
Abstract
Introduction Since December 2019, a novel coronavirus (SARS-CoV-2) has triggered a world-wide pandemic with an enormous medical, societal, and economic toll. Thus, our aim was to gather all available information regarding comorbidities, clinical signs and symptoms, outcomes, laboratory findings, imaging features, and treatments in patients with coronavirus disease 2019 (COVID-19).
Methods EMBASE, PubMed/ Medline, Scopus, and Web of Science were searched for studies published in any language between December 1st, 2019 and March 28th. Original studies were included if the exposure of interest was an infection with SARS-CoV-2 or confirmed COVID-19. The primary outcome was the risk ratio of comorbidities, clinical signs and symptoms, imaging features, treatments, outcomes, and complications associated with COVID-19 morbidity and mortality. We performed random-effects pairwise meta-analyses for proportions and relative risks, I2, Tau2, and Cochrane Q, sensitivity analyses, and assessed publication bias.
Results 148 met the inclusion criteria for the systematic review and meta-analysis with 12’149 patients (5’739 female) and a median age was 47.0 [35.0–64.6]. 617 patients died from COVID-19 and its complication, while 297 patients were reported as asymptomatic. Older age (SMD: 1.25 [0.78-1.72]; p < 0.001), being male (RR = 1.32 [1.13–1.54], p = 0.005) and pre-existing comorbidity (RR = 1.69 [1.48–1.94]; p < 0.001) were identified as risk factors of in-hospital mortality. The heterogeneity between studies varied substantially (I2; range: 1.5–98.2%). Publication bias was only found in eight studies (Egger’s test: p < 0.05).
Conclusions Our meta-analyses revealed important risk factors that are associated with severity and mortality of COVID-19.
1. Introduction
The severe acute respiratory syndrome (SARS) coronavirus 2 (SARS-CoV-2) initially emerged in Wuhan, Hubei, People’s Republic of China and has been identified as the causative agent of coronavirus disease 2019 (COVID-19). It’s pandemic spread presents a substantial medical challenge with an enormous societal and economic toll1,2. Similar to influenza and SARS-CoV-1, SARS-CoV-2 is considered a “crowd disease” that spreads most easily when individuals are packed together at high densities. Phylogenetic data implicate a zoonotic origin3 and the rapid spread suggests ongoing person-to-person transmission4. Additional factors contributing to the rapid spread constitute the duration of the incubation period5 and infectiousness peaking on or before symptom onset6 contribute to the rapid spread of SARS-CoV-2. Another factor contributing to the rapid spread and alarmingly high number of infected people is the SARS-CoV-2 nature of initial dormancy of symptoms. The most common symptoms associated with COVID-19 include a sudden onset of fever, coughing, and dyspnea2,7,8. Complications comprise acute respiratory distress syndrome (ARDS), pneumonia, kidney failure, bacterial superinfections, coagulation abnormalities and thromboembolic events, sepsis, and even death9,10. So far, only a few demographic and clinical factors, such as older age, diabetes, and cardiovascular diseases, have been linked with poor outcome and increased risk of mortality11,12. This knowledge gap extends to the risk of infections, disease progression, and outcome in vulnerable patient populations, including newborns, children, pregnant, and elderly patients. A better understanding of the risks for these vulnerable patient populations is critical in order to optimize their protection and tailor prevention and treatment strategies. Thus, the aim of our systematic review and meta-analysis was to gather available information in the literature and determine the most prevalent comorbidities, clinical signs and symptoms, imaging features, laboratory parameters, treatments, outcomes, and complications arising in patients with COVID-19. We stratified our systematic reviews and meta-analysis by different cohorts, namely pediatric/neonatal and adult COVID-19 patients including pregnant women. Furthermore, we aimed to assess current evidence for the associations between risk factors and in-hospital mortality. Based on previous reports, we addressed the hypothesis that male sex, older age, as well as pre-existing hypertension and diabetes mellitus are risk factors of morbidity and mortality in patients with COVID-19.
2. Methods
Our systematic review and meta-analysis adhere to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) statement13 and Meta-analysis of Observational Studies in Epidemiology (MOOSE) checklist14.
2.1. Search strategy and selection criteria
Four bibliographic databases were systematically searched: EMBASE, PubMed/ Medline, Scopus, and Web of Science. Our search was not restricted by language. We searched for studies published from December 1st, 2019 to March 28th, 2020, with search terms related to COVID-19 (“COVID-19”, “SARS-CoV-2”, “coronavirus disease 2019”, “severe acute respiratory syndrome coronavirus 2”, “2019 novel coronavirus”, “2019-nCoV”, “coronavirus”, and “corona virus”). The full search strategy is provided in Appendix 1. Manual searching was also performed, reviewing reference lists of relevant studies and comprehensive review articles. Records were managed by EndNote X 8.0 software to exclude duplicates.
2.2. Selection of studies
Two investigators (CRJ and MW) independently screened the titles and abstracts to determine whether studies should be included. Eligibility criteria were also applied to the full-text articles during the final selection. In case multiple articles reported on a single study, the article that provided the most data was selected for further synthesis. We quantified the inter-rater agreement for study selection using Cohen’s κ coefficient15. Articles written in Chinese were reviewed by our two native speaking authors (BT and CW) and if the inclusion criteria were met, these authors also extracted the specified data. All disagreements were discussed and resolved at a consensus meeting.
2.3. Inclusion and exclusion criteria
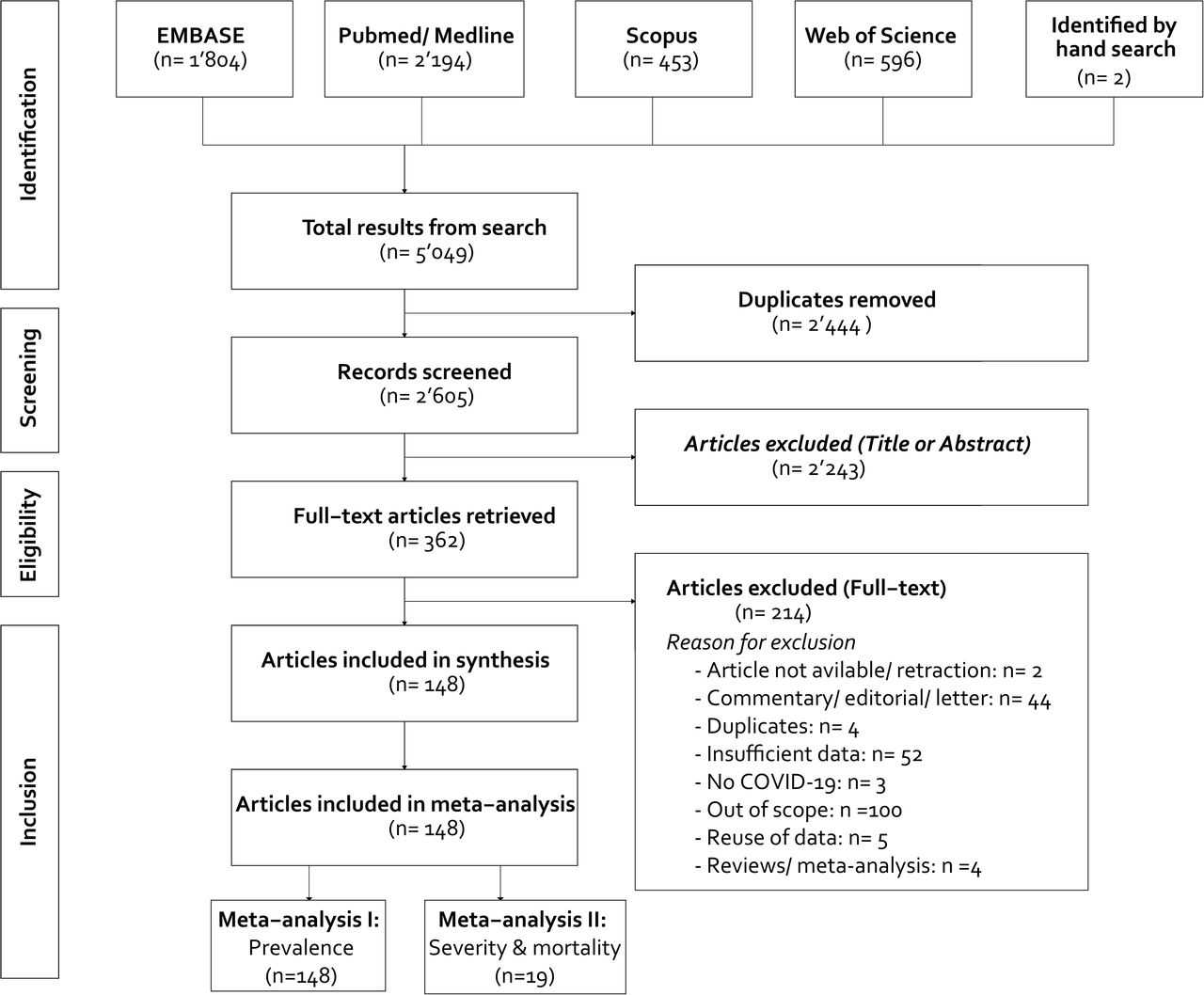
All full-text, peer-reviewed articles that described case-control, cohort studies, or case studies investigating the epidemiological and clinical features, comorbidities, laboratory parameters, imaging features, and/or treatment of patients that were diagnosed with COVID-19. We excluded duplicate publications, non-peer reviewed articles (e.g., preprints), reviews, meta-analyses, abstracts or conference proceedings, editorials, commentaries, letters with insufficient data, studies on non-human species, or out-of-scope studies (e.g., comparison with other infections, case-fatality reports). In case multiple studies published data from the same cohort, we included the article representing the most inclusive information on the population to avoid overlap. Lastly, studies that did not report demographics (i.e., age and sex) were also excluded. Figure 1 outlines our search strategy and application of inclusion and exclusion criteria.

A total of 148 studies were eligible for the literature review and the first part of the meta-analysis (i.e., prevalence). Nine-teen studies were included in the second part of the meta-analysis (i.e., severity and mortality).
2.4. Data extraction and synthesis
Data extraction tables were created with the following information: 1) publication information (i.e., author, date, language of article, country where the study was performed, study design [case study, case series, or cohort study]16, study population [pediatric/neonatal and adult COVID-19 patients including pregnant women); 2) demographics (i.e., age, sex); 3) clinical signs and symptoms (e.g., cough, fatigue, fever, sputum); 3) comorbidities (e.g., hypertension, diabetes, cardiovascular diseases); 4) therapies administered to treat COVID-19 (e.g., antibiotics, antivirals, invasive mechanical ventilation); 5) clinical outcomes (e.g., death, survival, recovery); and 6) complications associated with COVID-19 (e.g., sepsis and shock, ARDS). In case studies provided data for multiple patient groups(e.g., pediatric and adult patient), we extracted this information separately for each group. A full list of extracted variables is provided in Supplementary Table 1.
2.5. Statistical analysis
For the studies reporting mean and standard deviation (SD) for extracted variables, we computed the median and interquartile ranges (IQR) assuming a normal distribution (i.e., using the formula: IQR ∼ SD*1.35). To test if there is a bias by including the studies for which we computed the median and IQR (i.e., quartiles, Q1 and Q3), we performed a sensitivity analyses in which we calculated the median and IQR under the assumption of right-skewed and left-skewed distribution (see Appendix 2). We compared the results of the different distributions to test the robustness of our findings. Descriptive statistics (median, IQR, n, and %) were used to characterize the studies and patients included as well as the laboratory parameters. Weighted by study sample size, the pooled median and 95% confidence interval (CI) were computed for continuous variables. Normality approximation of the binomial was used to construct an approximate confidence interval (R package metamedian17). Welch’s two-sample t-test was employed to test if there are significant differences in the proportion of male and female patients across studies.
Our meta-analysis was structured in two parts. In the first part, we performed meta-analyses of all 148 studies to define the prevalence of comorbidities, clinical signs and symptoms, imaging features, treatments, outcomes, and complications associated with COVID-19. Using the metaprop function of the R package metafor18, we calculated the overall prevalence from studies reporting a single prevalence. Our meta-analysis was stratified by patient group (pediatric/neonatal [≤17 years of age], pregnant, and adult COVID-19 patients). Heterogeneity between studies was assessed visually by Forest plots, and analytically by I², tau T2, and Cochrane Q. Briefly put, I2 describes the percentage of variation across studies that is due to heterogeneity rather than chance19: 0% indicates no heterogeneity, whereas 25%, 50%, and 75% indicate low, moderate, and high heterogeneity, respectively. CIs for I² were calculated using the iterative non-central chi-squared distribution method of Hedges and Piggott20. Tau (T2) represents the absolute value of the true variance (heterogeneity) and is the estimated SD of underlying true effects across studies. Cochran’s Q is the weighted sum of squared differences between individual study effects and the pooled effect across studies, with the weights being those used in the pooling method (i.e., sample size)21. The second part comprised meta-analyses to calculate the relative risk (RR) of certain comorbidities, clinical signs and symptoms, imaging features, laboratory parameters, complications, and outcomes in patients with severe vs. those with non-severe disease condition (12 studies) as well as deceased vs. survivors (7 studies). The categorization into severe and non-severe COVID-19 disease was consistent with the groups reported by the reviewed studies (Supplementary Table 2). Owing to our judgment that considerable clinical and statistical heterogeneity exists among the studies (statistical heterogeneity was confirmed by the computed I2, T2, and Cochrane Q), we calculated pooled RRs with 95% CIs using a random-effects model with inverse-variance weighting (metabin function from R package meta). For continuous outcome data (e.g., age, laboratory parameters, and time from symptoms onset to hospital admission), we estimated the standardized mean difference (SMD) by means of a random-effect models with inverse variance weighting for pooling (metacont function from R package meta). To calculate the SMD, we converted medians, Q1s, and Q3s into means and standard deviations. The SMD, 95% CIs, and p values were reported. We produced Forest plots to visualize the results from the random-effect models (R function: forest). Publication bias was assessed visually by funnel plots (R function: funnel) and analytically by the Egger test (R function: regtest). An Egger test p<0·05 indicates a significant publication bias. All statistical analyses were performed in R (version 3.6.3) for MacOS X (Mojave, 10.14.4) with the packages meta (version 4.11–0) and dmetar (version 0.0.90)18. The code used for the analysis and to create figures and tables is provided in our GitHub repository (https://github.com/jutzca/Corona-Virus-Meta-Analysis-2020).
2.6. Role of funding source
The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
3. Results
Study selection and study characteristics
Our systematic literature search yielded 5’049 articles (including articles identified by manual searching). Upon removal of duplicates and exclusion of studies on the basis of their abstracts or following screening their full text, 148 met the inclusion criteria and were considered for the review and meta-analysis (Figure 1)4,8,28,118–127,29,128–137,30,138–147,31,148–157,32,158–165,33–37,9,38–47,11,48–57,22,58–67,23,68–77,24,78–87,25,88–97,26,98–107,27,108–117. The inter-rater agreement for study selection was very high (κ = 0·94 [95% CI: 0.91 –0.96], 97.0% agreement [11/ 362 studies with disagreement]). Detailed information on the included studies are provided in Tables 1–3. Included studies were conducted in 15 countries between December 1st, 2019 and March 28th, 2020 (Supplementary Table 3) and enrolled between 1 and 1’099 patients(median 12.5 [1.00 – 56.75]). The majority of the articles were written in English (123 studies, 83.1%) and the remainder in Chinese (25 studies, 16.9%). We classified studies according to their design16: cohort study (76 studies, 51.4%), case study/ report (41 studies, 27.7%), and case series (31 studies, 20.9%). While all studies reported information on demographics (148, 100%), the number of studies reporting information on comorbidities (84 studies, 56.8%), clinical sign and symptoms (130 studies, 87.8%), laboratory parameters (113 studies, 76.4%), imaging features (118 studies, 79.7%), treatments (91,61.5%), outcomes (118 studies, 79.3%), and complications (59 studies, 39.9%) varied markedly.
In terms of study population, 114 studies included only adult participants, 6 only pregnant women, 22 only children and neonates, and 6 included mixed cohorts. Of the total 12’149 patients included, 6’410 (52.8%) were male and 5’739 female (47.2%, Figure 2A and 2B). The median age of adult (11’058 patients, 91.0%), pregnant (35 patients, 0.3%), and pediatric (1’056 patients, 8.7%; including neonates) patients was 47.0 years [35.0–65.3] (Figure 3A), 30.0 [26.0–33.0] Figure 3B, and 10.0 [2.0–13.0] (Figure 3C), respectively. Approximately 7.8% (297/ 3’822 patients) were reported to be asymptomatic and 7.7% (617/ 8’047) died during hospitalization due to complications related to the infection with SARS-CoV-2. With the exception of one 10-month old child, all deaths were non-pregnant adult COVID-19 patients.

All case studies/ reports were pooled together for visualization (CS_adult, and CS_children [pediatric/neonatal]). The key to the study identifier can be found in Tables 1 (adults) and Table 3 (children).

Median age and interquartile ranges (IQR) are represented by the midpoints and error bars, respectively. The studies have been sorted by patients’ median age in years. The size of the midpoint (circle, square, triangle) indicates the study sample size. The red line indicates the pooled median age of the respective cohort. All adult case studies/ reports (CS_adult) were pooled for the visualization reasons. The key to the study identifier can be found in Table 1 (adults), Table 2 (pregnant women), and Table 3 (children).
Adult patients
Higher proportions of male than female patients were reported to be infected with SARS-CoV-2 (t = 2.678, df = 202, p-value = 0.008; Figure 2A) across all studies. Comorbidities were present in ∼31% of the adult patients (2’329/ 7’608), with hypertension being the most prevalent one (1’352/ 6’460 patients, 20.93%), followed by heart failure (37/ 354 patients, 10.5%), diabetes mellitus (678/ 6’535 patients, 10.4%), and coronary heart disease (194/ 2’388 patients, 8.5%) (Figure 4A, Table 4, Supplementary Figure 1). The most frequent clinical signs and symptoms were fever (6’955/ 8’859 patients, 78.5%), cough (4’778/ 8’885 patients, 53.8%), and fatigue (1’996/ 7’980 patients, 25.0%) (Figure 4B, Table 4). A little over five percent of the adult COVID-19 patients were asymptomatic (148/ 2’749 patients, 5.4%). Over 6’969 patients (89.6%) had abnormal CT imaging features. The most common patterns of CT abnormalities were indicating pneumonia (unilateral or bilateral; 6’620/ 7’917 patients, 83.6%), including air bronchogram (264/ 523 patients, 50.5%), and ground-glass opacity (GGO) with consolidation (153/ 323 patients, 47.4%) and without (2’446/ 5’591 patients, 43.8%) (Table 4, Supplementary Figure 2). In terms of laboratory parameters, inflammatory markers, such as interleukin 6 (22 pg/mL [4.68–51.8]), and erythrocyte sedimentation rate (32.5 mm/h [17.3–53.8]) were elevated across the adult population. Moreover, markers of coagulation, namely d-dimer (0.5 µg/mL [0.3–1.08]), fibrinogen (4.5 g/L [3.66–5.1]), and cell damage were also elevated (i.e., lactate dehydrogenase, U/L; 213 [173–268]). An overview of all laboratory parameters is provided in Supplementary Table 4. As shown in Figure 4D, the most common treatments were antivirals (4’475/6’068, patients, 73.8%), oxygen therapy (1’300/ 1’872 patients, 69.4%), and antibiotics (2’518/ 4’825 patients, 52.2%). Detailed information on all treatments is provided in in Table 4. Eight percent (616/7’727 patients) of the adults died during the hospitalization due to complications related to COVID-19. Amongst the survivors (7’111/ 7’727 patients, 92.0%), a total of 3’025 (68.7%) remained hospitalized, 1’751 (32.4%) were discharged, and 1’012 (27.1%) reportedly recovered (Figure 4C, Table 4). Important to note, for some patients it was stated that they both, recovered and were discharged (i.e., one patient can fall in multiple categories). The median duration between symptoms onset and hospitalization was 8 days [7 – 9.5]. A total of 195 (6.8%) patients were admitted to the intensive care unit (ICU). The most frequently reported complications associated with COVID-19 were pneumonia (1’032/ 1’489 patients, 69.2%), respiratory failure (141/ 413 patients, 34.1%), acute cardiac injury (242/ 1’250 patients, 19.4%), and ARDS (759/ 5’122 patients, 14.8%), (Figure 4D, Table 4).

The colors indicated the proportion of patients (%, 0 = yellow, 100 = dark purple). Note: Missing values are colored in white.
Pregnant woman
Studies investigating the effect of COVID-19 in pregnant women reported that only five pregnant women had any history of comorbidities. Hypothyroidism, allergies, or influenza were reported each for one pregnant woman (Supplementary Table 5). Fever (25/ 35 patients, 71.4%), cough (12/29 patients, 41.4%), and myalgia (3/ 9 patients, 33.3%) were the three most common symptoms observed in pregnant women that were infected with SARS-CoV-2 (Supplementary Figure 3, Supplementary Table 5). Abnormal CT features were evident in 88.6% (31/ 35 patients) of pregnant women diagnosed with COVID-19. Pneumonia (unilateral or bilateral, 31/ 35 patients, 88.6%), GGO (29/ 34 patients, 85.3%), and consolidation (8/ 16 patients, 50.0%) were among the most common patterns of CT abnormalities (Supplementary Figure 4, Supplementary Table 5). Inflammatory markers, such as C-reactive protein (19.25 mg/L [12.35–25.7]), procalcitonin (0.187 ng/mL), and neutrophil count (9.14 × 109/L) were elevated in this patient population. Along this line, lactate dehydrogenase concentrations were increased (544 U/L) reflecting cellular damage. An overview of all laboratory parameters is provided in Supplementary Table 4. Moreover, antibiotics (14/ 14 patients, 100.0%), antivirals (11/ 14 patients, 78.6%) and oxygen therapy (high flow nasal cannula; 3/ 12 patients, 25.0%) were used to treat pregnant COVID-19 patients (Supplementary Table 5). None of the pregnant COVID-19 patients died. Lastly, one patient was admitted to the ICU (Supplementary Table 5).
Pediatric and Neonatal Patients
Similar to the adult cohort, the proportion between female and male patients were comparable in the pediatric/neonatal cohort (t = 1.169, df = 26, p-value = 0.253; Figure 2B). Fourteen percent of the children and neonates were asymptomatic (149/ 1’054). With the exception of two children, no comorbidities were reported for any of the pediatric or neonatal patients (Supplementary Table 6). Similar to the adult and pregnant COVID-19 patients, children and neonates frequently presented with fever (170/ 320 patients, 53.1%), cough (149/ 311 patients, 47.9%), and sputum (14/ 51 patients, 27.5%) (Supplementary Figure 6 and Supplementary Table 6). Sixty-five percent of the pediatric and neonatal patients presented with CT abnormalities, including pneumonia (194/ 298 patients), GGO (108/ 278 patients, 38.9%), and local patchy shadowing (52/ 223 patients, 23.3%) (Supplementary Figure 7, Supplementary Table 6). An overview of all laboratory parameters is provided in Supplementary Table 7. As the reference values vary considerably within the pediatric/neonatal patient population, the results of the laboratory parameters have to be interpreted with caution. In terms of treatment, children and neonates received antibiotics (31/ 43 patients, 72.1%), oxygen therapy through high flow nasal cannula (5/ 9 patients, 55.6%), and alpha interferon aerosol inhalation therapy (31/52, 59.6%) to treat COVID-19 and its complications (Supplementary Figure 8, Supplementary Table 6). With the exception of a 10-month-old child that died four weeks after admission of multi-organ failure, all children survived. Less than 30% remained hospitalized (90/ 293 patients), 74.5% were discharged (216/ 290 patients) and 87.4% reportedly recovered (236/ 270 patients) (Supplementary Figure 9, Supplementary Table 6). The median duration between symptoms onset and hospitalization was 6 days [4.0–8.5]. Fifteen percent (6/ 39 patients) had to be admitted to the ICU. Complications associated with COVID-19 comprised pneumonia (16/ 26 patients, 61.5%), secondary bacterial infection (12/ 21 patients, 57.1%), and respiratory failure (10/ 33 patients, 30.3%) (Supplementary Table 6).
Non-severe vs. Severe
Twelve studies (2’596 patients) provided separate data for patients with a severe (500 patients, 19.3%) and non-severe disease status (2’096, 80.7%). No differences regarding sex were found between severe (t = 0.604, df = 16.645, p-value = 0.554; male: 278 patients [55.6%] and female: 210 patients [42.0%]; unknown sex: 12 patients [2.4%]) and non-severe disease status group (t = 0.217, df = 16.393, p-value = 0.831; male: 1’059 patients [50.5%] and female: 925 patients [49.5%]) (Supplementary Figure 10). In terms of age, patients with non-severe COVID-19 were significantly younger (median age in years = 45.0 [34.0–57.0]) than those with a severe disease progression (61.4 [44.5–75.5], Figure 5). Our meta-analysis revealed that older age (SMD: 0.68 [0.40–0.97]; p < 0.001), being male (RR = 1.11 [1.01–1.22]; p = 0.039), and preexisting comorbidities (RR = 2.11 [1.02–4.35], p = 0.046) were associated with a higher risk of increased disease severity. Specifically, hypertension (RR = 2.15 [1.64–2.81], p < 0.001), diabetes mellitus (RR = 2.56 [1.50–4.39], p = 0.005), any heart condition (RR = 4.09 [2.45–6.84], p < 0.001), and chronic obstructive pulmonary disease (COPD, RR = 5.10 [3.08–8.45], p < 0.001) (Figure 6, Table 5) were associated with worse outcome (i.e., severe disease). To test if the increased risk of heart conditions is attributable to the study that has classified their patients into severe and non-severe based on the presence or absence of cardiac injuries, we conducted a sensitivity analysis excluding these studies44. The risk of any heart condition remained significantly elevated in the severe disease patient cohort (RR = 3.87 [1.85 – 8.11], p = 0.005). Numerous laboratory parameters were significantly different between the non-severe and severe patient cohorts. Patients with severe disease status presented with decreased levels of albumin (SMD = 1.60 [−2.97 – (−0.24)]; p = 0.022), hemoglobin (SMD = –0.23 [−0.41-(−0.06)]; p = 0.001), and thrombocytes (SMD = –0.57 [−0.68-(−0.45)]; p < 0.001) in comparison to patients with non-severe disease status. Additionally, C-reactive protein (SMD = 1.47 [0.88–2.07]; p < 0.001), lactate dehydrogenase (SMD = 1.71 [1.08–2.34]; p < 0.001), and aspartate transaminase levels (SMD = 0.85 [0.61–1.09]; p < 0.001) were elevated in patients with severe disease status. In terms of complications, patients with severe COVID-19 disease were at an elevated risk of developing ARDS (RR = 10.59 [2.44–46.01], p = 0.014, Figure 6). The heterogeneity between the studies varied substantially (Table 5). Publication bias, measured by means of the Egger’s test, was only evident in three analyses. However, Egger’s test may lack the statistical power to detect bias when the number of studies is small (i.e., fewer than 10) as we only included 4–8 studies.

The median age and Interquartile ranges (IQR) are represented by the midpoints and error bars, respectively. The studies have been sorted by patients’ median age in years. The size of the midpoint indicates the study sample size. The red line indicates the pooled median age of the respective cohort. The key to the study identifier can be found in Table 1.

Funnel plots indicate the potential of publication bias. The key to the study identifier can be found in Table 1.
Survivor vs. non-survivors
Seven studies (957 patients) provided disaggregated data for COVID-19 survivors (617 patients, 64.5%) and non-survivors (340, 35.5%). No differences regarding sex were found in the survivor group (t = 0.258, df = 11.879, p-value = 0.801; male: 326 patients [52.8%] and female: 291 patients [47.2%]), but a significantly higher proportion of male patients were amongst the deceased cohort (t = 4.30, df = 12, p-value = 0.001; male: 236 patients [69.4%] and female: 104 patients [30.6%]) (Supplementary Figure 10). In terms of age, COVID-19 patients that survived were significantly younger (median age in years = 52.0 [35.0–66.0]) than non-survivors (68.0 [62.0–76.0], Figure 5). The meta-analysis yielded older age(SMD: 1.25 [0.78-1.72]; p < 0.001), being male (RR = 1.32 [1.13–1.54], p = 0.005), pre-existing comorbidities (RR = 1.69 [1.48–1.94]; p < 0.001) as potential risk factors of in-hospital mortality. Pre-existing cerebrovascular diseases (RR = 36.88 [8.50–160.04]; p = 0.009), heart conditions (RR = 3.95 [1.03–15.20], p = 0.047, Figure 7A), and hypertension (RR = 2.09 [1.65–2.64]; p = 0.001) were found to be associated with the highest risks of mortality. Clinical signs and symptoms as well as imaging features were comparable between survivors and non-survivors. In terms of treatments, non-survivors were more frequently mechanically ventilated than survivors (RR = 6.05 [1.41–26.05]; p = 0.026, Figure 7B) and more commonly received extracorporeal membrane oxygenation (RR = 4.39 [1.64–11.78], p = 0.014). Non-survivors had higher risks of complications, particularly acute kidney injury (RR = 20.77 [2.43–177.44], p = 0.017; Figure 7C) and ARDS (RR = 4.24 [1.30–13.83], p = 0.026, Figure 7D). Low levels of albumin (SMD = –1.13 [−1.41 – (−0.85)]; p < 0.001) and lymphocytes (SMD = –0.92 [−1.3 – (−0.55)]; p < 0.001) as well as elevated level of interleukin 6 (SMD = 1.21 [0.93 – 1.5]; p < 0.001), leucocytes (SMD = 2.21 [0.61 – 3.64]; p = 0.06), and prolonged prothrombin time (SMD = 7.99 [4.64 – 11.34]; p < 0.01) were associated with death (Table 5). Publication bias, measured by means of the Egger’s test, was only evident in five analyses.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plots indicate the potential of publication bias. The key to the study identifier can be found in Table 1.
4. Discussion
As of May 1st, 2020, more than 3.3 million confirmed cases of COVID-19 and more than 230’000 deaths attributable to the disease, have been reported worldwide166,167. In-depth knowledge of clinical, laboratory, and imaging factors that are associated with the disease progression and outcome is critical to inform clinical decision making and pandemic preparedness initiatives. An ever-growing number of research studies have been performed, but thus far the meta-analytical evidence is sparse. To address this paucity, we conducted a systematic review and meta-analysis of 148 studies involving over 12’000 patients providing an unprecedently comprehensive overview of comorbidities, clinical signs and symptoms, laboratory parameters, CT imaging features, treatment, outcomes, and complications in adult, pregnant, and pediatric/neonatal COVID-19 patients. Approximately eight percent of the patients were reported to be asymptomatic, while over seven percent died from complications associated with COVID-19. Recent analysis suggests that up to 75% of the coronavirus infections caused no illness168–170. Presumably, the virus has been circulating for longer than generally believed and large swathes of the population have already been exposed. Although our fatality rate lies within previous estimates171,172, it is important to mention that only a limited number of studies reported on the outcome of COVID-19 (i.e., death, survival, recovery) and thus, caution has to be exercised when interpreting this number. Through our meta-analysis, we revealed several important risk factors that are associated with severe disease progression and mortality. Among these risk factors were two demographic factors, namely older age and being male. Well-studied consequences of ageing are the decline in the immune function (e.g., T-cell and B-cell function) and excess production of type 2 cytokines173,174. These age-dependent changes in the immune response are suspected to cause deficiency in control of viral replication and more prolonged proinflammatory responses, potentially leading to poor outcome175. Corroborative evidence stems from preclinical studies that found an age-dependent host innate responses to virus infection in non-human primates inoculated with SARS-CoV-1176. Confirming previous findings177,178, sex-specific differences in mortality and vulnerability to the disease were evident in the current study. Specifically, men were disproportionately affected by an infection with SARS-CoV-2 (i.e., proportion of men presented with COVID-19 was larger compared to women) and the in-hospital mortality amongst male patients was significantly higher compared to female patients. Emerging evidence pinpoints towards differences in the immune system140, genetic polymorphism179, life style factors including smoking180, personal hygiene habits181, pre-existing comorbidities182,183, and expression of angiotensin-converting enzyme 2 (ACE2)184,185 as potential explanations for the increased vulnerability in men. This sex difference in vulnerability has also been observed for SARS and MERS186, two previously emerging coronavirus diseases. The lack of sex-disaggregated data in the reviewed studies made it impossible to further explore these potential explanations for the discrepant findings in men and women. Overall, the preexisting comorbidities, namely hypertension, diabetes mellitus, and any heart condition, were found to be linked with both, more severe diseases status and increased in-hospital mortality. Smoking, by contrast, was not associated with disease severity or mortality. However, the low number of studies reporting smoking status (13/ 148) cautions against early assumptions. Clinical signs and symptoms were comparable between patients with non-severe and severe COVID-19 as well as survivors and non-survivors. Fever, cough, and myalgia were amongst the most frequent reported symptoms across all groups. Similarly, the present study revealed no differences in the CT imaging features. The majority of the COVID-19 patients presented with pneumonia (bilateral or unilateral) and GGO. These pathological findings are a hallmark of any viral pneumonia, and thus it is not surprising that asymptomatic patients had similar distinctive features187. In terms of laboratory parameters, elevated levels of interleukin 6, leucocytes, d-dimer, and lactate dehydrogenase as well as hypoalbuminemia and lymphopenia were more commonly seen in patients with severe COVID-19 illness and non-survivors. High levels of d-dimer have a reported association with 28-day mortality in patients with infections or sepsis admitted to the intensive care unit188. Systemic pro-inflammatory cytokine responses (e.g., interleukin 6 and other components) contribute to host defense against infections, such as SARS-CoV-2189–191. However, exaggerated synthesis of interleukin 6 can lead to an acute, severe systemic inflammatory response syndrome (SIRS) known as ‘cytokine storm’192. In addition to SIRS, hypoalbuminemia and lymphopenia were previously shown to be associated with increased odds of severe infection and infection-related death193–195. Complications were very common amongst patients with severe COVID-19 disease (over 50%) and non-survivors (more than two thirds). Acute cardiac injury, ARDS, and acute kidney injury were strongly linked to the outcome. Widely used treatments for COVID-19 and associated complications comprised antibiotics, antivirals, and oxygen therapy. Patients with severe COVID-19 disease required more often mechanical ventilation and renal replacement therapy compared to those with non-severe COVID-19. Moreover, corticosteroids have been commonly administered to hospitalized patients with severe illness, although their benefit is highly disputed. Evidence from MERS or influenza suggests that patients who were given corticosteroids had prolonged viral replication, receive mechanical ventilation, and have higher mortality196–199. Administration of antibiotics and antivirals was independent of disease-severity.
Pregnant women as well as pediatric and neonatal patients may be less vulnerable to complications of COVID-19. Comorbidities were almost non-existent in these patient cohorts. Clinical signs and symptoms, laboratory parameters, imaging features, and treatments were comparable to the adult (non-pregnant) cohort. While there was a considerable proportion of children and neonates with SARS-CoV-2 infections reported, most of these patients did not need hospitalization and recovered quite well. With the exception of a 10-month old neonate, no children were amongst the deaths reported. All pregnant women included in our study survived COVID-19 and associated complications.
4.1. Limitations of review
A limitation of the current review was that literature search was limited to articles listed in EMBASE, PubMed/ Medline, Scopus, Web of Science, or identified by hand searches. Considering the pace at which the research in this area is moving forward, it is likely that the findings of the publications described in this paper will be quickly complemented by further research. The literature search also excluded grey literature (e.g., preprints, reports, conference proceedings), the importance of which to this topic is unknown, and thus might have introduced another source of search bias. There is also a probability of publication bias, as well as potential for a search bias. Publication bias is likely to result in studies with more positive results being preferentially submitted and accepted for publication. Moreover, geographical bias cannot be rule out as the majority of the studies (129/ 148) were conducted in China. While symptoms might be quite comparable across countries, comorbidities, treatments, and outcome potentially depends on the country (and its healthcare system). There is also a considerable risk for a reporting bias towards comorbidities, clinical signs and symptoms, laboratory parameters, imaging features, treatment, outcome, and complications that are present. Specifically, only a minority of studies reported a zero when this information was assessed, but absent in patients. Lack of data on absent clinical signs and symptoms might lead to distorted estimates of proportion. The meta-analysis of severity and mortality could only be performed with a small number of studies as the minority of the 148 provided data separately for different disease severity groups (e.g., non-severe, severe, survivors, non-survivors). This needs to be considered when interpreting the results, including the publication bias as the Egger’s test may lack the statistical power to detect bias when the number of studies is small (i.e., < 10). Lastly, the criteria to classify patients in severe and non-severe COVID-19 disease cohorts varied between studies leading to additional heterogeneity between studies. By virtue of low number of studies available, we could not assess this heterogeneity nor adjust for it.
4.2. Conclusion and future directions
In conclusion, this unprecedentedly comprehensive systematic review and meta-analysis of the literature published during the first 120 days of the COVID-19 pandemic yields important information regarding the comorbidities, clinical signs and symptoms, laboratory parameters, imaging features, treatment, outcome, and complications. Male sex, older age, and pre-existing comorbidities are major risk factors for in-hospital mortality and complications. This study revealed a fatality rate of 7.7% and found that approximately 8% of the patients were reportedly asymptomatic. Based on recent reports, the latter number is likely 6- to 10-fold higher as only a few asymptomatic patients are captured by the health care system as they do not seek medical attention due to the lack of symptoms168 or are not hospitalized and thus, included in studies. Unnoticed asymptomatic cases of COVID-19 are likely a major source of ongoing transmission. Children and neonates appear to be the least vulnerable cohort. Forthcoming studies are needed that provide sex-disaggregated data to better characterize risk factors that affect both sexes or are specific to men or women, respectively.
Data Availability
The code used for the analysis and to create figures and tables is provided in our GitHub repository (https://github.com/jutzca/Corona-Virus-Meta-Analysis-2020).
Authors’ contribution
Catherine Jutzeler
Substantial contributions to the conception and design of the study; acquisition, analysis, and interpretation of data, drafting the manuscript, final approval of version to be published.
Lucie Bourguignon
Substantial contributions to acquisition, analysis, and interpretation of data, drafting the manuscript, final approval of version to be published.
Caroline Weis
Acquisition and interpretation of data, revising the manuscript critically for important intellectual content, final approval of version to be published.
Bastian Rieck
Acquisition and interpretation of data, revising the manuscript critically for important intellectual content, final approval of version to be published.
Bobo Tong
Acquisition and interpretation of data, revising the manuscript critically for important intellectual content, final approval of version to be published.
Cyrus Wong
Acquisition and interpretation of data, revising the manuscript critically for important intellectual content, final approval of version to be published.
Hans Pargger
Substantial contributions to the interpretation of data, revising the manuscript critically for important intellectual content, final approval of version to be published.
Sarah Tschudin-Sutter
Substantial contributions to the interpretation of data, revising the manuscript critically for important intellectual content, final approval of version to be published.
Adrian Egli
Substantial contributions to the interpretation of data, revising the manuscript critically for important intellectual content, final approval of version to be published.
Karsten Borgwardt
Substantial contributions to the interpretation of data, revising the manuscript critically for important intellectual content, final approval of version to be published.
Matthias Walter
Substantial contributions to the conception and design of the study; acquisition, analysis, and interpretation of data, drafting the manuscript, final approval of version to be published.
4.3. Conflict of interest
The authors do not report any (financial or otherwise) conflict of interest.
4.4. Acknowledgement
This study was supported by the Alfried Krupp Prize for Young University Teachers of the Alfried Krupp von Bohlen und Halbach-Stiftung (Borgwardt), and the Swiss National Science Foundation (Ambizione Grant [PZ00P3_186101, Jutzeler], SNSF Starting Grant [155913, Borgwardt}). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
5. References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.
- 35.
- 36.
- 37.↵
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.↵
- 45.
- 46.
- 47.↵
- 48.↵
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.↵
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.↵
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.↵
- 78.↵
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.↵
- 88.↵
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.↵
- 98.↵
- 99.
- 100.
- 101.
- 102.
- 103.
- 104.
- 105.
- 106.
- 107.↵
- 108.↵
- 109.
- 110.
- 111.
- 112.
- 113.
- 114.
- 115.
- 116.
- 117.↵
- 118.
- 119.
- 120.
- 121.
- 122.
- 123.
- 124.
- 125.
- 126.
- 127.↵
- 128.
- 129.
- 130.
- 131.
- 132.
- 133.
- 134.
- 135.
- 136.
- 137.↵
- 138.↵
- 139.
- 140.↵
- 141.
- 142.
- 143.
- 144.
- 145.
- 146.
- 147.↵
- 148.↵
- 149.
- 150.
- 151.
- 152.
- 153.
- 154.
- 155.
- 156.
- 157.↵
- 158.↵
- 159.
- 160.
- 161.
- 162.
- 163.
- 164.
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.
- 170.↵
- 171.↵
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.↵
- 183.↵
- 184.↵
- 185.↵
- 186.↵
- 187.↵
- 188.↵
- 189.↵
- 190.
- 191.↵
- 192.↵
- 193.↵
- 194.
- 195.↵
- 196.↵
- 197.
- 198.
- 199.↵



