
Abstract
BACKGROUND Recurrent skin and soft tissue infections (SSTI) caused by Community-Associated Methicillin-Resistant (CA-MRSA) or Methicillin-Sensitive Staphylococcus aureus (CA-MSSA) present treatment challenges.
OBJECTIVES Can an evidence-based intervention (CDC Guidelines, topical decolonization, surface decontamination) reduce SSTI recurrence, mitigate household contamination and transmission, and improve patient-reported outcomes?
DESIGN Randomized trial
SETTING Community settings
PARTICIPANTS Participants (n=186) with confirmed MRSA(+)/MSSA(+) SSTIs and household members.
INTERVENTION Community Health Workers/Promotoras conducted home visits and provided participants with instructions, a five-day supply of mupirocin for nasal application, chlorhexidine for body cleansing, and disinfecting wipes for household cleaning (EXP) versus Usual Care (UC).
MEASUREMENTS Primary outcome was six-month SSTI recurrence recorded in electronic health records (EHR). Home visits (months 0/3) and telephone assessments (months 0/1/6) collected self-report data. Surveillance culture swabs (nares, axilla, groin) were obtained from index patients and participating household members. Secondary outcomes included household surface contamination, household member colonization and transmission, quality of life and satisfaction with care.
RESULTS Among patients with SSTIs (n=421), 44.2% were MRSA(+)/MSSA(+); an intent-to-treat analyses (n=186) demonstrated no significant differences in SSTI recurrence (OR: 1.4, 95% CI: 0.51-3.5). Among the enrolled cohort (n=119), there were no significant SSTI recurrence effects (OR=1.14, 95% CI=0.35-3.6). EXP participants showed reduced but non-significant colonization rates. There were no differential reductions in household member transmission or in reductions in proportions of households with ≥1 contaminated surface. Mupirocin resistance did not increase. No significant improvements for patient-reported outcomes were seen.
LIMITATIONS A lower-than-predicted six-month recurrence rate may have limited the ability to detect effects.
CONCLUSION This intervention did not reduce clinician-reported MRSA/MSSA SSTI recurrence. No differences were observed for household members decolonization or household surfaces decontamination.
Methicillin-Resistant Staphylococcus aureus (MRSA) causes multi-drug resistant infections that pose serious clinical and public health challenges. Skin and soft tissue infections (SSTIs) (1, 2) caused by MRSA carry significant morbidity and mortality, and impact patients, families, caregivers, and health-care institutions (3, 4). While studies comparing protocols for reducing healthcare-associated MRSA (HA-MRSA) infections (5) exist, those adapted for community-associated MRSA (CA-MRSA) (6) SSTIs have provided mixed results (7-12). CA-MRSA SSTIs commonly affect healthy, young individuals without exposure to healthcare risk factors or contacts (13).
Most CA-MRSA SSTIs are treated successfully in ambulatory care. However, treatment failure may result in risk of exposure and transmission to household and community members (10, 14-18). Even when primary treatment is successful, recurrent infections are common, ranging from 16% (14, 19, 20) to 43% (9, 21). Little research has examined the feasibility and effectiveness of implementing evidence-based interventions in primary care settings (22). This trial tested two community-based interventions: (1) Usual Care (UC): CDC-Guidelines directed care (incision and drainage (I&D) and antibiogram-selected oral antibiotics (versus (2) Experimental (EXP): UC combined with universal household decolonization and environmental decontamination interventions based on the REDUCE MRSA Trial (5, 23, 24), provided in the home by Community Health Workers (CHW)/Promotoras. We evaluated the comparative effectiveness on SSTI recurrence rates (primary outcome) and household contamination, household member colonization and transmission, and patient-centered measures (pain, depression, quality of life, and care satisfaction) (secondary outcomes) using a two-arm 1:1 randomized controlled trial (RCT). We hypothesized that participants assigned to EXP would experience fewer SSTI recurrences compared to UC.
METHODS
This RCT included practicing clinicians, patients, clinical and laboratory researchers, NY-based Federally Qualified Health Centers (FQHCs) and community hospital Emergency Departments (EDs). The stakeholder research collaborative expands an earlier partnership, the Community-Acquired MRSA Project (CAMP1) which developed research to address CA-MRSA (25-29). The study was approved by Institutional Review Boards at Clinical Directors Network and Rockefeller University.
Study Setting
Three NYC FQHCs and three EDs recruited participants presenting with an SSTI with culture-positive MRSA or MSSA.
Participants
Inclusion/Exclusion Criteria
Participants included were: (1) between 7-70 years, (2) fluent in English or Spanish, (3) planning to receive follow-up care at the FQHC or ED, (4) presenting with SSTI signs/symptoms, (5) had laboratory-confirmed baseline wound culture positive for MRSA or MSSA (also a significant cause of SSTIs; (6) willing/able to provide informed consent, and (7) willing to participate in two home visits. Participants were excluded if they were: (1) unwilling to provide informed consent, (2) acutely ill or visibly distressed (for example, crying, wheezing, bleeding, screaming or shaken), and/or (3) unable to participate in home visits or in a discussion about the study.
Study Protocol
Screening
Patients seeking care for an SSTI were identified via the site’s electronic health record (EHR) or clinical dashboard. CHWs flagged patients for treating clinicians to determine eligibility.
Procedures
Recruitment, informed consent, and baseline clinical assessments were conducted by trained CHW/Promotoras with clinicians and FQHC/ED staff. Following written informed consent, clinicians conducted baseline clinical assessments and collected wound cultures. Wound and surveillance (nasal, axilla, and groin) cultures were sent to one commercial clinical laboratory (BioReference) for culture, antibiotic susceptibility testing, and speciation. Additional molecular epidemiologic testing was carried out by Rockefeller’s Laboratory of Microbiology and Infectious Diseases (27) Mupirocin susceptibility was tested using E-test strips (bioMérieux, Durham, NC) following CLSI recommendations (30).
All participants received clinician-directed standard-of-care treatment, including I&D and/or oral antibiotics. If I&D was performed, a sample of purulent drainage material was obtained; if I&D was not indicated, the clinicians took a swab of the wound or, if the wound was weeping or draining, obtained purulent material. During the same visit, on-site CHW/Promotoras scheduled the home visit. If a CHW/Promotora or other research staff member was not present, per “warm hand off” procedures (31), clinical staff informed participants that a CHW/Promotora would telephone them.
When culture lab results became available (2-3 days later), medical staff disclosed MRSA/MSSA status. CHW/Promotoras then called each participant to inform them of eligibility. For those with MRSA+ or MSSA+ SSTIs, CHW/Promotoras confirmed the baseline telephone interview appointment and baseline home visit.
Assessments
Baseline Assessments
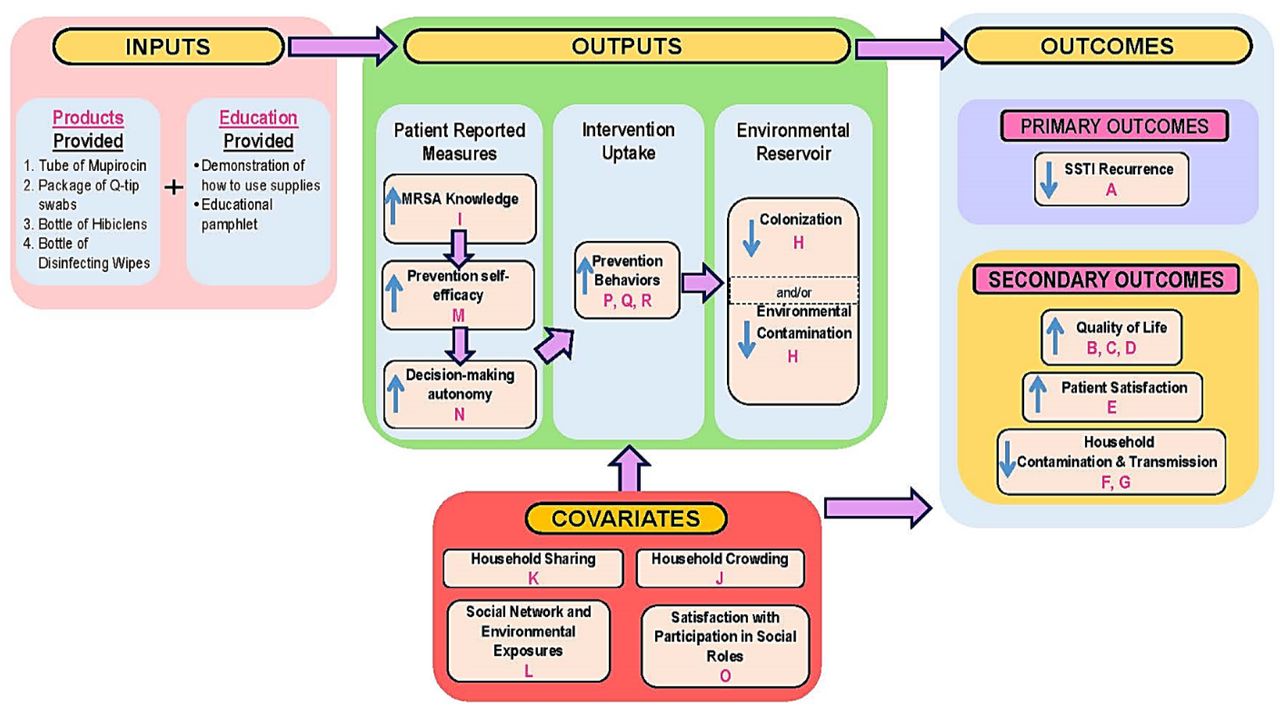
Supplement Figures 1a and 1b detail the full assessment protocol. A Baseline Telephone Questionnaire including demographics, medical history, comorbidity, social, occupational and environmental exposures, household composition and patient-centered outcomes (Supplement Table 1) was administered in English or Spanish.


*Letters in Figures 1a and 1b refer to measures described in Supplemental Table S1
Measures, Data Sources and Time Points¥
The Baseline Home Visit Assessment (T1) captured: (1) consenting household members’ demographics, comorbidities, SSTI history, and index patient and household member personal hygiene, (2) household sharing behaviors, (3) collection and retrieval of self-sampled surveillance cultures from the index patient and consenting household member, (4) census of the numbers of rooms, household inhabitants and regular visitors, (5) 13 samples obtained from high touch/high traffic household environmental surfaces (see figure 3a) using ESwabs™ (Copan Diagnostics, Inc., Murrieta, CA).

* “Intent-to-treat” cohort (n=186)** “Analysis” cohort (n=119). An additional n=66 participants were eligible for participation based on having either MRSA+/MSSA+ wound culture and provided informed consent; however these participants did not complete the baseline home visit, and therefore never received the intervention. Since these participants had consented to be followed, their six-month chart review data were extracted and are provided as an additional “observation-only control group” (n=63 of these participants were analyzed, for a 95.5% response rate). Upon subsequent review, one patient was determined to have met criteria for HA-MRSA and considered ineligible and these data were removed from the analysis, leaving n=119 (“analysis cohort”). Data collection spanned 11/01/2015 and 11/25/2017.


CHWs/Promotoras oversaw participants’ and household members’ self-sampling of nares, inguinal folds, and axillae. Prior to randomization, participants received the educational pamphlet, “Living with MRSA”, available in English and Spanish (32).
Follow Up Assessments
Home visits occurred at three-months (T3). Interim telephone assessments at one-month (T2) and six-month follow-up (T4) were conducted (Supplement Figure 1a). Reviews of EHRs were conducted at T4 to record SSTI recurrence (i.e., one or more discrete clinical SSTI(s) at the same or new site in addition to the baseline infection during the six months following trial enrollment). Patient-reported SSTI recurrence was also recorded. While we had planned to combine SSTI recurrence data from EHR and self-reports, participants’ self-reports had poor concordance with EHR-based clinician reports, so we limited the main analysis to clinician-documented SSTI recurrence.
Randomization
After baseline questionnaires and household sampling data were collected, and while still at the home, CHWs/Promotoras opened a sealed opaque envelope containing the computer-generated randomization (1:1), overseen by the offsite, blinded study statistician (JCdR). Participants were not stratified during randomization based on recruitment site or pathogen (MRSA or MSSA). If randomized to UC, the CHW/Promotoras explained the timeline for remaining assessments and concluded the visit. No further intervention materials were provided to UC.
Interventions
Modeled on the REDUCE MRSA trial (5), EXP received CDC and Infectious Disease Society of America guidelines-directed usual care (23, 33) combined with universal household decolonization and environmental decontamination educational interventions (5) and materials from CHWs/Promotoras. They received detailed verbal, written, and demonstrated instructions of the five-day protocol of twice-daily application of mupirocin ointment to the anterior nares with a clean cotton applicator (34), once-daily Hibiclens® (chlorhexidine gluconate solution 4% w/v) whole body wash (9, 12, 23, 35-37), and household decontamination instruction including: (1) proper handwashing technique, (2) laundering bed linens and pillows in warm water every other day, and (3) disinfection of “high touch” environmental surfaces with disposable disinfecting wipes (33, 38).
Retention and Withdrawal
Participants who withdrew were asked to provide reason(s) for withdrawal (see CONSORT Diagram, Figure 1. We attempted to reach all participants until the trial completion date.
Sample Size Calculations and Power
Sample size estimation was based on SSTI recurrence rate from CAMP1, where 33.3% experienced an recurrence during the six months following their index SSTI (28); previous studies of HA-MRSA reported reductions between 30% and 55% (39-41) To achieve 80% power at 5% significance level in a two-sided Chi Square/Fisher’s Exact test for recurrence at 6-month follow-up, estimated sample size requirement was 120 participants (60 per group).
Analytical and Statistical Approaches
Chi-square tests were applied for comparison of proportions and t-tests were used for continuous quantitative variables. All primary main effects outcomes analyses (n=186) were evaluated according to “Intent-to-Treat” (ITT). Subsequent planned analyses included patients who completed the baseline home visit (n=119, “analysis cohort”) and pre-specified subgroups. Logistic regression and generalized linear mixed effect models were used for hypothesis testing. All analyses were conducted with SAS (Version 9.3) or R (Version 3.0).
Missing Data/Sensitivity Analyses
Although we observed a small proportion of missing data, data were assumed to be “missing not at random” (MNAR) so we used a sensitivity approach rather than multiple imputation. No meaningful or statistically significant differences were revealed between the original versus sensitivity analysis results.
Role of Funding Source
The trial was funded by Patient-Centered Outcomes Research Institute (PCORI). PCORI scientific staff played no role in study design and conduct, and were actively involved in the preparation of the final report.
RESULTS
Baseline Comparisons: Experimental versus Usual Care
A total of 602 patients were assessed for eligibility (Figure 1; 115 from FQHCs and 487 from EDs), of whom 421 (86.4%) provided informed consent, and 186 (44.2%) tested positive for MRSA or MSSA, and were invited to complete the baseline home visit (i.e., “intent-to-treat cohort”). Of 186 eligible consented participants, 120 (65%), completed baseline home visits.
Patients who did (n=120) and did not (n=66) complete the baseline home visit were similar (Supplement Table 2), with equal proportions undergoing I&D (60.7%). Both groups exhibited similar dermatologic symptoms, with no differences in lesion location, size, type, purulence, or signs/symptoms of SSTIs (Supplement Table S2). We also compared those who completed the allocated intervention and had 6-month follow-up data (n=92) to those who received the allocated intervention but did not complete the 6-month follow-up survey (n=28, Supplement Table S3). Rates of I&D, MRSA/MSSA, and recruitment source (FQHC vs ED) were similar.
Characteristics of Consented Participants who Completed the Baseline Home Visit (T1) versus Patients Who Did Not Complete the Baseline Home Visit (T1)
Demographics of Participants who were Followed-up vs. Not Followed-up
No statistically significant differences were detected between EXP and UC in baseline demographics, comorbidity, baseline occupational or environmental or social exposures (Tables 1a-1c) or in the proportion of household members who participated in the study: 64.1% of household members provided surveillance cultures (EXP=67.5%, UC=60.2%, p=0.34; see Figure 4). About half (52.5%) spoke English as their primary language and 36.4% spoke Spanish as their primary language. Microbiological and dermatologic characteristics, and health care utilization were similar, (Supplement Table S4) but MRSA+ wounds were more common among patients randomized to EXP (66.1%) as compared to UC (32.1%, p=0.0004).
Microbiologic and Dermatologic Characteristics of Study Participants at Baseline
Demographic Characteristics by Treatment Group at Baseline
Comorbidity and Health Care Utilization by Study Condition at Baseline
Occupational and Social Exposures for Study Participants at Baseline

SSTI Recurrence
We used logistic regression analyses to detect treatment group differences on EHR-documented SSTI recurrence at six-month follow-up (Table 2). We conducted initial main effects analysis using all randomized subjects (n=186, “intent-to-treat cohort”). Based on the sensitivity analysis, we conducted all further analyses using completed cases (n=119, “analysis cohort”). The ITT analysis demonstrated no significant differences in infection recurrence between EXP (11.1%) and UC (10.7%; OR=1.4, 95% CI=0.51-3.5). Likewise, when examining the analysis cohort, there were no statistically significant differences between EXP and UC on EHR-documented SSTI recurrence: 11.1% of EXP vs 10.7% of UC had a documented SSTI recurrence (OR=1.14, 95% CI=0.35, 3.6; Table 2).
SSTI Recurrence at Six-Month Follow-Up1
Differences in SSTI recurrence based on self-report (Table 2) showed a trend in the opposite direction: EXP reported a greater recurrence rate at 6 months (22.2%) than UC (7.5%, OR = 3.5 95% CI=0.89, 13.8). Given the differences between EHR-documented and self-reported recurrence we examined concordance by treatment group and by baseline wound characterization. 15.4% of participants with a self-reported SSTI recurrence also had a documented clinical SSTI recurrence. Retrospective self-report of pre-study infections found 30.5% of participants reported ≥1 prior SSTI, whereas 90.7% of participants had documented pre-study SSTIs in their EHRs, indicating poor concordance between EHR and self-report.
The ITT analysis resulted in similar trends when restricted to the enrolled analysis cohort. We also added one additional unplanned analysis comparing the EHR-measured 6 month SSTI outcome with an “observation only control group” (n=66) comprised of eligible individuals with a confirmed MRSA+/MSSA+ wound culture who had initially consented to participate, but did not complete the baseline home visit, so their randomization assignment was never disclosed to these participants or study staff (Supplement Table 2). These participants did not receive any intervention or assessment beyond what was extracted from the EHR, and had no further interactions with research staff, although they continued to receive care where they were recruited. The observed prospective SSTI recurrence rate at 6 month EHR review for the “observation only control group” (10.5%) was similar to those of the EXP (11.1%) and UC (10.7%) groups.
Index Patient Colonization
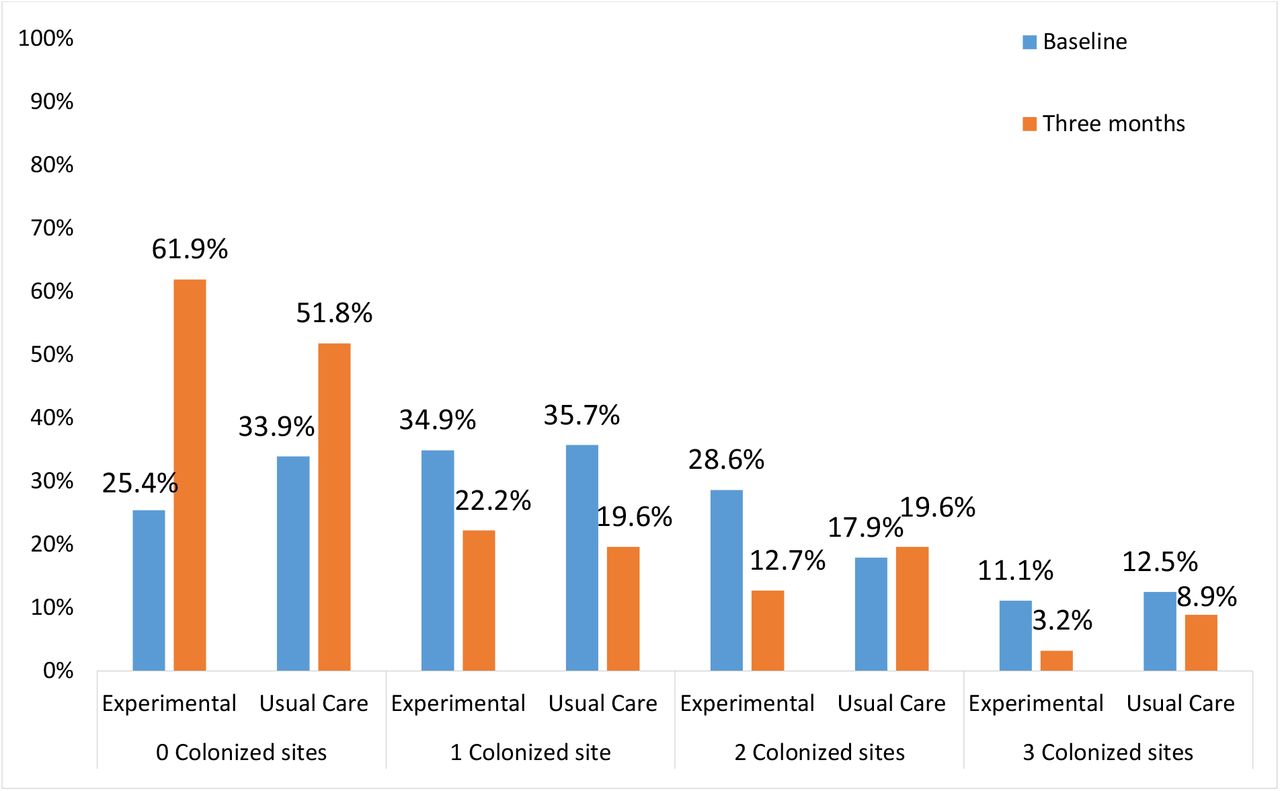
Index patient colonization (nares, axilla, and groin) was measured at baseline and three months. Similar baseline colonization rates were observed: nares (EXP = 41.3% vs UC = 32.1%), axilla (EXP = 34.9% vs UC = 32.1%), groin (EXP = 49.2% vs UC = 44.6%; Figure 2a). S. aureus was recovered at baseline from at least one site (Figure 2b) in most patients (EXP = 74.6 % vs UC = 66.1%). While most patients were colonized at one site (EXP = 34.9 % vs UC = 35.7%), some were colonized at two (EXP = 28.6% vs UC = 17.9%) or three sites (EXP = 11.1% vs UC = 12.5%)
Three months post-intervention, there was an overall reduction in colonization, with S. aureus less frequently recovered from all body sites. Implementation of the decolonization intervention demonstrated that colonization rates in EXP were non-signifiicantly reduced at three months for nares (OR=0.41, 95% CI=0.16-1.04), axilla (OR=0.77, 95% CI=0.31-1.91) and groin (OR=0.53, 95% CI=0.24,1.20), whereas there were little decreases in UC (Figure 2a). Overall, the increase in participants with no organisms detected at three months was greater in EXP (36.5% point increase) as compared to UC (17.2% point increase; Figure 2b). We did not observe any increase in mupirocin resistance between baseline (3%) and three months (0%; data not shown).
Patient-Centered Outcomes
No intervention-related behavioral changes were observed, including infection prevention knowledge and hygiene, prevention self-efficacy, decision-making autonomy, mupirocin and chlorhexidine adherence, QoL or patient satisfaction (Supplement Tables S1 and S5).
Patient Reported Outcomes Scores at Baseline and Six Months for the Total Sample, Experimental Condition, and Control Condition
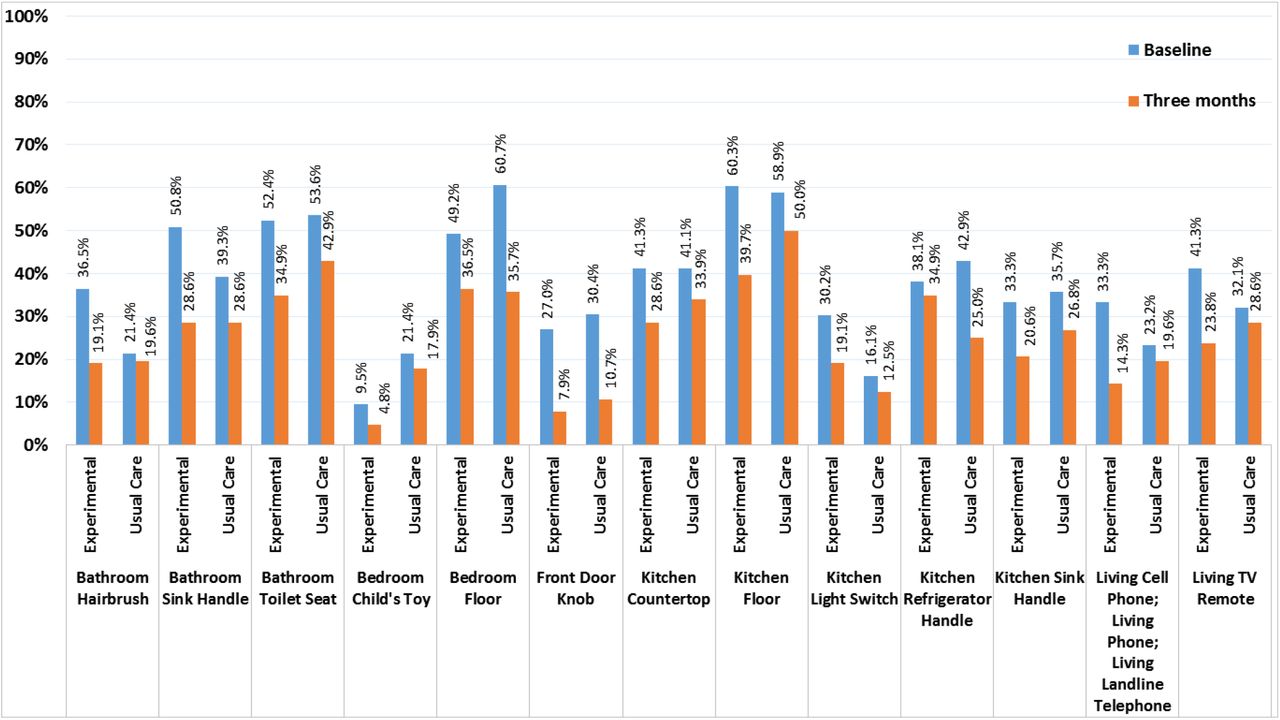
Household Surfaces Contamination
At baseline, the most frequently contaminated surfaces included: toilet seat (EXP = 52.4% vs UC = 53.6%), bedroom floor (EXP = 49.2 % vs UC = 60.7%), and kitchen floor (EXP = 60.3% vs UC = 58.9%; Figure 3a), and most households had ≥1 contaminated surfaces (EXP = 96.8% vs UC = 96.4%). Both groups showed similar reductions in environmental contamination (Figure 3b). There were no differences in reductions in proportions of households with ≥1 contaminated surfaces, EXP (96.8% to 60.3%) vs UC (96.4% to 66.1%). Linear regression examining the average difference in numbers of contaminated surfaces (0-13) showed that there were 0.31 fewer contaminated surfaces at follow-up in EXP versus UC, after adjusting for baseline number of contaminated surfaces (p=0.08; data not shown). Multivariate models with treatment allocation and number of household surfaces did not reveal any associations among these environmental-level factors and SSTI recurrence.
Household Members Colonization and Reported Infection
Consenting household members were screened for colonization (nares, axilla, groin) at baseline and three months. Among household members, similar reductions in proportions of colonized sites were seen for nares (EXP 27.0% to 17.5% vs UC 23.2% to 17.9%), axilla (EXP 17.5% to 9.5% vs UC 14.3% to 10.7%) and groin (EXP 28.6% to 19.1% vs UC 21.4% to 19.6%; Figure 4a). There was a non-significant reduction in household member colonization for EXP (9.5% to 3.2%) versus UC (8.9% to 5.4%). MSSA+ household members were similar at baseline and three-month follow-up in both EXP and UC, with no observed reductions in percentages of household members colonized by MSSA (Figure 4b).
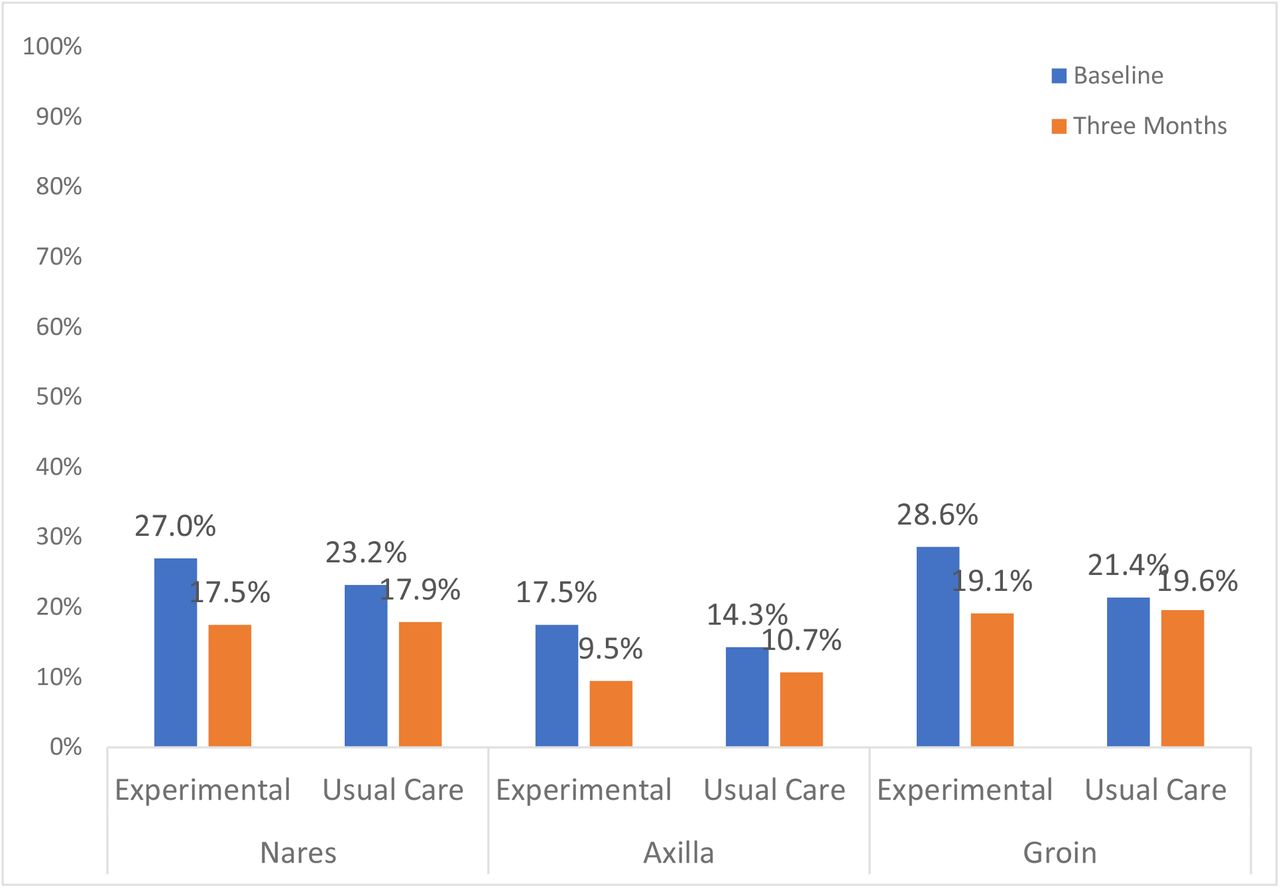
Note: 64% of household members participated in the study and provided surveillance cultures (EXP = 67.5%, UC=60.2%, p=0.34) There were no differences by treatment group in the number of co-residents in households where the index patient had a MRSA wound (EXP=2.4 vs UC = 3.4, p=0.06.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Subgroup Considerations/Heterogeneity of Treatment Effects (HTE)
We conducted pre-specified subgroup analyses using logistic regression with treatment assignment and with each subgroup coded as dummy variables. Consistent with previous studies (28), foreign-born participants were more likely to have MSSA+ than MRSA+ wound cultures. Other HTE subgroup comparisons [wound culture type (MRSA vs MSSA), birthplace (USA vs non-USA), household contamination levels (low vs high), household members colonization (present vs absent), pets living in the household (present vs absent), recruitment site (ED vs FQHC), and baseline I&D treatment (yes vs no)] revealed no statistically significant differences for EHR-documented SSTI recurrence (data not shown).
DISCUSSION
This study adapted and implemented an effective hospital ICU-based intervention (5) into the community. We examined the comparative effectiveness of usual care: CDC/Guidelines-directed care (23, 24) versus an experimental intervention: UC combined with universal decolonization and environmental decontamination (5, 23, 24). Results suggest that this was a null trial. There were few observed hypothesized intervention-related differences for clinical, microbiological and patient-centered outcomes.
The primary and secondary outcomes analyses indicated that EXP fared as well as UC. Despite a significant baseline difference in MRSA-positive (more common in EXP) and MSSA-positive (more common in UC) cultures which we had not anticipated and therefore did not stratify during randomization, we saw no evidence that this baseline imbalance affected the analyses.
Interestingly, the overall study rate of SSTI recurrence was substantially lower (10.8%) than previous studies (42, 43), although a recent cohort study reported a comparable 3-month recurrence rate (10.3%) (10). It is possible that high study rates of I&D plus oral antibiotics contributed to the lower than expected SSTI recurrence rate. One recruitment site, a large public hospital ED, predominated, which might explain a lower than expected recurrence (44) since treatments used there have been demonstrated effective in preventing treatment failure and SSTI recurrence (10, 17, 45, 46); thus suggesting a statistical floor effect hindered detection of differences in recurrence. Similarly, the low event rates of household and environmental outcomes reduced the study’s power to detect significant treatment effects. Finally, EXP were more likely to have no detectable S. aureus colonization at three months, but again the difference was not significant.
The environmental persistence of S. aureus and as a colonizer despite active eradication efforts is well-documented and multifactorial (9, 44, 47-49) and likely modulated by interactions inside the household and surrounding community (10, 19, 50-53). Overall, the percent of households with no environmental contamination increased substantially (from 3.2% to 39.7%). However, 60.3% of households were still contaminated and enhanced antimicrobial measures were not more effective (9) than standard patient education and UC. This reflects the inherent challenges of eradicating this opportunistic pathogen in residential settings. While previous studies have demonstrated higher rates of colonization and contamination are associated with recurrence (21, 53, 54), there are conflicting reports of whether reduction in bioburden translates into less recurrence (22, 55, 56). Previous interventions to reduce S. aureus carriage and SSTI recurrence provide mixed results (7, 9, 11, 12, 22, 56-60). Interestingly, Golding, et al showed community education focusing on patient and household hygiene decreased SSTI incidence (61). The universally distributed Living with MRSA pamphlet (32) likely contributed to total study recurrence reduction, potentially obscuring the intervention impact.
Study Limitations
This study’s results likely reflect unmeasured and uncontrolled variables, including application and effectiveness of bioburden reduction and microbial dynamics in an open system (44, 48, 49, 62). Additionally, there were significantly more MRSA+ wounds in EXP vs UC. This higher MRSA bioburden may have made decolonization and decontamination more challenging (53), thereby obfuscating any study treatment-related differences. Since EXP participants were aware of the intervention methods, it is plausible that their sensitization led participants to focus on minor skin symptoms that were ignored by UC, resulting in higher self reported SSTI recurrence.
In order to minimize the burden of multiple home visits and increase study participation, follow-up sampling took place at three months, rather than immediately following initial decolonization and decontamination. Therefore, the immediate effectiveness of the experimental protocol was not measured. It is possible that organisms detected after three-months were not eradicated at baseline since S. aureus can exhibit long-term survival on surfaces (63, 64). However, host recolonization and replenishment of the environment over time is also possible.
Future directions
Implementing common hospital cleaning protocols (5, 33, 65, 66) within a community setting was a formidable challenge and warrants further investigation. Future studies should stratify on infection wound culture type [MRSA(+) vs MSSA(+)] prior to randomization, to ensure balance in treatment assignment, and may wish to power each subgroup sufficiently for SSTI recurrence, as well as measure effects of active antimicrobial measures immediately following completion of the regimen. While nasal decolonization routine herein is standard practice (24), it is possible that a longer and/or more potent decolonization protocol is required to reduce MRSA recurrence (12, 43, 54, 67, 68). In fact, recent studies implementing a similar yet more intense decolonization intervention decreased recurrent MRSA infection recurrence (12, 67). These data, combined with our data, indicate that greater frequency and longer duration of decolonization may be required.
Conclusions
This trial aimed to understand systems-, patient-, pathogen-, and environmental-level factors associated with SSTI recurrence and household transmission. Home visits presented a major challenge. Although the perceived (or actual) intrusiveness of home visits proved difficult to overcome, the “warm hand-off” strategy facilitated a modest improvement in home visit completion rates (69). The lower-than-expected six-month recurrence rate (10.9% here as compared to our previous observational study of 33.3% (28)) may have limited the power to identify a treatment effect. Multiple well-designed studies conducted in different settings have all converged on similar findings: decolonization and decontamination can be accomplished in the household to varying degrees, but extensive, long-term decontamination may be required to achieve a medically meaningful reduction in disease recurrence. These findings suggest that other mechanisms may also contribute to the disconnect between exposure and outcome, such as intrinsic host factors including immunologic competence, as well as perturbations of host and environmental microbiomes. These factors warrant further observational and experimental studies.
Data Availability
Data will be made available following permission from the authors after publication.
Acknowledgements
The authors wish to thank the Clinical Directors Network, Inc. (CDN) Research Team (TJ Lin, MPH; Dena Moftah, BA; Anthony Rhabb, MA, Branny F. Tavarez, MD, Cynthia Mofunanya MD, Jasbir Singh MBBS, MPH, Jessica Ramachandran, MD, Johana Gonzalez, MD, Musarrat Rahman, MPH, Raul Silverio MD, Sisle Heyliger, BA, Tameir Holder MPH, Umamah Siddiqui, BS, Viktorya Snkhchyan MD, Lois Lynn, MS), the The Rockefeller University Research Team (Barry S. Coller, MD, Rhonda G. Kost, MD, Joel Corrêa da Rosa, PhD, Roger Vaughan MS DrPHm Andrea Leinberger-Jabari, MPH, Cameron Coffran, MS, Helen Marie Curry, Kimberly S Vasquez, MPH, Maija Neville Williams, MPH, Marilyn Chung, Teresa H. Evering, MD, MS, Mina Pastagia, MD, MS, Teresa L. Solomon, JD, Alexander Tomasz, PhD, Hermínia de Lencastre, PhD, Maria Pardos de la Gandara MD PhD), the Federally Qualified Health Centers (FQHCs): Community Health Network (Satoko Kanahara MD, FAAP, Tyler Evans, MD), Family Health Centers at NYU Langone (William Pagano, MD, MPH, Barry Kohn MD, PhD, Isaac Dapkins MD; Paula Clemons PA; Viral Patel, MD, Jason Hyde, LMSW, M.Ed), Maria Ferrer, Keenan Millan; Open Door Family Health Center (Daren Wu, MD, Asaf Cohen MD), Urban Health Plan (Claude Parola, MD, Tracie Urban RN, Franco A. Barsanti, PharmD; Ali Saleh PA, Scott Salvato PA, Jennifer Concepcion), Hospital Emergency Departments (EDs): NYC Health + Hospitals/Coney Island Hospital ED (Regina Hammock DO; Rosalee Ngyyen, DO; Candace Gopaul; Ronette Davis), NYC Health + Hospitals/Metropolitan Hospital ED (Getaw Worku Hassen MD; Van Johnson), Patient and Community Stakeholders (Rosa Perez, RPh/Cordette Pharmacy and Dennis Mitchell/Denny Moe Barber Shop), the Data and Safety Monitoring Board (DSMB: Katherine Freeman, DrPH, DSMB Chair/Extrapolate Statistics LLC and Florida Atlantic University; Marilyn Gaston, MD/Assistant Surgeon General and HRSA Associate Administrator for Primary Health Care (ret.), Maria Ferrer/Patient Representative)
Scientific Consultants/Advisors (Susan Huang, MD, MPH, Christopher R. Frei, PharmD, Msc, Eric Lofgren, PhD, Christopher Mason, PhD, Ebhrahim Afshinekoo, BS, Chou Chou, MD, Shirshendu Chatterjee, PhD, Sarah Johnson, MD, Bárbara Milioto, E Denise Digirolomo, Edward Clayton, Vicki Seyfert-Margolies, PhD, Dana Wershiner, Trang Gisler, MS, Suzanne Lechner, PhD, Suzanne Hower, PhD and Sara Vargas, PhD.
The Corresponding Author attests that he has listed everyone who contributed significantly to the project.
Footnotes
FUNDING SOURCE: PCORI Contract Number CER-1402-10800
Corrected author list to remove middle initial from Suzanne Hower, Ph.D.
REFERENCES



