
Abstract
Background Many countries have successfully managed to stop the exponential spread of SARS-CoV-2. Still, the danger of a second wave of infections is omnipresent and it is clear that every containment policy must be carefully evaluated and possibly replaced by a different, less restrictive policy, before it can be lifted. Contact tracing and consequential breaking of infection-chains is a promising strategy to help contain the disease, although its precise impact on the epidemic is unknown.
Objective In this work we aim to quantify the impact of tracing on the containment of the disease.
Design We developed an agent-based simulation model that simulates the spread of the disease and allows for exploratory analysis of containment policies. We apply this model to quantify the impact of contact tracing in different characteristics in Austria and to derive general conclusions on contract tracing.
Results This modelling study displays the dynamics of the interplay between strictness of the tracing policies, isolated persons, and active COVID-19 infections. It shows that a strict tracing policy does not necessarily imply that the total number of quarantined persons is high as well, because the disease is better contained.
Limitations The results are limited by the validity of the modeling assumptions, model parameter estimates, and the quality of the parametrization data.
Conclusions The study shows that tracing is indeed an efficient measure to keep COVID-19 case numbers low but comes at the price of too many precautious quarantined people if the disease is not well contained. Therefore, contact tracing must be executed strictly and compliance within the population must be held up to prevent new disease outbreaks.
1 Introduction
In the middle of April 2020 the SARS-CoV-2 coronavirus was heavily spreading and not many countries worldwide have managed to stop the exponential increase of case numbers (for example, see situation report 88 by the World Health Organization (1)). By that time, besides a few countries in Asia, such as China and South Korea, most countries in Europe have succeeded in containing the disease due to swift and rigorous government policy making. This averted a potential overload of their health care systems, as happened in Lombardy in March (2,3) or in Wuhan in January (4). Of these European countries – including Germany, France, and Norway – Austria stands out by virtue of its especially fast policy making, which allowed the country to rapidly overcome the first disease wave.
Most of the introduced policies, such as the closure of schools, shops and restaurants, appear to have been effective in stopping the initial growth of the pandemic. However, due economic and social reasons, lockdown policies cannot be upheld long enough to eradicate the disease completely (5). After a certain time, most of them must be lifted again, while other measures must be enforced to prevent a new upswing of the disease.
Contact tracing seems to be a viable method to keep the epidemic at bay. It allows for the detection and isolation of potentially infected contacts even before they become infectious, leading to successfully broken infection-chains. Yet, besides many successfully detected and isolated new infections, many healthy contacts would also be put into quarantine this way. This results in unintended adverse in particular mental health effects (6) and economic losses.
Although stigmatized as a violation of personal freedom, tracing is not always related to personal data-tracking devices like mobile apps (7). Successful tracing of contacts starts by isolation of household members or by temporarily closing workplaces of confirmed COVID-19 patients. Many potentially infectious contacts can be traced by a simple patient interview as well.
Finding evidence that proves or quantifies the success of different tracing strategies is still difficult due to the novelty of the situation. Simulation models are currently the only opportunity to estimate the future impact of strategic changes. In Austria, simulation results are systematically used by the ministry of health and public health authorities to guide health policy decision making and planning. The authors of this study are part of this process (8).
In this study, we develop and apply an agent-based model (ABM) fully documented in the Methods section and the Appendix. In contrast to typical aggregated compartment models such as the classic SIR model by Kermack and McKendrick, (9) agent-based models (ABM) do not treat the populations as one continuously changing variable, but as the aggregate of individually modelled entities, so called agents (10,11). Consequently, not only the transmission of the disease, but also policies like contact tracing can be modeled via agent-agent-interaction laws posing a very low level of abstraction compared to reality. Moreover, also the stochastic nature of the transmissions in reality is modeled as such.
Key objectives of this work are to qualitatively and quantitatively analyze tracing as a containment policy for COVID-19. We will define formal measures for success and costs of a policy and define differently strict tracing strategies. With respect to these measures, we ask which strategy is the most successful, comes with the least social and economic costs, under which circumstances it works best, and if the disease is contained by this measure alone, or whether additional policies are required.
2 Methods
For the development and analysis of our model, we followed the international guidelines of the ISPOR-SMDM Joint Modeling Good Research Practices Task Force (12,13) in the selection and justification of the model type as well as the description of methods and the reporting of our results.
We applied an agent-based modelling strategy in which each inhabitant is statistically represented by a model agent with certain demographic and disease related features. Disease transmission occurs via contacts between agents which occur inside of locations where agents interact with each other. The model is capable of introduction of certain policies, in particular different tracing strategies, that change the behavior of agents and/or transmission behavior of the disease.
2.1 Model Type
The chosen agent-based modeling type is a complex approach for simulation of epidemics. There are widely used simpler simulation methods, such as the classic SIR cohort model by Kermack and McKendrick (9), which uses a system of differential equations and is deterministic in nature. These simpler strategies would be preferred if the modeling purpose only considered simulation of the epidemic. Yet, modeling of contact tracing policies requires modeling of person-to-person contacts which excludes population-based model types (see (13)). Consequently, a stochastic agent-based approach is necessary.
The model is comparable with similar models developed for Australia (14) and the UK (15) but stands out by several features described in detail below. Briefly, (a) our model is based on a very accurate spatial and demographic image of the Austrian population in which each Austrian inhabitant is represented as an agent; (b) it utilizes a contact network based on different locations, such as households, workplaces, and schools; and (c) it allows for tracing of agent-agent contacts and, consequently, for analysis of related tracing policies.
2.2 Decision-analytic Framework of the Policy Question
The target population of our study is the entire population of Austria in 2020. The analytic time horizon of our analysis is February 21st to December 31st, 2020. The time span between April 9th and December 31st is used for different simulations comparing tracing-policies. The interval from February 21st to April 9th is used for a so-called initialization simulation, that is (1) used for calibration of specific parameter values and (2) to generate an initial agent population for the strategy comparison simulations.
Regarding comparison, we evaluate 6 different tracing strategies with three scenarios each: 1 strategy without tracing, 3 strategies with location tracing (household tracing, workplace tracing, combined household and workplace tracing), and 2 different strategies of direct contact tracing (see Section 2.5.3 and 2.5.4). All strategies are compared for 3 different assumptions for contact reduction compliance of the population (see Section 2.5.2).
In addition, we also analyze the outcomes of the calibration simulation (February to April), specified in Section 2.5.1. It has no direct relation to the comparison of tracing strategies but reveals interesting insights into the epidemic.
We use our simulation to observe the timeline of the total number of COVID-19 cases, both active and cumulative. We distinguish between the different stages of the disease (pre-symptomatic, unconfirmed symptomatic, confirmed, undetected). Moreover, we observe the total number of agents quarantined due to tracing measures.
Compared to other models, we use a large number of parameters which are obtained from various data sources (Tables A1-A5 in the Appendix).
Population parameters including fertility, mortality, and migration are parametrized via official publicly available census data from the Austrian national statistics office Statistics Austria (16). Parameters related to contact behavior are primarily based on the POLYMOD contact survey (17), but also on open source data from Statistics Austria and the official data repository of the city of Vienna about household structure, employment rate, schools and workplaces (18–20).
COVID-19 related parameter values are based on recently published literature, expert opinions, the official disease reporting system of Austria and calibration processes. Time intervals (such as incubation time, disease duration, etc.) are parametrized using information from published literature (21,22) and opinions from local virology experts from the Austrian Ministry of Health. Hospitalization ratios and age distributions are gathered from statistical postprocessing of data from the official COVID-19 reposting system of Austria, the Elektronisches Meldesystem (EMS, (23)). The probability of having an undetected disease progression is based on early antibody tests from Iceland (24). Finally, the infection probability and the impact of the already implemented lockdown measures in Austria were calibrated, using the officially reported Austrian COVID-19 cases by EMS as a reference.
For more details on the model parametrization, the reader is referred to the Appendix, Section A1.3.4.
2.3 Model Specification
According to the Modeling Good Research Practices guidelines (12) we offer a short, but easy understandable model description here. For a detailed and reproducible description, the reader is referred to the Appendix, Section A1.
The agent-based model is stochastic and population dynamic. It depicts each inhabitant of Austria as one model agent. It uses sampling methods to generate an initial agent population with statistically representative demographic properties and makes use of an discrete-event simulator to update time.
Model Input. The model’s input consists of a timeline of policy events that change the dynamics of the model at certain dates, based on which different strategies can be compared. In the simulation, each element of this timeline is translated to an event-notice scheduled at the specified time. As soon as the event takes place in the simulation, the specified policy is executed by changing certain parameters or model mechanisms.
Model Initialization. To begin the simulation, the model generates the initial agent population, that is one agent per Austrian inhabitant. Therefore, a population sampling routine is run that has been implemented in a prior research project (see DEXHELPP (25)). This sampling routine, a part of the Generic Population Concept (GEPOC, see (26)), ensures that the demography of Austria is accurately represented by the agent-population, that is, statistically correct age, sex, and residence, in form of a GPS coordinate, of each agent.
Moreover, the start date of the COVID-19 simulation model must be a point in time between March 2020 and the current day and may be run arbitrary long. To start the simulation at the defined point in time, say to, the model applies an initialization-simulation run from February 2020 until t0 to (1) calibrate the model parameters to the timeseries of the confirmed COVID-19 cases in Austria until t0, and (2) generate a valid initial agent-population for the actual simulation. Hereby it guarantees, that the correct number of susceptible, infectious, hospitalized, etc., model agents are present, when the actual simulation is begun.
The dynamics of the model are given by the interplay of four different submodels, a population, contact, disease, and policy model.
Population Model. First, agents are constantly affected by particular demographic changes. Based on mortality and fertility rates, each agent has a certain time and age dependent probability to die or produce offspring any time during the simulation. Migration behavior is not present in the model, due to the closed borders of Austria during the pandemic.
Contact Model. The model makes use of a location specific contact model to establish interactions between agents. Hereby, agents meet daily at workplaces, schools, households and in leisure-time, by which they can transmit the virus with a certain transmission probability if they are infectious.
Disease Model. After being infected, agents go through a detailed disease and/or patient pathway that depicts the different states of the disease and the treatment of the patient. This pathway is modeled via a distributed transition times specifically and is not Markovian. It contains branches with respect to disease severity (asymptomatic or symptomatic, etc.), and with respect to treatment (hospitalization or home isolation, normal bed or intensive care unit, etc.) and always ends in the recovery of the agent. Disease related mortality is not regarded as related research questions have not been within the modeling purpose yet. The disease severity and treatment states influence the contact behavior of the agent and, consequently, its probability of transmitting the virus.
Policy Model. Clearly, not only the disease and treatment state, but also the currently active policies influence the contact behavior of agents. Policies may lead to closure of certain locations, which make them unavailable for contacts, but may also cause a reduction of contacts or a reduction of the infectivity of contacts due to increased hygiene. We focus on tracing policies which mandate additional quarantine at home for contacts of newly infected agents. This removes traced contacts from the contact network and reduces their capacity to transmit the disease.
Model Output. The outcomes of the model are presented as a time series, with new outcomes projected each day. The outputs consist of aggregated numbers describing the current nation-and/or region-wide spread of the disease, as well as the contact behavior of agents. These include, for example, the cumulative number of confirmed cases, the number of currently active asymptomatic cases, the total number of daily new infected 10-to-30 year-old females, the total number of daily contacts for school children, or the average number of secondary infections per agent (=Reff). The outcomes particularly observed for this study are the total (active and cumulative) number of COVID-19 cases with different degrees of severity and the total number of persons quarantined via tracing measures.
2.4 Model Implementation
The simulation of ABMs like the COVID-19 described above is a huge challenge with respect to computational performance. As the model cannot be scaled down, almost 9 million interacting agents need to be included in the model to simulate the spread of the disease in the entire population of Austria.
These high demands exclude most of the available libraries and software for agent-based modelling including AnyLogic, NetLogo, MESA, JADE, or Repast Simphony (27–31). Most of these simulators cannot be used as their generic features for creating live visual output would be too computationally demanding.
Consequently, we decided to use our own agent-based simulation environment ABT (Agent-Based Template, see (32)), developed in 2019 by dwh GmbH in cooperation with TU Wien. The environment is implemented in JAVA and specifically designed to support the reproducible simulation of large-scale agent-based systems. More technical details are found in the Appendix, Section A2.
2.5 Strategies and Scenarios
In this section, we define in more detail the tracing strategies and compliance scenarios mentioned in 2.2. These scenarios are divided into the following four sections: the initialization phase of the model is defined in 2.5.1, the three scenarios in which compliance is varied are described in 2.5.2., the reference strategy without tracing and the three strategies dealing with location tracing are defined in 2.5.3, and two strategies with different types of individual tracing are specified in 2.5.4. Figure 1 shows a diagram of all scenarios and policies evaluated in this work.
At some points, the specification of the strategies and scenarios are not fully reproducible to support readability. For tables containing the precise, reproducible model parametrization we refer to the Appendix, Section A3.

Diagram depicting all simulation scenarios and strategies compared in this work. The initialization phase stands out of this process having a different time-horizon and goal. The lines indicate that the different scenarios regarding compliance are evaluated in combination with each of the connected strategies.
2.5.1 Definition of the Initialization Phase
We chose April 9th, 2020, 08:00 AM as the initial time of our actual simulation – we will henceforth denote this time as. To start the simulation at this date, it is necessary to run an initialization phase that validly depicts the entire progression of the disease until this date. The final state of this phase is then saved as an input to the actual simulation. Interestingly, this initialization phase also reveals interesting insights into the disease which cannot be measured in the real world, such as the time series of all those cases which are not (yet) confirmed by a positive test.
By April 9th, a nationwide lockdown in Austria had already managed to reduce – the effective reproduction rate of the disease – below 1, causing the number of newly infected people per day to decrease. About 12,900 positive virus tests had been reported by this date 1. To guarantee that the final state of the model matches this number, a calibration process was performed adjusting both infectivity and impact of lockdown policies. This process is described in more detail in the Appendix, Section A1.3.4. The country implemented nationwide closure of schools and workplaces on March 16th, yet our calibration process revealed that this lockdown should rather be modelled as a process with several steps, which are briefly listed in the Appendix, Table A6. It is clear, that the modeled policy events – and, in particular, their parameter values – cannot be evaluated separately. Some of them might have a larger, some a smaller impact in reality than the model – yet the policies are feasible assumptions that permit a causal interpretation of the model input parameters when taken together.
2.5.2 Definition of Compliance Scenarios
To set the assumptions for the sensitivity of the strategies, three hypothetical compliance scenarios (high, medium, and low) are defined by varying the compliance of the population to maintaining hygiene and physical distancing practices.
All three define a fictional disease progress from t0 (April 9th, 2020) under the ongoing lockdown policies and consider the subsequent lifting of the implemented measures. In all three scenarios, the lockdown policies are almost fully lifted on May 1st. Contacts in schools, workplaces and households are back at their baseline level and only leisure time contacts are slightly reduced. Here the compliance is varied by different assumptions of the population to maintain leisure time distancing standards and the quantity of leisure time contacts:
high compliance: Leisure time infection probability is reduced by 50%, contact numbers are reduced by 75%.
medium compliance: Leisure time infection probability is reduced by 50%, contact numbers are reduced by 50%.
low compliance: Leisure time infection probability is reduced by 50%, contact numbers are not reduced at all.
A detailed specification of the compliance scenarios can be found in the Appendix, Table A7.
We want to emphasize that the disease progression scenarios defined here are not designed to represent the current or future situation in reality, but rather function as a broad sensitivity analysis. For example, they do not include school closings during the summer or other holidays, and weekends are not considered either. Furthermore, we assume an unlimited testing capacity such that, even at the height of the epidemic, all symptomatic persons can be tested without increasing the reaction time between symptom onset and becoming a confirmed case. Yet, the scenarios allow us to focus solely on the specific impact of tracing related policies without any other disturbances. In particular, they are chosen so that none of the tracing policy scenarios pushes Reff below the critical threshold Reff =1. Having such a bifurcation within the parameter study would make it impossible to compare any two scenarios quantitatively.
2.5.3 Definition of No-Tracing and Location Tracing Strategies
In the simulation, all tracing policies are implemented on May 15th, a time when the new upswing of the epidemic can already be observed by an increasing number of new infections, independent of the compliance level.
To create a reference for evaluation of tracing strategies, we specified a no-tracing strategy in which no tracing is present whatsoever. As soon as an infected person agents becomes a confirmed case, they isolate themselves, but there are no consequences for their contacts whatsoever.
As the first tracing strategies to evaluate we defined so-called location tracing policies. While isolation of the affected person is done as usual, now all persons in the immediate physical surroundings of the infected person will become isolated as well, independent of their current disease state. In this process, the surrounding is defined as the group of persons that commonly visit the same locations as the infected person. By this measure we expect to find and isolate a high percentage of infected persons before they even become visible to the system.
In this work, we studied the effects of location tracing regarding two location types: household and workplace. The policy household tracing means that as soon as an agent enters the confirmed infection status, all other members of the agent’s household are isolated as well. In workplace tracing, the workplace of a confirmed COVID-19 patient is temporarily closed, and all the coworkers are put into preventive quarantine.
In isolation, agents only have contacts with the other members of their household. They do not attend school or work and do not have leisure time contacts. After a fixed number of days – we chose 14 days for our strategies – agents are released from isolation and can resume their normal behavior, if they turn out to be unaffected by the virus. Clearly, the availability of a precise test could reduce the required quarantine length, yet this feature is not included in the model thus providing conservative estimates.
We evaluated the impact of the location tracing for households and for workplaces separately as well as in combination, henceforth denoted as combined tracing strategy.
2.5.4 Definition of Individual Tracing Strategies
Extending the ideas of location tracing, we studied the effects of individual tracing of contacts. For this tracing policy, we assume that a certain amount of people track their contacts outside of their household, for instance, by using a tracing app on their smartphone or on a similar device. In this process, a contact is recorded if both involved persons use the tracing device. These contacts are saved for a specific recording period. If a person using the tracing device becomes a confirmed case of COVID-19, the recorded contacts are informed and placed under preventive quarantine. The implications of the preventive quarantine are the same as in Section 2.5.3.
The effectiveness of this policy has been evaluated on top of the location tracing policies for households and workplace contacts, that is, the combined tracing strategy. We considered rates of 50% and 75% of people using the tracing device and a recording period of 7 days. The length of the preventive quarantine is fixed at 14 days.
2.5.5 Outcome Measures
To evaluate and compare the stated strategies, we considered the reduction in the peak number of active confirmed cases, as well as the peak number of agents currently placed in preventive quarantine. As a measure for the effectiveness of the policy, we defined the costs c by
 where pq denotes the peak number of people in preventive quarantine, and rc denotes the absolute reduction in the peak number of confirmed cases compared to the corresponding baseline. The usefulness of this cost function is best explained based on examples: Suppose, two strategies lead the same reduction of the peak height, then the one with a smaller number of preventive quarantined persons leads to the smaller cost value and is considered as superior. Suppose, two strategies require the same number of quarantined people, the one with the higher peak reduction leads to a smaller cost value and should be preferred.
where pq denotes the peak number of people in preventive quarantine, and rc denotes the absolute reduction in the peak number of confirmed cases compared to the corresponding baseline. The usefulness of this cost function is best explained based on examples: Suppose, two strategies lead the same reduction of the peak height, then the one with a smaller number of preventive quarantined persons leads to the smaller cost value and is considered as superior. Suppose, two strategies require the same number of quarantined people, the one with the higher peak reduction leads to a smaller cost value and should be preferred.
3 Results
3.1 Initialization Phase
In the initialization phase the infectivity as well as various lockdown policies have been calibrated to fit the observed epidemiological data from Austria. This calibration process lead to a strong reduction of contacts at the day of the lockdown: On average, by March 16th, the modelled total contacts per day were reduced by about 78%, with additionally reduced infectivity of contacts at the workplace and in leisure time by 50%. As mentioned in the model description, the calibrated model provides the opportunity to carry out estimates for the reproduction numbers Reff and, most importantly, R0. The fitted model results indicate R0 ≈ 4.5.
Figure 1 depicts the results of the initialization phase. It clearly displays that the confirmed cases are only one part of the total infected population and that it is necessary to consider all of them to generate a plausible initial population at t0: the asymptomatic, that never feel any or only mild symptoms and remain undetected, the pre-symptomatic, that are still within the incubation period, and the unconfirmed symptomatic, that have not yet reacted on their symptoms or are waiting to be tested.
For calibration purposes, a bisection algorithm was applied iteratively, improving the value of one parameter value after the other. This strategy is possible as the impact of the calibrated parameters can be measured at different points in time: the base infection probability can be calibrated in the period before the introduction of control measures, the impact of the first policy can be calibrated in the period between the first and the second, and so on. Hence the multi-dimensional calibration problem can be decoupled into several scalar ones. More on this strategy is found in the Appendix, Section A1.3.4.

Comparison of the initial phase and reported data from Austria. Upper plot shows active cases while the lower plot displays cumulative.
3.2 No-Tracing Strategy
Without tracing, all hygiene and distancing compliance scenarios (high, medium and low, defined in Section 2.5.2) led to a new upswing of the disease around 14 days after the lifting of the lockdown policies. In the scenario with low compliance, the epidemic reaches a peak of around 2.47 million confirmed cases (28% of the population) approximately 9 weeks after the end of the lockdown. In total, the model contained 4.25 million confirmed infected agents (47% of the population) and 8.5 million total infected agents (95% of the population), which includes asymptomatic and pre-symptomatic agents as well.
In the scenario with medium compliance, the peak of the confirmed cases is reached around 11 weeks after the lifting of the lockdown policies with a value of 1.86 million confirmed infected agents (21% of the population). At the end of the pandemic, there has been a total of 3.87 million confirmed cases (43% of the population) and 7.74 million total infected agents, which accounts for 86% of the population. Compared to the low compliance scenario, the reduction of leisure time contacts in this scenario led to a 26% reduction of the confirmed infected cases at the peak of the epidemic.
In the high compliance scenario, the epidemic reached a peak of 1.43 million confirmed infected agents (16% of the population) 12 weeks after the lifting of the lockdown policies. Around 3.44 million agents (38% of the population) were confirmed in total, 6.88 million agents were infected (77% of the population). The further reduction of leisure time contacts managed to reduce the peak of the epidemic by 42% compared to the scenario with low compliance.
The simulated time series for the confirmed infected agents in the no-tracing strategy are displayed in Figure 3.

Simulation of the no-tracing strategy for the high, medium and low compliance scenario. The plot is split into two parts to allow a detailed image of the different scales without logarithmic scaling.
3.3 Location Tracing Strategies
Result plots of the three location tracing strategies household, workplace and combined tracing, defined in 2.5.3 can be seen in Figures 3-5 and Table 1, respectively. The results show that location tracing based on shared workplaces achieves a peak reduction by about 30% regardless of the compliance level, whereas the household tracing performs better with an increasing compliance. Moreover, household tracing leads to a slight delay of the epidemic peak. For all three compliance levels, combined tracing for households and workplaces achieves the greatest peak reduction, performing better with a higher level of compliance. The combined tracing scenario also achieves the lowest cost values indicating that the ratio between preventive quarantined persons and peak reduction is more favorable.
Simulation results for location tracing policies
3.4 Individual Tracing Strategies
The results of the individual tracing strategy, defined in Section 2.5.42.5.4, are shown in Figures 4-6 and Table 2.
Simulation results for individual tracing policies
For all levels of compliance, individual tracing manages to further decrease the epidemic peak without increasing the peak of the people placed under preventive quarantine. Interestingly, the reduction of the epidemic peak achieved by a tracing rate of 75% does not vary much based on the compliance level. However, since the height of the epidemic peak decreases with an increasing compliance level, fewer people must be placed under preventive quarantine to achieve this reduction. Thus, with an increasing level of compliance tracing becomes more efficient which is also indicated by the lower cost values.

Comparison of the total number of confirmed cases for six different tracing strategies displayed for the low compliance scenario.

Comparison of the total number of confirmed cases for six different tracing strategies displayed for the medium compliance scenario.

Comparison of the total number of confirmed cases for six different tracing strategies displayed for the high compliance scenario.
4 Discussion
In the course of this study we implemented an agent-based simulation model that is not only calibrated to match the previous course of the COVID-19 epidemic wave in Austria, but is also capable of making comparisons between various non pharmaceutical intervention strategies. In this study we applied this model to compare tracing policies in different characteristics and evaluated them with respect to social and economic costs in the form of the number of people placed under preventive quarantine.
4.1 Evaluation of Tracing Policies
The model results indicate that tracing, in any form, is an effective policy to contain the disease and can substitute lockdown policies if combined with additional contact reduction. Yet, isolating persons due to a preventive quarantine measure is always related to unintended economic and sociopsychological adverse effects. Consequently, any tracing measure should focus on keeping the total number of isolated persons as small as possible.
Some very interesting dynamics occur due to the interplay of two feedback loops which are depicted in Figure 7. If the feedback loop of the infectious and infected persons dominates the system, a lot of new infections will increase the number of persons in preventive isolation and therefore the economic costs. Increasing the strictness of the tracing measure, i.e. tracing more rigorously, will contribute to making the right feedback loop dominant, thereby containing the disease. Yet, it directly increases the number of quarantined people at first. Combined with high compliance among the population, both the infected and the preventive isolated people can be kept at a low level.
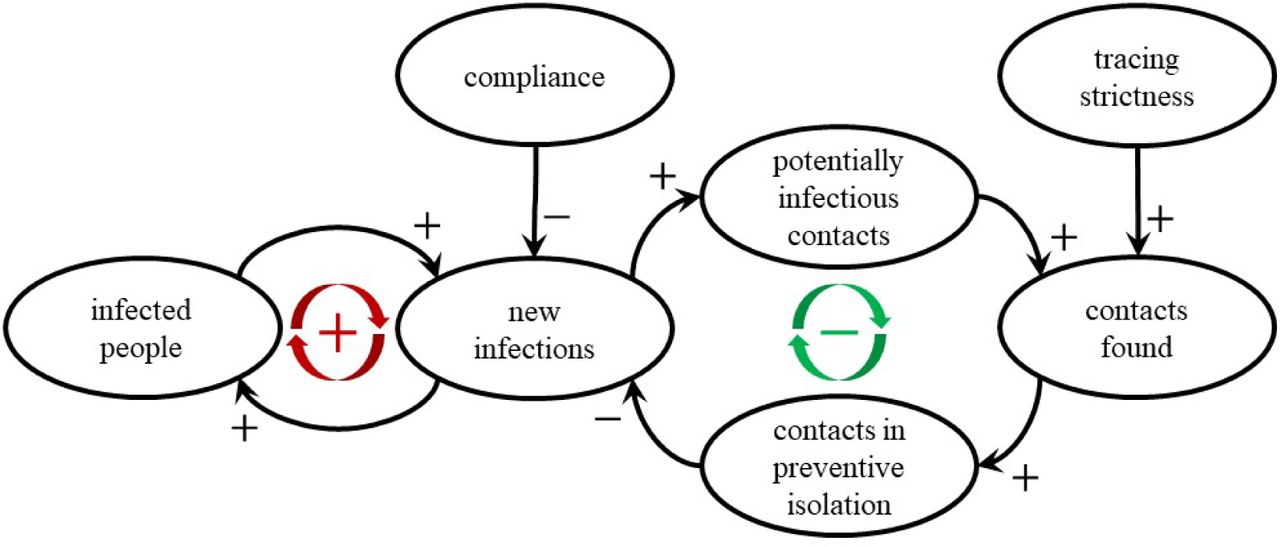
Causal Loop Diagram of relevant system components with respect to tracing measures. The more dominant the feed-back loop on the left-hand side relative to the right side, the more potentially infectious contact partners need to be isolated to contain the disease.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Impact of all location and individual tracing policies on both the epidemic peak of the active confirmed cases and the number of persons isolated at home. Although tightening the policies leads to a higher number of quarantined people at first, the number of isolated persons tends to decrease with the epidemic peak size if the policies are effective.
In general, the findings of this work match the experience of countries that have already implemented large-scale contact tracing like Singapore, certain provinces of China, or South Korea (33–35). The disease progression in South Korea, however, indicates that contact tracing alone might not be sufficient to fully contain the disease. With respect to quantity, the reduction of the peak under tracing measures is 80% for the 75% individual tracing strategy, which matches with the highest estimate in a summary of 29 COVID-19 studies (10 modelling studies). In this study, the reduction of incident cases under quarantine measures ranges from 44% to 81% (36).
The defined cost function c in equation (1) nicely reflects the tradeoff between reduction of the peak and number of quarantined persons and well suited to quantify the efforts of a specific tracing strategy. To reduce the costs any tracing strategy not only needs to “flatten the curve”, but also keep the number of quarantined persons as low as possible, for example by being accurate in the sense, that not every contact partner of an infected person is equally likely infected as well. Temporary closing of workplaces is clearly the least “precise” of the modelled policies. If put in contrast to the other policies, the high cost and quarantine peak values of the workplace quarantine indicates that, though a large number of persons are put under quarantine, the peak is not reduced appropriately. Consequently, a lot of persons are put under quarantine for no epidemiological reason. Isolating household members is more “accurate” but leaves many infections outside of households untraced. Our model suggests that the better the disease is contained, the higher the percentage of infections within households, and consequently, the more effective (with respect to the cost function) the isolation of household members of infectious persons.
Figure 8 shows a comparison between the height of the peak of the disease and the maximum number of agents in preventive isolation over the course of the modeled period for all tracing strategies. It reveals a highly interesting interplay between the number of isolated persons and the maximum peak height of the disease wave: On the one hand, a lower peak height implies stricter quarantine policies and more persons affected by them. On the other hand, a lower peak height leads to fewer persons requiring isolation. As the latter impact is nonlinear, the negative correlating impact dominates the positive one: if the disease is contained well, strict tracing policies are less costly than loose ones. For example, the number of preventive quarantined persons in the high compliance scenario increased to about 37% of the population with the combined tracing and decreased again to 28% with the 75% individual tracing, even though the latter policy is more restrictive. Compared to the low compliance scenario in which the corresponding numbers were 53% and 51%, an effect in the same direction is visible, but at a lower magnitude.
Clearly, the defined cost function cannot remain the only one that should be considered to evaluate and compare measures. We must consider costs with respect to implementation and control of the policy and, in particular, heavy losses of personal freedom that can hardly be quantified at all. Unfortunately, the model indicates that the least efficient policies are the ones which could be implemented the easiest, and vice versa.
In summary, the model indicates that all tracing measures contribute to reduction of the maximum peak-height. The effect of the policy varies with the compliance to another policy that focuses on reduction of leisure time contacts. As displayed in Table 1, the no-tracing strategy peak with high compliance is very similar to the combined location tracing peak with low compliance. Consequently, according to the definition of the scenarios and strategies in Section Error! Reference source not found., the model indicates that well performed location tracing could substitute the effect of a reduction in the number of leisure time contacts by 75%. Additional individual tracing would substitute for an even higher reduction. If only household or workplace tracing is applied, the benefits vary with the compliance – the higher the compliance, the more effective tracing of households becomes in comparison to workplace tracing.
The previous months (May to September) gave us the opportunity to review and mostly validate the findings of the simulation experiments established end of April. Clearly, in Austria the release of the lockdown measures was not done as fast (May 1st) and as thoughtlessly as defined in our scenarios. Yet, the low infection numbers throughout the summer months despite the absence of harsh containment measures verify the simulation outcome that the combination of strict contact tracing and compliance is sufficient to contain the disease at a low level. Yet, the recent upswing of the numbers due to steadily decreasing compliance among the population furthermore confirm that contact tracing alone is not sufficient for containment.
4.2 Estimate of R0 and General Consequences for Disease Containment
Although not directly related with tracing, the calibration process revealed a modelled basic reproduction number R0 of COVID-19 in Austria of about 4.5, which is considerably high compared to most other estimates in the literature. We assume that this is mainly due to two reasons: First of all, the number originates from the calibration data which is not cleaned with respect to a reporting bias. It is legitimate to assume that the slope of the actual curve at the beginning of the disease-wave is smaller than reported (see report for “nowcasting” attempts by the Robert Koch Institute (RKI, (37)). The second, more important reason for our comparably high R0 is that typical estimates for this number, gained by fitting a Susceptible-Infectious-Recovered (SIR) or an exponential model, are usually lower than analogous R0 estimates based on fitting a Susceptible-Exposed-Infectious-Recovered (SEIR) model – or generally any model that includes a latency/incubation phase (see (38)).
In any case, the modelled R0 indicates that – holding mortality and recovery constant – the infection rate needs to be reduced below 1/ R0 ≈ 22% of its original value in order to reach a fully contained behaviour of the disease, either by reduction of contacts and/or strict distancing and hygiene measures. As a matter of fact, this number is almost impossible to interpret in real life, mainly because there are lots of processes for which infectivity can hardly be reduced properly. The most important of these are definitely contacts within households which hardly be reduced by any measurement or policy.
Our model considers this problem and makes it possible to implement policies much more realistically. Considering that household contacts cannot be the target of any policy, our model indicates that all other contacts would have to be reduced below approximately 12%, instead of 22%, of their original value to achieve full containment. Without tracing and only considering policies for reduction of leisure time contacts, but not school or workplace contacts, this point cannot be reached at all. Consequently, it is not surprising that the chosen compliance scenarios do not lead to a properly contained disease in the model.
4.3 Limitations
With respect to limitations, we must distinguish between limitations of the model as a decision support tool and the limitations of the simulation results of this study.
Interpreted as a decision support tool, the model is primarily limited by comparably long computation times and fundamental simplifications made during the modelling process. The former is caused by the problem, that the model cannot be scaled down and always requires simulation with the full population of the country. Hereby, a huge number of agents (about 9 Million for Austria) leads to long computation time, and the necessity of Monte Carlo simulation for flattening of stochastic results increases the time required to get simulation output even more. Consequently, the simulation’s capabilities of dealing with multivariate calibration problems are limited and the model is not a suitable tool to generate accurate prognoses for a short time horizon. With respect to model reduction during the modelling process, probably the most restrictive limitation of the model is that “death” is not regarded as a final disease state. The model does not distinguish between deceased and recovered agents and regards both as immune agents. This feature could easily be added to the model, we made this simplification as a conscious decision at the beginning of the modelling process as we did not specify forecasting of death counts in our modeling purpose. We might reconsider this in the future and possibly add this feature to become more flexible.
The model results are, as all simulation outcomes, limited by modelling and data uncertainty. Still, many disease parameters of the novel coronavirus are unknown and will surely improve in future due to increasing availability of data. Similarly, the parameters and the modeling assumptions for the tracing strategies are based on expert opinions. Consequently, the tracing algorithm is modeled in an idealized form and cannot validly depict the actual work of professional contact tracers.
4.4 Conclusion
We have presented an agent-based simulation model that is not only capable of simulating epidemics but can also be used to evaluate and compare different containment strategies. Beside classic lockdown interventions like closure of schools or workplaces, the model can also be used to compare different tracing policies, which makes it unique and powerful.
Through this work, we also demonstrate the limits of classical cohort models, as comparable scenarios would not be feasible with such aggregated modelling approaches. By aggregating individual contacts into global contact rates, individual contact chains are lost, and tracing cannot be modelled.
For our policy question on tracing, we investigated six tracing strategies for three compliance scenarios regarding a second outbreak of COVID-19 in Austria. They allowed us to simulate and quantify the impact of different tracing policies and draw conclusions about tracing in general.
The results demonstrate that tracing of potentially infectious contacts and subsequent isolation of affected persons is a very useful measure to slow the spread of COVID-19 and that there are more and less restrictive ways to do so. The model results displayed that a well contained disease also reduces the socioeconomic costs of tracing in terms of fewer quarantined persons per reduction in infections. Consequently, the model results recommend strict tracing strategies and high compliance for hygiene and contact reduction among the population.
The features for evaluating the effectiveness of tracing policies is only one of many features of this advanced ABM. Although the model has limitations, it is a well-founded basis for COVID-19 related decision support as it is capable of including complicated model logic and diverse and high-resolution data. In future, we plan to extend the policy comparisons started in this study by direct comparison with other interventions, such as a more advanced testing regime or the introduction of a vaccine.
Data Availability
All parametrisation data and links to data sources are found in Appendix and References.
Partial results of this work have been presented at
Webinar of the Austrian Association for Public Health: Martin Bicher, „Mathematik als wichtige Public Health Disziplin: Modellbildung und Simulation als Eckpfeiler im Kampf gegen COVID-19“
X-Europe joint data-science webinar: Martin Bicher, “Modelling the spread of SARS-CoV-2: How reliable are simulated forecasts?”
Grant or other financial support
Corona Emergency Call, Österreichische Forschungsförderungsgesellschaft, FFG
Medizinisch-Wissenschaftlicher Fonds des Bürgermeisters der Bundeshauptstadt Wien
Financial support for this study was provided in part by Österreichische Forschungsförderungsgesellschaft, FFG, and Medizinisch-Wissenschaftlicher Fonds des Bürgermeisters der Bundeshauptstadt Wien. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Footnotes
martin.bicher{at}tuwien.ac.at, claire.rippinger{at}dwh.at, christoph.urach{at}dwh.at, domink.brunmeir{at}dwh.at, uwe.siebert{at}umit.at, niki.popper{at}tuwien.ac.at
Revised discussion and representation of the simulation outcomes. Moreover the research question was respecified and the reproducible, full model documentation has been put into the appendix section.
↵1 This number corresponds to the actual state of the confirmed cases on the specified date at the specified time. Due to a reporting bias, this number is subject to constant changes and will probably increase in the future.
References



