
ABSTRACT
Background Individuals with Mild Cognitive Impairment (MCI) have more gait variability under dual-task conditions than cognitively healthy adults. However, characteristics associated with this susceptibility of gait to dual-task stress are unknown.
Methods Testing was performed at baseline in the Study of Mental And Resistance Training (SMART). Ninety-three adults with MCI (age 70±6.8 years; 66.6% female) performed a single- and dual-task walk (cognitive distractor=letter fluency), in random order. Linear and non-linear gait variability were measured using force-sensitive insoles. Cognitive performance during dual-tasking was assessed by the number of correct words vocalized. Cognitive function, brain Magnetic Resonance Imaging (MRI), muscle strength, aerobic capacity, body composition, physical and psychosocial function were also assessed as potential correlates of gait dynamics.
Results Gait dynamics worsened during dual-tasking, with decrements in both stride time variability (p<0.001) and detrended fluctuation analysis (DFA) (p=0.001). Lower aerobic capacity and thinner posterior cingulate cortex were associated with greater decrements in DFA (p<0.05). Smaller hippocampal volume, worse psychological well-being and poorer static balance were associated with greater decrements in stride time variability (p<0.05). By contrast, cognitive performance did not change under dual-task conditions compared to seated testing (p=0.13).
Conclusions Under dual-task conditions, participants with MCI preserved their cognitive performance at the expense of gait stability. Decrements in dual-tasking gait were associated with lower aerobic fitness, balance, psychological well-being, and brain volume in cognitively-relevant areas of the posterior cingulate and hippocampus, all potentially modifiable characteristics. Trials of targeted interventions are needed to determine the potential plasticity of gait variability in high-risk cohorts.
INTRODUCTION
The prevalence of gait abnormalities increases with age, affecting up to 35% of community-dwelling older adults1. Gait abnormalities are characterized by a more variable gait pattern, leaving affected individuals with an increased risk of falls2 and reduced mobility3. Adults with mild cognitive impairment (MCI), an intermediate stage between normal cognition and dementia, are more likely to have greater gait variability4 and consequently, double the risk of injurious and multiple falls compared to cognitively normal adults5.
Dual-tasking is a sensitive method used to investigate interactions between gait variability and cognitive function6, with worse gait performance under dual-task conditions associated with an increased fall risk amongst older adults78. Dual-tasking impairs gait in individuals with deficits in cognitive function, including MCI and Alzheimer’s disease9. However, studies evaluating dual-task associations between cognition and gait variability in older adults with MCI are limited. Furthermore, imaging studies of brain regions and their associations with gait variability have mainly focussed on single-task gait variability, or the effects of dual-tasking on gait speed10-12 rather than more comprehensive assessments of gait variability or cognitive performance under dual-task stress. Finally, identification of modifiable characteristics associated with gait dynamics under dual-task conditions could lead to targeted interventions to improve gait dynamics and ultimately reduce falls in older adults with MCI and other vulnerable cohorts. Therefore, the aim of the present study was to determine the effects of dual-tasking on gait dynamics and cognitive performance in older adults with MCI, as well as to identify relevant physical, psychosocial, and structural brain characteristics associated with decrements during dual-tasking (dual-task cost). We hypothesized that there would be a worsening of both gait and the performance of the secondary cognitive task during the dual-task condition, and that these reductions would be associated with lower strength, aerobic capacity, functional performance, psychosocial function and smaller hippocampal volume and posterior cingulate cortex thickness. These factors were selected a priori due to their known decrements in individuals with cognitive impairment, frailty, or elevated falls risk13.
METHODS
The complete study protocol for the Study of Mental and Resistance Training (SMART) has been published14, with primary15 and secondary outcomes published16,17. The study was approved by the Royal Prince Alfred Human Research Ethics Committee (X08-0064) on 24th of April, 2008, and written informed consent was obtained from all participants. The study was prospectively registered with the Australia New Zealand Clinical Trials Registry (ACTRN12608000489392). A cross-sectional analysis of baseline data from the SMART trial was used for this investigation.
Participants
One hundred community-dwelling older adults with MCI (Peterson criteria18) were recruited. Two participants could not wear gait monitors due to fused toes, while technical issues including incomplete data recording, precluded full gait data in five others. Thus, gait dynamics data were available for 93 participants. All participants were assessed at The University of Sydney, New South Wales, Australia.
Assessment of cognitive function
The primary outcome of the SMART trial was global cognition assessed using the Alzheimer’s Disease Assessment Scale - Cognition (ADAS-Cog). Global, executive, and memory cognitive domains were also calculated for the 93 participants with available gait variability data. Additional details can be found in the Supplementary methods.
Assessment of letter fluency at rest
Letter fluency, a subcategory of verbal fluency, was assessed using the COWAT19 to measure cognitive performance at rest. All participants were tested in a private room with a single research assistant, in a resting, non-fasting state at a similar mid-morning time. Participants were instructed to verbalize as many words as possible beginning with the letter “F” in 1 minute (FSINGLE), excluding proper nouns, repeated words, and variations of the same word using a prefix or suffix (e.g., foam and foaming). A score was calculated by totaling the number of admissible words written down by the research assistant.
Assessment of gait dynamics
Gait dynamics were assessed similarly to methods previously described20,21. Briefly, force-sensitive insoles were placed in the participants’ shoes to measure the force applied to the ground during a 2-minute period of ambulation at habitual pace using any assistive devices needed. Participants were instructed to wear low-heeled shoes, comfortable clothing and visual and hearing aids if required.
Gait assessment was performed under two conditions, ‘single-task’ (undistracted walking) and ‘dual-task’ (distracted walking), in a randomized order. Participants were not provided with any instruction regarding task priority (i.e, cognitive or gait performance), and were told to perform as well as possible for both tasks. Stride time variability (coefficient of variation, CV) and detrended fluctuation analyses fractal scaling exponent (DFA22,23 were calculated for both single-task [(CVSINGLE) and (DFASINGLE)] and dual-task [(CVDUAL) and (DFADUAL)] conditions. To assess stride-to-stride variability and arrhythmicity of gait, the coefficient of variation (CV) in each participant’s stride time was calculated using the formula CV = (Standard Deviation / Mean) * 100, with lower CV indicating more stable gait. To quantify how the dynamics of stride times fluctuate and change over time, we applied detrended fluctuation analysis (DFA) to each participant’s sequence of stride times. In general, physiologically healthy systems have fractal scaling indices between 0.8 and 1.0, with lower values (closer to 0.5) indicating a less healthy state24.
The secondary (cognitive distractor) task was the COWAT test, with the number of correct “F words” counted in the first minute of walking (FDUAL). The letter “F” was selected to remain consistent with the seated COWAT test described above (FSINGLE). The words were recorded using a portable recorder (Samsung YP-U3, Samsung Electronics Co., South Korea) and the recording was subsequently reviewed by the research assistant who counted the number of admissible words during the first and second minute. The number of correct words in the first minute only of the dual-task gait condition (FDUAL) was compared to the number of correct words during the FSINGLE condition. The order was not randomized for the assessment of “F” words, with the dual-task condition performed 1 week after the seated COWAT. The ‘dual-task cost’ for CV, DFA and F words were calculated (CVCOST= CVDUAL – CVSINGLE; DFACOST= DFADUAL – DFASINGLE; FCOST = FDUAL – FSINGLE).
Assessment of Neuroimaging Outcomes
Details of the neuroimaging assessment outcomes have been published14,17. Briefly, MRI data were acquired on a 3.0-Tesla Philips Achieva System (Amsterdam, The Netherlands). Brain structure was assessed using a T1-weighted whole-brain scan with isotropic voxel 1 mm3 (sequence: T1TFE; TR/TE: 6.39/2.9 ms; slice thickness 1.0 mm without gap; in-plane resolution 1 × 1 mm). Left, right hippocampal volume was manually traced, using ANALYZE (version 10, Mayo Clinic) following the published protocol25 For cortical thickness measurement, FreeSurfer (v5.1.0, http://freesurfer.net) was applied to calculate the cortical thickness at whole brain level. Then, the posterior cingulate mean cortical thickness was generated using the standard FreeSurfer parcellation (Desikan-Killiany Atlas)26.
Assessment of peak strength
Maximal strength testing was assessed via the one-repetition maximum (1RM) on Keiser pneumatic resistance machines (Keiser Sports Health Equipment, Ltd., Fresno, CA, USA). Participants’ 1RMs were determined on the leg press, knee extension, hip abduction, chest press and seated row machines. One RM tests were performed twice, one week apart, with the best performance used.
Assessment of peak aerobic capacity
Aerobic capacity (VO2peak) was determined via indirect calorimetry during a physician-administered, graded treadmill walking test to volitional fatigue. Methods and data handling have been previously published16.
Measures of physical function
Details of the physical function assessments have been published14. Static balance was assessed on one attempt using six different positions (wide stance, narrow stance, semi-tandem stance, tandem stance, one leg with eyes open and one leg with eyes closed). Dynamic balance was assessed using the time taken to forward tandem walk over a 3-meter marked course. Habitual and maximal gait velocities were assessed over two metres using an Ultra-timer (Raymar, Oxfordshire, UK). Lower extremity function and power was assessed using time to complete 5 sit-to-stands and stair climb power. Stair climb power was calculated using the following formula P (watts) = (M × D) × 9.8/t Where: M = Body mass (kg), D= Vertical distance (m), D = vertical height of the staircase, and t = Time (s). The 6-minute walk test (6MWT) was assessed twice, at least one week apart, with the furthest distance walked used. Further detail regarding these assessments can be found in the Supplementary methods.
Anthropometry and Body Composition
Height, naked body mass and waist circumference were measured as the mean of triplicate measures after a 12-hour overnight fast. Waist circumference was measured with Lufkin steel tape measure (W606 PM, Apex Tool Australia Pty Ltd, Albury, NSW, AU), using the International Diabetes Federation (IDF) protocol. Bioelectrical Impedance Analysis (BIA; RJL Systems, Inc., Clinton, MI, USA) was used to evaluate body composition. Whole body skeletal muscle mass (kg) and fat free mass (kg) were calculated using the average resistance and reactance values of three sequential BIA measures. Further details of the assessments are published14.
Measures of Psychosocial Function
Psychosocial function and wellbeing were measured via the Life Satisfaction Scale (LSS), Scale of Psychological Well Being (SPWB), Quality of Life Scale (QOLS), Physical and Mental Health Short-36 (SF-36), Depression Anxiety Stress Scale (DASS 21), Memory Awareness Rating Scale – Memory Functioning Scale (MARS-MF), Duke Social Support Index Scale (DSSIS) and Life Experience Questionnaire (LEQ). Further detail regarding these assessments has been published14
Statistical Methods
Data were inspected for normality. Normally-distributed data are presented as mean±SD and non-normally distributed data presented as median (interquartile range). All CV (CVSINGLE, CVDUAL and CVCOST) variables were log-transformed prior to use in parametric statistics. Sequential linear regression models (adjusted for age and sex) were constructed including potential confounders associated with the number of F words during the COWAT test (FSINGLE) and single- and dual-task gait dynamics (CVSINGLE and DFASINGLE). Next, linear mixed models with repeated measures were constructed to determine the effect of dual-tasking on both letter fluency and gait dynamics. The single-task condition (FSINGLE, CVSINGLE and DFASINGLE) was entered as time point 1, and the ‘dual-task’ condition (FDUAL, CVDUAL and DFADUAL) as time point 2. A compound symmetry covariance matrix was used. Models were adjusted for age and sex, with gait dynamics outcomes further adjusted for the order of the walking condition. Next, linear regression models were constructed to determine variables associated with FCOST, CVCOST and DFACOST. Models were adjusted for age, sex, and baseline score of the dependent variable and order of the condition for the gait dynamics assessment. All models involving cognitive performance (including FSINGLE and FCOST) were further adjusted for education, while models involving hippocampal volume and posterior cingulate cortex thickness were adjusted further adjusted for total intracranial volume. Models involving DFA were also adjusted for the number of medications, as justified below. Statistical significance was assumed at α<0.05. All data were analysed using IBM SPSS (version 24; IBM Corp., Armonk, NY, USA).
RESULTS
Baseline clinical characteristics of the participants have been published15. Data for the available 93 participants (66.6% women), were similar to the overall cohort (p>0.05 for all variables). The average age was 70.0±6.8 years, MMSE score 27.5±1.4, and habitual gait speed 1.21±0.24 m/s, with 17% of participants having a gait speed below 1.0 m/s. Participant characteristics data are presented in Table 1.
Factors associated with single task gait dynamics
The number of medications prescribed was inversely associated with DFASINGLE (r=-0.23, p=0.029), but not CVSINGLE (r=-0.03, p=0.75). There were no associations between age, sex, years of education, smoking status, drinking status or the number of chronic diseases and either index of gait dynamics. Consequently, all analyses with DFACOST as a dependent variable were adjusted for the number of medications.
Dual-Task Cost
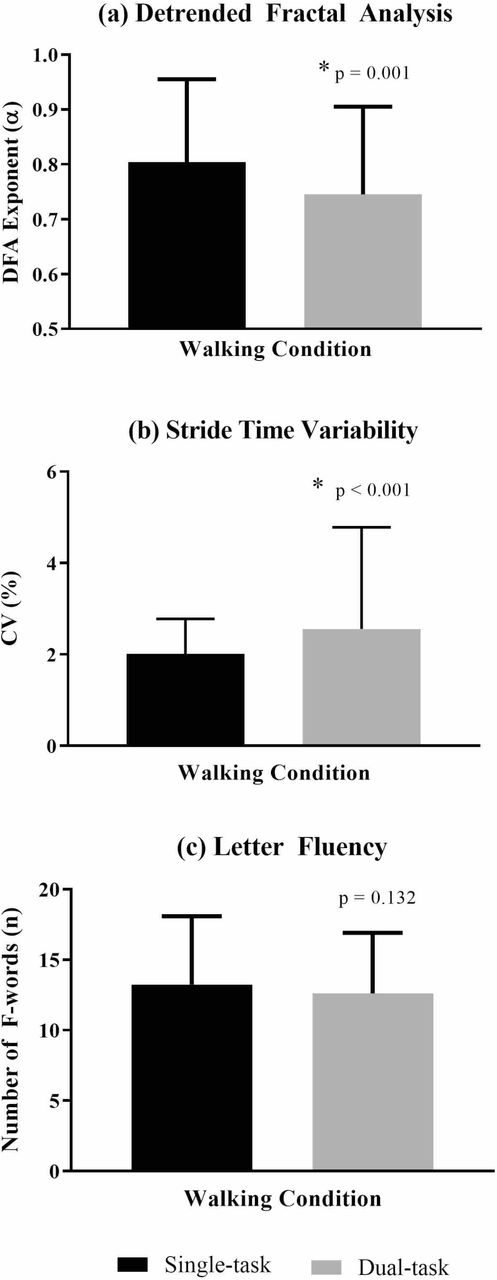
Data are presented in Figure 1. As hypothesized, gait dynamics worsened significantly during dual-tasking, with decrements in performance observed for stride time variability [single-task 2.012 (0.767), dual-task 2.555 (2.227); p<0.0001 and DFA (single-task 0.804±0.151, dual-task 0.745±0.160; p=001). However, contrary to our hypothesis, cognitive performance on the COWAT did not significantly change under dual-task conditions (single-task 13±5 words, dual-task 12±4 words, p=0.13; Figure 1). Changes in letter fluency (FCOST) were not associated with changes in gait dynamics for either CVCOST (r=-0.14, p=0.171) or DFACOST (r=0.03, p=0.746).
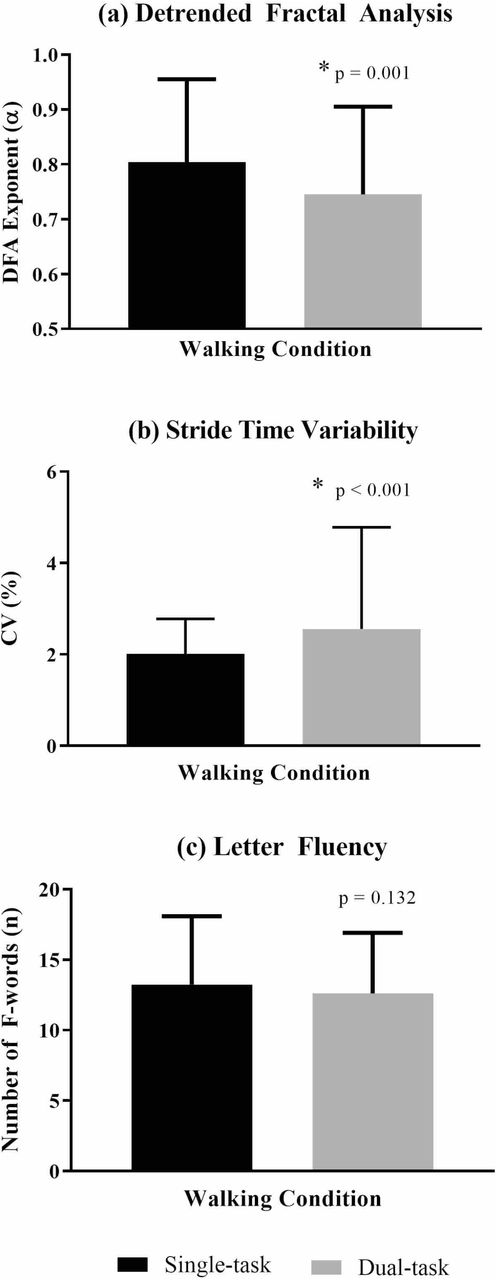
Gait dynamics and cognitive performance under single-task and dual-task walking conditions.
Graphed results under single-task and dual-task walking conditions for (a) DFA, (b) Stride time variability (CV) and (c) Letter fluency. Data for (a) and (c) are presented as mean±SD and data for (b) are presented as median (IQR) with all adjusted pairwise. DFA = detrended fluctuation analysis fractal scaling exponent; CV = coefficient of variation. Higher scores are worse for CV. Lower scores are worse for DFA and Letter Fluency.
Factors associated with changes in stride time variability component of gait during dual-tasking (CVCOST)
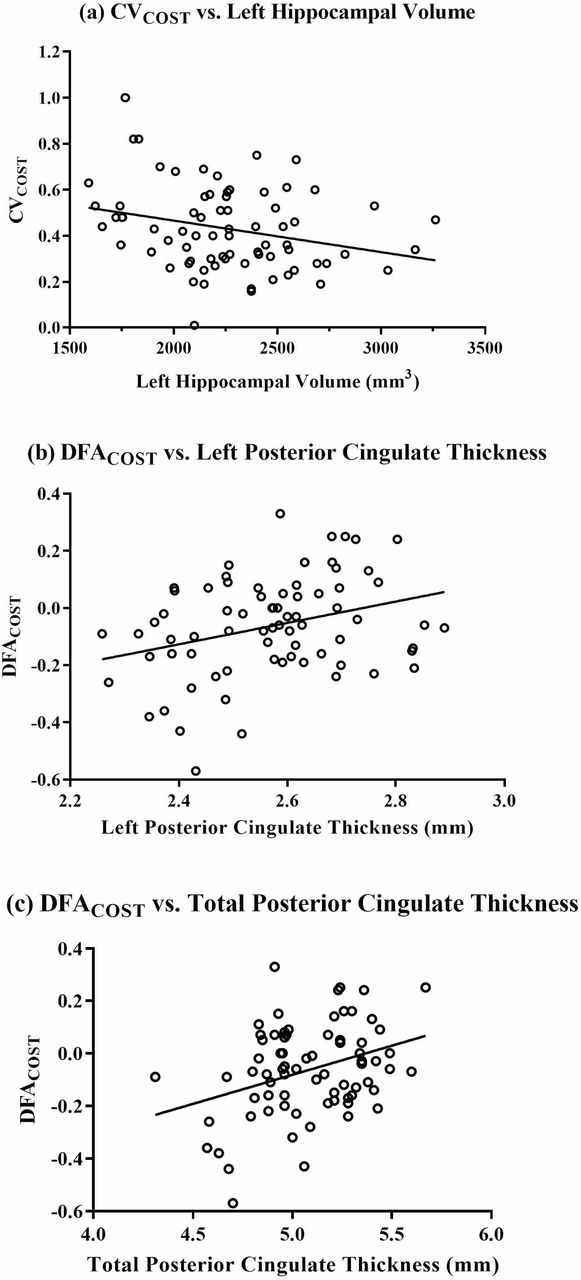
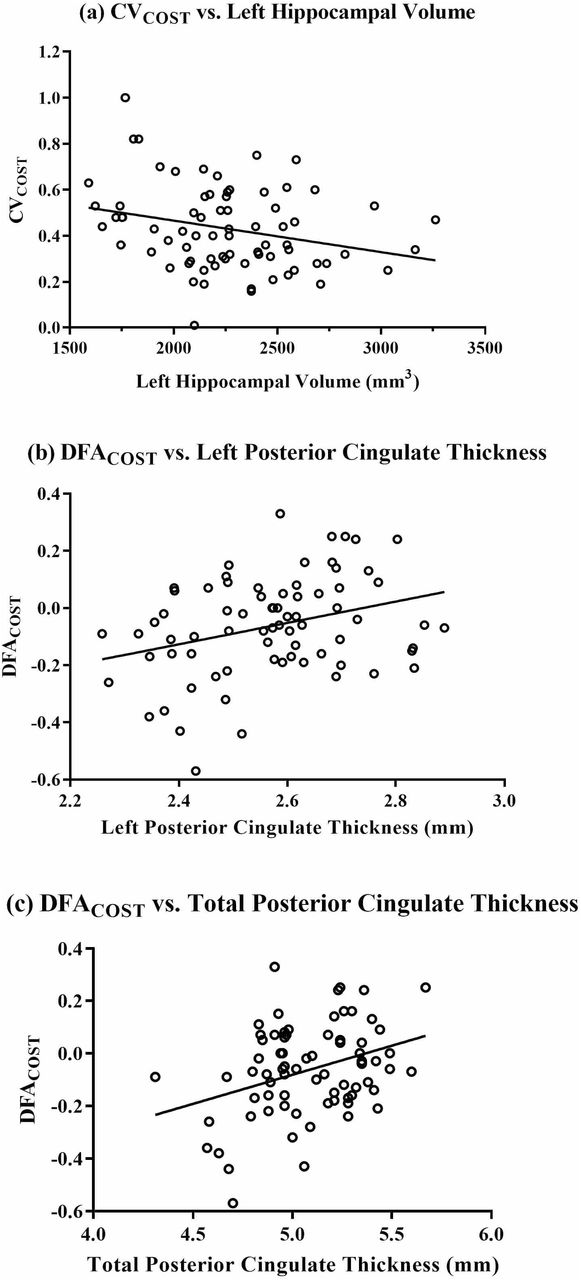
For simplicity, significant associations are presented in Table 2. A complete set of results can be seen in the Supplemental material. Contrary to our hypotheses, cognitive performance (executive function, memory, attention and global domains) was not associated with CVCOST under dual-task conditions (p>0.05). However, higher (worse) CVCOST was associated with smaller left hippocampus volume (r=-0.35, p=0.023) with a similar trend for total hippocampus volume (r=-0.31, p=0.050). Gait dynamics and brain morphology data are presented in Figure 2.
{kind=link}
{kind=link}
Relationship between gait dynamics and brain morphology Graphed results of gait dynamics and MRI associations for (a) CVCOST and left hippocampal volume, (b) DFACOST and left posterior cingulate thickness, and (c) DFACOST and total posterior cingulate thickness. CVCOST = the dual-task cost of stride time variability. DFACOST = the dual-task cost of DFA. DFA = detrended fluctuation analysis fractal scaling exponent. CV = coefficient of variation. Cost variables are calculated by subtracting the single-task from the dual-task. Higher cost indicates greater gait decrement during dual-tasking.
Worse dynamic balance (longer tandem walk time) was directly associated with a higher CVCOST (r=0.28, p=0.022). However, CVCOST was not associated with body composition, aerobic capacity, strength or other measures of functional performance.
As hypothesized, psychological well-being was inversely associated with CVCOST, with higher (better) Environmental Mastery, Personal Growth, Personal Relations, Purpose in Life, Self-acceptance and total score on the Psychological Wellbeing Scale associated with preservation of gait under dual-task conditions (p<0.05). Similarly, CVCOST was inversely associated with Duke Social Support Index Scale (DSSIS), indicating that the lower level of, and satisfaction with, social support was associated with a greater gait impairment during dual-task conditions (p<0.05).
Factors associated with changes in fractal scaling exponent of gait during dual-tasking (DFACOST)
For simplicity, significant associations are presented in Table 2. A complete set of results can be seen in the Supplemental material. Contrary to our hypotheses, cognition and psychosocial function were not associated with DFACOST under dual-task conditions (p>0.05). Notably, as anticipated, greater left (r=0.23, p=0.026) and total (r=0.25, p=0.015) posterior cingulate cortex thickness as well as better performances in the 6MWT (r=0.25, p=0.025) and aerobic capacity (r=0.24, p=0.033) were related to preservation of gait during dual-tasking. However, DFACOST was unrelated to lower body strength (r=0.25, p=0.063), whole body strength (r=0.25, p=0.079), static balance time (r=0.18, p=0.075) or tandem walk score (r=-0.12, p=0.254).
DISCUSSION
The primary finding from this novel investigation was that in older adults with MCI, resting cognitive performance on a letter fluency task was preserved under dual-task conditions, whereas a significant worsening of gait dynamics, both in the magnitude (CV) and time course (DFA), was observed. This finding in adults with MCI is consistent with the concept of “posture second” that has previously been observed in healthy older adults27 and adults with Parkinson’s disease28. In adults with MCI who have a reduced cognitive reserve compared to cognitively healthy adults, the preservation of cognitive function at the expense of a stable gait may partially explain why people with MCI are at a greater risk of falling than healthy peers5. Furthermore, worsening of DFA was associated with lower posterior cingulate cortex thickness and aerobic and walking capacity, while worsening of stride time variability was associated with smaller hippocampal volume, static balance and psychological well-being. In contrast, single-task (seated) cognitive function predicted neither gait variability nor gait dynamic changes during dual-tasking. Although previous studies4 have focused on the decrements in gait under dual-task conditions, our study has also investigated for the first time the effects of dual tasking on cognitive performance in MCI, as well as the mediating role of brain morphology and physical/psychological function on gait stability in MCI.
This is the first report to our knowledge that thicker left and total posterior cingulate cortices were associated with preservation of DFA during dual-tasking. This is in agreement with previous data showing a greater dual task cost on gait speed (slowing down) is associated with lower grey matter volume of the hippocampus and cingulate cortex (including both anterior and posterior cingulate cortex) amongst other regions12. More recently, greater dual task cost on gait speed was associated with lower entorhinal cortex volume in older adults with MCI11, a region of the brain known to have structural and functional connections with the posterior cingulate cortex29,30. The posterior cingulate cortex contributes to motor imagery31, and assists in directing the focus of attention32,33, and is known to be one of the areas to atrophy early in the course of Alzheimer’s disease33,34. Posterior cingulate thickness reduction with age, MCI or dementia could theoretically reduce walking coordination and result in a more variable gait, particularly during dual-tasking.
We also report for the first time in this cohort that lower left and total hippocampal volume were associated with greater deficits in stride time variability during dual-tasking. The hippocampus contributes to rhythmicity of locomotion35 and is known to atrophy in individuals with MCI faster than in healthy adults36. Hippocampal volume has been associated with gait variability in both cognitively healthy adults, and adults with cognitive impairment10, but data are lacking under dual-task conditions. Our findings suggest that hippocampal atrophy associated with MCI may contribute to a diminished ability to regulate gait dynamics under the stressful condition of dual-tasking in this cohort.
Notably, we have previously shown that high intensity strength training increases posterior cingulate thickness17 and that this change in posterior cingulate thickness is directly associated with the cognitive benefits of the strength training17. While no change in the hippocampus was observed in SMART17 or other studies of progressive resistance training37, hippocampal volume has been shown to increase following aerobic exercise in adults with MCI37. Future investigations are needed to determine whether gait dynamics under dual-task conditions improve following structured aerobic or resistance training programs, and if any observed improvements are mediated by structural brain changes.
Higher aerobic capacity and 6-min walking distance were associated with better preservation of DFA during dual-tasking. High intensity treadmill training has been shown to improve aerobic capacity and cognition in adults with amnestic MCI38, whereas most other low-moderate intensity aerobic interventions have yielded non-significant findings in this cohort39. Progressive resistance training can also improve aerobic capacity and cognitive function, (mediated by muscle strength gains), as we have previously shown within this cohort16. However, given the cross-sectional nature of our analyses, reverse causality cannot be excluded. Individuals with a less variable gait may be more likely to walk more frequently and thus have a greater aerobic capacity and functional performance compared to individuals with a more variable gait pattern. Longitudinal exercise studies are required to investigate whether improved aerobic/walking capacity will also improve gait variability during single- and dual-task conditions.
Muscle strength was not related to the preservation of either DFA or stride time variability during dual-task walking. This differs from data we previously reported showing that higher muscle strength was related to lower variability measures in community-dwelling older adults2, and that improvements in muscle strength following a multi-modal exercise program were associated with reduced stride-time variability in older adults with functional impairment40. However, consistent with the current findings, others have reported that stride time variability in older adults with higher level gait disorders was not associated with muscle strength24, nor was step time variability improved by a muscle strengthening intervention41. All of the above studies only measured gait variability under single-task conditions, and thus, the potential benefit of interventions to improve muscle strength on gait variability under dual-task conditions are unknown.
The dual-task cost of stride time variability was greater in those with lower psychological well-being (SPWB) across the domains of Environmental Mastery, Personal Growth, Personal Relations, Purpose in Life and Self-acceptance. These data are in agreement with previous evidence suggesting that worse stride time variability is associated with an increased fear of falling24, and fear of falling itself has been previously associated with limitations in physical, mental and social functioning42. Additionally, MCI has been associated with reduced psychological wellbeing43 and increased falls2, supporting a potential link between worsened gait dynamics and poor psychological wellbeing, although reverse causality or bi-directional relationships cannot be ruled out. Consistent with our findings on psychological well-being, depression is a well-known risk factor for falls and hip fractures44, independent from anti-depressant medications, which pose additional fall risk45. It is important to note however that our cohort was free from clinical depression at entry into this study by design. Given the known relationship between hippocampal atrophy and depression46, the potential link between depressive symptoms, brain morphology and gait dynamics is an important area for future investigation in relevant high-risk cohorts with this co-morbidity.
Limitations
As noted above, reverse causality may explain some of the study outcomes due to the cross-sectional study design. Also, the order of the COWAT assessment and dual-task walking was not randomized. The presentation of the “F” word task at rest prior to dual-tasking may have produced a learning effect, minimizing any potential to observe cognitive deficits during dual-tasking. Future studies should randomize the sequencing of single- and dual-task cognitive performance.
CONCLUSIONS
Older adults with MCI preserved their cognitive performance at the cost of the variability and dynamics of their gait under dual-task conditions. Novel associations were observed between worsening of the fractal scaling exponent of gait and posterior cingulate cortical thickness, while worsening of stride time variability was associated with lower hippocampal volume. Better aerobic and walking capacity, psychological wellbeing and static balance were also associated with preservation gait stability during dual-tasking. Notably, all of these factors have previously been shown to be modifiable with robust exercise modalities in clinical trials. Longitudinal research is required to determine the extent to which gait dynamics are also modifiable, and the optimal exercise prescriptions needed to promote optimization of gait patterns, resilience to stressors, and ultimately reduce fall risk in vulnerable cohorts.
Conflict of Interest
MV has previously received honoraria for speaking at Pfizer and The Brain Department Pty Ltd sponsored events, and receives industry in-kind support from collaborating software companies Synaptikon, Cambridge Brain Sciences and COGSTATE. He is also scientific founder of University of Sydney spin-out company Skin2Neuron Pty Ltd, from which he receives consulting fees and in which he has a financial interest in through the University’s shareholding and IP Policy. These interests have no relationship to this work. HB is an Advisory Board member for Nutricia Australia. BB is a member of advisory boards and/or gave presentations for the following companies, for which he has received honoraria: AstraZeneca, Lundbeck, Pfizer, Servier, and Wyeth. PS has received honoraria from Biogen Australia Pty.
Funding source
This study was funded by a National Health and Medical Research Council of Australia Dementia Research Grant (512672). Additional funding for a research assistant position was sourced from the NHMRC Program (568969), and the project was supported by the University of Sydney and University of New South Wales. MV was supported by a University of New South Wales Vice Chancellor’s Fellowship and a NHMRC Clinical Career Development Fellowship (1004156).
Author Contributions
Study concept and design: TCH, RS,YM, MAFS and JMH. Acquisition of data: NG, GCW, NJ, JM, CS, MKB, NF and YW. Analysis and interpretation of data: TCH, RS, YM, MAFS and JMH. Drafting of the manuscript: TCH, RS, YM, JMH and MAFS. Critical revision of the manuscript for important intellectual content: TCH, RS, NG, GCW, NJ, JM, WW, MKB, NF, YW, HB, NS, BTB, CS, PSS, MV, YM, MAFS and JMH. Statistical analysis: TCH, RS and YM. Obtained funding: HB, WW, NS, BTB, PSS, MV, MAFS. Administrative, technical, and material support: NJ, JM, CS. Study supervision: NG, HB, PSS, MV and MAFS.
Acknowledgements
This work fulfilled a portion of the degree requirements for PhD for NG and CS, and Master’s Degree for TH. Donations for participant rewards were received from Gregory and Carr Funerals. We would also like to thank the extraordinary generosity and commitment of the participants and their families who devoted their time to the SMART study.
Footnotes
Trial Registration: Australian New Zealand Clinical Trials Registry (ANZCTRN1260800048932)
REFERENCES




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos