
Abstract
Objective To determine the impact of the COVID-19 pandemic on mortality, life expectancy and lifespan inequality in the first half of 2020 (from week 1 to week 26 starting June 22) in England and Wales.
Design Demographic analysis of all-cause mortality from week 1 through week 26 of 2020 using publicly available death registration data from the Office for National Statistics.
Setting and population England and Wales population by age and sex in 2020.
Main outcome measure Age and sex-specific excess mortality risk and deaths above a baseline adjusted for seasonality in the first half of 2020. We additionally provide estimates of life expectancy at birth and lifespan inequality defined as the standard deviation in age at death.
Results We estimate that there have been 53,937 (95% Prediction Interval: 53,092, 54,746) excess deaths in the first half of 2020, 54% of which occurred in men. Excess deaths increased sharply with age and men experienced elevated risks of death in all age groups. Life expectancy at birth dropped 1.7 and 1.9 years for females and males relative to the 2019 levels, respectively. Lifespan inequality also fell over the same period.
Conclusions Quantifying excess deaths and their impact on life expectancy at birth provides a more comprehensive picture of the full COVID-19 burden on mortality. Whether mortality will return to - or even fall below - the baseline level remains to be seen as the pandemic continues to unfold and diverse interventions are put in place.
What is already known on this topic COVID-19 related deaths may be misclassified as other causes of death thereby underestimating the full impact of the pandemic on mortality. Excess mortality, the difference between observed deaths and what would have been expected in the absence of the pandemic, is a useful metric to quantify the overall impact of the pandemic on mortality and population health. Life expectancy at birth and lifespan inequality assess the cumulative impact of the pandemic on population health.
What this study adds We examine death registration data from the Office for National Statistics from 2015 to week 26 (mid-year) in 2020 to quantify the impact of the COVID-19 pandemic on mortality in England and Wales thus far. We estimate excess mortality risk by age and sex, and quantify the impact of excess mortality risk on excess deaths, life expectancy and lifespan inequality. During weeks 10 through 26 of 2020, elevated mortality rates resulted in 53,937 additional deaths compared with baseline mortality. Life expectancy at birth for males and females in the first half of 2020 was 78 and 81.8 years, which represent a decline of 1.9 and 1.7 years of life lost relative to the year 2019. Lifespan inequality, a measure of the spread or variation in ages at death, declined due to the increase of mortality at older ages.
Introduction
Estimating the number of deaths caused by the coronavirus disease 2019 (COVID-19) is an important challenge [1]. Insufficient testing capacity for SARS-CoV-2 during the pandemic and misclassification of causes of death make the true toll of COVID-19 hard to estimate [2]. Moreover, the events and interventions that took place during the pandemic may have indirectly affected other causes of death [3]. For example, both fear of COVID-19 and the overstretching of the healthcare system may have deterred care-seeking for both chronic and acute conditions, potentially increasing mortality from other, non-COVID, causes[4].Similarly, lockdown policies might have decreased deaths from external causes such as road traffic accidents, or increased deaths from causes such as suicide or related to domestic violence.
Thus far, COVID-19 mortality in England and Wales has been tallied via confirmed or presumed deaths due to COVID-19, usually due to a positive SARS-CoV-2 test. An alternative approach to estimate the mortality burden of COVID-19 is to quantify the number of deaths during the pandemic compared to a baseline level of what would have been expected if the pandemic had not occurred. This approach for estimating excess all-cause mortality has been widely used to quantify the mortality toll of previous epidemics such as influenza[5] or HIV[6]. Excess mortality may be quantified in different ways and the “excess numbers of deaths’’ approach has been commonly used so far in England and Wales[7]. While this metric provides an important measure of the burden of the pandemic on a society, simply counting these excess deaths does not provide an understanding of the substantial variation by age and sex over time in elevated mortality risks[8,9], nor do excess deaths provide an understanding of the cumulative impact of the pandemic on life expectancy. Life expectancy at birth is a commonly used indicator of population health that expresses the average number of years a newborn is expected to live given the death rates in a particular period[10]. Life expectancy is sensitive to the ages at which deaths occur and can therefore shed additional light on the cumulative burden of COVID-19 on population health. Lifespan inequality is another complementary indicator of population health which has implications for public health planning. While life expectancy is a measure of average mortality, lifespan inequality is an indicator of the spread or variation in length of life (or conversely, ages at death). It is akin to the Gini Coefficient used by policymakers in understanding patterns of economic inequality. Lifespan inequality has important implications at both the individual and the societal level[11,12]. Greater lifespan inequality means that individuals face greater uncertainty about when they will die, potentially affecting decisions such as health behaviours over the life course[13]. Lifespan inequality also has important implications for health and social care planning and budgets, with higher levels implying greater dispersion in the ages at death and allocation of resources for different needs[11]. Lifespan inequality is one of the most fundamental measures of inequality that reflects how unevenly population health improvements are shared within a population[12].
We estimate all-cause excess deaths from week 10 (March 2-8), the week in which the first death attributable to COVID-19 was registered in England and Wales, to week 26 of 2020 (June 22-28). Week 26 marks the middle of the year 2020. We also provide estimates of life expectancy and lifespan inequality during the first 26 weeks of 2020 and compare them with previous trends. By considering all three measures together: excess deaths, life expectancy and lifespan inequality, the present study presents a comprehensive assessment of the mortality impacts of the COVID-19 pandemic thus far.
Methods
Data
We extracted all-cause death counts stratified by week of death registration, sex and 6 age-groups (0-14, 15-44, 45-64, 65-74, 75-84 and 85-older years of age) from 2010 to week 26 of 2020 from the Office for National Statistics (ONS) for England and Wales. We also obtained population estimates from ONS from 2010 to 2019[14], and population projections for 2020[15]. As these projections represent the population at the mid-year point, we used standard interpolation techniques[16] to estimate weekly mean population by sex and age groups over the study period. Yearly death counts by 5-year age groups were used to calculate annual indicators[17] such as life expectancy and lifespan inequality. All analyses use publicly-available aggregated data. The population coverage of vital registration in England and Wales is complete. Between March and May 2020, 81.1% of all deaths and 86.5% of deaths involving COVID-19 were registered within 1 week of occurrence[7]. Death registration in this period witnessed increased efficiency compared to trends noted in previous years due to changes implemented in the Coronavirus Act 2020 [18,19]. Based on trends from past years, 92% of deaths are registered within 1 month of occurrence.
Excess mortality
We estimated the baseline number of deaths in the absence of COVID-19 by fitting a Generalized Additive Model assuming a Poisson distribution of deaths during the period of study[20]. The model includes smooth effects for the long term trend, age and seasonality, and an interaction between age and seasonality (see Supplement section 1). The smoothed effects are stratified by sex. We then subtracted the expected number of deaths from the observed deaths for the period involving weeks 10 through week 26 of 2020, from March 2 to June 28, 2020.
We fitted the model to the weekly deaths counts from January 4, 2010 to the week starting on March 2, 2020. This baseline was then projected forward until June 28, 2020 (week 26). Excess mortality is then defined as the observed weekly death count minus the baseline, summed across the pandemic period from March 2 to June 28, 2020. From this baseline, 95% predictive intervals were constructed by sampling death counts from a Poisson distribution.
Demographic Methods
Life expectancy and lifespan inequality by sex were estimated using the yearly death counts and population estimates for the years preceding 2020 using standard demographic techniques [10], from which 95% predictive intervals were generated[21]. For the first half of 2020, death counts over the first 26 weeks were aggregated over age groups and death rates were calculated using half of the mid-year population estimate.
Results
Estimates of excess deaths
We report results for the deaths that occurred above the age of 14 since estimates below this age fall within the predictive intervals of the model due to the small number of deaths occurring in this age group.
The first death attributable to COVID-19 in England and Wales was registered in the week starting in March 2, 2020 (week 10). From that week to week 26, which ended on June 28, 2020, there were 228,178 registered deaths over the age of 14, from which an estimated 53,937 (53,092, 54,746) are excess mortality above the expected baseline (see Figure 1). This estimate represents a 31% (30.3, 31.5) increase in mortality compared to the expected level.

Cumulative excess deaths in England and Wales through the COVID-19 pandemic weeks 10-26 by sex. Shaded areas represent 95% prediction intervals. Excess deaths are defined as the total observed deaths subtracting the estimated baseline mortality.
Death rates during the pandemic were consistently higher among males in all groups compared to females (see Supplement Figure 3). Male excess deaths accounted for 54% (28,889 deaths) of this total, compared to 46% (25,048 deaths) among females over the same period. These numbers are 28.7% (27.8, 29.5) and 33.2% (32.3, 34.1) higher, respectively, than the baseline.
The 15 to 44 year old age group accounted for 290 (154, 418) excess deaths (6.1% (3.2, 9) above the expected level). For older age groups excess deaths rose sharply (see Figure 2). The toll of the pandemic resulted in 5,786 (5,504, 6,070) and 7,514 (7,176, 7,845) excess deaths among people between 45-64 and 64-74 years of age, respectively. These numbers are 28.4% (26.7,30.2) and 26.1% (24.7, 27.6) above the baseline. The largest numbers of lives lost were estimated among the groups 75-85 and 85 and older, with 29.1% (28, 30.3) and 36.8% (35.8,37,9) above the expected mortality. Among the former, 15,091 (14,641, 15,547), excess deaths were estimated, while among the oldest age group there were 25,255 (24,720, 25,768) deaths above the baseline. Note the larger number of female excess deaths in the 85+ group is due to there being 1.6 times more females in this age group compared to males.
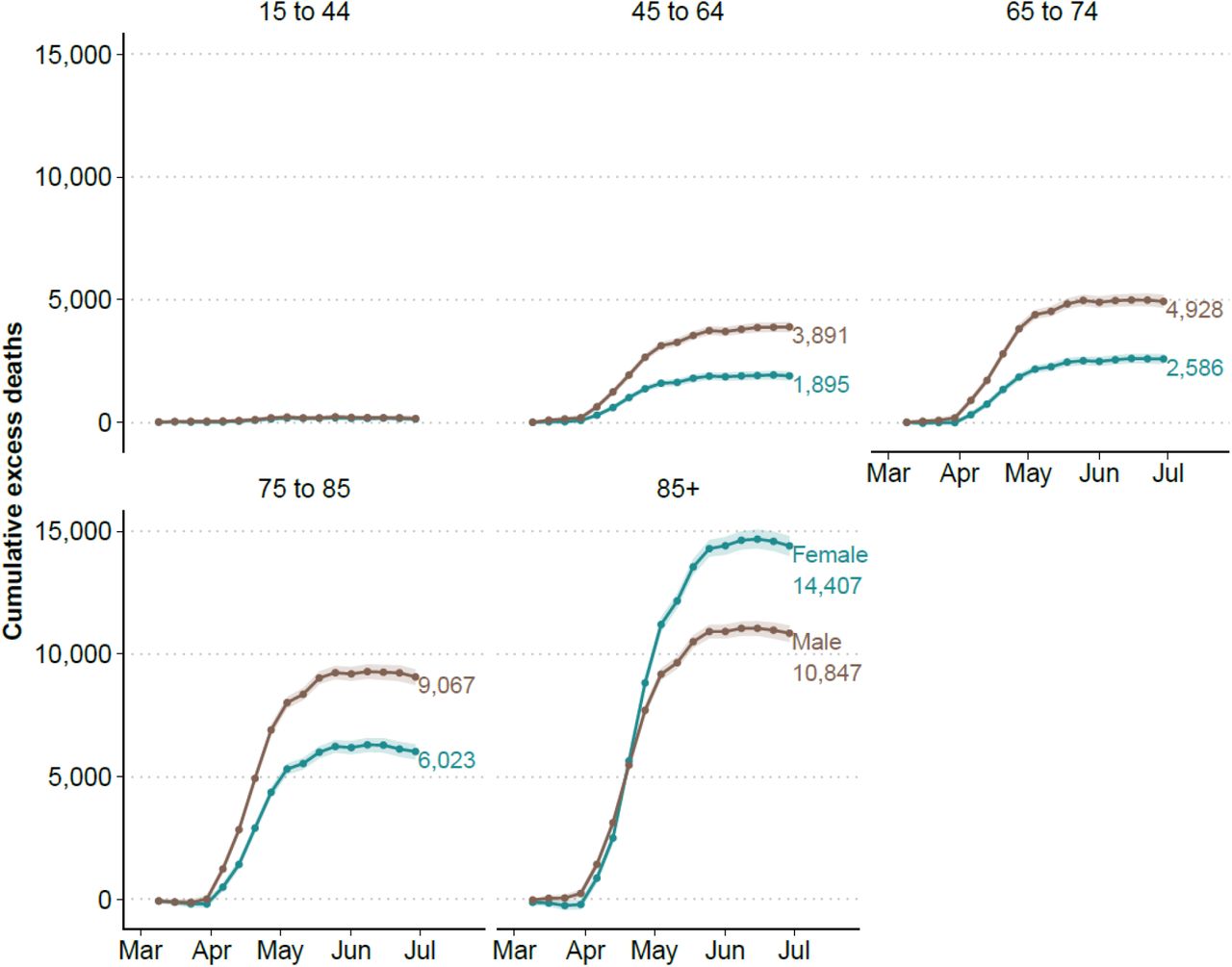
Cumulative excess deaths in England and Wales through the COVID-19 pandemic weeks 10-26 by sex and age groups. Shaded areas represent 95% prediction intervals. Excess deaths are defined as the total observed deaths subtracting the estimated baseline mortality.

Life expectancy and lifespan inequality (standard deviation of ages at death) estimates for the periods 2001-2019, and for 2020 considering the first 26 weeks of the year by sex. Shaded areas represent 95% prediction intervals.
Estimates of life expectancy and lifespan inequality
Life expectancy at birth increased from 81.4 (81.3-81.4) years in 2005 to 83.5 (83.5,83.6) years in 2019 for females in England and Wales. Similarly, male life expectancy increased from 77.1 (77.1,77.2) to 79.9 (79.8,79.9) years in the same period. Using data from the first 26 weeks of 2020 yields an estimated life expectancy at birth of 81.8 (81.8,81.9) and 78.0 (77.9,78.0) for females and males, respectively. A reduction of 1.7 year for females and 1.9 years for males.
From 2005 to 2019, lifespan inequality declined slowly from 13.8 (13.7, 13.9) to 13.5 (13.4,13.6) years for females and from 15.0 (15.0, 15.1). to 14.7 (14.6, 14.7) years for males. In the first half of 2020, we estimate that lifespan inequality fell sharply to 12.9 (12.8,13.0) and 14.0 (13.9, 14.1) years for females and males, respectively, corresponding to a reduction of over six months for both sexes.
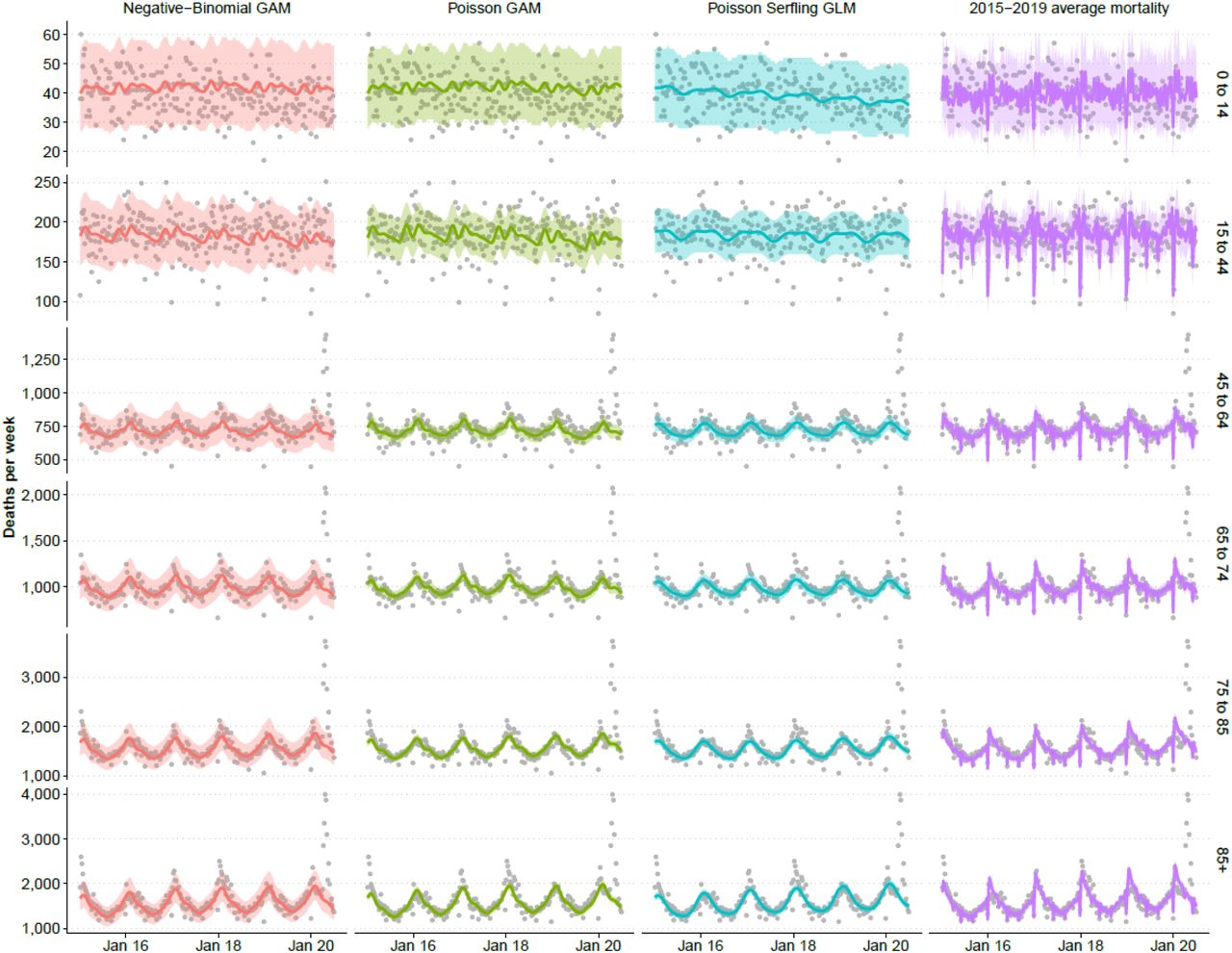
We performed several sensitivity analyses. Firstly, we refitted the seasonal baseline without including the first 9 weeks of 2020. This adjustment did not have major effects on our estimates and by taking the first 9 weeks into account made our predictions in line with the observed trend in the beginning of the year. Secondly, we fitted a GAM model under the assumption of a Negative Binomial distribution and a Generalized Poisson Linear Model adjusted for year-to-year seasonality[24], also known as extended Serfling model[25] (see Supplement Section 1). Finally we created an empirical baseline by averaging the death rates observed in each week of the years 2015-2019 (see Supplement Figures 1 and 2). While these model variations produce central estimates of the number of excess deaths between 49,429 and 58,982 depending on the choice of the model and its assumptions, they do not substantively affect the pattern of our results. For full details please see Supplement Tables 1 and 2. In addition, we also estimated life expectancy using a piecewise constant hazard model and the results did not change.

Discussion
Excess deaths during the first half of the year 2020 shed light on the cumulative burden of the COVID-19 pandemic in England and Wales. While several European countries have experienced substantially increased mortality over the course of the pandemic, data at hand suggests that England and Wales are amongst the worst performers in terms of excess deaths, especially in the working age group 15 to 64[26]. We estimated that 53,937 (53,092, 54,746) deaths would not have occurred in the absence of the pandemic. As previously noted by several studies, the toll of the pandemic had unequal impacts by age and sex in Europe and other regions[8,27,28]. Similarly, excess mortality varied between sexes, with males accounting for 54%. Excess deaths increased sharply over age and male deaths were estimated to exceed females in all age groups, with the exception of those above age 85. This is largely explained by the population composition of England and Wales where more females survive to higher ages. Excess risk of mortality was consistently higher among men in all ages groups (see Supplement Figure 3).

Life expectancy in England and Wales had been steadily improving for 50 years before stagnating in the past decade [29,30]. We have provided estimates of life expectancy for 2019 and the first half of 2020 which show that life expectancy dropped a staggering 1.7 and 1.9 years for females and males respectively between these years. Moreover, our mid-2020 estimates for life expectancy fall 1.7 and 2 years below the official projected life expectancy in 2020 for females and males[31], respectively. To put this into perspective, male and female life expectancy in the first half of 2020 regressed to the levels of 2008. It is likely that our estimates of excess deaths and life expectancy losses until this period are underestimated, as these estimates are based on deaths registered so far, a small fraction of which may have experienced registration delays[7]. Recent evidence suggests that reversals and stagnation in life expectancy amongst developed countries are usually a result of mid-life mortality crises [30]. In contrast, life expectancy losses during the pandemic have come about from sharp increases in older age mortality in both sexes. Trends across the second half of the year are unclear. Provided there is not a substantial ‘second wave’ of COVID-19 and that the pandemic affected the most fragile individuals[32] (e.g. in the most deprived areas[33] and with pre-existing conditions[7]), the remaining population may see lower than usual death rates in the second half of 2020, thereby making the overall life expectancy losses less severe. However, even if death rates fall 10% below the baseline level, life expectancy for 2020 would still be 4.4 and 6.6 months lower than expected for females and males. Alternatively, there could be long-term health effects among the millions of COVID-19 survivors that continue to impact future mortality risk[34]. For instance, if mortality declines but is still 10% higher than the baseline death rates for the rest of the year, life expectancy losses would be around 1.3 and 1.6 years for females and males, respectively.
Between March 1st and May 31st, 2020 there were 46,687 deaths involving COVID-19, 94% of which assigned COVID-19 as the underlying cause of death[18]. A sizable fraction of our estimate for excess deaths is thus likely to be directly linked to COVID-19. An additional 2,924 deaths were noted where COVID-19 was involved, but not identified as the underlying cause of death. Deaths occurring from Alzheimer disease and dementia, ischemic heart disease, cerebrovascular diseases, neoplasm of the trachea, influenza and pneumonia and ‘symptoms signs and ill-defined conditions’ category were all higher during the pandemic period. Together Alzheimer and ‘symptom signs and ill-defined conditions’ experienced the largest increases in magnitudes compared to their size in previous years, and deaths occurring from asthma and diabetes at home also increased[18]. These preliminary cause-of-death patterns indicate that a significant fraction of the unexplained mortality may be attributable to undiagnosed COVID-19. As new data become available over coming months, future research should seek to develop methods to disentangle excess deaths attributable to COVID-19 versus those arising indirectly due to effects such as reduced care for other conditions.
Historically, lifespan inequality has tended to fall as life expectancy has increased [28], although more recently, studies have found a reversed relationship with lifespan inequality increasing as life expectancy improves [11]. Our results show that life expectancy and lifespan inequality can indeed move in the same direction in periods of massive mortality stress such as during the pandemic. This effect has not been noted or documented elsewhere. While less inequality in lifespans is desirable in the context of life expectancy increases, here the high burden of mortality at working and older ages has contributed to lowering lifespan inequality at the expense of decreasing life expectancy, which is a failure. Whether lifespan inequality will increase or decrease over the next months, or years, will depend heavily on how mortality develops as the pandemic continues to unfold as well as the health and wider policy responses put in place by the government.
Our results have important implications for health and social care planning in England and Wales. To return life expectancy to an increasing trend will require major efforts from a healthcare system weakened by the unfolding pandemic as well as sustained investment in wider societal policies driving population health. These include the high levels of inequality with respect to health and length of life[35] which have worsened in the past decade[36]. It is also likely that uneven demand for healthcare services[37] for the next months due to the pandemic will put additional pressure on healthcare systems. In the midst of this uncertainty these systems must begin to address the huge impact on hospital waiting lists of months of deferred treatments for chronic health conditions, as well as the huge drop off in referrals for routine care[38] and the longer-term consequences of the suspension of programmes such as routine cancer screening during the pandemic[39]. In this context, the potential impact of low-cost, non-pharmaceutical interventions, such as facemasks use[40] and social contact restrictions[41] to help reduce the number of future COVID-19 cases and deaths is of the highest importance.
Ethical approval
Not required.
Data sharing statement
This analysis used publicly available data. All data and scripts are available at https://doi.org/10.5281/zenodo.3946492
Contributors
JMA, JS, RK and JBD contributed to the design of the study. JMA, CA and RK drafted the manuscript. JS and JMA performed the statistical analysis. All authors contributed to interpretation of data, revised the article critically for important intellectual content, and approved the final version of the manuscript. JMA and RK, the corresponding authors, attest that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding
JMA and RK acknowledge support from the Newton International Fellowship; JMA and JS acknowledge support from the Rockwool Foundation; JMA, RK, JBD and MM were supported by Leverhulme Trust, John Fell Fund and ERC Advanced Grant 835079.
Competing interests
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the Newton Fund, British Academy, Rockwool Foundation, Leverhulme Trust, John Fell Fund and ERC Advanced Grant 835079 for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Section 1. Estimation of the baseline mortality risk using 4 different approaches using training data from 2010 to week 10 of 2020 by age and sex
Generalized Additive Model assuming a Negative Binomial distribution to account for overdispersion of deaths during the period we study[1]. The model includes smooth effects for the long term trend, age and seasonality, and an interaction between age and seasonality. The smooth effects are stratified by sex. The basic structure of the model is as follows:

Where E(Yt) are the expected deaths in a given week, θt are the offset, fi are smooth functions. f1 and f2 are penalized splines for the long term trend and the age effect, respectively. f3 is a penalized cyclic spline for the seasonality and f4 is a smooth interaction between age and seasonality.
The second approach is a Generalized Additive Model assuming a Poisson distribution with the same structure as above.
The third approach is a Generalized Linear Model assuming a Poisson distribution used to estimate baseline mortality during influenza epidemics and known as Serfling model[2,3]. The basic structure of the model is as follows:
We constructed an empirical baseline mortality based on the average mortality rate over the previous five years 2015-19 within each week and stratum. The associated deaths from this approach result from multiplying the average death rates by the population exposed to the risk.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Excess deaths produced with different models
Excess deaths by the end of week 26 for ages 15 and above estimated with 4 different models with 95% predictive intervals in England and Wales.
Excess deaths by the end of week 26 for ages 15 and above estimated with 4 different models by age and sex with 95% predictive intervals in England and Wales.
References



