
Abstract
Importance With the increasing number of infections for COVID-19, the global health resources are deficient. At present, we don’t have specific medicines or vaccines against novel coronavirus pneumonia (NCP) and our assessment of risk factors for patients with severe pneumonia was limited. In order to maximize the use of limited medical resources, we should distinguish between mild and severe patients as early as possible.
Objective To systematically review the evidence of risk factors for severe corona virus disease 2019 (COVID-19) patients.
Evidence Review We conducted a comprehensive search for primary literature in both Chinese and English electronic bibliographic data bases including China National Knowledge Infrastructure (CNKI), Wanfang, Weipu, Chinese Biomedicine Literature Database (CBM-SinoMed), MEDLINE (via PubMed), EMBASE, Cochrane Central Register, and Web of science. The American agency for health research and quality (AHRQ) tool were used for assessing risk of bias. Mata-analysis was undertaken using STATA version 15.0.
Results 20 articles (N=4062 participants) were eligible for this systematic review and meta-analysis. First in this review and meta-analysis, we found that elderly male patients with a high body mass index, high breathing rate and a combination of underlying diseases (such as hypertension, diabetes, cardiovascular disease, and chronic obstructive pulmonary disease) were more likely to develop into critically ill patients. second, compared with ordinary patients, severe patients had more significant symptom such as fever and dyspnea. Besides, the laboratory test results of severe patients had more abnormal than non-severe patients, such as the elevated levels of white-cell counts, liver enzymes, lactate dehydrogenase, creatine kinase, c-reactive protein and procalcitonin, etc, while the decreased levels of lymphocytes and albumin, etc.
Interpretation This is the first systematic review investigating the risk factors for severe corona virus disease 2019 (COVID-19) patients. The findings are presented and discussed by different clinical characteristics. Therefore, our review may provide guidance for clinical decision-making and optimizes resource allocation.
Question What are the risk factors for severe patients with corona virus disease 2019 (COVID-19)?
Findings First in this review and meta-analysis, we found that elderly male patients with a high body mass index, high breathing rate and a combination of underlying diseases were more likely to develop into critically ill patients. second, compared with ordinary patients, severe patients had more significant symptom such as fever and dyspnea. Last, we also found that the laboratory test results of severe patients had more abnormal than non-severe patients.
Meaning This review summaried the risk factors of severe COVID-19 patients and aim to provide a basis for early identification of severe patients by clinicians.
Introduction
In December 2019, COVID-19 was discovered in Wuhan, Hubei Province, China[1]. On January 7, 2020, the causative agent was identified as a 2019 novel coronavirus (2019-nCoV)[2-4]. According to the WHO report[5], as of 10:00 on March 23, 2020, a total of 334,695 confirmed cases and 14,526 deaths were reported in 140 countries and regions worldwide. While the epidemic in China is gradually under control, Europe and the Middle East have shown the signs of rapid spread. For example, Italy, Iran, Germany, Spain, the United States, South Korea and Japan have seen a sharp increase in the number of infections[5].
Nowadays, with the increasing number of infections, the global health resources are extremely poor. In order to maximize the use of limited medical resources, we should distinguish between mild and severe patients as early as possible. At present, we don’t have specific medicines or vaccines against novel coronavirus pneumonia (NCP) and our assessment of risk factors for patients with severe pneumonia was limited. In this regard, we have summarized the published studies with critically ill patients aimed at explaining the risk factors of the NCP and providing Chinese experience for people around the world in responding to COVID-19.
Methods
This meta-analysis was performed in accordance with PRISMA-2009 (Preferred Reporting Items for Systematic Reviews and Meta-analyses)[6] and MOOSE (Meta-analysis of Observational Studies in Epidemiology) guidelines[7].
Search strategy
Relevant studies were searched from both Chinese and English electronic bibliographic databases including China National Knowledge Infrastructure (CNKI), Wanfang, Weipu, Chinese Biomedicine Literature Database (CBM-SinoMed), MEDLINE (via PubMed), EMBASE, Cochrane Central Register and Web of science from inception to 8 March 2020. The MeSH terms of COVID-19 and corresponding synonyms were included into the searching strategy. Limiting our search to human-subjects but without language limitation. Reference lists of retrieved articles were also reviewed to further identify potentially relevant studies. The searching procedures were independently performed by two reviewers (Lizhen Xu and Yaqian Mao) and disagreements were settled by discussion.
Inclusion criteria
The inclusion criteria were as follows: (i) prospective or retrospective original literature; (ii) all patients were clearly diagnosed with COVID-19; (iii) characteristics of severe and non-severe patients were documented; and (iv) complete medical records were available for data extraction.
Definition of severe COVID-19[8]: Severe COVID-19 was designated when the patients had one of the following criteria:1) Respiratory distress with respiratory frequency≥30/min; 2) Pulse Oximeter Oxygen Saturation≤93% at rest; 3) Oxygenation index (artery partial pressure of oxygen/inspired oxygen fraction, PaO2/FiO2)≤300 mmHg (1 mmHg=0.133 kPa). At high altitudes (above 1000 meters), PaO2 / FiO2 should be corrected according to the following criteria: PaO2 / FiO2 [Atmospheric Pressure (mmHg) / 760]. Pulmonary imaging showed that the lesions progressed more than 50% within 24-48 hours should be managed according to Critically ill patients.
Quality assessment
The observational study quality evaluation criteria recommended by the American agency for health research and quality (AHRQ) were used to evaluate the study quality. These criteria included 11 items, including subjects selection, research quality control and data processing. Each question will be answered with “yes,” “no” or “unclear.”
Data extraction
The following characteristics were extracted from selected studies: authors, sample size, region, study period. In addition, the following possible risk factors were recorded independently: patient characteristics, comorbidities, vital signs, symptoms, laboratory findings. Data extraction was accomplished independently by two reviewers (Lizhen Xu and Yaqian Mao). Any disagreement was resolved by joint discussion to reach a consensual conclusion. There were a few points that need to be explained. First, in order to minimize the risk of duplication of data, when two or more studies presented possible overlap, where sampling periods overlapped and patients were from the same region, the one with largest populations was included. Second, continuous variables were expressed as medians and interquartile ranges or simple ranges in some studies, the standard deviation and mean value were not estimated due to inaccurate.
Data synthesis and statistical analysis
For categorical variables, analysis was performed by calculating the odds ratio (OR) with 95% confidence interval (95% CI). For continuous outcomes, Weighted Mean Difference (WMD) and standardized mean difference (SMD) with the corresponding 95% CI were calculated. The heterogeneity was assessed by using the I2 test, with I2>50 % indicating the existence of heterogeneity. If there is significant heterogeneity, a random effect model (DerSimonian-Laird method) was used to calculate the pooled effect; otherwise, the fixed model (Mantel-Haenszel method) was used. Possible publication bias was evaluated via observing the symmetry characteristics of funnel-plots. If the number of included studies in each outcome was <10, the funnel plot was not performed due to limited power[9]. Data analysis was undertaken using STATA, version 15.0 (Stata Corp).
Results
Literature search results
The entire process of literature searching and screening was displayed in Figure 1. Initially, 6354 publications were identified through database searching. After the removal of 2622 duplicates, there remained a record of 3732 studies. We excluded 3654 records by reviewing their titles and abstracts. As a result, only 78 articles were subject to a full-text review. Finally, 20 articles met the inclusion criteria were included in the synthesis.

Study characteristics
The main characteristics of the studies were summarized in Table 1. All articles were observational studies. All the subjects are from China, including more than 30 provinces and cities. The study period spans from 11 December 2019 to 23 February 2020. About the comparison of mild and severe patients, 15 studies[1, 10-23] described patient characteristics, 15 studies described comorbidities[1, 10-17, 20-25], 8 studies[1, 10, 14, 17, 19, 20, 22, 23] described vital signs, 17 studies compared symptoms[1, 10-12, 14-26] and 19 studies[1, 10-27] described laboratory findings. Guan, etc’study included 1099 patients from 552 hospitals in 30 provinces, and described the clinical characteristics of mild and severe patients in detail. Because of this article may be overlaps in population data with other studies, and the results are mainly described using median and quartile intervals, so we did not include the data in our meta-analysis, and mainly used descriptive analysis to compare the results with our studies.
Quality assessment
The quality of included studies was assessed by the observational study quality evaluation criteria recommended by AHRQ. All studies included clear data sources, inclusion and exclusion criteria, and reasonable control of confounding factors. However, only a few studies clearly reported the quality control of the study and the treatment of missing data (See Appendix table 1).
Meta-analysis
The results of the meta-analysis are shown in Table 2. More intuitive results can be found in the forest-plot (Figure 2, Figure 3).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient characteristics (Age, Gender, BMI and Smoking)
A random-effects model (I2=54.4%) was used on 6 articles[10, 12, 13, 17, 22, 23] involving 681 patients to analyze the risk factors of age for severe patients with COVID-19. Compared with non-severe patients, the average age of severe patients was older (WMD=11.89 [8.63, 15.14]) than mild patients. Results about gender on ten studies[10, 12, 13, 15-17, 19, 21-23] included 1494 patients suggesting that men were more likely to have severe pneumonia than women (OR=1.61 [1.25, 2.07]). Only have two studies[18, 23] on BMI included 79 patients showed that the BMI value of severe patients was higher than non-severe patients (WMD = 3.38 [0.07, 6.69]). A fixed-effects model was used on 3 articles[10, 15, 23] involving 412 patients to analyze the risk factors of smoking showed that there was no significant correlation between smoking and the severe pneumonia (OR = 1.4 [0.65, 3.01]).
Comorbidities (Diabetes, Hypertension, Coronary heart disease, Chronic obstructive pulmonary disease)
Our research show that patients with the following underlying diseases are more likely to develop severe COVID-19: Diabetes mellitus (DM):OR = 3.04 [2.01, 4.60], Hypertension (HTN):OR = 2.31 [1.68, 3.18], Coronary heart disease (CHD):OR = 2.76 [1.39, 5.45], Chronic obstructive pulmonary disease (COPD):OR = 3.56 [1.33, 9.54]. All results were low heterogeneous (I2<50%).
Vital Signs (respiratory rate) and Symptoms (Fever and Dyspnea)
Regarding breathing, our study in 2 article[14, 23] (included 70 patients) showing that patients with severe COVID-19 breathed faster (WMD = 5.29 [2.56, 8.01], I2 = 42.8%). Our study on fever (11 articles[10, 12, 14-17, 19, 22, 23, 25, 26]) and dyspnea (8 articles[10, 12, 14, 15, 17, 19, 22, 25]) founded that fever and dyspnea may be the risk factors for severe patients (Fever: OR = 2.11 [1.11, 4.02]; Dyspnea: OR = 8.83 [2.82,27.67]).
Laboratory Findings (Blood routine, Biochemical indicators, Inflammatory biomarkers and Coagulation)
Our study in laboratory findings showed that white-cell count (WMD=1.76 [0.31, 3.22]) increased in severe patients, while the proportion of lymphocytes decreased (WMD=-0.42 [-0.52, -0.33]). Compared with non-severe patients, severe patients have higher alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total bilirubin (Tbil) (ALT: WMD = 16.97 [2.18, 31.76]), AST: WMD = 20.60 [6.81, 34.40], Tbil: WMD = 3.93 [2.01, 5.86]), but creatinine (Cr), albumin (ALB) and neutrophil count (N count) does not seem obvious difference (Cr: WMD = 8.32 [-1.63, 18.28], ALB:WMD = -5.74 [-7.94, -3.54], N count, WMD=2.92 [-1.33, 7.17]). Regarding of C-reactive protein (CRP) and Procalcitonin (PCT), severe patients were higher than non-severe patients (CRP: SMD = 2.11 [0.71, 3.51], PCT: WMD = 0.16 [0.04, 0.28]). What’more, our study found that compared with non-severe patients, lactate dehydrogenase (LDH), creatine kinase (CK) and D-dimer (D-D) increased more significantly in severe patients (LDH: SMD = 2.0 [1.20, 2.80], CK: WMD = 23.55 [17.08, 30.02], D-D: WMD = 0.67 [0.02, 1.32]).
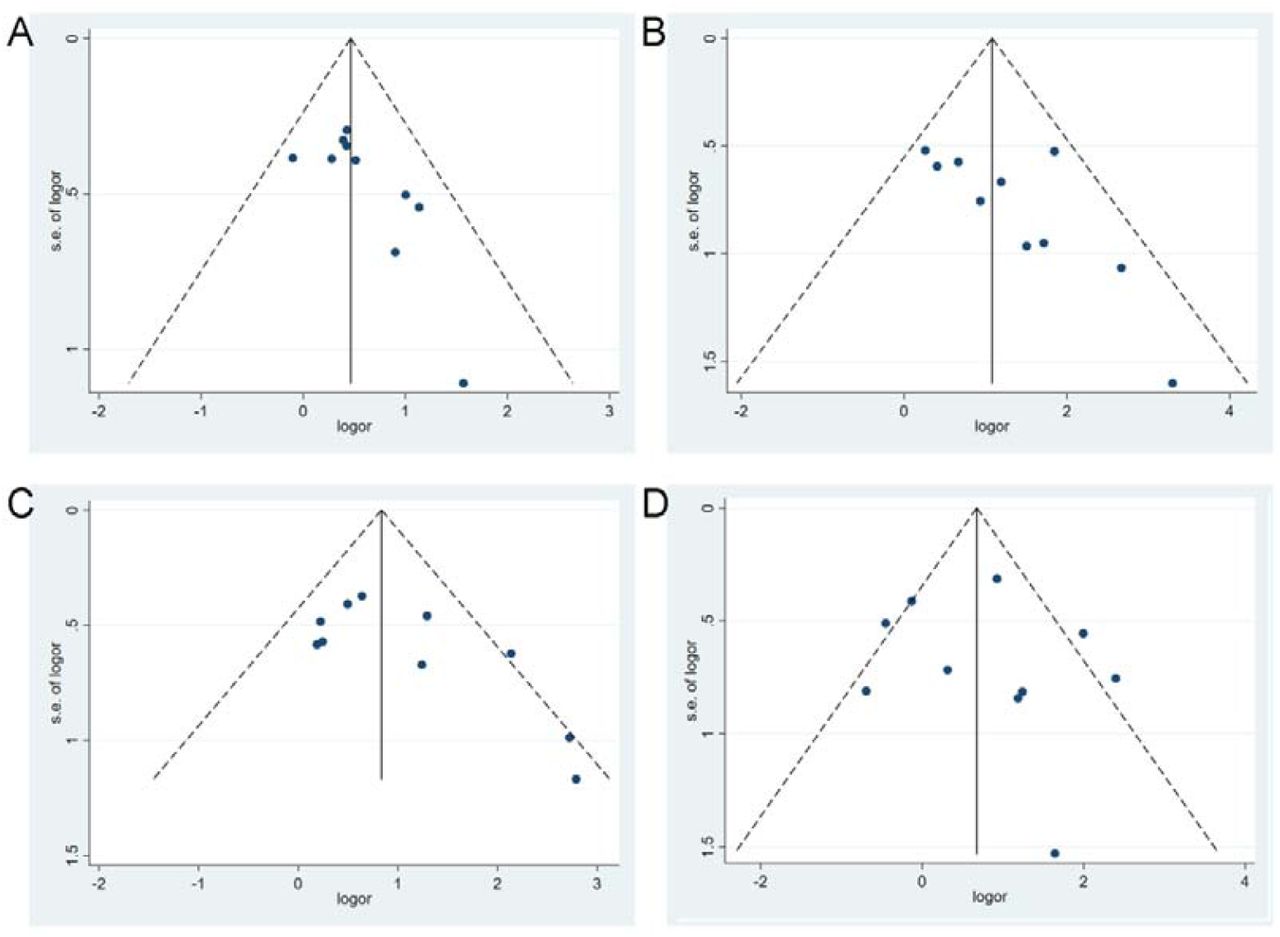
Publication bias
We only draw a funnel-plots for the outcome indicators with more than 10 studies, and judge the publication bias of the results by observing the symmetry of the funnel-plots. As shown, our funnel-plots is roughly symmetrical, indicating that publication bias is small. In addition, our research not only includes published studies, but for unpublished literature on medRxiv and bioxiv, as long as it meets our inclusion criteria, we also include them, aim to minimize publication bias.
Discussion
This study shows the conclusive evidence as risk factors for severe COVID-19 patients, such as patient characteristics (age, gender, BMI), comorbidities (DM, HTN, CHD, COPD), vital signs (respiratory rate), symptoms (fever and dyspnea) and laboratory findings (blood routine, biochemical indicators, inflammatory biomarkers and coagulation).
At present, no special drug for SARS-CoV-2 infection has been found and the research process of the vaccine is still in clinical trials, the treatment of COVID-19 is mainly by Symptomatic treatment. Based on Chinese experience, mild patients and their close contacts treated in close isolation and follow-up are likely to be sufficient to manage the disease[29-31]. But for severe patients, intensive care and aggressive treatments are needed. By searching various databases, we found that this is the first article of systematic review and meta-analysis to summarize the characteristics of severely infected patients with SARS-CoV-2.
The article[1] of Guan, etc shows that the Median (IQR) age of critically ill patients was 52.0 (40.0–65.0) which was older than the non-critically ill patients whose median (IQR) age was 45.0 (34.0–57.0). Similarly in our review, we found that patients with critically ill were older than those with non-critically ill patients, and most patients are male. Moreover, the presence of coexisting illness (such as DM, HTN, CHD, COPD) was more common among patients with severe disease than among those with nonsevere disease. We all know that the elderly with basic diseases, especially those with diabetes usually have a high blood glucose status for a long time, so their ability to defend against infection is low[32]. They are at high risk for various infections, and once infected, they can easily develop into severe diseases. The lower sensitivity of women to viral infections may be due to the protection from X chromosomes and sex hormones, which play an important role in innate and adaptive immunity[33]. So, we think that elderly male patients with underlying diseases are at high risk for severely ill with COVID-19 and needs special attention from clinicians. In addition, our study also found that patients with high BMI are more likely to develop into severe pneumonia, which may be related to the high expression of angiotensin-converting enzyme 2 (ACE2) in obese patients[34]. We know that ACE2 is a binding receptor for SARS-CoV-2 and has a very high affinity between them. Obese patients are richer in adipose tissue, have a larger total amount of ACE2 receptors[34], and are more susceptible to SARS-CoV-2. It is suggested that obese people are at high risk of COVID-19, and they are the key protection targets in epidemic prevention work.
The symptoms of COVID-19 include fever, cough, sputum production, sore throat, fatigue or myalgia, dyspnea, nausea or vomiting, diarrhea, chills and headache, etc. In most studies, the symptom of fever and dyspnea occur more frequently in critically ill patients[1, 11, 12], which is consistent with our study. regarding of vital signs, we found that critically ill patients usually breathed more faster than non-critically ill patients, which related to the low level of blood oxygen saturation caused by severe lung disease in critically ill patients. A study[23] from 49 people found no significant difference in pulse rate between severe patients and non-severe patients (90.6 ± 10.3 vs. 93.8 ± 13.7, p = 0.440), which is consistent with the findings of fang, et al[22]. At the same time, the fang’s study[22] also found that the blood pressure of severe patients seems to be higher than that of non-severe patients [SBP: 133.3 ± 16.5 vs. 121.2 ± 9.5, p <0.001; DBP: 83.3 ± 11.7 vs. 74.2 ± 9.5, p <0.001]. while the study by Xiang, et al[23] found no significant difference in systolic blood pressure (p = 0.769), but lower diastolic blood pressure (69.1 ± 10.8 vs. 80.7 ± 12.7, p = 0.013) compared with non-severe patients.
As for laboratory tests, patients with severe disease had more prominent laboratory abnormalities (including lymphocytopenia, hypoalbuminemia, elevated levels of ALT, AST, Tbil, LDH, CK, etc) than those with nonsevere disease. Many previous studies have reported lymphocytopenia in patients with COVID-19[35], lymphocytopenia is a significant feature of severe patients with SARS-CoV-2 infection because targeted invasion by SARS-CoV viral particles can damages thecytoplasmic component of the lymphocyte and cause its necrosis or apoptosis[36]. In this meta-analysis, we found that SARS-CoV-2 can damage the various organs throughout the body in addition to the lung, manifested as the elevated levels of ALT, AST, Tbil, LDH, CK, etc in different degree. As we know, coronavirus (CoV) is a pathogen that infects the respiratory, gastrointestinal, liver, and central nervous systems of humans and many other wild animals[37, 38]. SARS-CoV-2, also known as the sister virus of SARS-CoV, has 85% nucleotide homology[39, 40]. The latest pathology reports[41] found that the pathological manifestations of SARS-CoV-2 and SARS-CoV are similar, mainly manifesting as acute respiratory distress syndrome (ARDS) and multiple organ failure, which also explains the cause of multiple organ dysfunction in critically ill patients. SARS-CoV-2 has been shown to infect human respiratory epithelial cells through the angiotensin-converting enzyme 2 receptors on human cells[42, 43]. Many studies[34, 44] have found that the levels of ACE2 RNA was higher in heart, kidney, intestinal tract, gallbladder, adipose tissue and testicles than lungs in human body, which also explains the reason why multi-organ dysfunction is prone to occur in severe patients.
Inflammatory biomarker is also a common feature in the patients with COVID-19 and might be a critical factor associated with disease severity and mortality. In the study, we found that CRP and PCT increased in varying degrees for severe patients. Some research also reported the elevated level of ESR, IL-6, and IL-10 in critically ill patients[24]. It is considered that multiple cytokines are secreted after the infection of microorganisms causing a strong inflammatory response and the damage of immune system, indicated that critically ill patients may have more severe systemic inflammatory response, so attention should be paid to strengthen the treatment of anti-inflammatory[23].
Limitations
However, there are still some limitations lying in our study. First, all included studies were cross-sectional, precluding the possibility to establish inferences regarding causality. Second, populations, risk factors analyzed, lengths of follow-up, and statistical methods might differ and cause study heterogeneity. Third, although this study reviewed the risk factors of severe COVID-19 patients and their impact, assessing the effect size of each risk factor and developing risk models were important.
Conclusion
The severity of SARS-CoV-2 pneumonia has placed great pressure on intensive care resources in hospital, especially in some developing countries where lacking of medical staff and health resources, so early identification of severe patients and taking active and effective measures can reduce deaths.
Data Availability
all data included in this study are available upon request by contact with the corresponding author.
Article Information
Author Contributions
Gang Chen had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Lizhen Xu and Yaqian Mao contributed to the study equally.
Concept and design: Lizhen Xu, Yaqian Mao, Gang Chen.
Acquisition, analysis, or interpretation of data: Lizhen Xu, Yaqian Mao
Drafting of the manuscript: Lizhen Xu, Yaqian Mao
Critical revision of the manuscript for important intellectual content: Lizhen Xu, Yaqian Mao, Gang Chen
Statistical analysis: Lizhen Xu
Administrative, technical, or material support: None
Supervision: Gang Chen
Conflict of Interest Disclosures
The authors declare that they have no conflicts of interest for this work.
Funding/Support
None
Acknowledgments
We thank all patients and their families involved in the study. Authors are also thankful to the Department of Endocrinology, Shengli Clinical Medical College of Fujian Medical University.
Appendix
References



