
Abstract
BACKGROUND Laparoscopy-assisted trans-anal TME (ta-TME), or hybrid ta-TME, inherited the advantages of both trans-anal surgery and trans-abdominal surgery, and is gaining increasing acceptance from colorectal surgeons worldwide. This research aims to make a comprehensive comparison between hybrid ta-TME surgery and traditional laparoscopic TME (la-TME) surgery regarding surgical quality and long-term survival.
METHODS Cochrane Library, EMbase, Web of Science and PubMed were searched for studies comparing hybrid ta-TME with traditional la-TME. Indicators for surgical quality and long-term prognosis were extracted and pooled. Heterogeneity was assessed with I2 index and was significant when p < 0.1 and I2 > 50%. Publication bias was estimated by Egger’s test, where p<0.1 was considered statistically significant.
RESULTS 13 studies with 992 patients were included in meta-analysis, of which 467 were in hybrid ta-TME cohorts, and 525 were in traditional la-TME cohorts. Compared with traditional la-TME, hybrid ta-TME has lower rate of positive circumferential margin (RR=0.454, 95%CI 0.240~0.862, p=0.016) and lower conversion rate (RR=0.336, 95%CI 0.134~0.844, p=0.020). On rate of positive distal resection margin, completeness/near-completeness of meso-rectum, overall complications, anal leakage, ileus, urinary dysfunction, 2-year DFS and 2-year OS, there were no significant difference between the two techniques.
CONCLUSIONS Hybrid ta-TME is significantly superior to traditional la-TME in ensuring CRM safety and lowering intra-operative conversion rate, and is meanwhile not inferior on other major outcome indicators concerning surgical quality and long-term survival. To further understand this new surgical technique, we need high-quality RCTs, as well as previous researchers’ updates with results of prolonged follow-up.
1. Introduction
Total meso-rectal excision (TME) is the golden standard for the surgical treatment of middle and distal rectal cancer [1]. In 2016, NCCN Practice Guidelines in Oncology: Rectal Cancer made conditional recommendations on the application of laparoscopic surgeries [2], balancing the need for both radical resection and micro-invasiveness. However, for patients with obesity, extra-large tumors, narrow pelvis, male gender or history of neoadjuvant radiotherapy, laparoscopic TME (la-TME) can be particularly difficult to operate, thus undermining the quality of resected specimen. Whereas TME specimen with incomplete meso-rectum, positive circumferential resection margin (CRM), narrow distal resection margin (DRM) or ruptured intestinal wall will naturally increase the risk of local recurrence [3].
With the evolution of concepts and techniques, existing issues in the traditional laparoscopic approach for rectal cancer resection, particularly concerns over the quality of specimen [4], are currently raising increasing awareness. In 2010, Sylla and Atallah respectively reported a radically resected case that were operated trans-anally with the assistance of laparoscopy [5–6], both of which were successful, bringing forward the notion of trans-anal total meso-rectal resection (ta-TME). In pure-NOTES hybrid ta-TME, the operator will have to dissociate around the tumor before prospecting the abdominal cavity, which clearly violated the basic principle for resecting malignant tumors and was thus limited in its application [7]. Hybrid ta-TME, or laparoscopy-assisted hybrid ta-TME, inherited the advantages of both trans-anal surgery and trans-abdominal surgery, and is gaining increasing acceptance from colorectal surgeons worldwide.
To make a comprehensive comparison of surgical quality and long-term survival between traditional laparoscopic TME (la-TME) surgery and hybrid (laparoscopy-assisted) trans-anal TME surgery, key indicators were extracted from relevant studies and pooled for further analysis.
2. Methods
2.1. Literature search strategy
Protocol of this research was registered with PROSPERO (CRD42020169185). Cochrane Library, EMbase, Web of Science and PubMed were searched for relevant studies published during 2010.1 ~2020.1. Search strategy was adopted as: RECTAL and CANCER or NEOPLASM and TRANSANAL and LAPAROSCOPIC and TOTAL MESORECTAL EXCISION or TME or TA-TME. Each of the literature screening processes was conducted by two researchers, where disputes were settled by consultation with a third senior researcher.
2.2. Inclusion and exclusion criteria
Inclusion criteria: studies focusing on rectal cancer patients receiving surgical treatment; with two comparing cohorts (i.e. patients receiving hybrid ta-TME surgeries, and patients receiving la-TME surgeries); language was restricted to English only.
Exclusion criteria: ta-TME cohort contains patients receiving pure-NOTES ta-TME surgeries (i.e. without trans-abdominal procedure at all); ambiguous about whether or not its ta-TME cohort included patients receiving pure-NOTES ta-TME surgeries.
Additionally, studies where ta-TME cohort has excessively long duration of surgery (over 300 minutes, mean or median) were also excluded, as insufficient surgical skillfulness of the new technique might confound the pooled result and bring unnecessary heterogeneity.
2.3. Quality evaluation and data extraction
Articles included in this research were all non-randomized controlled trials (non-RCTs). Therefore Newcastle Ottawa Scale (NOS) was adopted for quality evaluation [8].
Items collected from literatures include: author; year of publication; gender ratio; age; BMI; neo-adjuvant therapy (Y/N); ratio of LAR (low anterior resection) procedure; duration of surgery; incidence of CRM+, DRM+, completeness/near-completeness of mesorectum, overall complications, anal leakage, ileus, urinary dysfunction, conversion to open surgery, re-operation, 2-year disease free survival (DFS) and 2-year overall survival (OS).
2.4. Statistics
Statistical analyses in this research included pooling of outcomes, test of heterogeneity and assessment of publication bias. Pooled analysis was conducted for each selected outcome indicator. All indicators were dichotomous data, therefore relative risk with corresponding 95% confidence interval were calculated. Heterogeneity was assessed with I2 index, where p < 0.1 and I2 > 50% was considered significant and a random-effect model (Inverse Variance) was thus adopted; otherwise a fixed-effect model (Mantel-Haenszel) was used [9, 10]. Exclusion of a study due to significant heterogeneity was forbidden, so as to display a comprehensive analysis result that was true to the study screening mechanism. Publication bias was estimated by Egger’s test, and was considered significant when p<0.1 [11, 12]. All analysis was processed on STATA software, version 15.0 (StataCorp LP, College Station, TX, USA). Initial results were further validated with MedCalc, version 19.1.3 (MedCalc Software, Ostend, Belgium).
3. Results
3.1. Search results
13 cohort studies [13–25] were included based on the above selection mechanism. 9 out of the 13 were matched case-control studies (propensity score matching on a 1:1 basis). Literature selection process is demonstrated in Figure 1. Characteristics of included studies and patients were displayed in Table 1.

Flowchart of the literature screening process.
Characteristics of included studies
3.2. Meta-analysis result
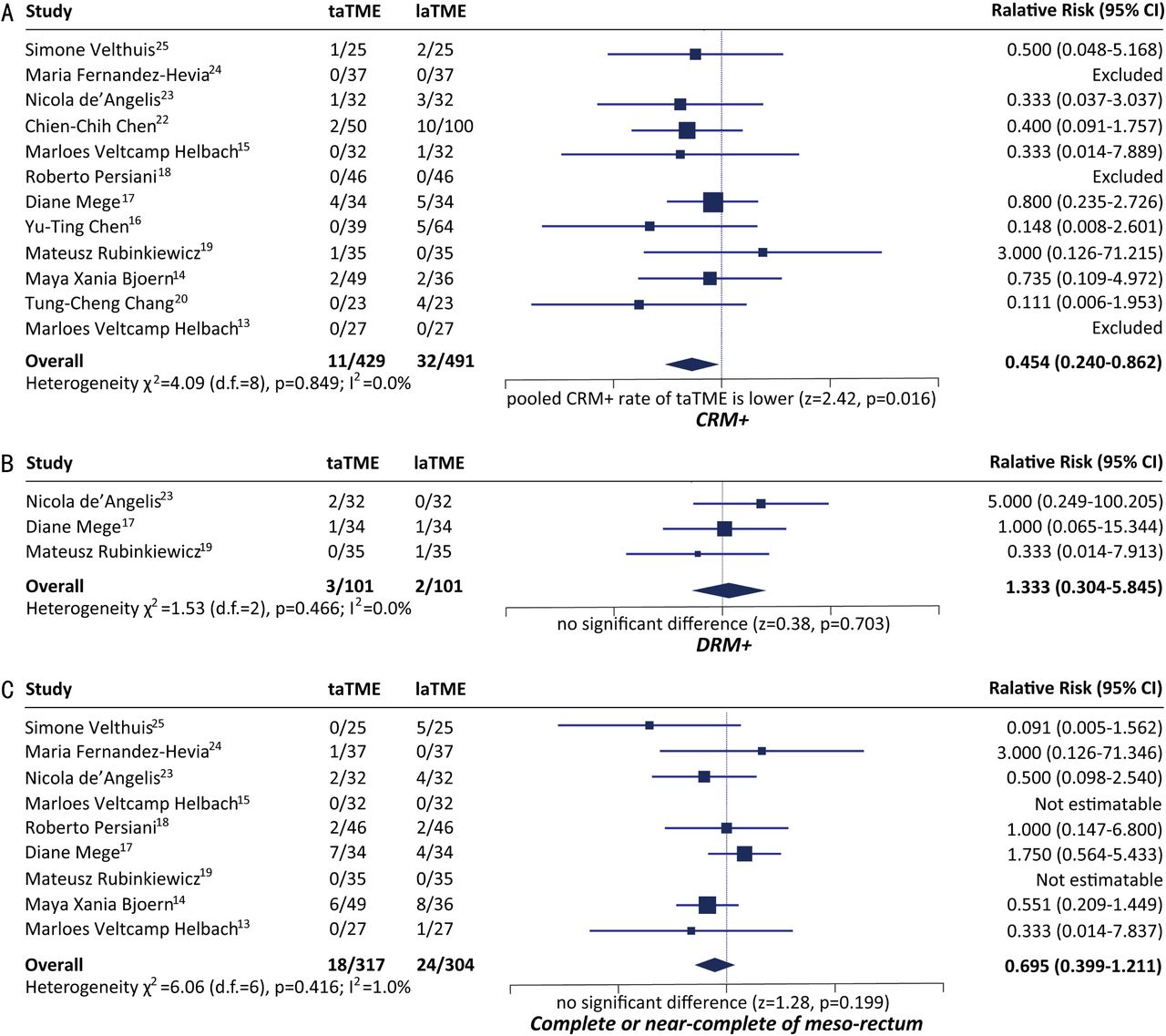
3.2.1. Quality of resected specimen
CRM+
12 studies compared the rate of CRM+ between hybrid ta-TME and traditional laparoscopic TME. Pooled rate of CRM+ of hybrid ta-TME is significantly lower than that of traditional laparoscopic TME (Relative Risk=0.454, 95%CI 0.240~0.862, p=0.016) (Figure 2). Analysis was conducted with a fixed-effect model as no significant heterogeneity was observed (p=0.849, I2= 0.0%). Egger’s test for publication bias is negative (p=0.509).

Comparison of quality of resected specimen.
DRM+
3 studies compared the rate of DRM+ between hybrid ta-TME and traditional laparoscopic TME, and pooled result indicated no significant difference between the two techniques (Relative Risk=1.333, 95%CI 0.304~5.845, p=0.703) (Figure 2). Analysis was conducted with a fixed-effect model as no significant heterogeneity was observed (p=0.466, I2 = 0.0%). Egger’s test was infeasible due to insufficiency of studies.
Integrity of mesorectum
9 studies compared the complete/near-complete rate of meso-rectum between hybrid ta-TME and traditional laparoscopic TME, and pooled result indicated no significant difference between the two techniques (Relative Risk=0.695, 95%CI 0.399~1.211, p=0.199) (Figure 2). Analysis was conducted with a fixed-effect model as no significant heterogeneity was observed (p=0.416, I2= 1.0%). Egger’s test for publication bias is negative (p=0.934).
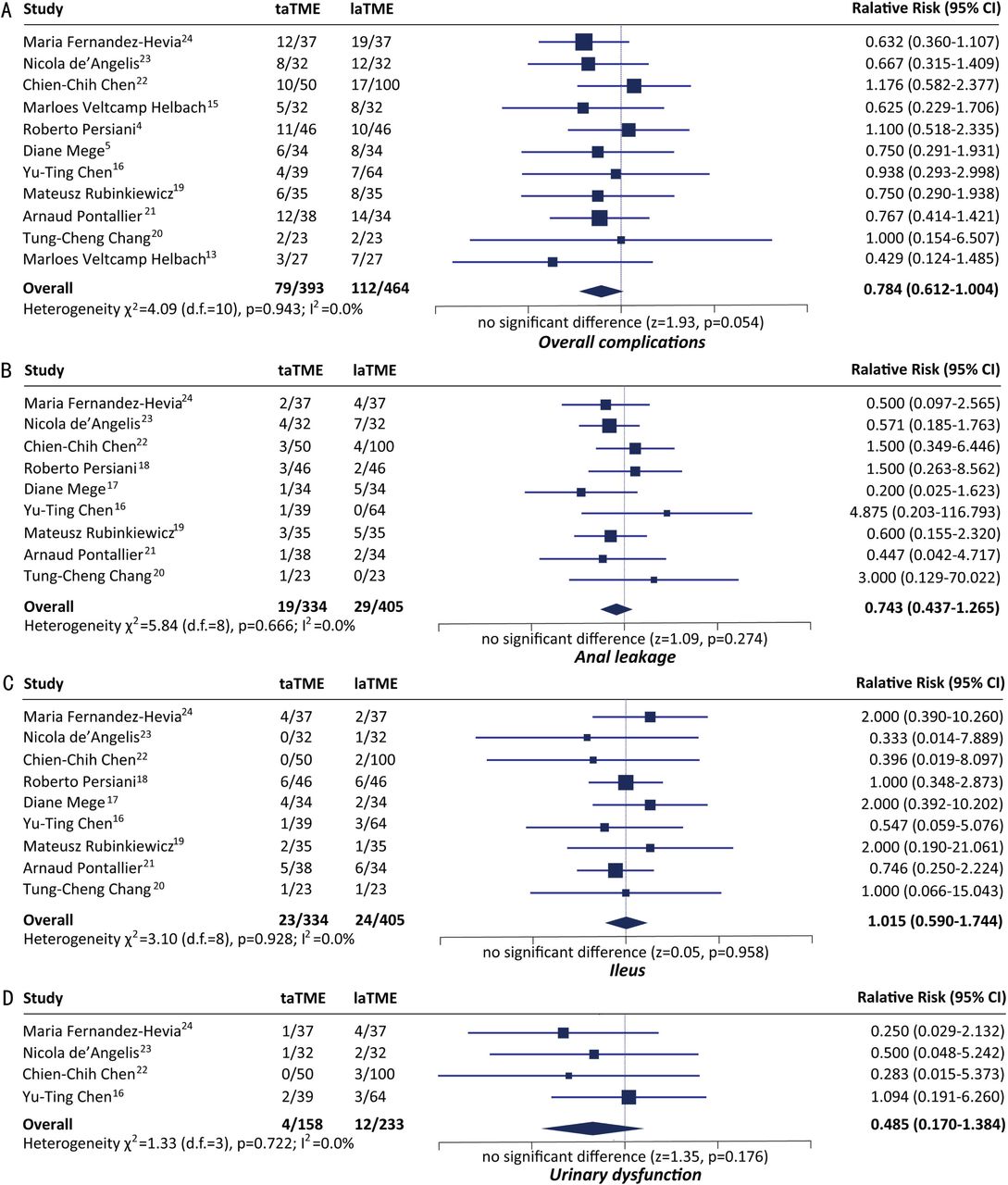
3.2.2. Post-operative complications
Overall complications
11 studies compared the incidence rate of overall post-operative complications between hybrid ta-TME and traditional laparoscopic TME, and pooled result indicated no significant difference between the two techniques (Relative Risk=0.784, 95%CI 0.612~1.004, p=0.054) (Figure 3). Analysis was conducted with a fixed-effect model as no significant heterogeneity was observed (p=0.943, I2= 0.0%). Egger’s test for publication bias is negative (p=0.510).

Comparison of incidence of post-operative complications.
Anal leakage
9 studies compared the incidence rate of post-operative anal leakage between hybrid ta-TME and traditional laparoscopic TME, and pooled result indicated no significant difference between the two techniques (Relative Risk=0.743, 95%CI 0.437~1.265, p=0.274) (Figure 3). Analysis was conducted with a fixed-effect model as no significant heterogeneity was observed (p=0.666, I2 =0.0%). Egger’s test for publication bias is negative (p=0.485).
Ileus
9 studies compared the incidence rate of post-operative ileus between hybrid ta-TME and traditional laparoscopic TME, and pooled result indicated no significant difference between the two techniques (Relative Risk=1.015, 95%CI 0.590~1.744, p=0.958) (Figure 3). Analysis was conducted with a fixed-effect model as no significant heterogeneity was observed (p=0.928, I2 =0.0%). Egger’s test for publication bias is negative (p=0.556).
Urinary dysfunction
4 studies compared the incidence rate of post-operative urinary dysfunction between hybrid ta-TME and traditional laparoscopic TME, and pooled result indicated no significant difference between the two techniques (Relative Risk=0.485, 95%CI 0.170~1.384, p=0.176) (Figure 3). Analysis was conducted with a fixed-effect model as no significant heterogeneity was observed (p=0.722, I2 =0.0%). Egger’s test for publication bias is negative (p=0.463).
3.2.3. Unplanned surgical events
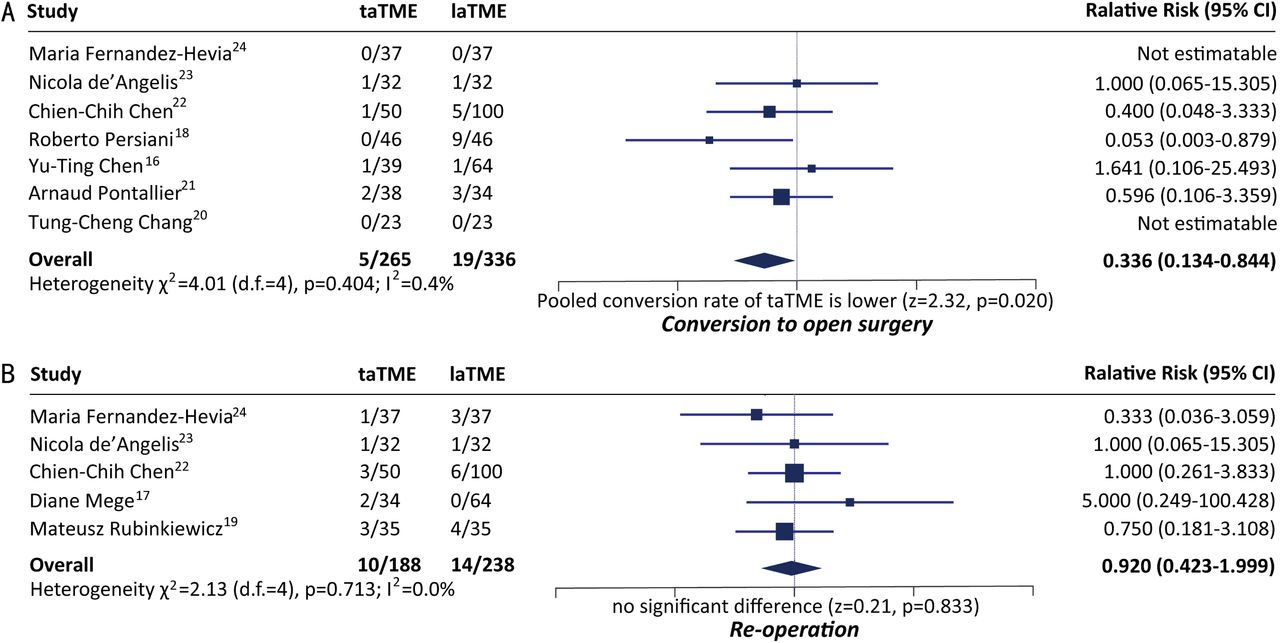
Conversion to open surgery
7 studies compared the conversion rate between hybrid ta-TME and traditional laparoscopic TME. Pooled conversion rate of hybrid ta-TME is significantly lower than that of traditional laparoscopic TME (Relative Risk=0.336, 95%CI 0.134~0.844, p=0.020) (Figure 4). Analysis was conducted with a fixed-effect model as no significant heterogeneity was observed (p=0.404, I2=0.4%). Egger’s test for publication bias is negative (p=0.243).
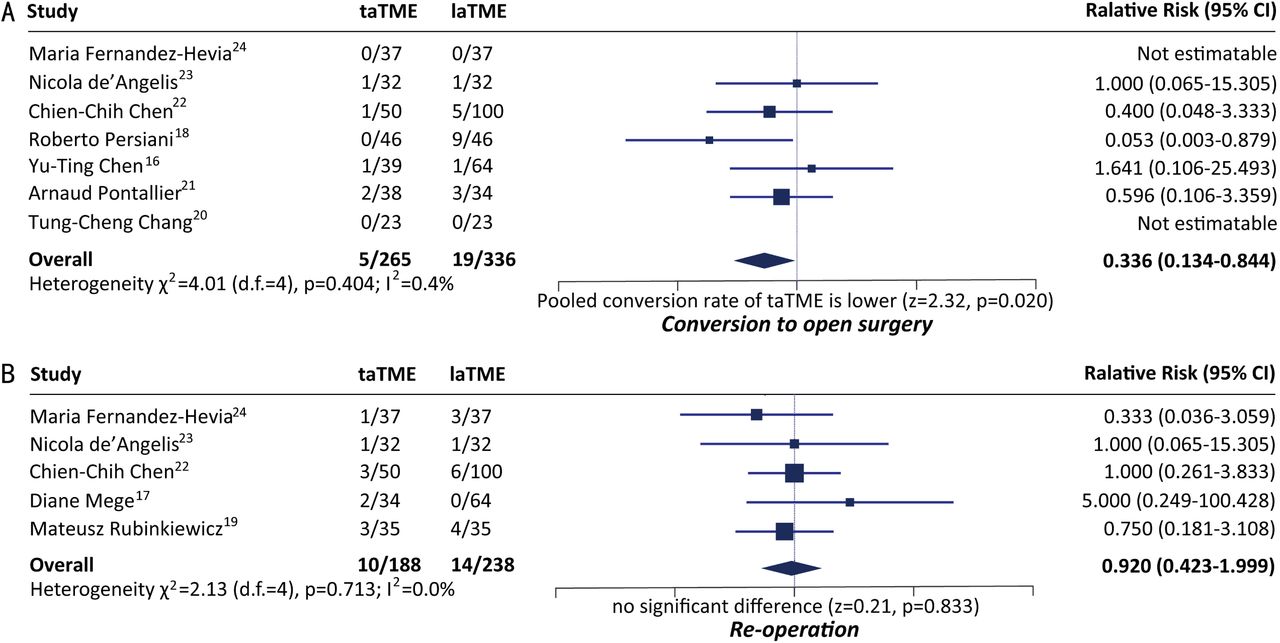
Comparison of incidence of unplanned surgical events.
Re-operation
5 studies compared the incidence rate of unplanned re-operation between hybrid ta-TME and traditional laparoscopic TME, and pooled result indicated no significant difference between the two techniques (Relative Risk=0.920, 95%CI 0.423~1.999, p=0.833) (Figure 4). Analysis was conducted with a fixed-effect model as no significant heterogeneity was observed (p=0.713, I2=0.0%). Egger’s test for publication bias is negative (p=0.577).
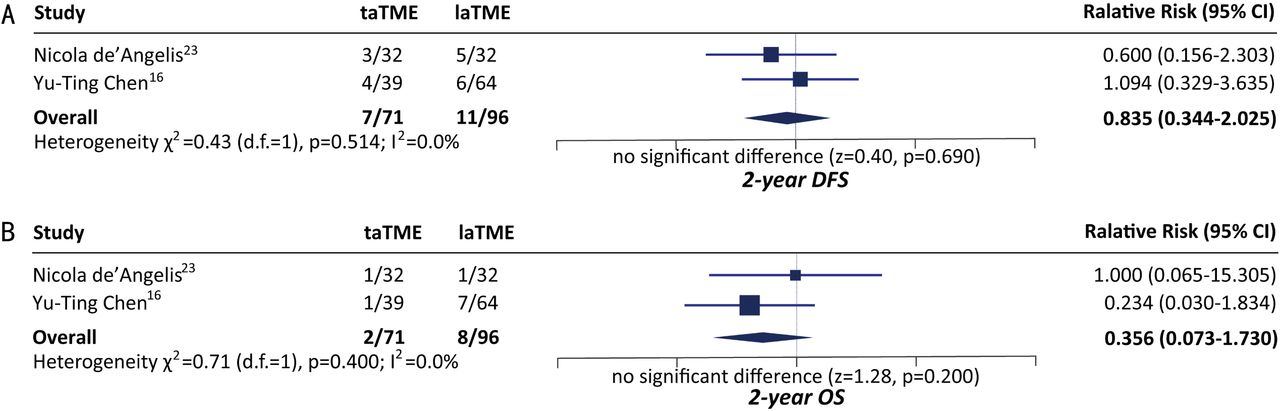
3.2.4. Long-term oncological outcome
Two-year DFS.
2 studies compared the two-year DFS between hybrid ta-TME and traditional laparoscopic TME, and pooled result indicated no significant difference between the two techniques (Relative Risk=1.017, 95%CI 0.914~1. 131, p=0.757) (Figure 5). Analysis was conducted with a fixed-effect model as no significant heterogeneity was observed (p=0.530, I2 =0.0%). Egger’s test was infeasible due to insufficiency of studies.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of long-term survival.
Two-year OS
2 studies compared two-year OS between hybrid ta-TME and traditional laparoscopic TME, and pooled result indicated no significant difference between the two techniques (Relative Risk=1.048, 95%CI 0.974~1.127, p=0.211) (Figure 5). Analysis was conducted with a fixed-effect model as no significant heterogeneity was observed (p=0.170, I2 =46.8%). Egger’s test was infeasible due to insufficiency of studies.
4. Discussion
As indicated by the results of meta-analysis, pooled CRM+ rate of hybrid ta-TME is significantly lower than that of la-TME, which is in accordance with our empirical understanding that ta-TME better ensures the safety of circumferential resection margin. However, no significant differences were observed on rate of DRM+, as well as rate of completeness/near-completeness of mesorectum. Regarding overall post-operative complications, post-operative ileus, post-operative anal leakage and post-operative urinary dysfunction, there are no significant differences between hybrid ta-TME and traditional la-TME. Yet it’s worth mentioning that among these four indicators, the difference on rate of overall complications is close to reaching significance (p=0.054). As to unplanned surgical events, the pooled conversion rate (ratio of cases converted to open surgery) of hybrid ta-TME is significantly lower than that of la-TME, indicating ta-TME’s distinct advantages in handling complex surgical scenarios over la-TME. Nonetheless, no significant difference was observed on rate of re-operation, suggesting that there was no significant difference between hybrid ta-TME and traditional la-TME on severe post-operative complications. Last but not the least, as the primary concern of clinical physicians, difference on 2-year DFS and 2-year OS between the two surgical strategies were insignificant. Notably, significant heterogeneity and publication bias were observed in pooling of none of the above indicators, indicating good credibility of the results (Table 2).
A summary of pooled analysis results
Quality of TME surgeries depends heavily on the integrity of resected mesorectum [26], and rectal surgery’s higher demand on intra-operative visual field and quality of specimen prompted the rapid development of ta-TME [27]. The trans-anal procedure started directly from the otherwise most difficult part of TME surgeries, providing clearer field of view and broader space to maneuver. Operating trans-anally can ensure sufficient length of distal margin and guarantee the effectiveness of the radical resection, meanwhile increase the anus-preserving rate of patients with low or ultra-low rectal cancers. This down-to-up strategy allows, even on male patients with narrow pelvis, for easy dissociation along the Denonvilliers fascia after cutting open the rectal wall, decreasing the risks of injuring prostate gland, seminal vesicle, posterior wall of vagina, and pelvic plexus. Hybrid ta-TME, as the combination of trans-abdominal surgery and trans-anal surgery, inherited the advantages of both. In a regular hybrid ta-TME surgery, laparoscopic team prospects the abdominal cavity, ligatures blood vessels, dissect lymph nodes and dissociate the proximal and middle mesorectum; and the trans-anal team dissociate distal mesorectum and retract specimen via natural orifice.
Compared with traditional laparoscopic TME surgeries, hybrid ta-TME significantly decreased the difficulty in a series of surgical actions, including exposing in pelvic bottom, ensuring completeness of resected meso-rectum, anticipating distal resection margin and severing rectum [28–30]. From an empirical point of view, we believe hybrid ta-TME is advantageous over traditional laparoscopic TME primarily in 5 aspects: (1) can accurately sever distal rectum from within rectal cavity, better ensuring the safety of distal resection margin; (2) enters the interstices around distal meso-rectum more conveniently, increasing the safety of circumferential resection margin; (3) does not require an extra incision on the abdomen for specimen retraction, contributing to the idea of micro-invasiveness; (4) reduces usage of anastomosis devices and alleviate patients’ costs; (5) avoids multiple triggering of linear stapling devices, potentially lowering risk of anal leakage [31–33]. The advantages described in (3) and (4) were obvious and need no further explanations. And as results of our meta-analysis indicated, pooled rate of CRM+ of hybrid ta-TME is significantly lower than that of traditional laparoscopic TME (Relative Risk=0.454, 95%CI 0.240~0.862, p=0.016), supporting our empirical statement in (2). However, statements in (1) and (5) were not supported by the pooled results, which may need higher-level evidences from further research.
Nevertheless, hybrid ta-TME surgery also has apparent flaws: (1) trans-anal procedures are time-consuming, and requires abundant experiences of single-port laparoscopic surgeries, dictating a prolonged learning curve; (2) operating trans-anally can obviously increase the risks of pelvic and abdominal infection; (3) when operating trans-anally, judgement on the location of the end of meso-rectum is very difficult to make [34], which may cause, precisely opposite to the original purpose of ta-TME, incomplete resection of meso-rectum. Naturally, towards a new technique, there will be constant doubts and questioning. However, there will never be a perfect technique that befit all patients. Only by actively selecting the most suitable patients and determining the optimal indications for ta-TME can we maximize its efficacy. Currently, existing studies on ta-TME technique are mostly retrospective studies with small-sized samples. In 2015, an international, multi-centered, prospective, random controlled trial code-named COLOR was initiated by researchers from Netherland. COLOR aimed to include 1098 mid and lower rectal cancer patients from around the globe to compare the safety and efficacy of ta-TME and traditional laparoscopic TME [35]. As a participating center of COLOR, our hospital founded the Steering Committee of COLOR Trial in China so as to provide appropriate assistance to interested centers across China. Meanwhile, we had established the national ta-TME database of China, which has now registered over 1000 ta-TME cases from 40 domestic centers, hoping to provide more higher-level evidence for the development of ta-TME technique.
In conclusion, hybrid ta-TME is significantly superior to traditional la-TME in ensuring CRM safety and lowering intra-operative conversion rate. But as to the rate of DRM+, completeness/near-completeness of meso-rectum, overall complications, anal leakage, ileus, urinary dysfunction, 2-year DFS and 2-year OS, there are no significant difference between the two TME techniques. To further understand this novel surgical strategy, we need high-quality RCTs, as well as previous researchers’ updates with results of prolonged follow-up.
Data Availability
All research data are available via reasonable request by email to corresponding author.
Footnotes
Acknowledgement: This work was funded by Beijing Municipal Education Commission (IDHT20170516).
Conflict of interests: none.
Referrences




