
Abstract
Background Poor adolescent mental health is a growing concern over recent decades with evidence of increasing internalising mental health problems corresponding with decrease in anti-social, smoking and alcohol behaviours. However, understanding whether and how the associations between mental health and health-related behaviours such as substance use, anti-social behaviour and obesity have changed over time is less well-understood.
Objectives We investigate whether the associations between different health-related outcomes in adolescence are stable or changing over time in two recent cohorts of adolescents born ten years apart.
Method Data from two UK birth cohort studies, the Avon Longitudinal Study of Parents and Children (ALSPAC, born 1991-92, N=5627, 50.7% female) and Millennium Cohort Study (MCS, born 2000-1, N=11318, 50.6% female) at age 14 sweeps are used. The health outcomes of focus are depressive symptom score, substance use (alcohol, smoking, cannabis and other drugs), antisocial behaviours (assault, graffiti, vandalism, shoplifting and rowdy behaviour), weight (BMI), weight perception (perceive self as overweight) and sexual activity (had sexual intercourse).
Results Our results suggest although directions of associations between mental-health and health-related behaviours (eg smoking) are similar over time, their strength across the distribution has changed. While smoking and alcohol use behaviours are decreasing in adolescents, those that endorse these behaviours in 2015 are more likely to have co-occurring mental-health and other problems than those born in 2005. Similarly, higher body mass index is more strongly associated with depressive symptoms in 2015.
Conclusions Our findings suggest that associations between these factors has changed over time, which has implications for public health and our understanding of the mechanisms underlying their observed associations in the population.
Introduction
There is substantial evidence from population based surveys and diagnostic prevalence studies that the rates of common internalising mental health difficulties such as depression and anxiety has been rising over the last few decades.1,2 Similarly, there is clear evidence that the age at first smoking and drinking and prevalence of underage substance use is steadily decreasing,3 and evidence for antisocial behaviour is less consistent but suggest decreasing trends in recent decades.4-6 Alongside these changes in prevalence, there is a large body of epidemiological evidence showing links between these outcomes, for example between substance use and depression, 7-9 where evidence across many substances including alcohol, tobacco and cannabis consistently shows a positive association with increased rates of depression or depressive symptoms. Similarly, antisocial behaviour and substance use are known to be associated positively,10 and antisocial behaviour and depressive symptoms are also more likely to co-occur in adolescence.11
In our recent paper comparing prevalences of mental health and health-related behaviours in two cohorts of adolescents aged 14 in 2005 and 2015,4 we found an almost two fold increase in the prevalence of high depressive symptoms and marked reductions in antisocial behaviours and lower cigarette, alcohol and drug use in 2015 compared to 2005.4 We also observed an increase in BMI and obesity, and differences in other health related behaviours such as sleep, weight perception and sexual behaviour.4 There are a number of possible explanations for these differing changes in trends that see some outcomes increasing and others decreasing over this decade. First, these findings might indicate that the associations between these factors are dynamic, and have changed between the cohorts. Second, it could indicate that the associations are not causal, and that other confounding factors are responsible for any associations seen, and it is these confounding factors that have changed. Third, the associations between these factors are stable over time, but changes in other explanatory factors might account for the changing trends observed.
This paper will investigate whether the predictors of mental health, antisocial behaviour and substance use in UK adolescents have changed between 2005 and 2015, using two large birth cohorts; the Avon Longitudinal Study of Parents and Children (ALSPAC, born 1991-92) and Millennium Cohort Study (MCS, born 2000-02).
Methods
Participants
Avon Longitudinal Study of Parents and Children (ALSPAC) is a cohort born in 1991-92. ALSPAC recruited 14,541 pregnant women resident in Avon, UK with expected dates of delivery 1st April 1991 to 31st December 1992. When the oldest children were approximately 7 years of age, an attempt was made to bolster the initial sample with eligible cases who had failed to join the study originally. The total sample size for analyses using any data collected after the age of seven is therefore 15,454 pregnancies, resulting in 15,589 foetuses. Of these, 14,901 were alive at 1 year of age. 12,13 The study website contains details of all the data that is available through a fully searchable data dictionary and variable search tool (http://www.bristol.ac.uk/alspac/researchers/our-data/). Ethics approval for the study was obtained from the ALSPAC Ethics and Law Committee and the Local Research Ethics Committees. Data were collected frequently via different modalities, with clinic visits and postal questionnaires having taken place in adolescence every year. This study uses data from ages 13, 14 and 15. In the current study, data were available from 6132 participants at age 14 representing 41.7% of the 14701 participants alive past 1 year. Attrition is predicted by a range of variables in ALSPAC including lower educational level, male gender, non-White ethnicity, and eligibility for free school meals.
Millennium Cohort Study (MCS) is a cohort of 19,517 children born in 2000-02 sampled from the whole of the UK.14 Data so far have been collected in 6 sweeps at ages 9 months, 3, 5, 7, 11 and 14 years. The study website (https://cls.ucl.ac.uk/cls-studies/millennium-cohort-study/) contains details regarding all the data available and information on accessing the datasets. Ethics approval for the age 14 sweep was obtained from the National Research Ethics Service Research Ethics Committee. At the age 14 sweep, 15415 families were issued into the field (those not issued due to emigration, permanent refusal, untraceability), of which 11726 families participated in the age 14 sweep (representing 60.9% of the original sample).15 Attrition at the age 14 sweep compared to the full sample is predicted by a range of demographic variables including male gender, Black ethnicity, lower occupational and educational level and single parent family.16
For this study, we analysed data from participants who had provided data on at least one of these outcome variables at the age 14 sweeps of the studies (depressive symptoms, smoking, alcohol, cannabis and other drugs; ALSPAC n= 6132, MCS n= 11351). Furthermore, participants without the demographic data required for increasing the comparability of the datasets (sex, ethnicity, age, maternal education and maternal age) were excluded, resulting in an analysis sample of 5627 from ALSPAC and 11318 from MCS.
There have been changes in socio-demographic characteristics of the country in the ten years between these cohorts (e.g. higher proportion ethnic minorities, higher education levels). To account for confounding due to socio-demographic differences between cohorts, we control for socio-demographic factors (sex, age, ethnicity, maternal age and parent education) in analysis.
Measures
The measures in this study were harmonised as part of a previous study,4 where we tried to harmonise a range of mental health, health related behaviour data.
The harmonised measures used in this study include socio-demographic controls, mental ill-health (depressive symptoms), substance use (alcohol, smoking, cannabis and other drugs), antisocial behaviours (assault, graffiti, vandalism, shoplifting and rowdy behaviour), weight (BMI), weight perception (perceive self as overweight) and sexual activity (had sexual intercourse).
Measures that were not perfectly harmonised in our previous prevalence study (e.g. self-harm, question relates to lifetime self-harm in ALSPAC and last 12 months in MCS), or did not derive concurrently from the same data sweep (e.g. sleep) are excluded from this study, in a deviation to this study pre-registration,17 as the differences in assessment do not make cross-cohort comparisons of associations possible.
Depressive symptoms
Depressive symptoms were assessed using the Short Moods and Feelings Questionnaire,18 with a cutoff score of 12 or above indicating high depressive symptoms.18
Antisocial behaviour
Five harmonised measures of assault, rowdy behaviour, graffiti, vandalism and shoplifting were included in both cohorts, and combined to create an index of anti-social behaviours (higher score indicating engaging in higher number of antisocial behaviours).
Substance use
Harmonised measures of ever trying the following substances: tobacco, alcohol, cannabis or other drugs are analysed separately, but also combined to create an index score of substance use with a range of 0 (tried no substances) to 4 (used all substances). We also investigate the extent of use with tobacco (weekly smoking) and alcohol (heavy drinking).
Health-related behaviours
We include the harmonised variables of BMI, weight perception (perceiving oneself as overweight) and underage age sexual activity.
Analysis
We first present descriptive statistics and correlations between the variables of interest in both cohorts. We examine rates of poor health behaviours/ antisocial behaviours as binary outcomes and as indices (the latter providing data on cumulative substance use/anti-social behaviours). In ALSPAC 10.4% and in MCS 1.22% of cells were missing. Multiple imputations (20 imputations) were carried out using chained equations separately in the two cohorts before combining the datasets for joint analysis. As a preliminary step in our investigation, we estimate odds of health outcomes for those with and without high depressive symptoms in each cohort.
We estimated four sets of regression models, each with depressive symptoms, substance use index score and antisocial behaviour index score as outcomes. In the first regression, we estimated the cohort interaction for each predictor separately, thus estimating the unadjusted association between each predictor and outcome and whether this is moderated by cohort. In the second regression we included a set of socio-demographic confounders, thus adjusting the association moderated by cohort accounting for these potential confounders. In the third step, we examined whether there are any non-linear associations between predictor and outcomes using a quadratic term for continuous predictors. Where non-linear associations were observed, the final model includes the non-linear term. In the fourth and final model, we mutually adjusted for all predictors (including the other outcomes) in the same model, examining whether the predictor-outcome association and the moderation by cohort are independent of the other predictors.
In our previous study, to estimate comparable prevalences entropy balancing weights were used to re-weight MCS estimates to match the ALSPAC socio-demographic distribution,4 indicating small adjustments to the nationally representative prevalence estimates in MCS when applying these weights. In these analyses, we control for these socio-demographic characteristics in our models to ensure differences in associations are not confounded by differences in socio-demographic characteristics and use MCS sampling weights in all analyses.
Lastly, to examine if there are any sex differences in the associations between these factors in the two cohorts we estimated three way (sex*cohort*predictor) interactions for each of our regression outcomes.
Results
As detailed in our previous paper,4 we report prevalences of our main variables of interest in this investigation in Table 1. We report pairwise correlations between all variables of interest within the two cohorts in Supplementary Table 1.
Descriptive statistics for mental health, antisocial behaviours, substance use and other health related behaviour outcomes in 2005 (ALSPAC) and 2015 (MCS)
Depressive symptoms as outcome
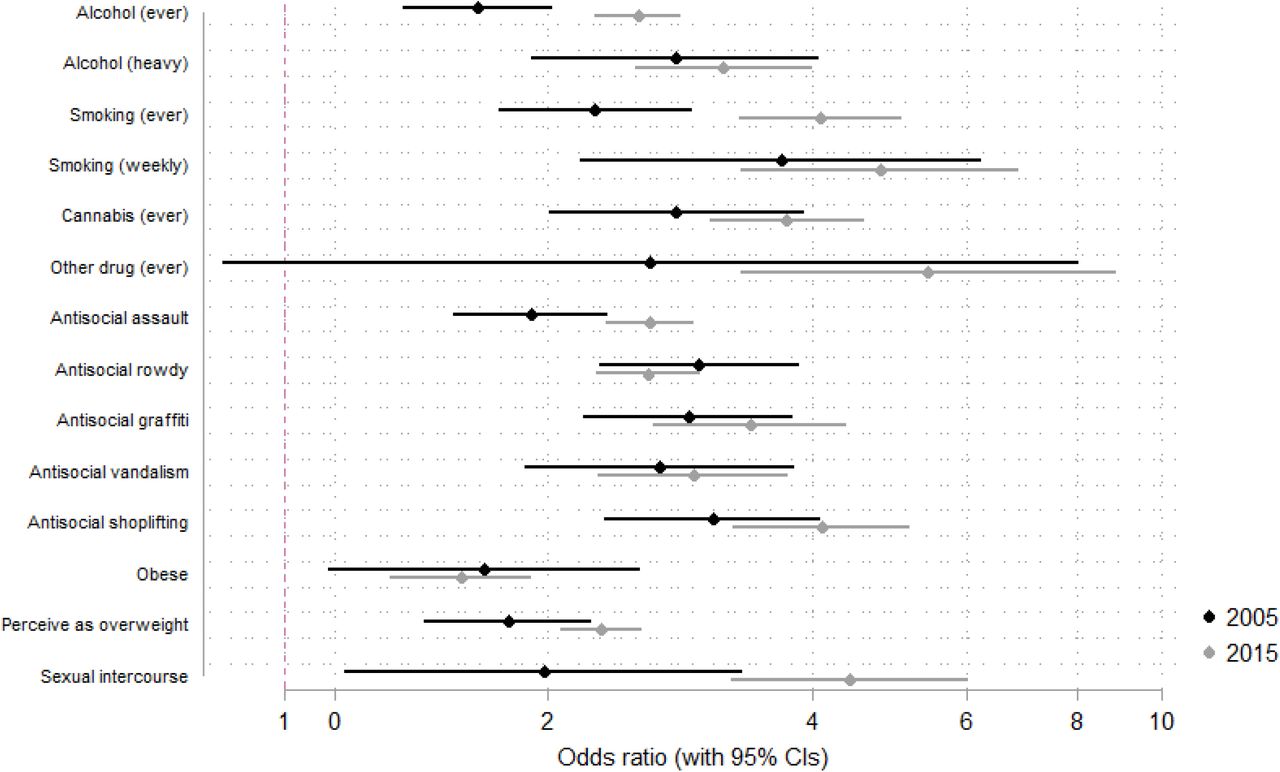
When investigating the association between rates of each different health and antisocial behaviours as predictors of depressive symptoms in both cohorts, we found that in all cases, across both cohorts, higher rates of these behaviours predicted likelihood of higher depressive symptoms scores, although the association between the use of an illicit drug other than cannabis and depressive symptoms was weak in 2005, with confidence intervals crossing the null. Results were broadly consistent between the two cohorts (see Figure 1) although having had sex, having assaulted someone, and having ever smoked a cigarette or drunk alcohol were more strongly associated with depressive symptoms in 2015 than in 2005.
Odds of health outcomes for individuals with high depressive symptoms in 2005 and 2015.
In the first regression model we observed that cohort moderates the association between all five predictors and depressive symptoms, with stronger associations at higher levels of the predictors in 2015 compared to 2005. All of these remained after adjusting for confounders in step 2 (Table 2). There was a non-linear association between anti-social behaviours and depressive symptoms, especially in 2015, whereby depressive symptoms were highest in the mid-range of antisocial behaviours (see Figure 2, 1A-1E).
Regression coefficients from unadjusted and adjusted models for depressive symptoms, antisocial behaviours and substance use as outcomes
Fully adjusted regression model with all predictors and their cohort interactions included in the same model

Associations between predictor and outcomes variables in 2005 and 2015. Each row of the figure corresponds to a different outcome variable (1A-E: depressive symptom score; 2A-E: number of antisocial behaviours endorsed; 3A-E number of substances tried).
In the final regression mutually adjusting for all predictors, we found evidence of a substance use by cohort interaction, where cumulative substance use more strongly predicted depressive symptoms in 2015 than in 2005. Similarly, there was a weight perception by cohort interaction, where perceiving oneself as a higher weight more strongly predicted depressive symptoms in 2015 than in 2005 (see supplementary Figure S1).
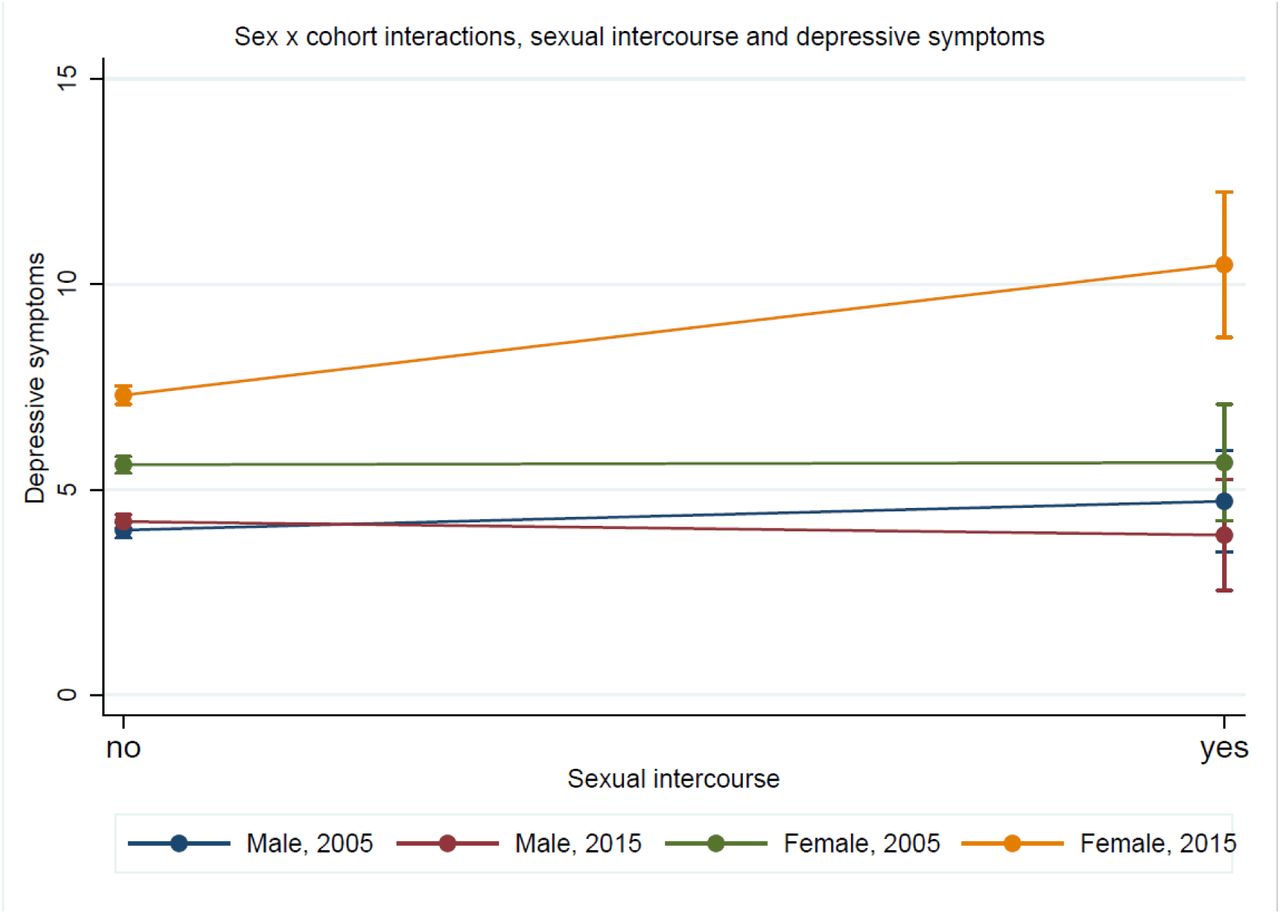
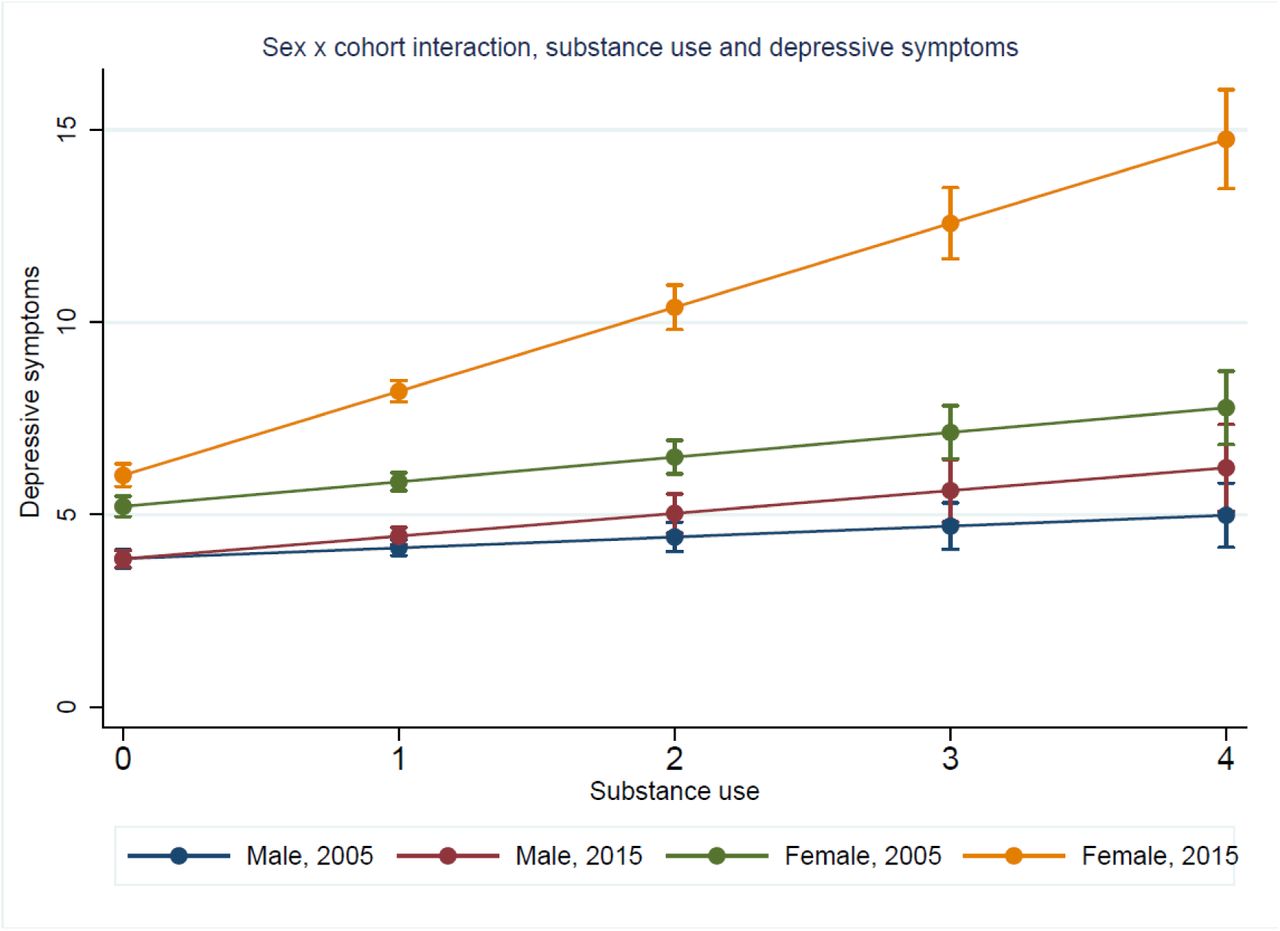
We investigated whether the cohort*predictor interactions were moderated by sex, and find that the cohort differences in substance use and sexual intercourse associations with depressive symptoms are primarily driven by differences in females between the cohorts, where females in 2015 demonstrate stronger associations where females with higher levels of substance use and having had sexual intercourse experience greater levels of depressive symptoms (see supplementary Fig S2a and 2b).
Antisocial behaviour as outcome
For antisocial behaviour, in the first model we observed associations moderated by cohort for depressive symptoms, BMI and weight perception, with the findings for depressive symptoms attenuated in the second model after adjusting for confounders (see Figure 2, 2A-2E). There was a slight non-linear association between substance use and anti-social behaviour where at higher levels of both they were more strongly associated. In the final model controlling for all other predictors there was evidence of interactions between cohort and weight perception and depressive symptoms (Figure S1). We found no evidence of moderation by sex of the cohort differences in these associations.
Substance use as outcome
For substance use, in the unadjusted model we observed associations moderated by cohort for depressive symptoms, antisocial behaviour and sexual intercourse and these were still observed in the adjusted model. There was a non-linear association between BMI and substance use, where the association was stronger at above average BMI and weaker at very high BMIs (see Figure 2, 3A-3E). In our final regression, after controlling for all other variables of interest and socio-demographic factors, we found evidence of an antisocial behaviour by cohort interaction whereby at lower levels of antisocial behaviour the association was stronger in 2005 than 2015, and at higher levels of antisocial behaviour the association with substance use was stronger in 2015 than in 2005. We found no evidence of moderation by sex of in the cohort differences in these associations.
Discussion
Examining prevalences in these two cohorts born 10 years apart indicated decreasing substance use and antisocial behaviours and increasing depressive symptoms.4 In this paper we examined cohort differences in the risk factor associations for these health outcomes to explore whether they are changing over time or are stable between cohorts. Broadly, we found that the associations are not always the same across cohorts, suggesting that they may be dynamic across time and are potentially modifiable by changes in environment, for example. Understanding the dynamic nature of these associations over time is valuable for identifying causal risk factors and their changing influence as societal and environmental factors also change. This will help in identifying potential targets for interventions that can be targeted as relevant for different generations.
In both cohorts, these outcomes were associated in expected ways, where higher levels of depressive symptoms, antisocial behaviours, substance use and health outcomes were associated positively and more likely to co-occur. However, the strength of these associations varied between cohorts, with some associations also varying at different parts of the distribution. In the more recent MCS cohort, outcomes seemed to be worse for those already at higher risk, for instance, stronger associations between higher BMI and substance use with depressive symptoms. In the case of substance use this cohort difference seemed to be primarily occurring in females. The findings highlight the potentially changing influence of certain risk factors in more recently born cohorts.
Turning to some of the specific findings, we found that having a higher BMI was more strongly associated with depressive symptoms in 2015 than in 2005. Part of this association was explained by the changed role of weight perception in mediating their association, with adolescents in 2015 who perceive themselves as being overweight having higher depressive symptoms than those who perceive themselves as overweight in 2005. These findings suggest that the implications of being overweight are more severe now than they were previously, and this might be attributed to an increasing focus on appearance and perceived pressures on young people to look a certain way,19 although we cannot test this in our data. Similarly, we observed a change between cohorts in the likelihood of antisocial behaviour and substance use in relation to depressive symptoms. For antisocial behaviour, there was a weakening in the association between depressive symptoms and the likelihood of these behaviours in 2015 compared to 2005, suggesting that the co-occurrence of these behaviours with higher psychological distress is decreasing, potentially reflecting a shift in how young people cope with difficulties, or the changing social acceptability of anti-social behaviours in adolescence. It is pertinent here that high levels of antisocial behaviours are less common in the more recent cohort. For substance use, we found lower levels of trying substances in the more recently born cohort, however, adolescents who report greater substance use, especially 3-4 substances (which are a small group, especially in 2015), have higher depressive symptoms in the recent cohort.
A key strength of this investigation is the use of two large contemporary cohorts with harmonised variables available at the same age. It is important to note that one cohort, ALSPAC, is a regional cohort and MCS is a national cohort. We control for socio-demographic characteristics in our analysis and given the focus on associations between these variables, rather than prevalences, the non-nationally representative nature of one cohort is less likely to lead to bias 12. It is also important to note that missing data was higher in ALSPAC than MCS, and although we conducted multiple imputation with key socio-demographic factors and all examined variables informing the imputation to reduce bias in estimates, some estimates might remain biased due to unmeasured factors associated with missingness and their potential association with our outcomes of interest. These analyses are cross-sectional and it is possible that the longitudinal associations between these outcomes is also dynamic across cohorts. Understanding the early life predictors that might be changing across these cohorts will provide additional insights into the changing prevalences and associations observed between these generations.
As well as our specific research findings, we believe this paper has important implications more broadly, about the nature of how risk factors impact on outcomes. That we have found evidence for changes in associations between cohorts suggests that risk factors are not stable over time, but rather dynamic, and a product of the societal and cultural contexts of the day. As societal and cultural factors change, these can augment or diminish the impact of certain risk factors on outcomes of interest, all of which are not independent of each other either. To assume that risk factors remain stable in terms of their ‘riskiness’ goes against the evidence. As such, where we rely on historical findings it is worth considering revisiting these in contemporary datasets, in order to ensure that any resulting public health interventions are likely to be effective. It is also important to consider that the relative impact of any one risk factor on an outcome is likely to depend on the strength of impact of all the other risk factors at play. For example, we know that the impact of genetic risk on outcomes is greater where environmental risk factors are minimised 20,21. Similarly, broad-brush interventions that improve outcomes such as public health efforts to reduce smoking might actually increase inequality, as they are more likely to be effective for those with better resources or support 22. Using non-linear modelling to investigate the patterns within the data might help to uncover examples where this is occurring. In our data, we find evidence that gradients are steeper for the more recent cohort, suggesting that even though smoking and alcohol use behaviours are decreasing at the population level in recently born adolescents, those that are involved in these behaviours are more likely to have co-occurring mental health and other problems than in previous generations.
Data Availability
ALSPAC and MCS cohorts are available to use upon application, and in the case of ALSPAC a fee.
Funding
This work did not receive specific funding. Praveetha Patalay is supported by a Wellcome Trust Grant (Ref: ISSF3/H17RCO/NG1). The UK Medical Research Council and Wellcome (Grant ref: 217065/Z/19|Z) and the University of Bristol provide core support for ALSPAC. A comprehensive list of grants funding is available on the ALSPAC website (http://www.bristol.ac.uk/alspac/external/documents/grant-acknowledgements.pdf)..The Millennium Cohort Study is supported by the Economic and Social Research Council and a consortium of UK government departments. The funders had no role in study design, data collection, data analysis, data interpretation, or writing of this report.
Author contributions
SG and PP planned the study, analysed the data and prepared the manuscript for publication. Both SG and PP have full access to the data presented in this report and act as guarantors for the paper.
Competing interests
Authors declare no competing interests.
Supplementary Materials for
This supplementary section includes
Correlations between all outcomes in ALSPAC (bottom left of the table) and MCS (top right of the table)
Fully adjusted regression model with all predictors investigating sex and cohort and sex interactions

Associations between predictor and outcome variables, including mutual adjustment for other predictors in 2005 and 2015. Each row of the figure corresponds to a different outcome variable (1A-E: depressive symptom score; 2A-E: number of antisocial behaviours endorsed; 3A-E number of substances tried).

Sex x cohort interaction for the association between number of substances used and depressive symptoms
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sex x cohort interaction for the association between sexual intercourse and depressive symptoms
Acknowledgments
We are grateful to all the families who took part in this study, the midwives for their help in recruiting them, and the whole ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists and nurses. The authors are grateful for the cooperation of the Millennium Cohort Study families who voluntarily participate in the study. They would also like to thank a large number of stakeholders from academic, policy-maker and funder communities and colleagues at the Centre for Longitudinal Studies involved in data collection and management. The authors would like to thank Richard Silverwood for advice on analytic approach.
Footnotes
Pre-registration: Gage SH, Patalay P. How have associations between mental health and health-related behaviours changed between 2005 and 2015? 6 Feb 2019.osf.io/bcrfu
References



