
Abstract
Influenza-like illness (ILI) accounts for a large burden of annual morbidity and mortality worldwide. A finer-grained knowledge of the parameters and dynamics of the viruses commonly underlying ILI is needed for modeling, diagnostic, and intervention efforts. We conducted an extensive literature review for epidemiological parameter values for influenza, respiratory syncytial virus (RSV), rhinovirus, human coronavirus (HCoV), and adenovirus. We also developed a deterministic SEIR model for ILI, and derived an expression for R0. We here report ranges and means for parameters for these five common viruses.
1 Introduction
Influenza-like illness (ILI) accounts for a large burden of annual morbidity and mortality worldwide (WHO 2020). Despite this, diagnostic testing for specific viruses underlying ILI is relatively rare (CDC 2019). This results in a lack of information about the pathogens that make between 9 million and 49 million people sick every year in the United States alone (CDC 2020). Yet knowledge of the specific diseases is necessary for timely treatment to prevent unnecessary suffering and death (Nguyen 2016, Van Asten et al. 2012, Pawelek et al. 2015).
ILI is defined by the CDC as fever of 100°F and a cough and/or a sore throat without a known cause other than influenza (CDC 2020). Defining ILI as a cluster of symptoms rather than a specific disease or diseases is necessary for keeping track of case counts, as well as for important analysis and forecasting (Osthus and Moran 2019). However, the cluster of symptoms known as ILI is caused by many under-lying pathogens (Taylor 2017, Galindo-Fraga 2013). Positive diagnosis is a prerequisite for accurate treatment. To respond to this need and to gain a finer-grained understanding of ILI that will contribute to a practical foundation for advances in diagnostics and interventions, we here review the literature for parameter values. We then compare the dynamics of five common upper respiratory viruses implicated in ILI: influenza, respiratory syncytial virus (RSV), rhinovirus, human coronavirus (HCoV), and adenovirus.
We conducted a literature review to establish plausible ranges for model parameters, and developed a deterministic system of ordinary differential equations to model the general dynamics of these five viruses.
2 Results of Parameter Literature Review
2.1 ILI Viruses
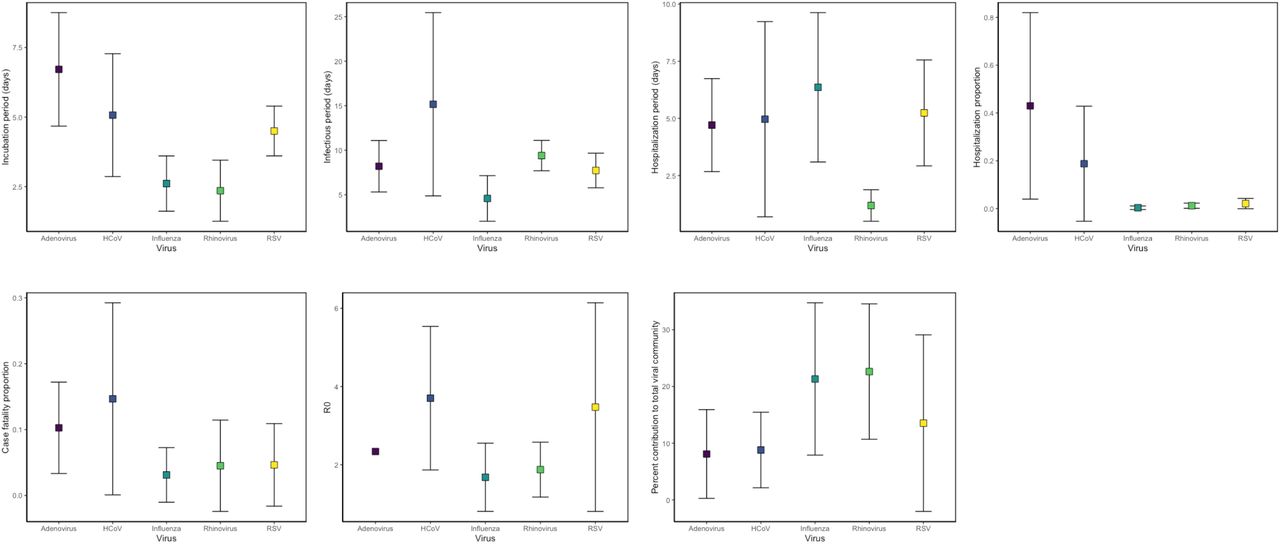
We reviewed the literature for the epidemiological parameters: incubation period, infectious period, hospitalization period, hospitalized proportion, case fatality proportion, and R0. We included results from experimental and observational studies, as well as from systematic reviews when there were insufficient studies. R0 values were estimated from modeling studies. In one case, (SARS-hCoV), we included an estimate for the infectious period, since values were lacking in the literature (Chowell 2004). We also searched the literature for the contribution made by each of the five viruses to the total viral community in people with ILI. Across ten study populations, at least one virus was identified in an average of 62% of individuals with ILI symptoms. Out of these 62% of patients with ILI in whom viruses have been identified, adenovirus was identified in 8.1% of samples, human coronavirus in 8.8%, RSV in 13.5%, influenza in 21.3%, and rhinovirus in 22.6%. Coinfection was not taken into account in these estimates.
Parameters for Influenza-like illness
2.2 Human Coronavirus
Parameters for HCoV
In view of the current outbreak of novel coronavirus 2019-nCoV, and given the need for plausible parameters for modeling efforts, we conducted an in-depth literature review for human coronavirus. 2019-nCoV has been identified as a member of genus betacoronavirus, along with SARS and MERS (WHO 2020). Until the genomes of 2019-nCoV have been further characterized, it seems reasonable to suspend assumptions about the epidemiological behavior of the novel virus, and to include all known strains in the parameter sets. Thus, our review includes values for strains 229E, NL63, OC43, HKU1, SARS, and MERS. Means have been collected when possible; when not available, medians have been recorded. Information on the studies, the strains, the sample sizes, and the references is available on pages 26-27 of this paper.
We included values for R0 only for SARS and MERS, and attempted to include them only for the period before large-scale interventions were implemented, since R0 is defined as the average number of sec-ondary infections produced when one infected individual is introduced into a fully susceptible population (K. Deitz, 1975). Since the seasonal strains of human coronavirus are endemic in the world, there is, by definition, no fully susceptible population for 229E, NL63, OC43, or HKU1 in which R0 may be assessed.
Results of our review for human coronavirus include the following mean values: an incubation period of 5.01 days, an infectious period of 15.2 days, a hospitalization period of 4.96 days, a hospitalized proportion of 0.188, a case fatality proportion of 0.147, and an R0 of 3.7.
3 Deterministic Model
3.1 Description of Model Structure
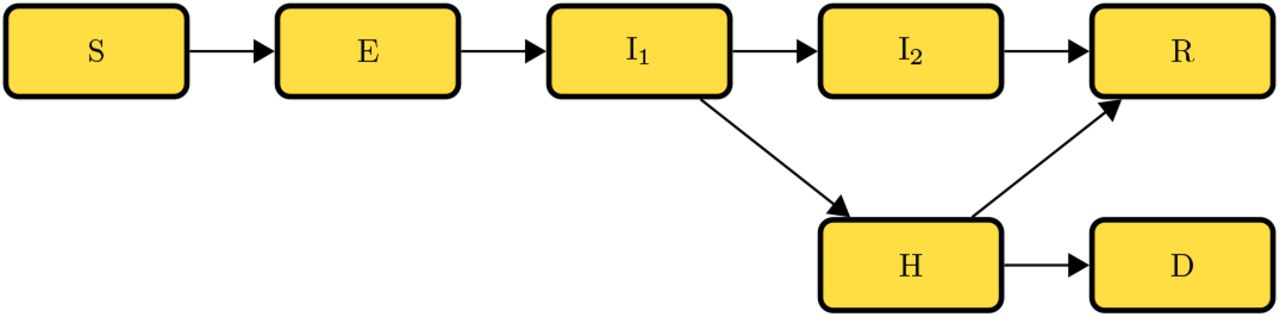
The model diagram (Fig.1) illustrates the progression of influenza-like illness (ILI) in a human population of a hypothetical small city containing 10,000 individuals. We assume density-dependence, that is, for a fixed population of 10,000 humans with negligible migration, the contact rate for individuals remains constant.

Viral Composition

Transfer diagram for ILI virus transmission.
The total population (N) consists of seven classes: susceptible (S), exposed but not infectious (E), first infectious class (I1), second infectious class (I2), hospitalized (H), recovered (R), or dead (D). Individ-uals are considered susceptible until they contact an infectious individual from (I1), (I2), or (H). Given contact with an infectious individual, transmission takes place with some probability. After transmission of the virus has occurred, susceptible people move to the exposed class (E), where they spend a number of days equal to the mean period of time between infection and the onset of infectiousness (the latent period). We assume here that the latent period equals the incubation period, or the mean period of time between exposure to the virus and the onset of symptoms. After the latent period, they move to the first infectious class (I1). The mean duration of the first infectious period differs according to the underlying virus. Symptoms worsen for some proportion of the first infectious class, who enter the hospital (H), where they remain infectious. Individuals who do not enter the hospital remain ill outside the hospital for the duration of the second infectious period (I2). From (I2), the length of which differs according to the underlying virus, where we assume that the progression of the illness is not severe, individuals recover. The duration of hospitalization differs according to the underlying virus. From the hospital, individuals either recover (R) or die (D). We assume that hospitalized individuals have 75% less contact with susceptible individuals, which results in 75% reduced transmission during hospitalization. We further assume that recovered individuals (R) gain full immunity to the virus causing the illness.
Descriptions of state variables
Model assumptions include:
From the initially infectious state, individuals progress to hospital or continued non-hospitalized infectious state.
From the non-hospitalized infectious state, individuals progress to recovery.
From the hospitalized state, individuals progress to death or recovery.
Everyone who recovers gains full immunity.
Total infected population = E + I1 + I2 + H.
Total infectious population = I1 + I2 + H.
The viruses operate independently.
The population is homogeneously mixed.
No demographics are included.
The transmission rate for each virus is calculated from the expression for R0 below, using the mean R0 values from the literature.
Descriptions and dimensions for parameters
3.2 Model Equations
The equations governing common upper respiratory virus dynamics are given by







The total population is N = S + E + I1 + I2 + H + R + D. Parameters
4. Quantities of Interest
4.1 Disease-free Equilibrium
We assume that the stable population, representing a hypothetical small city, is N = 10000. We further assume that the initial value for the Susceptible population is S0 = 10000. In the disease-free state, all infected classes are zero,that is, E = I1 = I2 = H = 0. Substituting and setting the derivatives equal to zero, it is evident that in the disease-free state, the other state variables R and D will continue to contain zero individuals, and that the Susceptible class S will remain equal to the total population N, as follows.







Additionally, if we set any one of E, I1, I2, or H to zero, the other three state variables representing infected classes must also be zero. In this case, N=S=10000. Thus, where x = (S, E, I1, I2, H, R, D) denotes solutions of the system, xdfe = (10000, 0, 0, 0, 0, 0, 0) represents the disease-free equilibrium for the system.
4.2 Basic Reproduction Number
Assuming a homogeneously mixed population, the basic reproductive number (R0) is defined as the average number of secondary infections produced when one infected individual is introduced into a fully susceptible population (K. Dietz, 1993). Four compartments, latently infected individuals (E), symptomatic and infected individuals (I1), symptomatic and infected and non-hospitalized individuals (I2), and hospitalized individuals (H), together characterize the total infected population for the ILI virus system. To calculate R0 for this system, we derive the next generation matrix (Van den Driessche and Watmough 2002).
Method:
Derive the matrix for the transmission term describing everyone entering (E): the “F” matrix;
Derive the matrix for the transition terms describing everyone transitioning between infected classes (E, I1, I2, H): the “V” matrix;
Next Generation Matrix (NGM) = (F)(V −1);
The largest dominant eigenvalue or spectral radius of the NGM = R0 for the system. The transmission term for the system is βS(I1 + I2 + cH)
The transmission terms for the system are (−γ1E), (γ1E − γ2I1), (γ2(1 − p1)I1 − γ4I2), (γ2p1I1 − γ3H).
The next generation matrix is
The spectral radius, or the largest positive eigenvalue of the next generation matrix, is the basic reproductive number of the system at the disease-free equilibrium, as follows.

This expression for the basic reproductive number (R0) depends on the parameters β, c, p1, γ2, γ3 and γ4, and on the initial conditions for the state variables. β is clearly directly proportional to R0.
CONCEPTUAL METHOD OF DERIVING R0
This result is equivalent to the result obtained, above, by the next generation method.
5. Discussion
There are several limitations to this study. First, the model is not age-structured. Second, the assumption that the latent period equals the incubation period may result in an overestimation of the latent period. This is because the beginning of the true infectious period may occur before the onset of symptoms; however, this is difficult to measure and is not generally reported in the studies that report values for the incubation period. Third, a single mortality rate has been modeled for the hospitalized infected and non-hospitalized infected classes. Fourth, many of the studies that generated parameter values evaluated populations treated at clinics or admitted at hospitals. However, a significant proportion of illness and death may occur outside of hospitals and clinics (see Cohen et al. 2017).
Much work remains to be done to elucidate the etiology of ILI.
Data Availability
The plots and spreadsheets that contain the details of our parameter review are included in the paper, after the reference section.
FUNDING STATEMENT
Research support provided by the U.S. Department of Energy through the Los Alamos National Laboratory. Los Alamos National Laboratory is operated by Triad National Security, LLC, for the National Nuclear Security Administration of U.S. Department of Energy (Contract No. 89233218CNA000001). LA-UR-20-21024.
JAS was partially funded by the University of New Mexico College of Arts and Sciences Dissertation Excellence Fellowship.

{kind=link}
{kind=link}
{kind=link}
INFLUENZA parameters: incubation period, infectious period, hospitalization period, hospitalization proportion, case fatality, R0
RSV parameters: incubation period, infectious period, hospitalization period, hospitalization rate, case fatality rate, R0
ADENOVIRUS parameters: incubation period, infectious period, hospitalization period, reduction of transmission in hospital, hospitalization rate, case fatality rate, R0
NOTE: adenovirus in the elderly produces keratoconjunctivitis, not a respiratory infection
HUMAN CORONAVIRUS parameters: incubation period, infectious period, onset of symptoms to hospitalization, hospitalization period, hospitalization proportion, case fatality, R0
RHINOVIRUS parameters: incubation period, infectious period, hospitalization period, hospitalization proportion, case fatality, R0
6 References



