
Abstract
Objectives Autologous blood transfusion (ABT) enhances athlete’s performance, is banned as doping by the World Anti-Doping Agency (WADA). Currently, there is no implemented detection method for ABT. Transfusion of one’s own, long-term cryopreserved red blood cells (cryo-RBC) immediately increases circulating RBC count, hemoglobin mass, blood volume and oxygen carrying capacity, resulting in enhanced physical performance. Functional viablity of cryo-RBC are maintained for decades, but storage lesions lead to removal of damaged RBC from circulation days after transfusion, with remaining circulating cryo-RBC displaying normal half-life.
Methods The cytosolic RBC peptidome from 22 human subjects (12 men and 10 women) was analyzed by UHPLC-MS/MS before and after ABT with cryo-RBC. As a control group and for investigation of confounders, 14 elite athletes and 5 recreational subjects were sampled multiple times, also at high altitude.
Results Here we report alteration in the cytosolic peptidome of circulating RBC weeks after ABT, discriminating doped from non-doped human subjects. A valid discriminating multivariate model (OPLS-DA) based on <200 peptides was accomplished (R2/Q2 = 0.88/0.59, P CV-ANOVA < 0.0001, ROC AUC = 0.97). Models did not show bias for sex, high altitude or elite endurance training and racing.
Conclusion Identified peptides with low intra- and inter-individual variation, and high multivariate model weight and probability scores, create a direct method for the detection of autologous blood doping.
Introduction
Autologous blood transfusion (ABT) enhances the athlete’s performance,1 and is viewed as doping, thus banned by the World Anti-Doping Agency (WADA); but with no implemented direct detection method,2 it remains difficult to survey by sporting authorities. Because cold-stored (+1° to +4°C) blood is viable for a maximum of 42 days,3 during which time the athlete’s physical performance is compromised from blood donation,4, 5 and erythropoietin is readily detected;6 the blood doping method of choice for cheating athletes is transfusion of one’s own, long-term cryopreserved red blood cells (cryo-RBC). Upon transfusion, increases are immediately observed in circulating RBC count, hemoglobin mass,7 blood volume and oxygen carrying capacity,8 resulting in enhanced physical performance.1, 9, 10 Cryo-RBC in storage maintain their function for more than a decade,11, 12 but display storage lesions altering physical properties13, 14 of both cytosolic15 and membrane 16 proteins, leading to an expedited removal of damaged cryo-RBC from circulation 6 h to 48 h after transfusion.17, 18 The remaining circulating cryo-RBC display normal half-life19 despite observable altered metabolic profiles20 and irreversible cytosolic protein alterations, derived from the process of freezing and thawing.21
Today, indirect detection of ABT exist using the hematological module of the Athletes Biological Passport (ABP). The ABP uses longitudinal monitoring of standard hematological parameters to identify possible blood manipulations,22 and can be considered less effective than anticipated in detecting ABT.23, 24 Also, the ABP is affected by exercise25 as well as increased fluid intake.26 Moreover, several tests claim to detect ABT via: immunological reactions,27 hematological variables,28 phthalate/metabolites29 and CO rebreathing30, 31, but no test is implemented for doping detection.
A direct and valid detection method for ABT remains elusive and unavailable,1, 32, 33 but must include intracellular biomarkers, as all cell-surface alterations, including storage-induced,34 initiate rapid removal of cryo-RBC from circulation by spleen macrophages,18 thus circumventing the effectiveness of such markers for detection of ABT.
Proteomic and bioinformatic methodologies allows detection of sample differences in minutiae across subjects and chronology. We proposed that screening the cytosolic fraction of circulating RBC (RBCc) sampled before and after cryo-RBC transfusion, will provide markers specific to ABT. Subsequently, applying liquid chromatography tandem mass spectrometry (LC-MS/MS) analysis will generate biomarkers (proteins and/or peptides), differentiating the two states of pre- and post-transfusion, defining Clean and Doped samples, respectively. In addition, identified biomarkers will be curated to remove those markers biased for sex, exercise, hypoxia and high-altitude exposure.
Method (Appendix 10)
Subjects
Autologous blood transfusion of eight men (age 29; 24-36 years [mean; min-max]) and seven women (age 27; 23-38 years) with peak oxygen consumption (VO2peak); Men (4.3; 3.2-5.0 L·min-1/53; 33-59 mL·min-1·kg-1) and women (3.0; 2.4-3.6 L·min-1/48; 45-56 mL·min-1·kg-1) with five recreational Control subjects sampled in parallel (Appendix 2, 3 & 9). Fourteen international level elite endurance athletes investigated confounders by resting blood samples at: Sea Level (<80 m), High Altitude Training (>1500 m), Hypoxic Tents (>10 h/day, 14 days, 3-4000 m) and in the Hypoxia group up to 28 days after a multisport race (700 km in 4.5 days reaching altitudes up to 4500 m, Appendix 2, 3 & 9).
TRANSFUSION
Women donated one (450 mL) and men two (900 mL) units of whole blood as s described in detail previously 1, 18. Whole blood was collected and glycerolized RBC stored at -80°C until transfusion.
SAMPLING
In total, participants (21 men and 15 women, Appendix 2, 3 & 9) gave 307 venous blood samples, where 85 were in a Doped state after cryo-RBC transfusion, 173 in a Clean state and 49 samples taken directly from the Blood Donation Bag (timeline for Transfusion indicated in Figure 1). Some samples were used multiple times (noted as Batch I, II and III in Tables and Appendices), resulting in 392 LC-MS/MS sample injections (Appendix 2, 3 & 9).

Hematology
Preparation
Erythrocytes were lysed, the cytosol isolated and hemoglobin removed before determination of protein concentration. Pre-digest internal peptide standard was added before trypsin digestion. Clean-up of trypsin digest samples was performed by C18 and dried samples were stored at -80°C.
Nano-UPLC-MS/MS Analysis
Internal retention time standards, pre-LC internal standard and TFA were added before injection using a nanoACQUITY UltraPerformance UPLC™ (Waters). Separated peptides were analyzed using a Synapt G2™ or G2Si™ (Waters). Initial data evaluation used the MassLynx™ software (Waters).
Data processing and analysis
Raw data processing, alignment, peptide identification, quantification (relative abundance) and comparative analysis were performed using Progenesis QI for Proteomics (Waters), Protein Lynx Global Server (Waters) and the open-source Skyline (https://skyline.ms). For peptide identification a curated human proteome database (Swiss-Prot) was used, acquired from Uniprot (www.uniprot.org).
Statistics
Mixed Model using Restricted Maximum Likelihood (REML) and multivariate analysis (MVA),1 with Principal Component Analysis (PCA), Orthogonal Projections of Latent Structures (OPLS)35, and its discriminant analysis OPLS-DA36 were applied. Samples from blood donation (Clean) and after transfusion (Doped), High Altitude Training, Hypoxic Tents and Elite Endurance Athletes created MVA models (Appendix 5 & 9). Regression (R2) and prediction (Q2) were investigated, with valid R2 and Q2 set to > 0.60, 35, 37, 38 in three datasets: Training (Men), Testing (Women) and Validation (Men and Women) for Screening, Selection and Validation of Biomarkers (Appendix 5 & 9).
Confounders
Data from two LC-MS/MS analyses which differed to the biomarker screening dataset (Appendix 6), were used to create four OPLS-DA models investigating confounders. Appendix 7: 1) If peptides separating fresh and cryo-stored RBCc could separate Clean from Doped subject 2) Bias for Elite Endurance training and 3) Summary model (four Y -variables) of Clean, Doped, Elite Athletes and High-Altitude Training. Appendix 8: Bias for High Altitude Training and Hypoxic Tents.
Patient and Public Involvement Statement
Participants in the study were recruited locally. Each participant was given continuous feedback. Lectures informed staff, participants and colleagues of the study objectives.
Ethical considerations
The Ethics Board for Northern Sweden approved the study (DNr: Ö1-2009, 08-196M, 2011-408-32M), and transfusions performed in a hospital clinical. Risks reviewed in Appendix 1. The study was conducted in accordance with the WMA Declaration of Helsinki 2013. Data is encrypted and stored on security protected servers.
Results (Extensive models in Appendix 5 & 9)
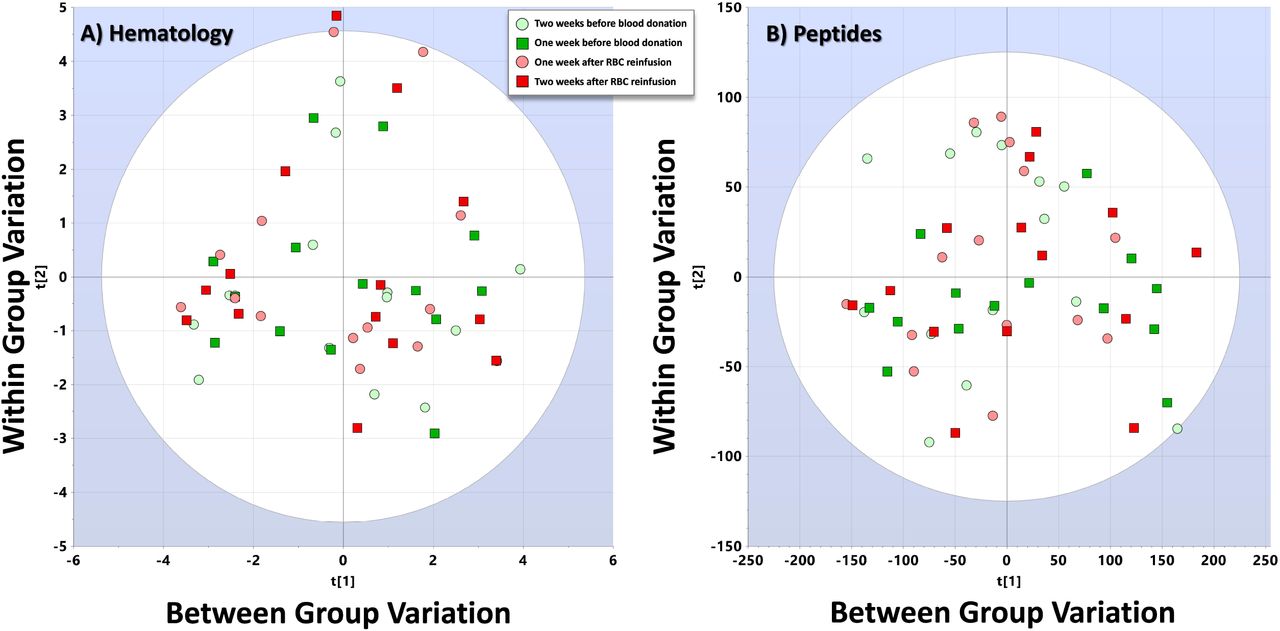
Normal distribution of samples is visualized in a PCA model for Hematological (Figure 1A) and Proteomic (Figure 1B) data.
Hematology
Autologous blood transfusion changed hematological variables (Figure 1, Table 3, Appendix 3 and 4), but with large individual variations, making regression analysis and prediction of samples to Clean (Before blood donation) or Doped (after transfusion of cryo-RBC) unreliable (Figure 2 and 3, Appendix 3 and 4). The visualized OPLS-DA analysis (Figure 3) indicate models with low R2 (<0.6) and Q2 (<0.2) in the Summary of Fit plot, and sensitivity and specificity displayed in the ROC curve, where AUC for Men = 0.97 and Women = 0.79. Selection for prediction by VIP Pred indicate different variables of importance for men and women.

PCA models

OPLS-DA models
Interpretation
Hematological data can generate weak regression models with low predictive power, even when used in combinations.
Proteomics
Multivariate data analysis (MVA) of quantified and identified peptides from circulating RBC cytosol created significant and cross-validated PCA and OPLS-DA models for regression and prediction of analyzed samples to Clean and Doped groups (Figures 3, Appendix 6). Separation of Clean and Doped samples by OPLS-DA analysis resulted in R2 and Q2>0.9 for men, and R2>0.6 and Q2<0.2 for women, displayed in the Summary of Fit plot. Sensitivity and specificity are displayed in the ROC curve, where AUC for Men = 1.00 and Women = 0.68. Selection for prediction by VIP Pred indicate different variables of importance for men and women.
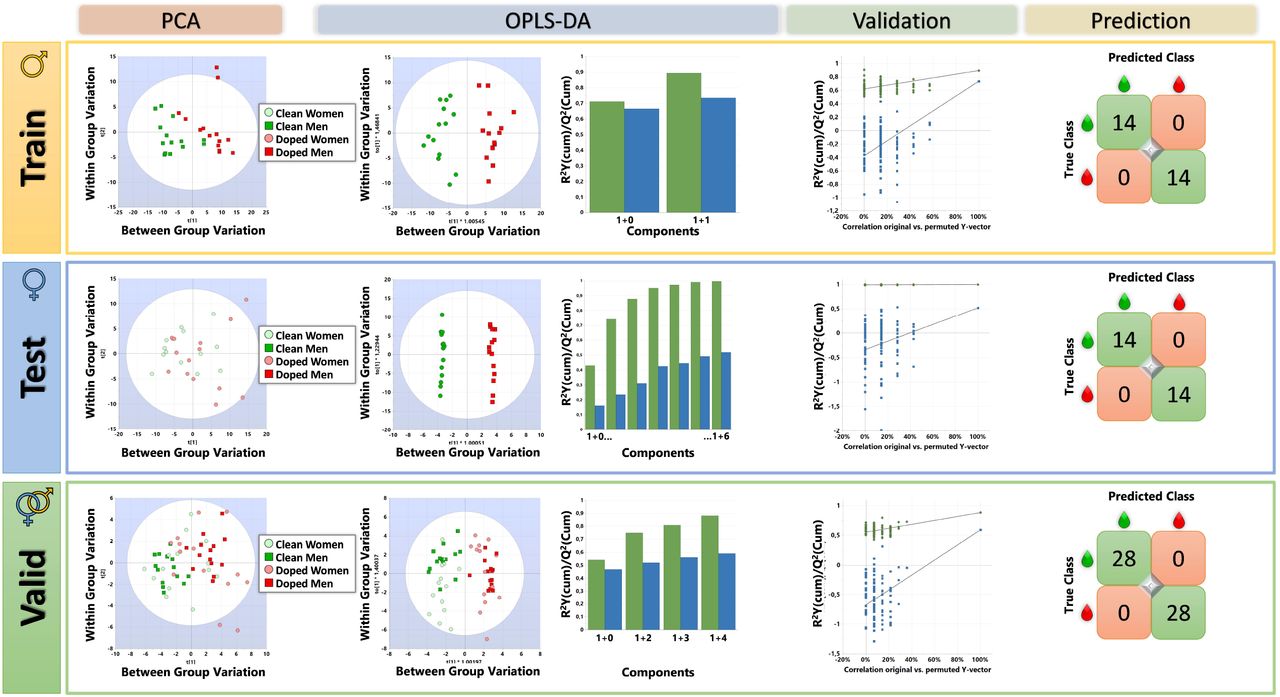
Further results when screening for biomarkers are displayed in Figure 4, where data is divided into three sets; Training (Men), Testing (Women) and Validation (Men and Women). Because the RBC cytosolic fraction (Hb removed) of RBC (RBCc) had different peptidomic profile in men and women, R2(cum) = 0.99/Q2 = 0.92; P <0.0001, different biomarkers in each sex may be assumed. Models excluding sex-separating peptides were also investigated (Appendix 6).
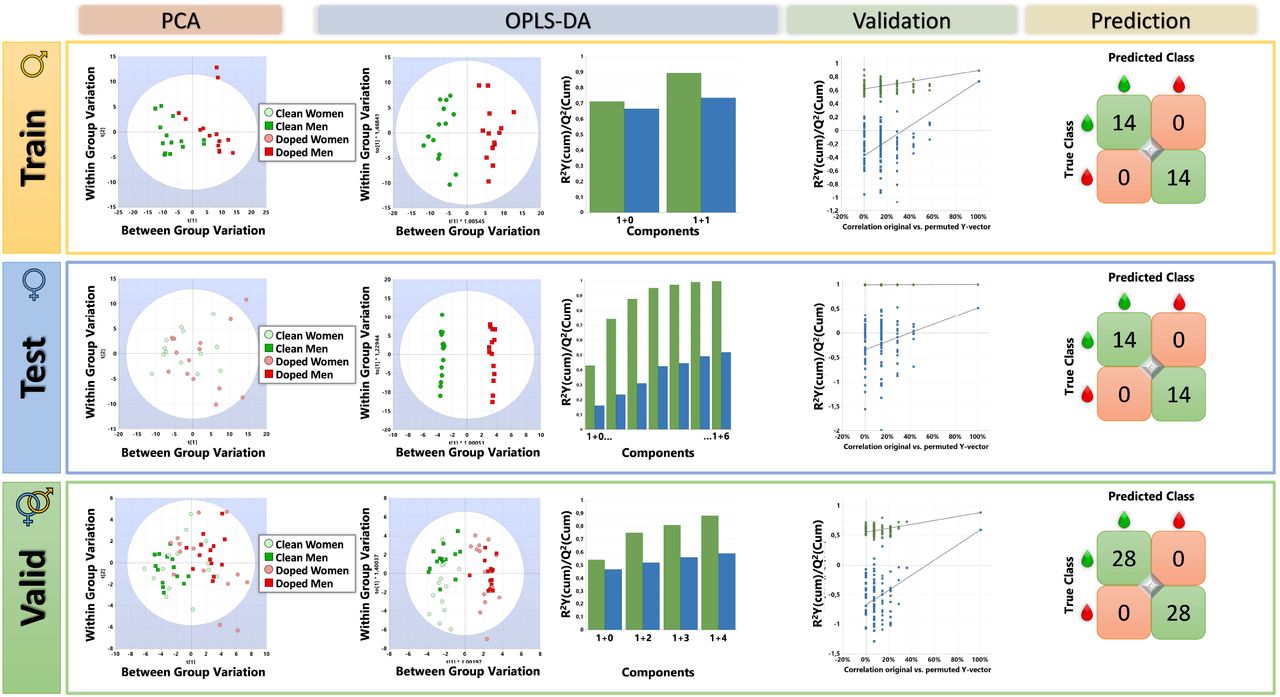
Training/Testing/Validation
Training (Men)
the model pared down data to the 200 most important peptides, separating Clean from Doped both in PCA and OPLS-DA analysis, with high R2/Q2 of 0.90/0.79, cross-validated by 100 permutations and predicting 28/28 samples to the correct class. AUC = 0.96.
Testing (Women)
of the model as accomplished by applying the 200 peptides from the Training model on a cohort of women, resulted in R2/Q2 of 1.00/0.52, cross-validated by 100 permutations and predicting 28/28 samples to the correct class. AUC = 0.92.
Validation (Men and Women)
of selected peptides for prediction of Doping used both male and female subjects in combination, starting with the 200 peptides from men and removing peptides until an optimized model was achieved, containing 50 peptides, reaching, R2/Q2 of 0.88/0.59, cross-validated by 100 permutations and predicting 56/56 samples to the correct class. AUC = 0.97.
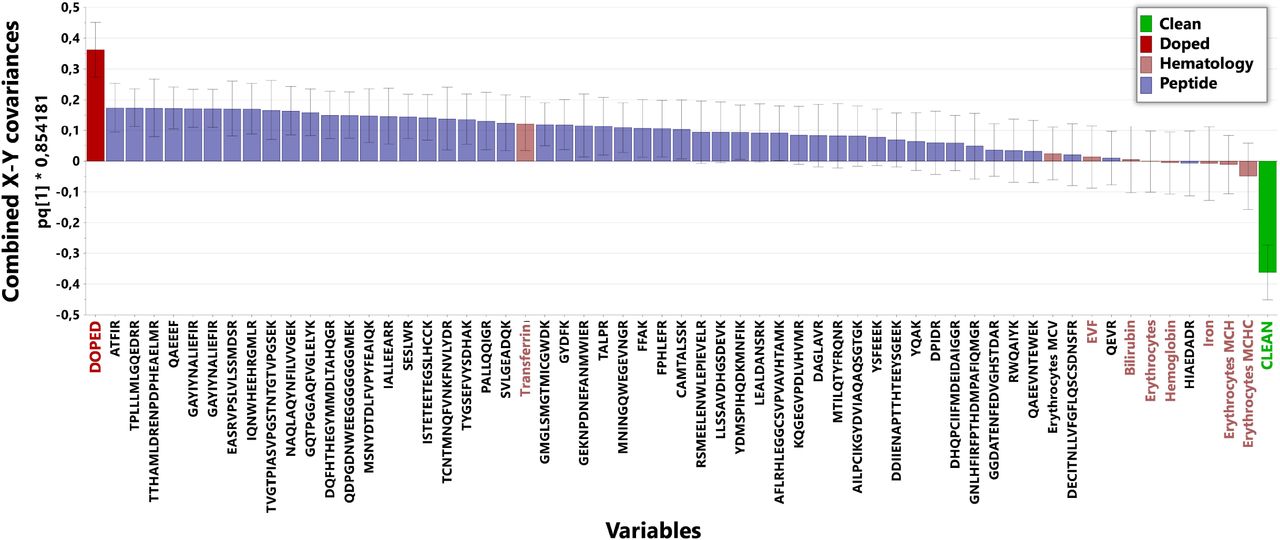
Ranking peptides by OPLS-DA loading scores suggests potential candidates for development of diagnostic tools applicable for the detection of autologous blood doping in humans (Figure 5). Merging hematological and peptidomic signature variables, demonstrate a lower loading impact of hematological variables, compared to peptides (Figure 5) in MVA modeling, supporting the previously demonstrated1 lack of predictive power using hematology (Figure 1, 2 and 3).

Loading plot
Confounders
In vitro peptides quantified and identified from analysis of the cytosolic fraction of RBCs, harvested from transfusion bags before and after cryo-preservation, created significant and cross-validated OPLS-DA models for the two conditions (Bags, Figure 6). In vitro identified peptides did not create significant and cross-validated OPLS-DA models for venous blood samples taken before and after cryo-RBC transfusion (i.e. autologous blood doping, Blood Sample, Figure 6). In vivo peptides quantified and identified from analysis of RBCc taken by venous blood sampling in humans before and after cryo-RBC transfusion, created significant and cross-validated OPLS-DA models (Appendix 9/Table 6/Model 19). In vivo Doped peptides (top 200 from the OPLS-DA coefficients for Doped) also separated venous blood samples taken from individuals (Elite Athletes) trained at High Altitude, living in Hypoxic Tents and Elite Athlete sampled at sea level (Figure 6, Appendix 9/Table 6). In the Summary plot (Figure 6), samples from Doped do not overlap with other investigated cohorts.
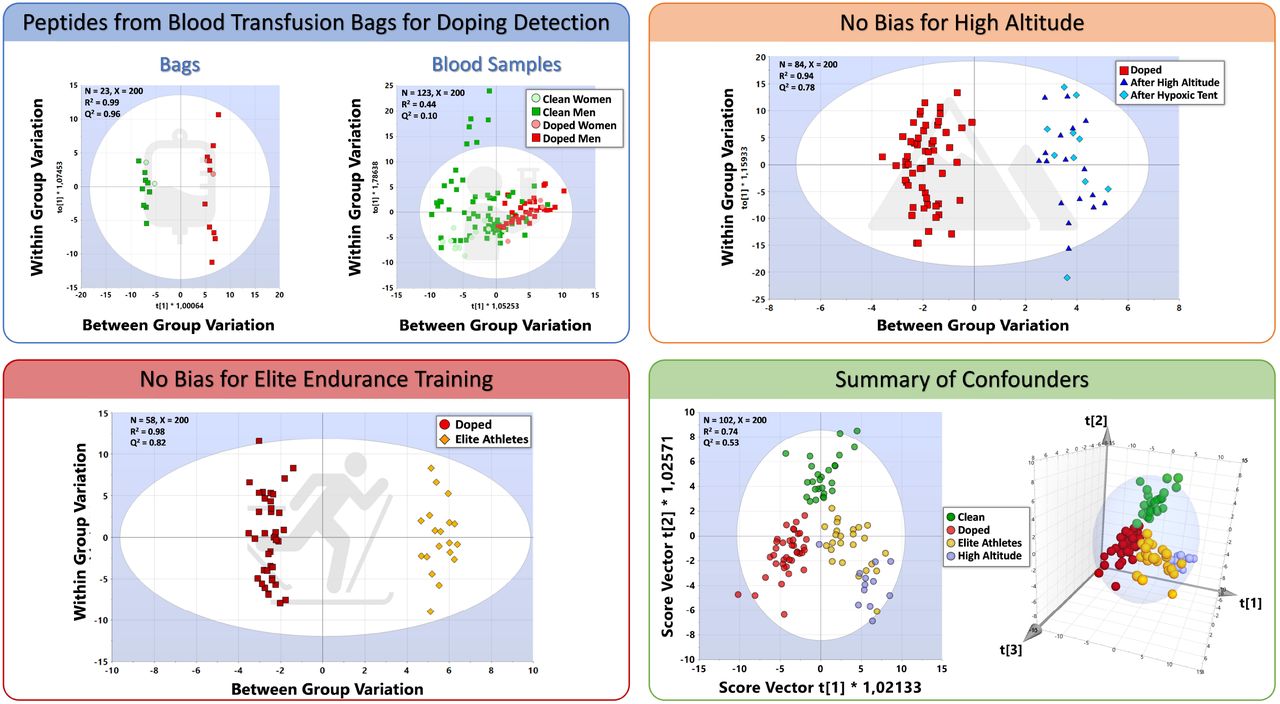
Confounders
Interpretation
Proteomic data can generate strong regression models with high predictive power, both for Men and Women, with no impact (bias) from investigated confounders.
Discussion
Autologous blood doping with cryo-RBC is detected in human subjects by unlabeled, quantitative nano-UPLC-MS/MS. Comparing peptide patterns from RBCc separated Clean from Doped individuals using the multivariate discriminating method OPLS-DA (R2>0.90, Q2>0.90, p<0.001, X<200). Cross-validated models did not show bias for sex, strenuous physical exercise, hypoxia exposure and high-altitude training in elite athletes. In comparison, hematological variables alone failed to generate significant OPLS-DA models when analyzed in parallel blood samples. Investigations were executed using prospective case-control, cohort and cross-sectional study designs.
Biomarkers in biological matrixes
Biomarkers for any diagnostics must be reliable, sensitive, specific, and discriminative.39, 40 In addition, validation must determine predictability of unknown samples to correct state (i.e. Clean or Doped). For practical implementation in anti-doping efforts to keep sports clean, aspects such as available sample matrices, Doping Control Laboratory (DCL) facilities, transport systems and cost are also important considerations.
Red blood cells are closed systems, unable to synthesis protein and with a life cycle of approximately 120 days in adult humans.41 Once set in circulation, RBC undergo an ageing processes, with changing plasma membrane and external structures,3, 41 making them susceptible to recognition and subsequent systemic removal by spleen macropahges.18, 42 While homologous blood transfusion can be detected via surface antigens,3 the only current method to detect autologous blood transfusion is via Hb mass by CO-rebreathing.43, 44 The WADA research initiative states that there is no unequivocal detection method for autologous blood doping, as CO is toxic it has no relevance in anti-doping control of healthy athletes who would be reluctant to have a toxic agent imposed on them repeatedly. Autologous blood doping with cryo-RBC is the preferred choice of cheating athletes, as RBC in cold storage (+4°C) has a known clinical safety limit of 42 days after donation, necessitating repeated blood donation, and subsequent decreased performance,45 during the preparation phase for competition as the red blood cell population are regenerated to compensate for the loss. Cryo-RBC on the other hand, may be stored for decades.12
Regardless of storage procedure, a fraction of all transfused RBCs is damaged and, just as aging RBC, removed from circulation not in 120 days but within 6 h to 48 h.19 Consequently, RBC with intact cell surface proteins, and remaining in circulation 48 h after transfusion, may be viewed as circulating time-stamps, containing bioinformation useful in the detection of ABT.46, 47 The cryo-induced formation of ice crystals, permanently damaging cytosolic RBC proteins,21 serves as a probable, but not the only inducer of potential biomarkers – creating unique detectable peptide fragments after protein trypsinization. An additional advantage of using altered cytosolic biomarkers, compared to hematological variables, is that plasma volume changes will not influence analytical results.
The present series of studies follows a general procedure for biomarker discovery and validation,39, 40 including establishing robust baseline values by repeated sample collection at rest in all investigated groups, transports and storage conditions and routine procedures in accredited, clinical laboratories. Current approaches with multiplexing orthogonal biomarkers into one assay increase robustness to confounders and inter-laboratory variations, while reducing analytical costs. The results are reliable, validated for several known possible confounders, have high specificity, sensitivity and discriminating power.39
True positives and Negatives
One unavoidable challenge when investigating ABT is the inclusion of true positives, vital for all statistical analysis and legal actions. As previously directly shown by us1, argued by others23 and here again demonstrated (Figures 2 and 3) - hematological markers are indirect indicators of ABT, and will always be subject for interpretation (what are limits for normal intra-individual variation?) and significant confounder (exercise, hydration, high altitude, diet, illness etc.) opening for cheating athletes to be legally dismissed from conviction. When investigating hematological intra- and inter-individual variations over time in Clean vs. Doped subjects, neither regression nor prediction models are reliable (Appendix 5). In the context of doping detection, median/range values from elite athletes22, 31, 48 (unknown status of doping) are not relevant for individual judgements, as mean/median values from true positively doped subjects1 can also stay within 95% CI (Figure 2 & Appendix 5). Also, when using cold stored RBC, detection of ABT by hematological measurements has shown low specificity and sensitivity31, 49, 50. Hematological variables changed with investigated confounders, even when more advanced statistical approaches are applied (Figure 1).
The present use of clean elite athletes for comparison is not often possible when validating biomarkers for doping, as athletes cannot serve as subjects. Using cohorts of elite athletes from routine sampling as controls adds uncertainty to any model, as their true state of Clean or Doped cannot be known. Elite athletes participating in this study volunteered to live for extended periods of time in hypoxic tents, before training and competing at high altitude. Knowing they would be tested for blood doping, it is highly unlikely doped athletes are included, also confirmed by the OPLS-DA analysis.
Window of detection
Theoretically, transfusion of cryo-RBC can be detected for up to 120 days, if the youngest RBCs at time of donation could be identified after transfusion.19 Limits of Quantification (LOQ) with the presented method is still not fully investigated, but a few samples (N=14) taken four and five weeks after transfusion (Batch I) are below critical limits (99%) when analyzed by Hotelling’s T2 indicating that these samples are no different compared to samples taken one to three weeks after transfusion. Because cryo-induced peptide abundance diminish as RCBs are aged and removed, LOQ should be determined by target analysis methods. Determining LOQ will also be valuable for detection of micro-dosing with cryo-RBC, a practice likely to be used by cheating athletes to avoid detection.
Alternative interpretations and limitations
An alternative biomarker selection procedure for Clean vs. Doped models could be to exclude the most important (highest OPLS-DA coefficient scores) peptides separating RBCc from Men and Women taken at rest (Clean). This approach may potentially remove peptides important for detecting reinfusion of only one unit cryo-RBC. Creating OPLS-DA models that include 5000 peptides which are most relevant for separating of Men and Women, then selecting the 200 peptides with the highest coefficient score for Doped, creates models for Clean vs. Doped, still biased for sex in the regression models, but without predictive power: Men vs. Women R2 = 0.45 and Q2 = -1.55, CV-ANOVA p =1.00. Data remaining after removing 5 000 peptides from the model of Men vs. Women, provides an OPLS-DA model for Clean vs. Doped using 200 peptides with R2/Q2 = 0.64/0.24, CV-ANOVA p < 0.0001. Removing 10 000 peptides gives R2/Q2 = 0.79/0.38, CV-ANOVA p < 0.001. As discussed, approaching the biomarker selection via a Training set consisting of Men (reinfused with two units RBC) resulted in stronger regression and prediction models (Figure 4). Alternatively, the models for sex investigate cryo-RBC reinfusion of one vs. two units. Data from the present study design cannot distinguish these two options.
Regardless, with the presented list of peptides (Appendix 6 & 9) ABT can be detected in both men and women, reinfused with either one or two units cryo-RBC for at least two weeks after reinfusion.
Conclusion
Doping with ABT is directly detected by cryo-induced alterations in cytosolic RBC peptides, with high sensitivity and specificity in both men and women.
Elite endurance training at low and high altitude did not significantly affect peptides discriminating Clean from Doped samples.
Presented peptides can be used for direct detection of autologous blood doping using standard equipment available in Doping Control Laboratories.
Future research
The potential of selected peptides for labeling and direct detection of autologous blood doping by target analysis should be explored, with independent prospective case-control trials and cross-sectional studies, including inter- and intra-laboratory analytical variability. Larger, both-sex cohorts of clean and doped subjects, elite athletes and different ethnic groups need to be sampled for investigation of sensitivity, specificity, false positive and likelihood ratios.
Data Availability
Data is available in Supplementary files
https://www.dropbox.com/sh/vprl88p6binepmb/AACVJ-mV6jdvqvwDMGDvic30a?dl=0
Contributors
CM conceived the idea, received funding, developed the methodology and clinical study, performed statistical analysis and was lead writer. IG, MH, PL developed the methodology, prepared samples, executed LC-MS/MS analysis and data cleanup. JL, LG, CH developed the method and executed LC-MS/MS analysis. NK developed the methodology, designed experiments and improved data cleanup. All author participated in writing and editing the final manuscript.
Funding
This work was funded by WADA: R07A1CM, 08C06CM and T13M04CM, VINNOVA; 2009-00462, 2013-05410, 2015-05299, 2018-0188, Centrum för Idrottsforskning; 2008 88/08 and Umeå Biotech Incubator. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgements
Outstanding cntributions were given by: The staff at Sunderby Hospital, Luleå for hosting the first series of blood transfusions, under the medical responsibility of Staffan Wikström. The staff at Winternet, Boden for performing all exercise testing and blood sample collection, especially Anna Tano-Nordin and Eva Edholm. The staff at Björknäs Health Center, Boden under guidance of Lillian Falk for organizing the first round of blood donations. The staff at Huddinge Blood Central, where Eva Trollin and Linda Larsson were responsible for blood cryopreservation, and head of unit Hans Gulliksson kindly supported the project. Blood donation, cryopreservation and transfusion, as well as blood sampling, has also been executed by the Center for Stem Cell Apheresis and Management at Huddinge University Hospital, where Emma Watz, Beatrice Asperval Diedrich and Peter Matha managed the study. Ogonna Obudulu for consultation on multivariate statistics. Gunnar Wingsle for technical support with LC-MS/MS, Raik Wagner and Johan Jakobsson for proof-reading and improving the manuscript. All participating subjects for enduring blood loss, exhaustive exercise and numerous trips to the labs.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}