
Abstract
The COVID-19 pandemic has shown a markedly low proportion of cases among children. Age disparities in observed cases could be explained by children having lower susceptibility to infection, lower propensity to show clinical symptoms, or both. We evaluate these possibilities by fitting an age-structured mathematical model to epidemic data from six countries. We estimate that clinical symptoms occur in 25% (95% CrI: 19-32%) of infections in 10-19-year-olds, rising to 76% (68-82%) in over-70s, and that susceptibility to infection in under-20s is approximately half that of older adults. Accordingly, we find that interventions aimed at children may have a relatively small impact on total cases, particularly if the transmissibility of subclinical infections is low. The age-specific clinical fraction and susceptibility we have estimated has implications for the expected global burden of COVID-19 because of demographic differences across settings: in younger populations, the expected clinical attack rate would be lower, although it is likely that comorbidities in low-income countries will affect disease severity. Without effective control measures, regions with older populations may see disproportionally more clinical cases, particularly in the later stages of the pandemic.
Posterior estimates for the consensus susceptibility and clinical fraction from 6 countries. Note that susceptibility is a relative measure.
Model parameters.

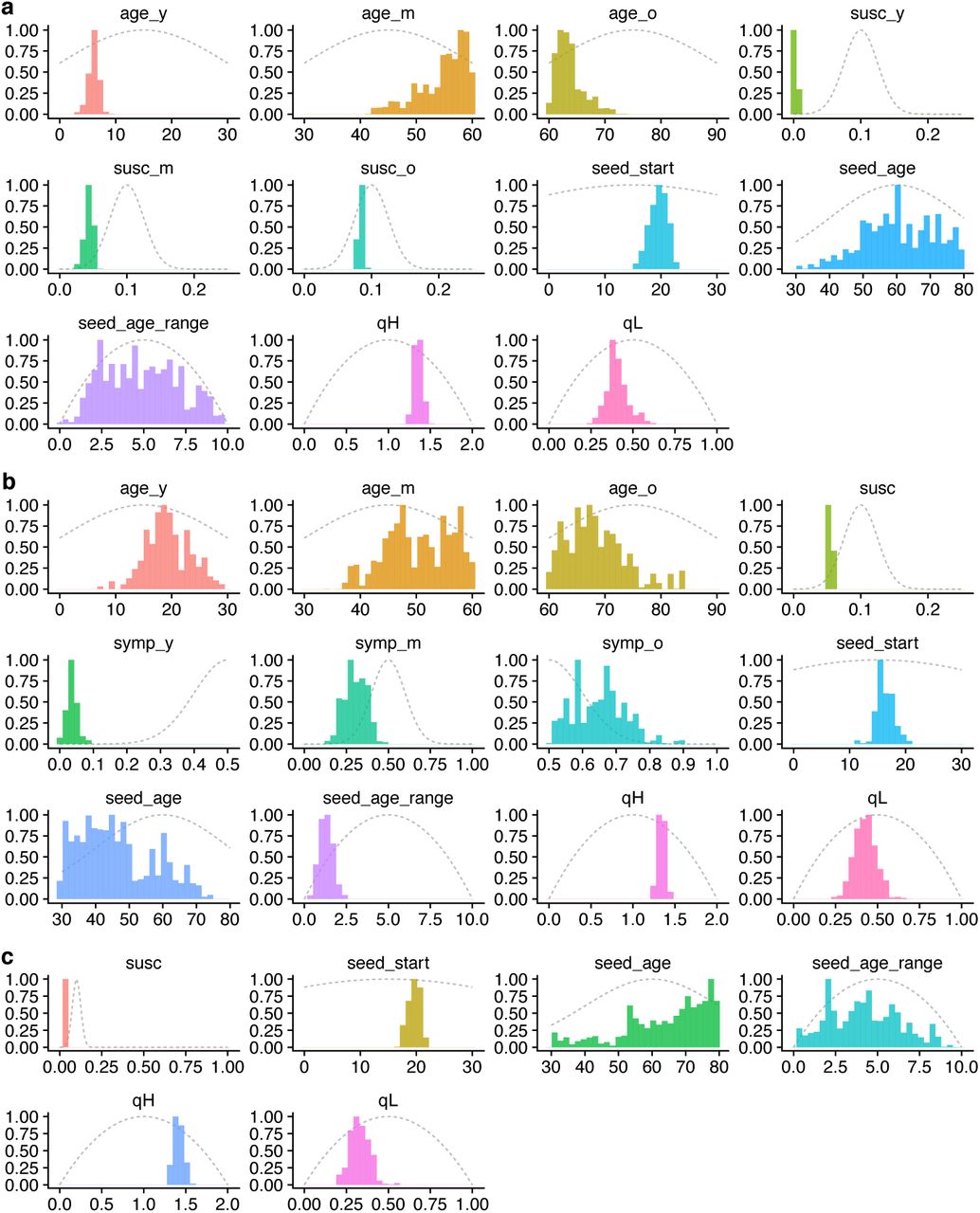
Prior distributions (grey dotted lines) and posterior distributions (coloured histograms) for model parameters fitting to the early epidemic in Wuhan (Fig. 1, main text); seed_start is measured in days after November 1st, 2019. (a) Model 1 (age-varying contact patterns and susceptibility); (b) Model 2 (age-varying contact patterns and clinical fraction); (c) Model 3 (age-varying contact patterns only). See also Supplementary Table 3.

Analysis showing how the inferred age-varying susceptibility (first column) and age-varying clinical fraction (second column) depend upon the additional data sources used.

Prior and posterior distributions for the epidemics in (a) Beijing and Shanghai, (b) South Korea and (c) Lombardy using the “consensus” fit for age-specific clinical fraction and assuming subclinical infections are 50% as infectious as clinical infections (see Fig. 2c, main text). For (a), times are in days after December 1st, 2019; for (b) and (c), times are in days after January 1st, 2019. Note, seed_d is the inferred duration of the seeding event. See also Supplementary Table 3.

Global projections assuming greater severity in lower-income countries. (a) Schematic age-specific clinical fraction for higher-income and lower-income countries. (b-f) Illustrative results of the projections for 146 capital cities assuming a higher age-varying clinical fraction in lower-income countries. See Fig. 4 (main text) for details.

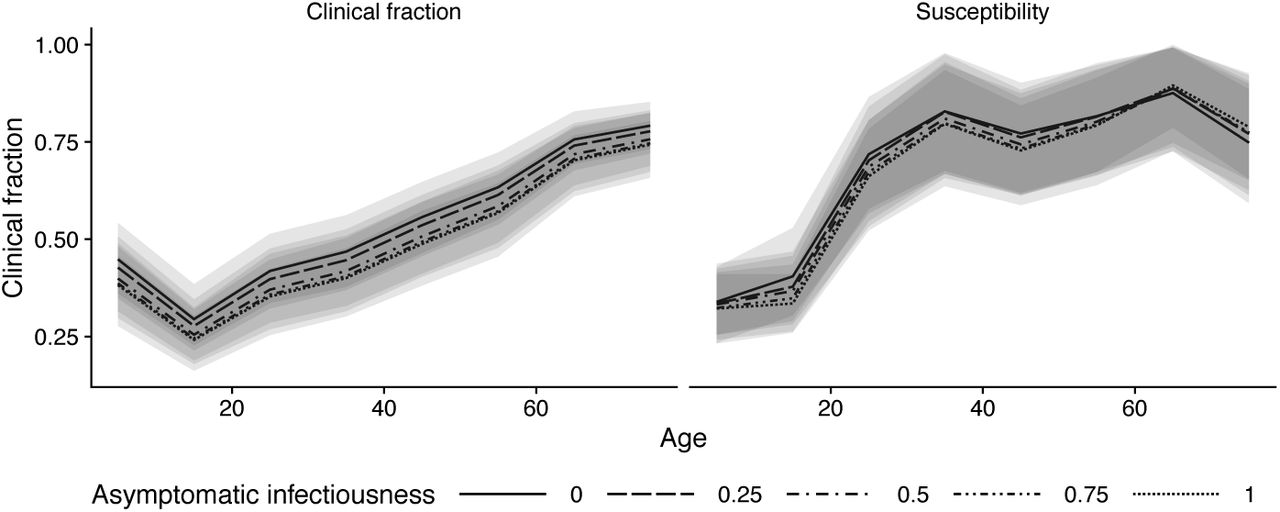
Consensus age-specific clinical fraction and susceptibility, assuming subclinical infections are 0%, 25%, 50%, 75%, or 100% as infectious as clinical infections.

(a) Projected total and peak clinical case attack rate for 146 capital cities, under different assumptions for the infectiousness of subclinical infections. (b) Projected total and peak subclinical infection attack rate for 146 capital cities, under different assumptions for the infectiousness of subclinical infections. (c) Projected differences in R0 among 146 capital cities, under different assumptions for the infectiousness of subclinical infections.

Comparison of school closures in three exemplar cities when susceptibility ui is fixed across settings instead of R0.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Footnotes
1 Carl A B Pearson, Billy J Quilty, Adam J Kucharski, Hamish Gibbs, Samuel Clifford, Amy Gimma, Kevin van Zandvoort, James D Munday, Charlie Diamond, W John Edmunds, Rein MGJ Houben, Joel Hellewell, Timothy W Russell, Sam Abbott, Sebastian Funk, Nikos I Bosse, Fiona Sun, Stefan Flasche, Alicia Rosello & Christopher I Jarvis. Order of working group determined at random.




Subject Area
Reviews and Context
1
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos