
ABSTRACT
Neural tube defects (NTD) are the most common congenital birth defects. The reason for the NTD cause is still not completely known, but it is believed that some genetic and environmental factors might play a role in its etiology. Among the genetic factors the polymorphism in the folate gene pathway is crucial. Numerous studies have suggested the possible role of maternal higher plasma concentration of homocysteine and low concentration of folate and cobalamin in the development of NTD but some negative studies are also published. So, in this study, authors tried to find out the exact relation between NTD and maternal biomarkers like folate, cobalamin and homocysteine by conducting a meta-analysis. Different electronic databases were searched for the eligible studies. Standardized mean difference (SMD) with 95% confidence interval (CI) was used to determine association between maternal markers as risk for NTD pregnancy. The p value <0.05 was considered statistically significant in all tests. All the statistical analyses were done in the Open Meta-Analyst program. The homocysteine is significantly associated with the increased risk of NTD (SMD= 0.57; 95% CI: 0.35-0.80, p= <0.001; I2= 93.01%), s-folate showed protective role in NTD (SMD= −0.48; 95% CI: −0.77 to −0.19, p= 0.001; I2= 95.73%), similarly cobalamin is also having protective role (SMD= −0.28; 95% CI: −0.43 to −0.13, p= <0.001; I2= 80.40%). In conclusion this study suggest that different maternal biomarkers may be used for the early prediction of the NTDs.
INTRODUCTION
Neural tube defects (NTD) are very common congenital birth defects [1]. NTD is the general term for a number of malformations but the most common of them are anencephaly, encephalocele and spina bifida. The prevalence of NTD is 1 in 33 infants globally [2]. A recent meta-analysis suggests that the prevalence of NTD in India is 4.5 per 1000 births [3]. NTDs are caused by the failure of closure of neural tube either partially or completely. The reason for the same is still not clear but it is believed that some genetic and environmental factors might play a role in the etiology of NTD [4]. Among the genetic factors the most important is the polymorphism in the methylenetetrahydrofolate reductase (MTHFR) gene. This gene has a polymorphism at 677th position which makes this enzyme thermolabile [5]. A recent meta-analysis suggests that polymorphism in this gene increases the chance of the NTD affected pregnancies [6]. The MTHFR enzyme regulates the level of homocysteine. Experimental studies have already suggested that the low level of homocysteine is responsible for the improper closure of the neural tube in mouse model [7]. Several published articles also reported that higher maternal homocysteine concentration is associated with the increased risk of NTD affected pregnancies [8-10]. Higher plasma homocysteine concentration is also reported as to be associated with different diseases like-Down syndrome [11-13], cleft lip and palate [14-16], cardiovascular disease [17-20], diabetes [21], and cancer [22-24] etc.
Although various previous studies have suggested that the elevated level of homocysteine [8-10] or lower level of the folic acid [8, 25, 26] and cobalamin [8, 10, 27] are the risk factors for the etiology of the NTD but the result are conflicting with some negative results. So here in this paper we try to find out the exact relation of these maternal biomarkers with the etiology of the NTDs by conducting a meta-analysis.
MATERIALS AND METHODS
Literature search
Different databases (PubMed, ScienceDirect, and SpringerLink) were searched for the eligible studies. The keywords used were “neural tube defects”, or “NTD” in association with “homocysteine”, “folic acid”, or “cobalamin”.
Inclusion and exclusion criteria
A study included in this meta-analysis only if it was-(i) a case-control study; (ii) reported the level of homocysteine, folic acid, and cobalamin in NTD mothers and control mothers; (iii) either provided mean ± standard deviation (SD) or sufficient data to calculate mean and SD. Similarly, the studies excluded if they were-(i) reviews, meta-analysis, animal model studies, letter to editor, case reports; (ii) not in English.
Data extraction
From all the eligible articles, following information were extracted-first authors family name; ethnicity; country of study; journals name with year of publication, mean and SD of homocysteine, folic acid and cobalamin. In some publications the authors provided median and range so we calculated the mean and SD as per the method of Hozo et al. [28]. All the information was retrieved by two authors independently (UY and PK) and if any discrepancy found it was sorted out by consultation with the corresponding author.
Statistical analysis
Standardized mean difference (SMD) with 95% confidence interval (CI) was calculated to determine association between risk for NTD pregnancy and maternal markers i.e. homocysteine, folic acid and cobalamin. The p value <0.05 were considered statistically significant in all tests. The between study heterogeneity was calculated by Cochran’s Q test and quantified by I2 tests [29] were applied. If heterogeneity is present (I2>50%) random-effects model was applied [30] otherwise fixed-effects model was applied [31]. Publication bias was determined by visualization of the symmetry of the funnel plot. Publication bias was evaluated by the Egger’s linear regression method [32]. All the statistical analyses were done by Open Meta-Analyst program [33]. All p-values were two-tailed with a significance level at 0.05.
RESULTS
Characteristics of selected studies and meta-analysis
(i) For homocysteine
Five hundred and ninety-six studies were retrieved by electronic database search. Out of which 33 studies were assessed the level of homocysteine in NTD mothers [8-10, 26, 27, 34-61]. Arbour et al. [40] reported two different populations (Cree and non-Cree) we treated them as separate studies so finally for homocysteine we have 34 studies (2,109 cases and 3,514 controls).
Meta-analysis revealed an SMD of 0.57 (95% CI: 0.35-0.80, p= <0.001; I2= 93.01%) indicating that elevated level of homocysteine is associated with NTD. High heterogeneity was found so random effect model was applied. Strong correlation was observed in the Asian population (SMD= 1.11, 95% CI: 0.56-1.66, p= <0.001; I2= 97.05%). The Caucasian population has low effect of homocysteine (SMD= 0.41, 95% CI: 0.21-0.62, p= <0.001; I2= 80.98%). Low effect of homocysteine is also found in the African population (SMD= 0.19, 95% CI: −0.40-0.78, p= 0.52; I2= 68.57%) (Table 1; Figure 2).

Flow diagram of study search and selection process.

Random effect forest plot of standardized mean differences of homocysteine. Results of individual and mean estimates, and 95% CI of each study were shown. Horizontal lines represented 95% CI, and dotted vertical lines represent the value of the mean.
(ii) For s-folate
Three hundred and ninety-three studies were retrieved by our search criteria. Out of which 36 studies were assessed the level of s-folate in NTD mothers [8-10, 25-27, 34-39, 41-43, 45-55, 58, 59, 61-68]. In the selected 36 studies the number of cases and controls were 2,131 and 3,983 respectively.
Meta-analysis revealed an overall SMD of −0.48 (95% CI: −0.77 to −0.19, p= 0.001; I2= 95.73%) indicate that elevation in s-folate level in controls play a protective role in the etiology of NTD. High heterogeneity was found so random effect model was applied. The level of s-folate is higher in the Asian population (SMD= −1.37, 95% CI: −2.14 to −0.61, p= <0.001; I2= 97.85%) in comparison to the Caucasian population (SMD= −0.17, 95% CI: −0.35 to 0.004, p= 0.05; I2= 78.89%). Low effect of s-folate is also found in the African population (SMD= −0.03, 95% CI: −0.56 to 0.49, p= 0.90; I2= 60.89%) (Table 1; Figure 3).
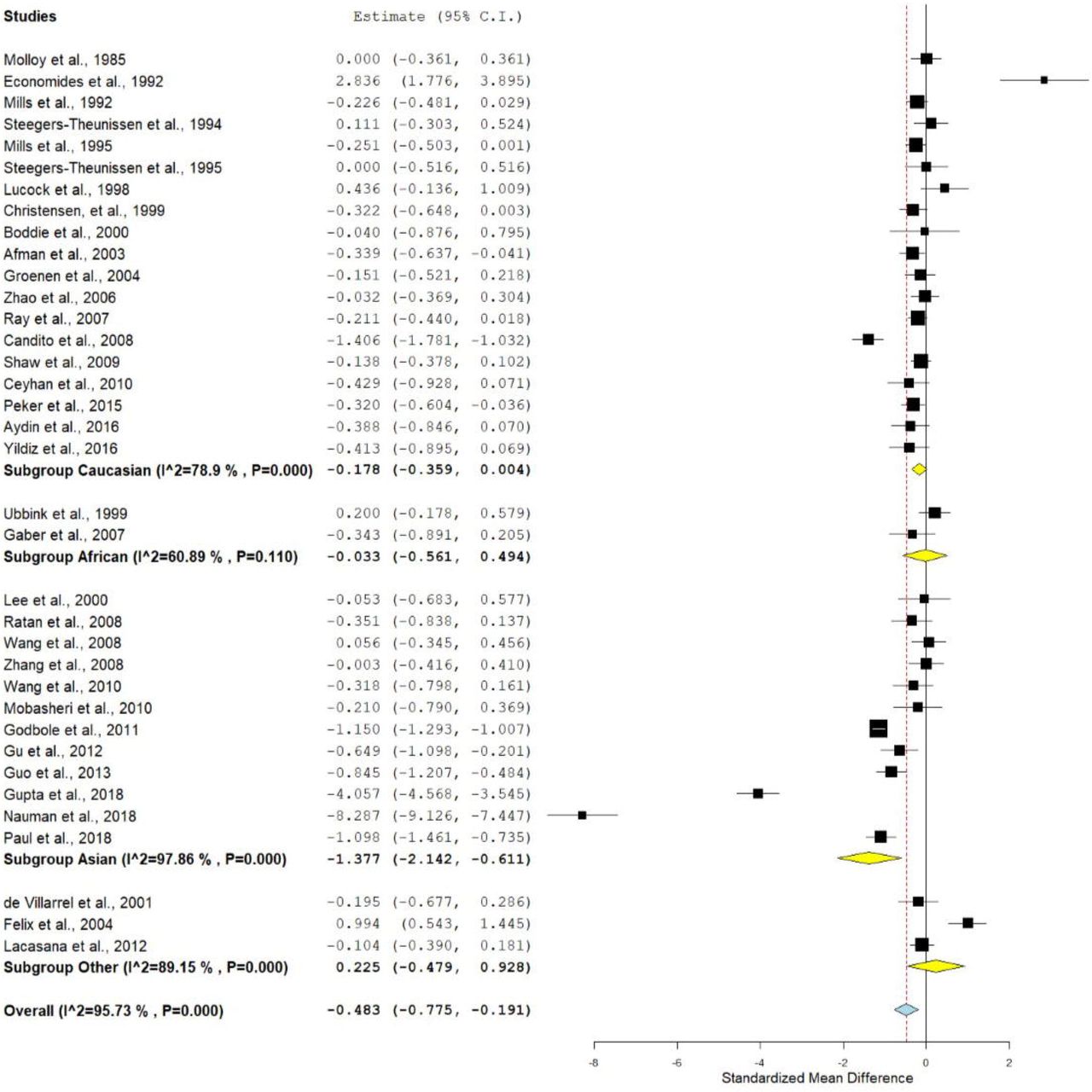
Random effect forest plot of s-RBC folate.
(iii) For cobalamin
Three hundred and twenty-six studies were retrieved by our search criteria. Out of which 28 studies were assessed the level of cobalamin in NTD mothers [8, 9, 26, 27, 34-43, 45-47, 49-54, 58, 59, 62-64]. Arbour et al. [40] reported two different populations (Cree and non-Cree) we treated them as separate studies so finally for cobalamin we have 29 studies (1,640 cases and 3,163 controls).
Meta-analysis revealed an overall SMD of −0.28 (95% CI: −0.43 to −0.13, p= <0.001; I2= 80.40%) indicate that elevation in cobalamin level in controls shows the decline in the NTD. Higher heterogeneity was found so random effect model was adopted. The level of cobalamin is low in the Asian population (SMD= −0.18, 95% CI: −0.67 to 0.31, p= 0.46; I2= 90.12%) in comparison to the Caucasian population (SMD= −0.30, 95% CI: −0.42 to −0.17, p= <0.001; I2= 52.95%). Low effect of cobalamin is also found in the African population (SMD= −0.40, 95% CI: −0.86 to 0.06, p= 0.09; I2= 49.85%) (Table 1; Figure 4).

Random effect forest plot of cobalamin.
Publication bias
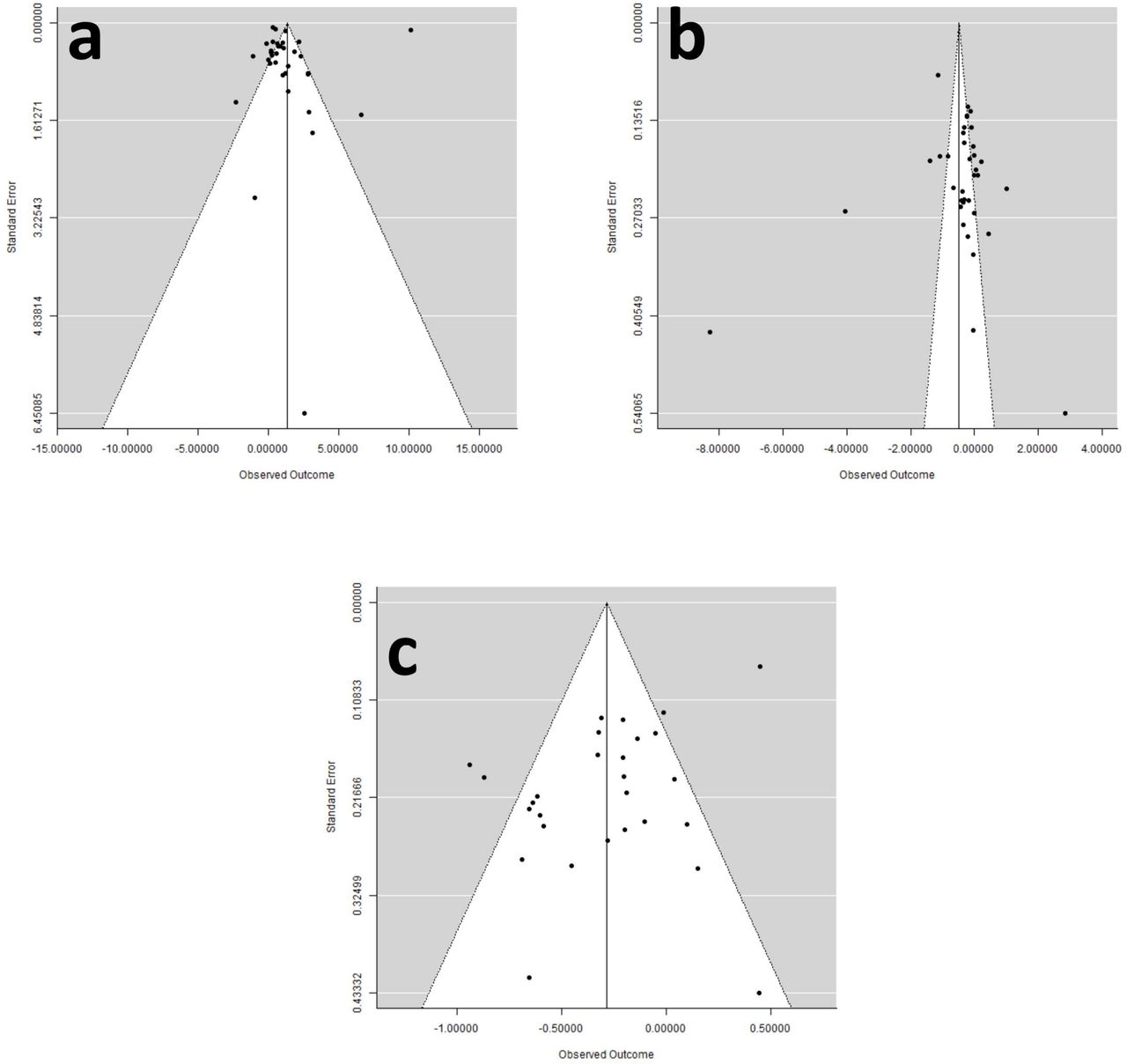
The funnel plots were symmetrical in all contrast models (Figure 5), and the P values of Egger’s test were more than 0.05, which provided statistical evidence for the absence of publication bias.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plots (standard error by mean difference)-a) homocysteine; b) s-RBC folate; c) cobalamin.
DISCUSSION
This meta-analysis was conducted to check the association between maternal homocysteine, folate and cobalamin levels as risk factors for the etiology of NTDs. We found that the homocysteine is a risk factor for the NTD affected pregnancies. While the folic acid and cobalamin level plays a protective role against the NTD affected pregnancies. It was long known before that the periconceptional folic acid supplementation prevent the NTD [35, 69]. The mechanism by which the NTDs are prevented by dietary folate supplementation is still not fully elucidated. Folic acid is essential for different cellular processes like-cell division, replication and DNA methylation etc. [70-73]. Proper DNA methylation is necessary for the maintenance of chromosome structure and gene expression and both are crucial for the normal development of the fetus [74]. Low plasma folate and /or MTHFR C677T polymorphism increases homocysteine in expecting mothers, which consequently affects the DNA methylation pattern and DNA synthesis of the developing fetus. Improper methylation interferes with the genes regulating neural tube closure [7]. Further higher concentration of homocysteine is toxic and generates free radicals by auto-oxidation and free radicals are toxic for the fetus [75].
Meta-analysis is an effective tool for combining studies having lower effect size. During past decade a number of meta-analyses were published examining the effect of different gene polymorphisms on various disease/disorder susceptibility like-MTHFR frequency [76], MTRR frequency [77], NTD [6], Down syndrome [78-79], schizophrenia [80-81], epilepsy [82], esophageal cancer [83], breast cancer [84], digestive tract cancer [85], and prostate cancer [86], etc.
During our literature search we found two meta-analyses evaluating the role of homocysteine and NTDs [87, 88]. Tang et al. [87] found that the homocysteine has an association with the NTD with ratio of means (RoM) of 1.16 (95%CI: 1.09-1.23, p= 1.8×10−6). They also reported that the NTD-affected mothers have lower levels of folate, RBC folate and vitamin B12. The other study was published in the year 2017 by Yang et al. [88]. The authors of this study only included homocysteine level in their meta-analysis and they found that a significantly higher mean log plasma tHcy level was found in the mothers of NTD affected offspring (log WMD: 0.06; 95%CI: 0.02–0.09, p= 0.001). The present meta-analysis included the larger number of studies with large sample size and results also supports the finding of the previous two studies.
The main strength of our meta-analysis is (i) we included largest sample sizes and also largest number of studies, (ii) we included three parameters viz. homocysteine, s-folate, and cobalamin, (iii) we found no publication bias in our study. Here we also want to acknowledge some of the limitations of our meta-analysis such as-(i) use of unadjusted weighted mean difference, (ii) not considered the environmental effect on the metabolites, and (iii) high heterogeneity between studies.
CONCLUSION
In conclusion, the meat-analysis reveals the role of different biomarkers for the early prediction of the neural tube defects. Also, this study strengths the hypothesis that the elevation in the level of homocysteine or depletion in the level of folate or cobalamin during the pregnancy will increases the chances of an NTD affected offspring.
Data Availability
All the data are provided in the manuscript.
FUNDING
There was no funding for this review.
ETHICAL APPROVAL
The article does not contain any studies with human or animal subjects performed by any of the authors.
ACKNOWLEDGMENTS
Upendra Yadav is highly grateful to VBS Purvanchal University, Jaunpur for providing financial assistance to him in the form of PDF.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.
- 13.↵
- 14.↵
- 15.
- 16.↵
- 17.↵
- 18.
- 19.
- 20.↵
- 21.↵
- 22.↵
- 23.
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.
- 37.
- 38.
- 39.↵
- 40.↵
- 41.↵
- 42.
- 43.↵
- 44.
- 45.↵
- 46.
- 47.↵
- 48.
- 49.↵
- 50.
- 51.
- 52.
- 53.
- 54.↵
- 55.↵
- 56.
- 57.
- 58.↵
- 59.↵
- 60.
- 61.↵
- 62.↵
- 63.
- 64.↵
- 65.
- 66.
- 67.
- 68.↵
- 69.↵
- 70.↵
- 71.
- 72.
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵




