max=2π), and the angle between the z axis and the xy-plane, φ, was randomly sampled from a triangular distribution (min=π/4, mode=π/2, max=3π/4). We then convert from spherical units to (x,y,z) to apply Eq. 1. We assumed that scenarios where the person exposed was behind the emitter (x<0) resulted in a zero dose.
To capture the shape of the plume, we use:


Assuming moderately stable conditions, Iy and Iz were randomly sampled from uniform distributions with minimums and maximums of 0.08-0.25 and 0.03-0.07, respectively.12
We note that inhalation and exhalation rates are both likely important to risk. For example, one infected dance instructor spread COVID-19 to 7/26 other instructors at a four hour workshop,24 representing a similar risk as for household contacts, despite the presumption that most were at >2 m. distance for most of this time. Limited air circulation or increased respiratory rates are important factors that cannot be captured in the current GAEN approach, but the four-hour duration of the workshop could be, combined with considerable uncertainty in the relationship between Bluetooth attenuation and distance, in order to correctly capture the high risk of such a scenario.
While wind velocity and relative humidity are important factors for determining droplet and fine aerosol dispersion and deposition,25,26 as is mask usage, these are uncertain factors that are not recorded by the app, especially considering that interactions may occur indoors or outdoors. By not accounting for deposition, and by assuming that masks are either not worn or not worn effectively, we will tend to overestimate dose at greater distances, and in the presence of masks. This will implicitly lower the app-imposed risk tolerance of individuals who comply with public health guidelines that recommend masks and physical distancing, and who might therefore also be more inclined to comply with quarantine recommendations. The 2-meter rule was based on the assumption that most transmission is via droplets (large aerosols) for which deposition occurs over this distance. However, there is increasing evidence for transmission via smaller aerosols,27-31 supporting our assignment of some risk to greater distances, reflecting short-to medium-distance airborne transmission.
3.0 Inhalation Dose per Interaction
An inhaled dose of viral particles due to person-to-person interactions was estimated based on the duration of the interaction (minutes) (T), the concentration of virus in the air at this {x,y,z} coordinate during the interaction (arbitrary units of viral particles/m3) C (x, y, z), and inhalation rates (m3/minute) (/),

Inhalation rates were randomly sampled from the same distribution as exhalation rates but allowing for a different value per iteration. As with exhalation rates, we left-truncated the distribution to avoid negative inhalation rates and therefore negative doses. Figure 2 shows the expected dose as a function of distance, with a discontinuity at 1m. arising from our assumption that this distance or below indicates face-to-face interaction.
4.0 Setting attenuation bin thresholds and corresponding weights
To select the threshold values (a, b) demarcating 3 attenuation bins, we optimized the differences in mean dose between two randomly sampled attenuation measurements. Specifically, we maximized the value of
 where A, B and C are the average doses D from Eq. 4, averaged across Monte Carlo sampling described above, corresponding to bins [0, a], (a, b], and (b, +), and pA, pB, and pC are the probabilities that an attenuation will fall within that bin in our pseudo dataset.
where A, B and C are the average doses D from Eq. 4, averaged across Monte Carlo sampling described above, corresponding to bins [0, a], (a, b], and (b, +), and pA, pB, and pC are the probabilities that an attenuation will fall within that bin in our pseudo dataset.
We examined multiple local maxima of this distance measure before choosing a partition pair. We also investigated alternative versions of a distance metric and alternative rebalancing schemes, to confirm that this is a relatively robust partition pair.
5.0 Probability of Current or Future Infectiousness
To calculate residual risk of infection as a function of initial risk plus time since exposure, we use the probability distribution of incubation periods from Lauer et al.7, available at https://iddynamics.ihsph.edu/apps/shiny/activemonitr/. Note that it is possible that incubation periods are even more dispersed than reported here32; this would lengthen quarantine recommendations.
To calculate risk of current or future infectiousness, we assume a fraction of symptomatic vs. asymptomatic cases and take an average of the discount factors applying in each case. Across a population, 20% of infections are estimated to be asymptomatic.34 Younger users are more likely to be asymptomatic33, so the fraction of asymptomatic cases could be personalized on the basis of user age if that information is collected on a voluntary basis. For the symptomatic cases, we discount according to the probability of subsequently developing symptoms, given that symptoms have not appeared yet.
For the asymptomatic cases, we combine the incubation periods from Lauer et al.7 with a distribution of shedding durations. Long et al.8 report slightly longer shedding durations for asymptomatic than symptomatic shedding, but other studies34-38 for which we were unable to obtain the data, report the opposite, or no difference. Shedding declines in magnitude post symptom onset and is considered by the CDC to have reached negligible levels by 10 days post symptom onset. We assume that asymptomatic shedding begins 3 days before what would have been the day of symptom onset if symptomatic, or else immediately upon infection, whichever occurs later.
Using this assumption, we calculated the probability distribution of the day that shedding ends, given both the distribution of incubation periods and a distribution of shedding durations. For the latter, we combine the asymptomatic and symptomatic shedding durations of Long et al. but on the basis of CDC advice for isolation, we truncate the distribution so that all shedding periods longer than 12 days are recorded as exactly 12 days.
Note that low dose exposures, e.g. to asymptomatic individuals, may result in longer incubation periods,32 suggesting that low initial risk scores should have longer rather than the shorter quarantines we calculate using this method. We currently ignore this by assuming that risk scores primarily capture uncertainty in the likelihood of infection with a minimal dose, and not variation in the infecting dose once above the minimal. To see how this assumption arises from our model, note that the exponential dose-response curve we use assumes that each virus has an independent probability of initiating infection. Under the resulting Poisson distribution for the number of viruses responsible for the initial infection, then even for the 30% infection rate of household contacts, the probability that infection is initiated with two or more viruses is only 5%, and with three or more viruses is only 0.6%. However, the higher variance in dose explored in Figure S2 could make initiation with multiple viruses common enough to matter for high infection probabilities. In this case, our simplifying assumption might require overly long quarantines following very high risk exposures. However, unless the variance is extreme, it might not significantly distort estimated probabilities among the range of lower risk exposures. We note that lognormal distributions of incubation periods with substantial variance occur even in the absence of variation in dose, due both to variance in within-host replication rate and to the stochastics of establishing infection in the first cells.39
6.0 Negative Test Results and Recommending a Day for Testing
Incorporation of negative test results can help exclude asymptomatic infection and hence allow for earlier release. From Bayes Theorem, and taking the false positive rate as negligible, a negative test result changes the probability of infection from p to  , where E is the false negative rate. This could be taken as 0.3 40,41 or made dependent on the timing of the test relative to exposure,42 which would require distinct application to each of multiple exposures.
, where E is the false negative rate. This could be taken as 0.3 40,41 or made dependent on the timing of the test relative to exposure,42 which would require distinct application to each of multiple exposures.
Kucirka et al.42 report a false negative rate as a function of the timing of a PCR test relative to symptom onset, but most of the data is post-symptom onset, with only a single patient’s data informing false positive rates prior to symptom onset. If sufficient data on false negative rates pre-symptom onset became available on a larger number of patients, it could be combined with the distribution of incubation periods to calculate the false negative rate as a function of time since exposure. Before use as E in Bayes Theorem above, it can be adjusted in a form of survivorship analysis; if testing is conditional on no symptoms to date, then the ratio of pre-symptomatic: asymptomatic individuals in the reference group will depend on time since exposure. Time-dependent false negative rates could then be used to recommend an optimal day for testing. For example, we could choose the days on which the probability of obtaining positive test results is highest.
We calculated this probability as the sensitivity on that day × the conditional probability of infection on that day given no symptoms to date. Given exposures on multiple days, the sum of this product can be computed to choose a date for testing. Alternative criteria for optimization could also be devised, e.g. explicitly prioritizing highly exposed individuals whose calculated quarantine in the absence of a test would exceed 14 days, or assigning a value to testing immediately after quarantine begins, in the service of rapid tracing of that individual’s contacts should they test positive.
7.0 Multiple Exposures and Total Risk
GAEN v1.1 will not record either a single long exposure or multiple exposures from a single individual beyond the 30 minutes cap for each of three attenuation bins, although this has changed in v1.5. However, it will record exposures happening on different days (considered to change at midnight UTC) as independent exposures. To calculate total risk, we combine the probabilities pi of each exposure i, each discounted as described in the section above, as  .
.
Figures 3 and 4 illustrate scenarios of a single exposure. When there are multiple exposures, quarantine durations are determined with respect to total risk. The risk threshold for initiation and completion of quarantine are the same. In other words, risk is treated in an internally consistent fashion to achieve the maximum possible benefit from a given number of recommended quarantine days across a population. When fixed quarantine durations are used, exposure must be significant on a single day, from which the 14 days are then calculated, and risks are not integrated across multiple days.
8.0 Variance in Dose
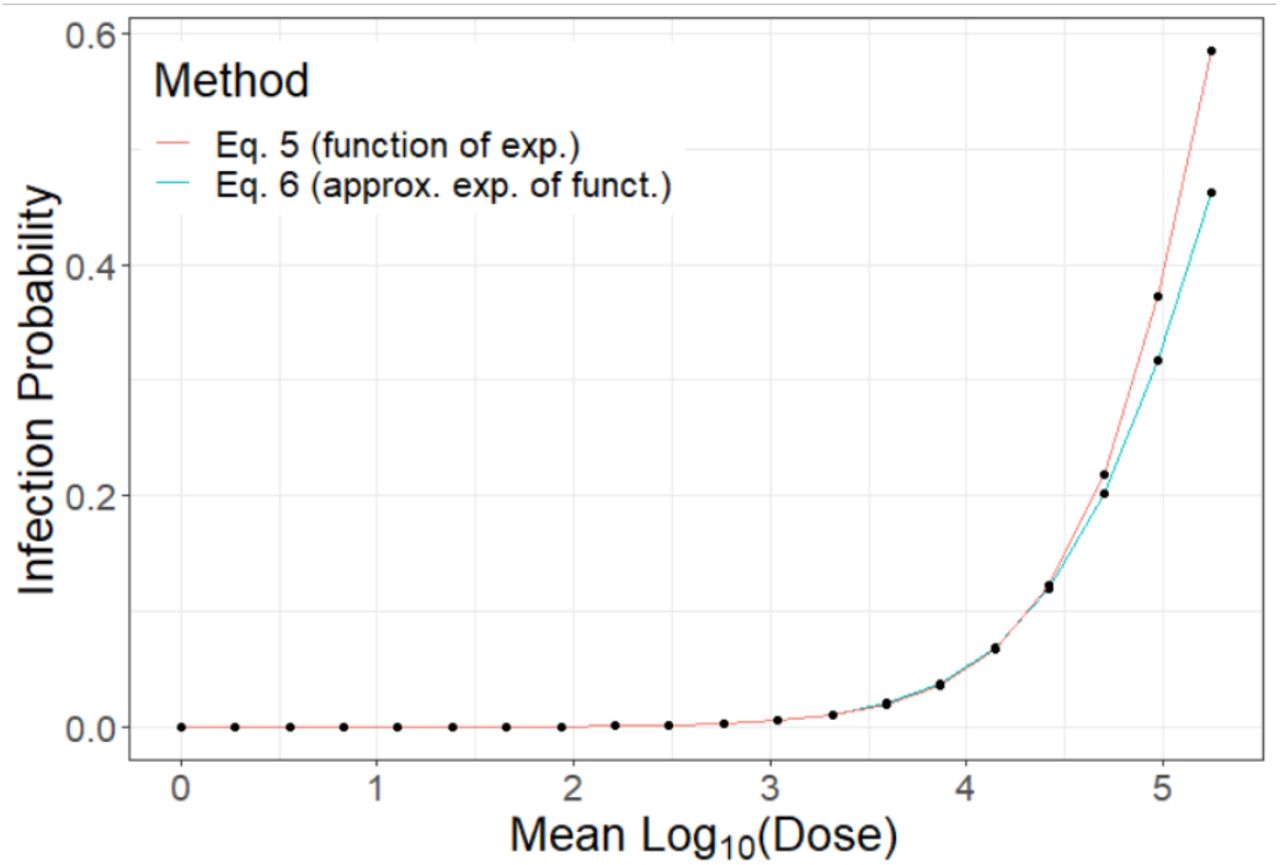
Our dose response curve is actually the probability of infection as a function of the expectation of dose, rather than dose. To consider the effect of variance in dose, we note that while E [1 – e-λD] is analytically intractable with respect to a log normally distributed dose, there is a viable saddle point approximation described by Rojas-Nandayapa (2008) While Eq. 5.6 in Rojas-Nandayapa contains a typo, we use the method given to derive
 where LW (x) is the Lambert-W function.
where LW (x) is the Lambert-W function.
Using this approximation, or the associated importance sampling method (Asmussen et al., 2016) which yields similar results, we can compare the shape for the dose response curves and consider whether an “effective” λ will perform acceptably. Ct counts in Long et al. (2020) have a standard deviation ~4, representing an upper bound of a 16-fold difference in viral load, because a difference of 1 Ct in PCR measures represents at most a 2-fold difference in underlying viral load, and because individuals are not sampled at exactly comparable times with respect to the timecourse of shedding. However, variance in dose from causes other than infectiousness, e.g. the intimacy of contact, is not included. With a standard deviation representing a 16-fold difference, we find that by using a value 3710th of λ = 3.50 E — 06, we can super-impose the two curves up to 20% infection probability (Figure S2).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Although our dose-response curve takes the function of an expectation, for low infection probabilities the effect of this is to change the interpretation of the value of λ, which is 3.50 × 10-6 when using Eq. 5 but 0.3 times this value when using Eq.6 with a distribution of log-dose with standard deviation corresponding to a 16-fold difference in dose.
9.0 Transmission Risk Levels
Transmission risk level in the GAEN API is a proxy for the magnitude of viral shedding and can be set by the app on the basis of a simple questionnaire administered to users reporting a positive diagnosis. We use this to inform expected shedding S.
The first question we ask to inform transmission risk levels is, “What day did your symptoms start”? A curve fit to known transmission events suggests peak transmission the day before symptom onset, and essentially no transmission more than three days before symptom onset.43 However, this might be confounded with behavioral changes with symptom onset, with ascertainment bias in terms of which transmission events are easiest to document, with onset of mild symptoms being overlooked and the later onset of more severe symptoms instead being reported, with possible errors in the direction of transmission given the variability of incubation periods, and with assumptions regarding the shape of the curve. Worse, the analysis appears to have significant technical flaws.4
A second source of information is quantitative polymerase chain reaction (PCR). However, this may reflect non-infectious viral remnants, especially late in the course of disease, where the proportion of culture-positive PCR results tends to decrease.1,2 However, this decline is also expected from a simple dose-response curve, where the probability of culture-positivity decreases as the amount of shedding decreases late in infection, i.e. the decline in infectivity might be quantitative rather than qualitative.
While informed by the two sources of data above, we focus the most on data in which virus was successfully cultured from patient samples, as a clear indication of infectivity. Arons et al. 2 took prospective samples throughout a nursing home, and were able to culture virus from six days before symptom onset until nine days after symptom onset, with little quantitative trend in shedding rate conditional on a positive test. In hospitalized patients, Wölfel et al. 3 were unable to isolate live virus from cultures more than 8 days post symptom onset, despite PCR evidence of high shedding. In one case report, live virus has been isolated 18 days after symptom onset, but this seems to be an outlier.44 Bullard et al. 1 quantified both TCID50 and PCR for 7 days post symptom onset, and saw an approximately 10-fold decline in infectious dose. We note that culture methods may not be sensitive enough to capture low concentrations.2 We nevertheless use this TCID50 data as motivation in assuming a 10-fold dynamic range in shedding rates as a function of day relative to symptom onset. More studies measuring infectivity in a quantitative manner are needed, particularly in populations that represent a broader base of cases of varying ages and health status. Encouragingly, our settings based on culture data agreed with those from epidemiological modeling after corrections to the latter were made.4 We slightly tweaked our settings for pre-symptomatic Transmission Risk Levels to agree with later epidemiological work.45
A final source of information comes from detailed Taiwanese contact tracing46, who found a 1.0% symptomatic attack rate (95% CI 0.6-1.6%) for those exposed within five days of symptom onset, and 0% (95% CI 0-0.4%) for those exposed after. Risk from exclusively pre-symptomatic exposure was 0.7% (95% CI 0.2%-2.4%). German contact tracing also points to highest transmission risk around the time of symptom onset.47
We use 6 of the 8 Transmission Risk Levels in the GAEN API to capture this range, evenly spaced on a log scale between 10 and 100 in arbitrary units, reserving the use of levels 7 and 8 for individuals for testing purposes and any future functionality. Transmission risk levels could also be manipulated for testing purposes, e.g. to help learn, if individuals voluntarily enter exposure details into a manual contact tracing database, how transmission risk varies in the real world, rather than just in TCID50 studies, as a function of a symptomatic status and time. We note that Transmission Risk Levels have been deprecated in the announced GAEN v1.5, and replaced with only two possible levels of infectiousness in v1.6. While the functionality of v1.1 should be preserved, we note that usage of Transmission Risk Levels would need to be standardized across different apps in order to ensure interoperability. In the description below, we outline not just our use of v1.1, but also the use we would make of six levels of infectiousness if they were to again be made available in a future API version. The assignments we use in this framework can of course be improved as more data become available. Our call for more than two levels of infectiousness comes from the fact that a systematic 10-fold difference in TCID50 has been observed, and that such a large difference seems to warrant more levels.
Based on a holistic reading of the four sources of evidence described above, we assign the maximum level of 6 from one day pre-symptom onset to two days post-symptom onset. Five days before symptom onset we assign level 1, four days before we assign level 3, three days before level 4, and two days before level 5. Three days after symptom onset we assign level 5, four days after level 4, five days after level 3, 6-7 days after level 2, and 8-9 days after level 1. Our termination at 9 days is based on current CDC guidance.9
For users who report a positive test but no symptoms, there is likely a reason they were tested, and so we ask for the most likely day of exposure, if known. If provided, we assume that shedding did not begin until two days after exposure, at the earliest. We also ask for the date of sampling for the positive test (which can be reported by the healthcare provider rather than the app user) and assume peak shedding at around this time. Subject to the constraint from day of exposure, we assign Transmission Risk Level 3 to dates within with one day of the test, and level 2 to dates between 2 and 4 days of the test, although as discussed below, one study reports substantially longer shedding than these 9 days.8 There is some evidence that viral shedding is lower in asymptomatic vs. symptomatic cases,48 while another study indicates the shedding magnitudes may be similar.49 Note that we assume that those with no symptoms at the time they receive a positive test result are asymptomatic rather than pre-symptomatic – should test turnaround times be sufficiently fast, it would be useful for users to be able to report symptom onset after the fact and trigger a change to previously reported Transmission Risk Levels, and we recommend that this functionality be added, together with restoring a greater number of Transmission Risk Levels, in future versions of the GAEN framework.
10.0 Considerations in recommending and messaging variable quarantine durations
The need for consistent guidance to the public is an important consideration for implementing tailored risk scoring and modified quarantine recommendations. If for the sake of a consistency, a public health authority is not willing to authorize variable quarantine recommendations, as is currently the case in Arizona, but only 0 or 14 day quarantines from time of the last individually significant exposure, then the threshold for going into quarantine at all would need to become more strict in order to maintain the same overall risk among the population under quarantine. In other words, retaining the same average probability of current or future infectiousness among the quarantined population would require some exposed individuals to no longer go into quarantine at all, in addition to others lengthening their quarantine out to 14 days. With a binary 0 or 14 day quarantine, the amount by which disease transmission is prevented per day of quarantine will be lower.
Alternatively, to avoid mixed messaging regarding quarantine even while the app recommends quarantine of variable duration, one option is to suppress all details about individual exposures from the user’s view, including their date. This has the additional advantage of decreasing the risk that users will be able to guess who exposed them, further preserving privacy.
The app can communicate the risk of infectiousness either as a simple recommendation for which days to quarantine, or also as a quantitative score in order to “game-ify” the process of quarantine and give users positive feedback for each day they succeed in remaining at home until risk falls to a lower level. Further research is needed to assess the most effective messaging strategies. E.g., the app could display both current and projected risk of infectiousness on a simple scale of 1 to 10, so users can see how that risk will fall with each day of quarantine. This visualization might change perceptions. E.g., an individual who wants to comply with a 14-day quarantine, but does not feel able to, might rush out to get groceries before starting their quarantine in earnest, while shedding virus pre-symptomatically. Visualizing projected risk into the future would then give the message that if the exposed individual can only make do for one more day before leaving the home for essentials, that will help, because if they do not develop symptoms, their risk will be lower even after a single day longer. Risk communication in an app could focus on day to day coaxing of this form.
Conflicting messages can still arise if manual contact tracers trace an individual who also received an exposure notification. In this case, it is likely that the two recommend different end dates for quarantine. While this is to be expected from our procedure for recommending variable quarantine durations, we note that even if the app were to issue 14 day quarantine recommendations only, it could still arise because the individual has been exposed more than once, on different days, and the manual contact tracer is following up an infected individual who may not have used the app. Until there is reliable data on app performance, we recommend that the manual contact tracer’s protocol should override whatever the app says. Should the app turn out to perform well, an alternative procedure might eventually be to go with whichever protocol recommends the longer quarantine. An intermediate possibility is for the manual contact tracer to ask for exposure notification details, to determine whether it may be a different exposure to the one being manually traced. There may also be conflicts in protocols for the timing of testing.
Note that with symptom onset sometimes as early as two days after exposure, and given the possibility of pre-symptomatic shedding, and the possibility of confusion regarding who infected whom, we currently ignore the possibility that shedding might not yet have begun. Current testing turnaround times are mostly long, making this reasonable. However, if same-day tests become more widely available, our approach could be extended to directly communicate the risk of current infectiousness, rather than as is currently the case, the risk of current or future infectiousness. A significantly lower risk of infectiousness will be present on the day of exposure and perhaps also the day after. Delays in going into public to prepare for a long quarantine could inadvertently lead to pushing individuals past the latent period before they go into public; displaying a full projected timeline of the projected risk of infectiousness could avert this, at the risk of significantly more complex messaging than “stay home until Friday”.
We currently consider the harm from the release of any infectious individual to be equivalent to that from the release of any other. Extensions of our approach could take into account greater harm from someone never quarantined and hence shedding for the full duration relative to someone released prematurely partway through asymptomatic or pre-symptomatic shedding, for whom a portion of the harm has already been mitigated. This would lead to steeper discounting and might also prevent the app from occasionally recommending quarantines of less than 5 days when initial risk is already very near the threshold.
Acknowledgements
We thank the many testers who participated in alpha testing of the app for their time and feedback, including those attempting to test in Androids who were stymied by technical issues. We also thank Marm Kilpatrick for literature pointers, Jacob Steinhardt and Bruce Helming for comments on a draft manuscript, Dave Lines for writing instructions for executing test scenarios and providing participant support, Ami Buczek for installing the app on loaner phones, Danielle Zhou for helping with testing instructions, setting up test logs, and making test assignments, all of the Covid Watch team for agreeing to include our risk scoring scheme into their app, Yuanxia Li and Sudha Ram for agreeing to let us publish alpha testing data ahead of and separately from their analysis, Luca Ferretti for sharing a manuscript in preparation that helped confirm our choice of pre-symptomatic Transmission Risk Scores, Gary Windham for doing the code reviews that led the University of Arizona to adopt Covid Watch, Darcy Van Patten for organizing the details of that adoption, and Joyce Schroeder for her leadership of the Covid Watch pilot at the University of Arizona. Funding was provided by the University of Arizona.
Footnotes
We now report on the application of the method to data, and the resulting tuning of parameters. Many other small changes throughout.
References
Reference



