
Abstract
Background Healthcare workers (HCW) treating COVID-19 patients are at high risk for infection and may also spread infection through their contact with vulnerable patients. Smell loss has been associated with SARS-CoV-2 infection, but it is unknown whether monitoring for smell loss can be used to identify asymptomatic infection among high risk individuals, like HCW.
Methods We performed a prospective cohort study, tracking 473 HCW across three months to determine if smell loss could predict SARS-CoV-2 infection in this high-risk group. HCW subjects completed a longitudinal, novel behavioral at-home assessment of smell function with household items, as well as detailed symptom surveys that included a parosmia screening questionnaire, and RT-qPCR testing to identify SARSCoV-2 infection.
Results SARS-CoV-2 was identified in 17 (3.6%) of 473 HCW. Among the 17 infected HCW, 53% reported smell loss, and were more likely to report smell loss than COVID-negative HCW on both the at-home assessment and the screening questionnaire (P < .01). 67% reported smell loss prior to having a positive SARS-CoV-2 test, and smell loss was reported a median of two days before testing positive. Neurological symptoms were reported more frequently among COVID-positive HCW who reported smell loss (P < .01).
Conclusions In this prospective study of HCW, self-reported changes in smell using two different measures were predictive of COVID-19 infection. Smell loss frequently preceded a positive test and was associated with neurological symptoms.
INTRODUCTION
A salient feature of SARS-CoV-2, the virus that causes COVID-19, is its ability to rapidly spread, leading it to affect over 100 countries in a matter of weeks. It is increasingly clear that asymptomatic and pre-symptomatic infection play an important role in the ongoing spread of COVID-19 [1]. Peak infectiousness likely occurs on or before symptom onset [2, 3], with a significant proportion of secondary infections arising from the index case during the pre-symptomatic stage [4, 5], highlighting the urgent need for non-invasive screening tools to identify people who may be asymptomatic or pre-symptomatic. This is especially true for healthcare workers (HCW) treating COVID-19 patients. HCW are at high risk for nosocomial infection themselves and may unknowingly spread infection through contact with hospital staff and patients [6–8]. However, universal masking, social distancing measures, and other interventions have decreased the risk for HCW in recent months [9, 10].
Reduced olfactory sensitivity, or anosmia, has been identified as a common manifestation of COVID-19. Olfactory loss has been identified by self-report in 15-85% of COVID-19 patients in Korea [11], Italy [8, 12–14], Spain [15], Canada [16, 17], the UK [18], and Iran [19]. Remarkably, the correlation between the risk of COVID-19 and self-reported olfactory loss has been reported to be as high as r = 0.87 [19]. Among patients with active COVID-19 assessed for smell loss, 41% and 98% had impaired tests of olfaction, on the Sniffin’ Sticks test [20] and the University of Pennsylvania Smell Identification Test (UPSIT) [21], respectively. Smell loss is also being evaluated for its diagnostic value in COVID-19 case identification [22]. However, smell loss has not yet been prospectively evaluated as a potential screening tool to identify SARS-CoV-2 infected individuals during the asymptomatic or pre-symptomatic phase.
Testing for objective smell loss using standard laboratory or clinical techniques is not feasible for widespread testing, and self-report surveys are not sufficiently reliable, therefore an accessible at-home smell sensitivity screen is of paramount importance. At-home self-monitoring for the first sign of diminished smell function would enable rapid testing and/or self-quarantine, thus protecting the community from exposure and preventing further spread prior to a formal diagnosis.
The aim of this study was to determine if tracking smell sensitivity and loss using an at-home assessment could identify HCW who are infected with SARS-CoV-2. High risk HCW who were undergoing routine (every 3 days) viral screening for SARS-CoV-2 infection completed a novel at-home brief smell sensitivity screen, the Yale Jiffy (Supplemental Table 1), to track their ratings of odor intensity perception using household olfactory stimuli. HCW also self-reported smell and taste loss changes across this time, along with commonly used symptoms to screen for COVID-19.
METHODS
Study Setting, Population, and Recruitment
We conducted a prospective cohort study of smell symptomology nested within the Implementing Medical and Public Health Action against Coronavirus (CT) (IMPACT) study at Yale University (HIC # 200027690). The goal of the parent study was to prospectively follow COVID-negative HCW at high risk of acquiring infection due to occupational exposures. The study recruited HCW working in the medical ICU or dedicated COVID-19 units at Yale New Haven Hospital (YNHH), a 1,541 bed tertiary care hospital located in New Haven, CT, USA. All participants provided written and/or verbal informed consent. Inclusion criteria for the IMPACT study included: a) aged 18 or older; b) English-speaking; c) working in a health care facility (YNHH or Yale Health); d) possible moderate to high risk exposure to COVID-19, or work in a COVID-19 unit in the hospital, and e) SARS-CoV-2 negative at study entry. For this analysis of smell alterations and COVID-19, we excluded subjects without at least one SARS-CoV-2 PCR result (described below) and those who had not completed at least one daily symptom questionnaire or Yale Jiffy (described below). All reported data were collected between March 31 and July 7, 2020.
Viral testing
SARS-CoV-2 real-time quantitative polymerase chain reaction (RT-qPCR) testing was performed on self-collected nasopharyngeal and saliva specimens every three days. Specimens were processed and tested on the same day as collection following previously described protocols [23, 24]. Two HCW reported positive results from a CLIA-certified lab outside of the study protocol.
Yale Jiffy
The Yale Jiffy is an online survey developed to screen for smell loss. The Jiffy can be conducted in under five minutes using readily available household items. The questionnaire includes two sections: 1) self-ratings of ability to smell, and 2) ratings of strength of smell in response to olfactory and trigeminal stimuli. Peanut butter (or jam/jelly if peanut butter was unavailable) was used as the olfactory stimulus as it has minimal or no trigeminal component, allowing for isolation of effects on the olfactory system. We also included a stimulus with a trigeminal component as a control stimulus (i.e., vinegar).
First, participants were asked to rate their ability to smell on a categorical scale (Poor/Average/Good/Very Good), to report any reduction in smell in the past week on a categorical scale (None/Slight/Moderate/Severe), and to rate the degree of reduction on a 100mm (0.0-10.0) visual analog scale (VAS). Next, participants were asked to hold the olfactory stimulus (i.e., peanut butter) one inch from their noses and to provide ratings of both the strength of smell (0.0-10.0) and how different it smells from normal (0.0-10.0). HCW then held the trigeminal stimulus (i.e., vinegar) one inch from their nose and rated strength of sensation of irritation and difference from normal, as above. Since olfactory sensitivity fluctuates across the day [25], HCW were asked to complete the survey at approximately the same time each day using the same stimuli each time they completed the test.
Responses were collected using Qualtrics, a secure HIPAA-compliant web-based survey platform, and retention was encouraged using daily e-mail reminders.
Daily Symptom Questionnaire
As part of the IMPACT study, HCW completed a daily symptom questionnaire administered via e-mail. HCW were given a list of symptoms and prompted to indicate whether they had developed such symptoms in the past 24 hours. Listed symptoms included objective fever (≥100.4°F), subjective fever, cough, shortness of breath, stuffy nose, sore throat, chills, sweating, malaise, fatigue, muscle pain, anorexia, nausea, vomiting, diarrhea, abdominal pain, and dizziness. In addition, we included screening questions for parosmia – changes in odor quality perception [26] – and for hypogeusia – reduced ability to taste [27]. Participants completed four parosmia screening questions(Supplemental Table 2), indicating how often they were bothered by common complaints caused by smell distortions, with responses ranging from “always” (1 point) to “never” (4 points). Parosmia was defined as a cumulative score less than or equal to 14 (out of 16) in any parosmia survey. HCW responded to four hypogeusia screening questions for saltiness, sourness, sweetness, and bitterness, by indicating that they could detect these tastes “Easily” (3 points), “Somewhat” (2 points), or “Not at all” (1 point). Hypogeusia was defined as any total score less than the maximum of 12 points.
Statistical Analyses
Descriptive statistics were used to characterize the study population. The Fisher’s exact and Wilcoxon rank-sum tests were used to compare COVID-19-positive and negative HCW. Multivariable logistic regression models were developed to calculate adjusted odds ratios for the associations between smell symptoms and COVID-19 diagnosis. Each model included one symptom as the predictor and additionally adjusted for age, sex, body mass index (BMI), ethnicity, and number of symptom surveys completed.
To further examine the strength of association between symptoms of smell loss and a diagnosis of COVID-19, we compared HCW reporting smell loss to a subset of HCW never reporting smell loss who were well-matched on age, sex, ethnicity, and the number of daily symptom surveys completed. We used the R package ‘MatchIt’ for this analysis, specifying a control to case ratio of 2:1 and employing optimal matching, which minimizes the overall differences between cases and controls in the dataset. To estimate the strength of association between smell loss and a diagnosis of COVID-19, we conducted conditional logistic regression using the matched dataset and the R package ‘survival.’ We compared results of three matched logistic regression analyses among those reporting smell loss on either survey (Yale Jiffy or daily symptom questionnaire), on the Yale Jiffy only, and on the daily symptom questionnaire only. Sensitivity analyses tested whether inclusion of covariates was needed to adjust for residual confounding after matching, determined by a change in the point estimate of > 10%.
Finally, we summarized responses to the Yale Jiffy and daily symptom questionnaires and used Fisher’s exact and Wilcoxon rank-sum tests to compare responses between COVID-19-positive and COVID-19-negative HCW. We also examined and described longitudinal responses among HCW who completed the questionnaires multiple times.
All analyses were conducted with a two-sided statistical significance level of P < .05 using R statistical software (version 3.4.2) and Microsoft Excel.
RESULTS
Participant characteristics
In total, 588 HCW were recruited and consented in the IMPACT study between March 31 and July 7, 2020, of whom 473 (80%) were eligible for the smell sub-study (Figure 1). Within the smell sub-study population, 373 (79%) participants were female; the mean (SD) age was 37.5 (11.2) years; 375 (79%) were white non-Hispanic/Latino; 261 (55%) were registered nurses (RNs) and 98 (21%) were medical doctors (MDs) (Table 1). Compared to HCW included in the smell analysis, IMPACT HCW ineligible for the smell sub-study were more likely to be Black, Asian, or other ethnicity (P < .001) and have higher BMI (P = 0.004) (Supplemental table 3).

Flow diagram of participants and reported changes in smell by COVID-19 status. Abbreviations: HCW, healthcare workers; IMPACT, Implementing Medical and Public Health Action against Coronavirus (CT).
HCW included in the smell sub-study completed the e-mail daily symptom questionnaire (including parosmia/hypogeusia screening) a median 23 times per HCW (IQR: 10, 34). Among the 313 (66%) HCW who completed the Yale Jiffy at least once, HCW completed a median of 10 (IQR: 3, 28) Jiffy questionnaires.
5771 SARS-CoV-2 RT-qPCR tests were performed on the 473 HCW in the smell sub-study (median = 11 tests per HCW) between March 31 and July 7. 17 (3.6%) HCW tested positive for SARS-CoV-2.
HCW who eventually tested positive for COVID-19 were more likely to report smell loss on the Yale Jiffy and daily symptom questionnaire
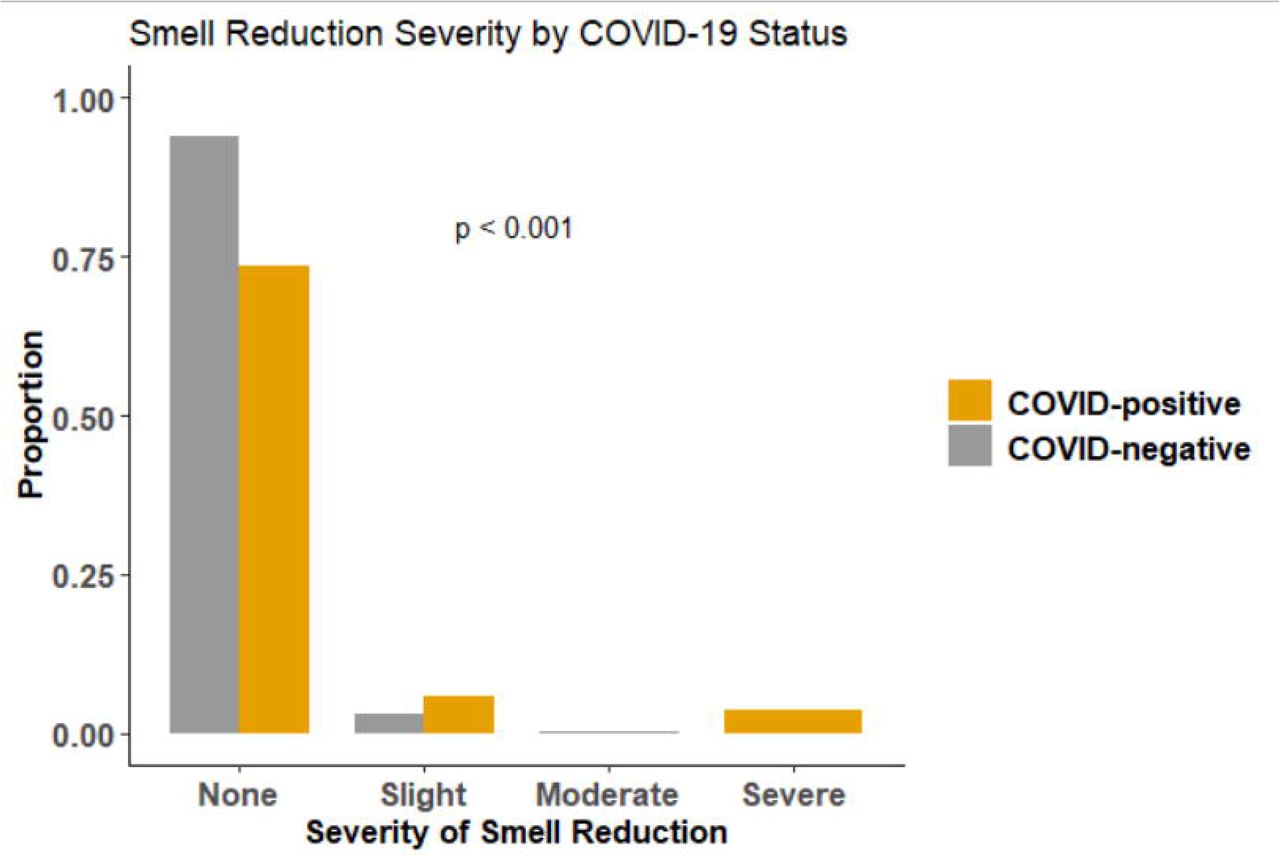
The demographic characteristics of COVID-19-positive HCW were similar to those of COVID-19-negative HCW (Table 1). Nine of the 17 (53%) COVID-positive HCW completed the Yale Jiffy at least once. COVID-positive HCW were more likely to report categorical smell loss on the Jiffy, with 5/9 (56%) COVID-positive HCW versus 43/304 (14%) COVID-negative HCW reporting smell loss (OR = 7.6, 95% CI: 2.0-29.4) (Table 1). The five COVID-positive HCW who reported categorical smell loss via the Jiffy had a mean (SD) reduction in smell of 5.8 (4.0) on a 100mm (0.0 to 10.0) scale; those indicating severe loss had a mean 8.3 (3.0) decrease compared to 2.2 (0.5) in those with slight smell loss. For individuals with any smell loss reported via Jiffy, COVID-positive HCW reported severe (60%) or slight (40%) smell loss on a categorical scale, while COVID-negative HCW reported slight (88%) or moderate (12%) smell loss. A Fisher’s exact test of independence showed that COVID-positive HCW reported more severe smell loss than COVID-negative HCW (P < .001) (Figure 2). Pairwise comparisons at each level of smell loss severity showed that COVID-positive HCW were more likely to report severe smell loss compared to COVID-negative HCW reporting any other levels of smell loss (Ps < .05).

Comparison of the proportions of self-reported severity of smell loss on the Yale Jiffy by COVID-positive and COVID-negative healthcare workers.
All 17 COVID-positive HCW eligible for the smell sub-study completed at least one daily symptom questionnaire. Eight (47%) reported parosmia compared to 83/456 (18%) COVID-negative HCW (OR = 4.0, 95% CI: 1.5-10.7). Hypogeusia was reported in seven (41%) COVID-positive HCW and 104/456 (23%) COVID-negative HCW (OR = 2.4, 95% CI: 0.7, 7.1) (Table 1). Six of those seven also reported smell loss.
Relative to Day 0 (defined as the day of the positive COVID test), the median timing of reported smell loss was Day −2 (IQR, Day −16 to Day +2) among COVID-positive HCW reporting smell loss, with 6/9 (67%) reporting smell loss before test positivity (Figure 3). Subjects recovered their sense of smell a median of nine days (IQR, 4, 16.5) after first reporting smell loss. Parosmia or smell loss was the first reported symptom in 3/9 (33%) COVID-positive HCW who reported smell loss.
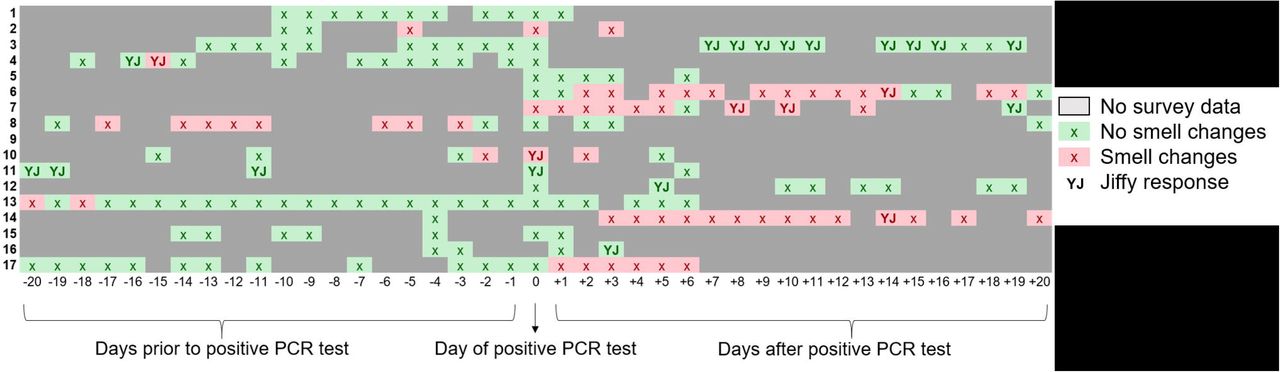
Chronology of smell changes among COVID-positive healthcare workers relative to day of positive test. Red boxes indicate smell change was reported via either the symptom survey or Yale Jiffy. Green boxes indicate no smell change reported. Solid gray boxes indicate there was no Yale Jiffy or symptom survey submitted for that day. Boxes with a “YJ” specifically indicate a Yale Jiffy response.
Associations between smell symptoms and COVID-19 diagnosis
Overall, in either the daily symptom questionnaire or Yale Jiffy, nine (53%) COVID-positive HCW reported smell loss or parosmia, compared to 105/456 (23%) COVID-negative HCW (OR = 3.7, 95% CI: 1.2, 11.5). After adjusting for age, sex, BMI, and number of symptom questionnaires, smell loss remained a significant predictor of a COVID-19 diagnosis (aOR = 4.5, 95% CI: 1.6, 13.3). Among other symptoms screened for in the HCW, only dyspnea (aOR 7.26, 95% CI: 2.22, 22.4) and headache (aOR 6.06, 95% CI: 1.78, 28.4) were more strongly predictive of a COVID-19 diagnosis.
Similar results were obtained through the matched analysis. 114 HCW reported any smell loss in either the daily symptom questionnaire or the Yale Jiffy. Optimal matching resulted in a sample of 228 HCW who never reported smell loss. The results of matching on age, sex, ethnicity, BMI, and number of questionnaires are shown in Supplemental Figure 1. Using this matched dataset, conditional logistic regression estimated a significant association between ever reporting smell loss and SARS-CoV-2 infection (OR = 6.0, 95% CI 1.6-22.2). Similar results were obtained when restricting the matched analysis to the 89 HCW who reported smell loss via the daily symptom questionnaire only (178 matched controls, OR = 3.2, 95% CI 1.1-9.8) or the 47 HCW who reported smell loss via the Yale Jiffy only (94 matched controls, OR = 5.0, 95% CI: 1.0-25.8), although the smaller sample size for the Yale Jiffy resulted in a less precise estimate. Results were not sensitive to the inclusion of covariates to adjust for residual confounding after matching.
Associations between smell loss and neurological symptoms in COVID-19 positive HCW
Table 2 summarizes findings among COVID-19-positive HCW stratified by smell loss as reported by either measure. COVID-positive HCW who reported smell loss were older than those who did not report any smell loss (median [IQR], 35.5 [29.8, 59.8] vs. 26.0 [25.0, 29.0] years, P = 0.05). There was also a trend toward lower cycle threshold (i.e., higher viral load) among COVID-positive HCW reporting parosmia specifically (mean [SD], 26.8 [4.5] vs. 30.9 [3.2], P = 0.07), but not among HCW reporting any smell changes in either survey.
Neurological symptoms as assessed by the daily symptom questionnaire, including headache and dizziness, were reported in all nine COVID-positive HCW reporting smell loss, and three (38%) of those who did not report smell loss. Prolonged neurological symptoms (> seven days after positive test) were reported in four (44%) COVID-positive HCW with smell loss versus one (13%) COVID-positive HCW without smell loss. Three COVID-positive HCW, all of whom experienced smell loss, had significantly prolonged neurological symptoms (> 20 days after positive test).
DISCUSSION
In this prospective study of a high-risk HCW population, we assessed loss of smell alongside routine viral testing, and found that HCW who acquired SARS-CoV-2 infection over the course of the study had significantly increased odds of reporting smell loss compared to COVID-negative HCW. This finding was consistent across bivariate (OR = 3.7), regression-adjusted (OR = 4.5), and matched (OR = 6.4) analyses. Likewise, COVID-positive HCW reported significantly more severe smell loss and parosmia compared to COVID-negative HCW. Overall, our findings demonstrate the efficacy and feasibility of using prospective, self-administered, at-home assessments of smell sensitivity to track changes over time in a group of individuals who are at high risk for SARS-CoV-2 infection.
Our findings are consistent with recent research demonstrating robust associations between smell perturbations and SARS-CoV-2 infection. These studies have found that smell and taste impairments are reported prior to (20%) or during (13%) hospitalization [12], typically lasting 4-17 days [28], and provide better predictive ability than fever or cough [29], two of the more commonly used symptoms to screen for COVID-19. Indeed, a large cross-sectional study found that sudden self-reported smell loss was the best predictive indicator of COVID-19 infection [30]. Our study extends these findings by uniquely assessing for prospective smell loss alongside viral screening in a high-risk group, all of whom were COVID-19 negative at study entry. We further describe an association between reduction in smell ability and neurological symptoms in COVID-19. Moreover, we found that distortion in smell was a better predictor of COVID-19 than many other physical symptoms. Cough, headache, and dyspnea were also significantly associated with an increased odds of COVID-19 diagnosis in this study. However, these symptoms are commonly experienced in other respiratory infections and not specific symptoms for COVID-19, and therefore less useful than loss of smell for monitoring for COVID-19 among asymptomatic individuals.
The mechanisms leading to COVID-19 related smell loss may be due to penetration of the spike protein of SARS-Cov2 into the sustentacular support cells in the olfactory epithelium, leading to inflammation and damage to the olfactory sensory neurons [31]. Under this model, we expected smell loss to specifically affect olfactory ability, and not influence trigeminal sensation. However, given limited data we were unable to sufficiently evaluate whether there were differences between olfactory and trigeminal stimuli ratings in COVID-negative vs COVID-positive HCW.
Our study has several limitations. Smell sensitivity and loss using the Yale Jiffy were evaluated using both categorical responses and a VAS [32]. Indeed, those indicating severe loss did show an average of an 8.3 point decrease on the 100mm (0.0-10.0) scale, compared to a 2.2 point reduction in those indicating slight loss, suggesting categorical responses are sufficient for identifying asymptomatic carriers. However, because many participants already had smell loss the first time they completed the VAS, we were not able to detect any changes. Consistent daily ratings of a household item could prove useful for further evaluating the magnitude of loss but would require further instructions and possibly practice using the scale. Adopting the generalized labeled magnitude scale (gLMS), a specialized line scale with semantic labels at empirically derived intervals, may also improve outcomes, as this scale is less subject to floor and ceiling effects. However, it does require some training and practice. Additionally, the low number of positive cases limited statistical power.
In our study, self-reported changes in smell perception were predictive of COVID-19 infection in a healthcare worker population. At-home smell assessments should be considered for non-invasive screening of groups that are at high risk for COVID-19.
Data Availability
All data generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Notes
Yale IMPACT Research Team authors
(Listed in alphabetical order) Staci Cahill, Edward Courchaine, Christina Harden, Chaney Kalinch, Daniel Kim, Lynda Knaggs, Eriko Kudo, Peiwen Lu, Alice Lu-Culligan, Nida Naushad, Allison Nelson, Isabel M. Ott, Annsea Park, Mary Petrone, Sarah Prophet, Lorenzo Sewanan, Maria Tokuyama, Jordan Valdez, Arvind Venkataraman, Chantal B.F. Vogels, Annie Watkins, Yexin Yang
Funding Statement
This work was supported in part by the National Institutes of Health [K23MH118999 and 1R01AI157488 to SFF], a gift to Yale for DMS from Mr. Brett Wilson, the Beatrice Kleinberg Neuwirth Fund and the Yale Schools of Medicine and Public Health.
Conflict of Interest
All authors declare no competing interests.
Acknowledgements
The authors are grateful to the study participants for their time and commitment to the study. We thank all members of the staff at the Yale IMPACT Study and to Mr. Brett Wilson for his generous donation to support this project.





{kind=link}
{kind=link}
{kind=link}