
Abstract
Background Drug resistance tuberculosis (DR-TB) continues to be a major public health threat globally. Due to the development of many rapid molecular diagnostic tools to detect gene mutations in M.tuberculosis (Mtb), specific genes conferring resistance to different anti-TB drugs have been identified. The aim of this meta-analysis was to assess the prevalence of the gene mutations associated with rifampicin (RIF) and isoniazid (INH) resistant Mtb in Ethiopia.
Methods Using PRISMA guideline, we systematically searched a literature on PubMed/MEDLINE, Web of Science, Scopus electronic databases, Cochrane library, and other database sources. The data analysis was done using STATA 11. The pooled prevalence of the gene mutations associated with resistance to RIF and INH were estimated using the random effect model. Heterogeneity was measured by the I2 statistical test, and the publication bias through the funnel plot and the Egger’s regression test.
Results Among all antimycobacterial resistance tested TB patients, prevalence of resistance to any anti-TB drug was 31.3%, while multidrug resistance TB (MDR-TB), any RIF and INH resistance were 22.2%, 24.9%, and 27.9%, respectively. In total, 909 (95.8%) of 949 INH resistant Mtb isolates had detectable gene mutation in katG315 and 5.9% in the inhA gene. The meta-analysis derived an estimated pooled prevalence of katGMUT1(S315T1) in INH resistant Mtb was 89.18% (95%CI 81.94-96.43%), while a pooled inhAMUT1 (C15T) resistant Mtb prevalence was 77.48% (95% CI 57.84-97.13%). Besides, 769 (90.8%) of 847 RIF resistant strains had detectable rpoB gene mutation, commonly in rpoBMUT3(S531L) probe (550 cases). The meta-analysis resulting a pooled rpoBMUT3(S531L) resistant Mtb prevalence of 74.20 % (95%CI 66.39-82.00%).
Conclusions RIF resistant Mtb isolates were spread widely, mainly with S531L mutation. Similarly, INH resistant Mtb isolates were spread with S315T1 and C15T mutations. It is significant to detect S531L among RIF resistant and S315T1 and C15T mutations among INH resistant isolates as it may be a determinant for subsequent development of MDR-TB. Rapid diagnosis of RIF and INH resistant Mtb strains in TB patients would expedite modification of treatment regimens, and proper infection control interventions could be taken on time to reduce the risk of further development and transmission of MDR-TB.
Highlights Tuberculosis(TB), particularly drug resistance TB (DR-TB) continues to be a major public health threat globally. Herein, we used a systematic literature search on reliable electronic databases, and perform a meta-analysis to assess the prevalence of the gene mutations associated with rifampicin (RIF) and isoniazid (INH) resistant Mtb in Ethiopia. The meta-analysis derived an estimated pooled prevalence of katGMUT1 (S315T1) in INH resistant Mtb was 89.18% (95%CI 81.94-96.43%), while inhAMUT1(C15T) resistant Mtb prevalence was 77.48% (95% CI 57.84-97.13%). Besides, among 90.8% of RIF resistant strains which had detectable rpoB gene mutation, a pooled S531L resistant Mtb prevalence was 74.20% (95%CI 66.39-82.00%). This review revealed that the RIF resistant Mtb strains were spread widely, mainly with S531L mutation, while the INH resistant Mtb isolates were spread widely with S315T1 and C15T mutations. So, it is significant to detect S531L among RIF resistant and S315T1 and C15T mutations among INH resistant isolates as it may be a determinant for subsequent development of MDR-TB. Rapid diagnosis of RIF and INH resistant Mtb strains in TB patients would expedite alteration of treatment regimens, and proper infection control interventions could be taken on time to reduce the risk of further development and transmission of MDR-TB.
Background
Tuberculosis (TB) disease caused by Mtb bacilli, continues as major public health threat globally [1, 2]. Despite the “TB incidence and mortality declined over the past decades, there were still an estimated 10.0 million new cases of TB and approximately 1.45 million deaths attributed to TB worldwide in 2018” [1]. The emergency of antimycobacterial drug resistance is threatening the TB prevention and control activities, and it remains to be a major public health threat on global scale [2]. “In 2018, there were about half a million new cases of RIF resistant TB, of which 78% had MDR-TB” [1].
Anti-TB drug resistance in Mtb arises as a result of spontaneous gene mutations that reduce the bacterium resistant to the most commonly used anti-TB drugs. These genes can encode drug targets or drug metabolism mechanisms and influence the effectiveness of anti-TB treatments [1-5]. Inappropriate treatment and patient’s poor adherence to anti-TB drug treatments contribute to the development of drug resistant TB, while the lack of drug resistance diagnosis and subsequent improper TB patients treatment rise the risk of direct transmission of DR-TB [3, 4, 6].
Due to the lack of accurate, rapid, and inexpensive diagnostic tests, there is low drug resistance, including MDR-TB detection rates in resource limited countries. Sputum smear microscopy, the most frequently used diagnostic methods for the “detection of TB disease does not detect drug resistance” [1]. Mycobacterial culture on liquid or solid media, standard drug sensitivity testing (DST), can take longer time to obtain test results, initiate proper anti-TB drug treatment and it needs well-furnished laboratory settings and substantial biosafety resources. This is impracticable in many low resource settings [1, 2, 4, 7]. During the past decade, several molecular (genotypic) DST methods which can detect gene mutations that confer drug resistance have been developed, including line probe assays, real-time polymerase chain reaction (PCR), deoxyribonucleic acid (DNA) sequencing, DNA hybridization on designed chips, and pyrosequencing [3, 8-10]. In pursuance of these molecular diagnostic approaches to correctly identify all resistant Mtb, the genes and specific nucleotide change conferring antitubercular drug resistance should be known and included in the diagnostic test. However, “geographical frequency and global distribution of RIF and INH resistance associated Mtb gene mutations have not yet been thoroughly measured in the pathogen population” [11].
Several previous review reports have identified different genes that encode anti-TB drug targets and have briefed different mechanisms of resistance to both RIF and INH [12-17]. More than 95% of RIF resistance is associated with the gene mutations in an 81 base pair section of the rpoB gene. The INH resistance appears more complex and has been associated with multiple genes, most commonly katG and at the promotor region of inhA gen [14, 17-21]. The current molecular diagnostic tests for INH resistance have focused on the detection of the “canonical” mutations in codon 315 of katG and position-15 in the inhA promoter region. Many earlier studies have identified highly variable frequencies of these mutations; with katG315 mutations accounting for 42 to 95% and inhA-15 mutations accounting for 6 to 43% of phenotypic INH resistance [3, 4, 12, 16, 17, 21-23]. The recent invention of “Xpert MTB/RIF” test [24] and the Line probe assays [25] “which span 81-base pair fragment of the ribonucleic acid (RNA) polymerase beta subunit (rpoB) gene have allowed for the rapid detection of resistance to RIF”.
To date there is no systematic review and meta-analysis that has assessed the most common gene mutations conferring RIF and INH resistance in Mtb in Ethiopia. Moreover, the pooled estimated prevalence of RIF resistance associated gene mutation, and the frequencies for co-occurring or multiple mutations have not been evaluated in order to understand the overall proportion of phenotypic INH and RIF resistance explained by the existing single or canonical gene mutations.
Hence, it is critically significant to understand the frequency and prevalence of drug resistance-conferring mutation associated with RIF and INH resistant Mtb in Ethiopia. “A failure to account for these variations limits the local effectiveness of molecular diagnostic tools currently available and constrains the development of improved genotypic diagnostic tests” [26]. Therefore, the aim of this meta-analysis was to estimate the frequency and prevalence of the most common gene mutations associated with phenotypic RIF and INH drug resistance in Mtb in Ethiopia based on the previously published literature’s data.
Methods
Study protocol
We strictly followed “the Preferred Reporting Items for Systematic review and Meta-analysis (PRISMA)” guideline [27] to searching records from the databases, paper screening by title, abstract, and evaluation of full text’s eligibility (Fig.1). The completed PRISMA checklist was provided as supplementary file (Table S1). This review protocol have submitted to the International Prospective Register of Systematic Reviews (PROSPERO) on May 2020, and assigned the submission identification number (ID# 186705).

PRISMA –adapted flow diagram showed the results of the search and reasons for exclusion of articles [27]
Databases and Search Strategy
The research papers published in English language were searched out on PubMed/MEDLINE, Web of Science, and Scopus electronic databases, Cochrane library and other database sources, without restricting the studies publication year. Research studies reported the gene mutations conferring RIF and INH resistance in Mtb in Ethiopia were included in the analysis. We used the following specific-subjects headings for databases searching: “Mycobacterium tuberculosis”, “tuberculosis”, “drug resistance”, “drug susceptibility testing”, “anti-tuberculosis drug resistance”, “antitubercular agents”, “first-line antitubercular drugs”, “isoniazid resistance tuberculosis”, “rifampicin resistance tuberculosis”, “gene mutations”, “drug resistance-conferring mutations”, “frequency of gene mutations”, “antitubercular drug resistance determinants”, “magnitudes of gene mutations”, “molecular diagnostics”, “molecular detection”, “molecular characterization”, “genotyping”, “line probe assay”, “GenoType®MTBDRplus assay”, “GeneXpertMTB/RIF assay”, “GenoType®MTBDRsl assay” and “Ethiopia”. The search strings were applied using “AND” and “OR” Boolean operators. The PubMed key search terms used were: (Mycobacterium tuberculosis [MeSH Terms] OR tuberculosis [MeSH Terms]) AND (INH OR isoniazid [MeSH Terms]) AND (RIF OR rifampicin [MeSH Terms]) AND (resistance OR resistant) AND (mutations [MeSH Terms]) OR sequence) AND Ethiopia. The full searching strategy detail for PubMed/MEDLINE database was provided as supplementary file (Table S2). Furthermore, we have reviewed the primary studies and review article’s reference lists to access potential studies and other grey literatures.
Screening and eligibility of studies
Papers retrieved from these databases were exported into the “EndNote reference software version 8.2 (Thomson Reuters, Stamford, CT, USA)”. Duplicate papers were sorted, noted and removed using the EndNote software. Some duplicated papers were identified manually due to the presence of difference in reference writing formats across the databases. Subsequently, two researchers (MAR and BA) independently evaluated the paper’s title and abstracts using the preset inclusion criteria. Two investigators (BA and BBA) also have independently collected full texts and assessed the eligibility of articles for final inclusion to the analysis. In each case, the discrepancies arose between two authors were resolved through discussion with the other authors to come into consensus.
Inclusion and Exclusion Criteria
All observational studies (cross-sectional, case-control, and cohort) which have diagnosed RIF and INH resistance in Mtb using standard World Health Organization (WHO) approved molecular DST tools, and had reported mechanisms of anti-tuberculosis drug resistance / or the gene mutations conferring RIF and INH resistance in Mtb in Ethiopia were included. Furthermore, studies addressing frequencies of the gene mutation, and some or all of the following criteria were included: (a) Studies reported data concerning the prevalence of antitubercular drug resistance among pulmonary and extra pulmonary TB patients (both retreated or newly diagnosed cases); (b) The prevalence of any ant-TB drug resistance or MDR-TB or extensive drug resistance TB (XDR-TB); (c) Studies which used standard WHO approved molecular anti-TB drug susceptibility diagnostic methods; (d) TB research conducted in Ethiopia and published in English language. We excluded those studies from the analysis with the following exclusion criteria: (a) the studies which were not reported mechanisms of ant-tuberculosis drug resistance/ or the gene mutations conferring RIF and INH resistance in Mtb; (b) The studies reported data on non-tuberculous mycobacterium; (c) Studies which did not assess DST of RIF and INH; (d) Studies performed anti-TB DST only through phenotypic methods. The editorial’s report, narrative review studies, case reports, and qualitative studies were excluded from the analysis. Additionally, we excluded citations without full text after contacting a study author twice through email.
Quality assessment
The critical quality assessment checklist recommended by the “Joanna Briggs Institute (JBI) was used to evaluate the quality of all included studies” [28]. The three investigators (MAR, BA and BBA) independently evaluate the quality of the full text articles. The discrepancy was resolved through discussion to reach on consciences, and to include articles to final analysis. The domain paper quality assessment criteria were; clear inclusion criteria, details of study subjects and the study settings, reliable/valid measurements for exposure, outcome variables and appropriate statistical analysis. Studies (case-control, cross-sectional and cohort) with the score of four and above were considered good quality and included, while the studies have the average score of three and below were considered as poor quality, and excluded (Table S3).
Data extraction
We used standard data extraction format prepared in Microsoft Excel sheet. Two authors (MAR and BA) independently extracted the following relevant information related to study characteristics (Autor/s’ name, publication year, study period, study region, type of TB patients, study design, molecular DST method/s, sample size, total positive cases, total Mtb isolates which DST was performed, frequency of any anti-TB drug resistance, any INH and RIF resistance and MDR-TB, and RIF and INH resistance mechanisms/frequency of gene mutations (rpoB, katG and inhA) and frequency of specific amino acid/nucleotide (codon) changes in each resistant gene loci/probe; at rpoB gene [rpoBMUT1 (D516V), rpoBMUT2A (H526Y), rpoBMUT2B (H526D), and rpoBMUT3 (S531L)], at katG gene [katGMUT1 (S315T1) and katGMUT2 (S315T2)], at inhA [inhAMUT1 (C15T), inhAMUT2 (A16G), inhAMUT3A (T8C), and inhAMUT3B (T8A)]. Furthermore, the absence of wild-type probe at each gene loci (rpoBWT1-8, katGWT1 and inhAWT1&2) were evaluated (Table 1 and Table S4).
Characteristics of included studies.
Outcome of interest
This systematic review and meta-analysis had estimated the pooled prevalence of gene mutations conferring RIF and INH resistance in Mtb in Ethiopia. Frequency of any anti-tuberculosis drug resistance, and resistance to any INH and RIF were drawn from each included study. The frequency of each resistant gene mutations were counted out of the total resistant Mtb isolates for a particular anti-TB drugs. Similarly, the rate of each amino acid/ or nucleotide (codon) changes at each resistant gene locus/probe (rpoB, katG and inhA) was calculated out of the total resistant gene. The pooled estimate of the prevalence of amino acid/ or nucleotide (codon) changes at each resistant gene loci/probe: rpoB gene [rpoBMUT1 (D516V), rpoBMUT2A (H526Y), rpoBMUT2B (H526D) and rpoBMUT3 (S531L)], at katG gene [katGMUT1 (S315T1) and katGMUT2 (S315T2)], at inhA [inhAMUT1 (C15T), inhAMUT2 (A16G), inhAMUT3A (T8C) and inhAMUT3B (T8A)] were measured. We have also estimated the pooled prevalence of gene mutations/the absence of band at each wild-type probe of rpoB gene (rpoBWT1-8), katG gene (katGWT), inhA gene (inhAWT1 and inhAWT2)(Table S4).
Data processing and statistical analysis
The relevant data were extracted from the included studies using standard format prepared in Microsoft Excel sheet and the data were exported into STATA 11.0 for further analysis. Using the binomial distribution formula, Standard error was calculated for each study. “Considering variation in true effect sizes across population, Der Simonian and Laird’s random effects model was performed for the analyses at 95% confidence level”. The heterogeneity of studies was determined using Cochrane’s Q statistics (Chi-square), invers variance (I2) and p-values. Publication bias across the studies was measured through the Egger’s regression test [29], and displayed with funnel plots of standard error of Logit event rate. A p-value less than 0.05 was considered statistically significant.
Results
Search results
As illustrated in figure 1, a total of 960 potential research studies were documented from searched electronic databases and other data sources. Of the total, 760 articles were non-duplicated and subjected for further evaluation; 452 were evaluated and excluded based on their title and abstract, while 308 papers were retained for full-text article review. After full-text article evaluation, 19 studies on the prevalence of gene mutations associated with RIF and INH resistant Mtb in Ethiopia were used for final analysis (meta-analysis).
Characteristics of included studies
As described in Table 1 and Table S4, a total of 19 studies with 5,057 TB patients (3504 culture, line probe assay and/or GeneXpertMTB/RIF assay positive Mtb isolates) were included for final analysis [30-48]. Five studies were from Addis Ababa [30, 38, 40, 41, 48], Amhara region [31, 35, 36, 42, 45], and Oromia region [32, 39, 43, 44, 47], respectively, while two studies were from South Nation Nationality and People [34, 46], and one studies from Somalia region [37]. In study design, fourteen studies were cross-sectional [30-38, 41, 42, 44, 45, 48], while five studies [39, 40, 43, 46, 47] have not stated the study design. Nineteen studies, of which eight studies [30, 32, 37-39, 44, 45, 47] have assessed RIF and INH resistance rate among pulmonary TB (PTB) patients, five studies [34-36, 43, 48] have assessed among extra pulmonary TB (EPTB) patients, while three studies [31, 33, 46] have done on both EPTB and PTB patients. GenoType®MTBDRplus assay and GeneXpertMTB/RIF assay were the most common molecular
/genotypic DST methods used [30-33, 35-48]. The resistance rate of Mtb to any ant-TB drugs, MDR-TB, and resistance to RIF and INH was calculated out of a total of 3406 Mtb isolates which their DST was performed [30-48]. In total, 17 studies evaluated the prevalence of any INH resistance [30-34, 36-42, 44-48], and any RIF resistance [30-33, 35-46, 48] among 3406 TB patients. Almost all included studies [30-33, 35-48], except one study had reported the prevalence of MDR-TB strains. All included studies [30-46, 48] had reported the gene mutations associated with resistance to RIF and INH. Moreover, seventeen studies [30-33, 35-46, 48] had quantified the frequency of rpoB gene mutation and nucleotide (codon) changes in an 81-base pair β-subunit (rpoB) gene among 847 RIF resistant Mtb isolates, while sixteen studies [30-34, 36-42, 44-46, 48] had reported the frequency of katG gene mutation and nucleotide (codon) changes among 949 INH resistant Mtb isolates. Only ten studies [30-33, 37, 41, 42, 44, 45, 47] had reported the gene mutation in inhA promotor region, while four studies [30, 31, 41, 42] reported the co-occurrence of inhA and katG genes among INH resistant Mtb isolates.
Prevalence of any RIF and INH resistant M.tuberculosis
Overall, 5057 pooled TB suspected patients were tested by Line probe assays (GenoType®MTBDRplus v.2.0 and/or GenoType®MTBDRsl assays) and GeneXpertMTB/RIF assay to identify MDR-TB, RIF and INH resistance pattern [30-48]. Prevalence of any anti-TB drug resistance among all diagnosed TB patients was 31.3% (1066/3406), while the prevalence of any RIF and INH resistant Mtb were 24.9% (847/3406), and 27.9% (949/3406), respectively. Moreover, prevalence of MDR-TB was 22.2% (755/3406) (Fig.2 & Table S5). The prevalence of any anti-TB drug resistance rate varies across the studies and geographical locations of Ethiopia. From the included studies, seven studies had reported higher prevalence of any anti-TB drug resistance ranged from 18.0% to 73.6% [30, 31, 37, 40-42, 44]. The prevalence of any INH resistant Mtb ranged from 0.8% to 72.2%, while the prevalence of any RIF resistant Mtb ranged from 1.3% to 68.1% [30-33, 35-46, 48] (Table 1 and Table S5).

Frequency of RIF, INH resistance and the associated resistant gene mutations
The frequency of rpoB, katG, and inhA gene mutations
“The Line probe assay (GenoType®MTBDRplus assay) (Hain Life science GmbH, Nehren, Germany) strip contains seventeen probes, with amplification and hybridization controls to confirm the diagnostic procedure” [7]. To detect INH resistance, one probe covers the wild-type S315 region of katG gene, while the other two probes (katMUT1 and katGMUT2) are designed to evaluate the S315T (Ser→ Thr) nucleotide (codon) change/ or mutations. Moreover, at the inhA promoter region is included on the new strip and covers the regions from positions 15 to 16 for the inhAWT1 probe and position 8 for the inhAWT2 probe. In inhA, four mutations (C15T, A16G, T8C and T8A) can be targeted with the inhAMUT1, inhAMUT2, inhAMUT3A and inhAMUT3B probes. To detect RIF resistance, one probe covers the wild-type probes rpoBWT1 to rpoBWT8 (507-533) regions of rpoB gene, while the other four probes (rpoBMUT1, rpoBMUT2A, rpoBMUT2B, rpoBMUT3) are designed to identify the (D516V, H526Y, H526D, and S531L) nucleotide (codon) change/or mutations, respectively. The resistant Mtb strain is confirmed when there is absence of one or more wild-type band or probe/s or the presence/ staining of mutant probes (Fig. S1).
A total of 949 any INH resistant Mtb strains were identified by standard WHO approved molecular diagnostic methods, among which a higher proportion of mutation was detected in the katG gene (95.8%; 909/949) compared with the gene mutation in the inhA promoter region (5.9%; 56/949). In INH resistant Mtb strains, the most common mutations were observed in katGMUT1 probe (860 cases) and katWT probe (309 cases). In the inhA promoter region, the most frequent mutations were observed in inhAMUT1 probe (inhA C15T; 31 cases), inhAWT1 probe (15/16; 30 cases) and inhAWT2 probe (8; 23 cases), while the frequency of mutation in inhAMUT2 probe was (15/16; 10 cases). The frequency of mutations in the inhAMUT3A and MUT3B were (8; 8 cases), respectively. In this systematic review, a total of 34 Mtb strains had mutations in both katG and inhA promoter region. The other most frequently occurring mutations in INH resistant Mtb isolates, at the position 15 of the inhA promotor region, was identified in 3.3% (31/949) of phenotypically resistant isolates, and the mutation in the inhA promotor region at a position 8 was identified among 8 (0.8%) of phenotypically resistant strains (Table 1 and Table S5).
Besides, a total of 847 any RIF resistant Mtb strains were identified by either Line probe assay or GeneXpert®MTB/RIF assay, among which frequency of mutation in the rpoB gene was (90.8%; 769/847). In RIF resistant Mtb strains, the most common mutations were found in rpoBMUT3 (S531L) probe (550 cases), rpoBWT8 probe (224 cases), and rpoBWT7 probe (91 cases), while the other gene mutations were observed in rpoBMUT2A(H526Y) (68 cases), rpoBMUT2B (H526D)(40 cases), and rpoBMUT1 (D516V) (25 cases). Moreover, the gene mutations at the rpoBWT3 and rpoBWT4 were 43 and 46 cases, respectively. Besides, ten RIF resistant Mtb strains revealed that the rpoB gene mutation at (codon 447-452), while the other one strain had rpoB gene mutation at CAA/G→ UUA/G(Q513L) (Table 1 and Table S5).
Meta-analysis
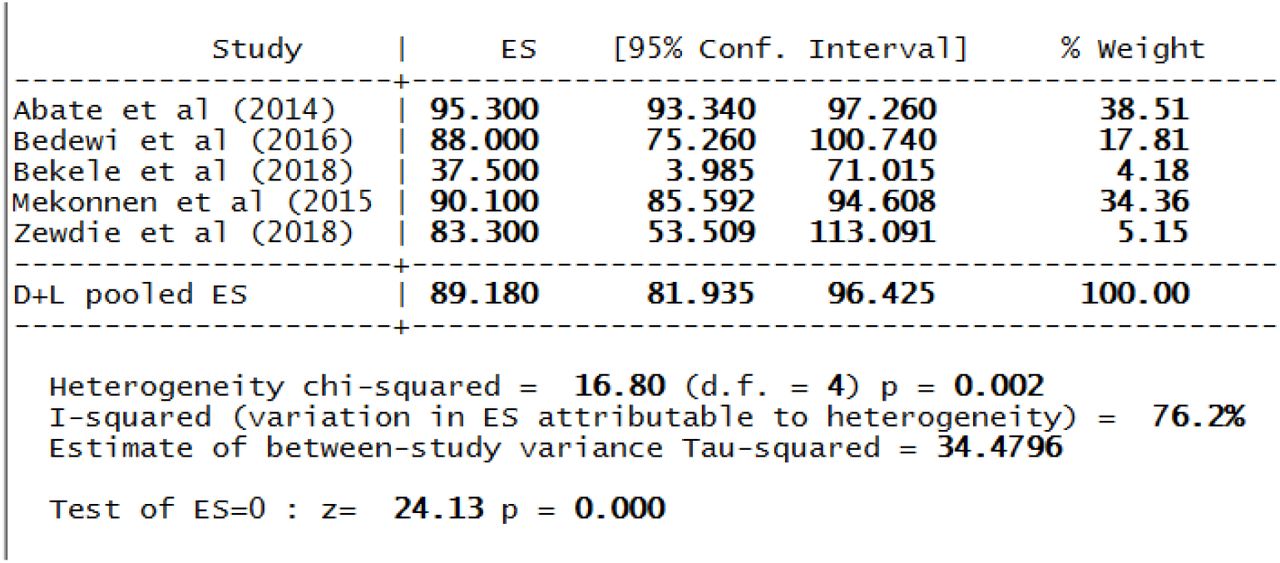
Nineteen studies, of which seventeen studies have evaluated 949 genotypically resistant Mtb isolates for mutations in katG gene inclusive of codon 315. In INH resistance, the increasing frequencies of co-occurring mutations were evaluated first by specific genes. This meta-analysis resulting a pooled katGMUT1 (S315T1) resistant Mtb prevalence of 89.18% (95% CI 81.94-96.43%) with a I2-value of 76.2% and p=0.002 (Fig.3 & Table 2). During our evaluation of publication bias, a funnel plot showed a symmetrical distribution, and the Egger’s regression test p-value was 0.071, which indicated the absence of publication bias (Fig. 4). However, this review derived low pooled prevalence of katGMUT2 (S315T2) resulting 0.91% (95% CI 0.195-1.63%) with I2-value of 0.0% and p=0.466 (Table 2). Besides, the pooled estimated prevalence of the absence of band at the wild-type (katGWT(315)) was 48.69% (95% CI -5.20-102.58%) with I2-value of 99.5% and p<0.001 (Table 2).

The pooled prevalence of katGMUT1 (S315T1) resistance among INH-resistant Mtb cases.

Funnel plot for publication bias, PREV (prevalence) represented in the x-axis and standard error (SE) of prevalence of katGMUT1 (S315T) in the y-axis
Results of mutations pattern of 949 any INH resistance tuberculosis patients.
The gene mutations at inhA promoter region were estimated, and the meta-analysis analysis derived a pooled inhAMUT1(C15T) resistant Mtb prevalence of 77.48% (95% CI 57.84-97.13%) with I2-value of 0.0% and p=0.848 (Fig.5 & Table 2). The publication bias was evaluated using the Egger’s regression test, and p-value was 0.460, which indicated the absence of publication bias. Similarly, the pooled estimated prevalence of the absence of band at wild-type inhAWT2(8) resistant Mtb was 20.65% (95%CI -5.36-46-66%) with I2-value of 0.0% and p= 0.594 (Table 2).
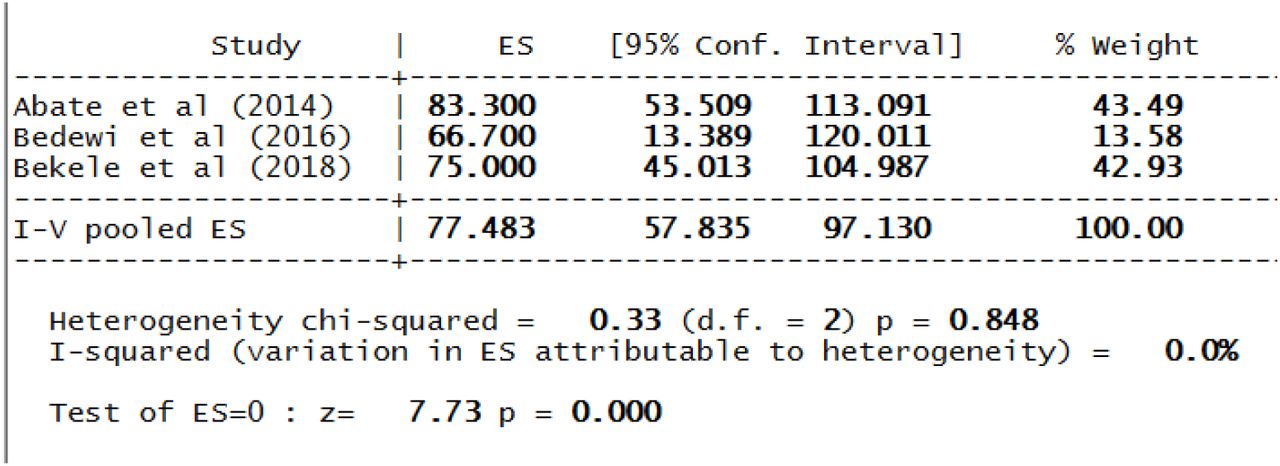
The pooled prevalence of inhAMUT1 (C15T) resistance among INH-resistant Mtb cases.
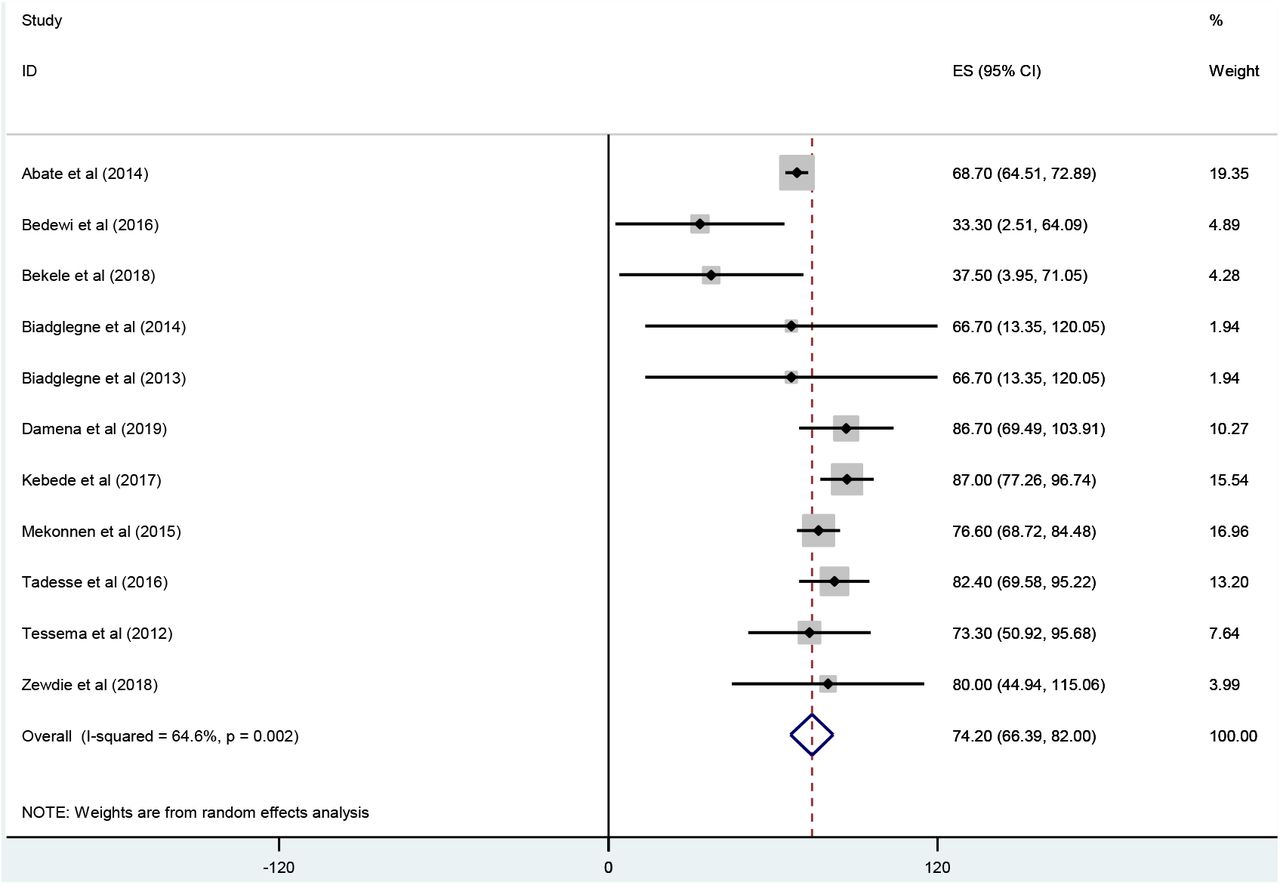
During our meta-analysis, seventeen publications evaluated 847 genotypically RIF resistant Mtb isolates for mutations in rpoB gene inclusive of an 81-base pair β-subunit ranged from codons 507-533, particularly, at codon 526, 526, and 531. Thus, the highest pooled estimated prevalence of the gene mutation associated with rpoB gene was observed in rpoBMUT3 (S531L), with 74.20 % (95% CI 66.39-82.00%) and the I2-value of 64.6% and p=0.002 (Fig 6 & Table 3). The publication bias was evaluated by using the Egger’s regression test revealed the p-value was 0.968 and a funnel plot showed a symmetrical distribution, which indicated the absence of publication bias (Fig.7). Moreover, the pooled prevalence of rpoBMUT2A (H526Y) was 17.20% (95% CI 8.25-26.15%) with I2-value of 85.7% and p<0.001 (Fig 8 & Table 3). During evaluation of publication bias, the funnel plot showed a symmetrical distribution; and the Egger’s test p-value was 0.107, which indicated there was no publication bias (Fig. 9). The analysis derived a pooled rpoBMUT2B(H526D) and rpoBMUT1(D516V) resistant Mtb prevalence of 13.91% and 2.96%, respectively. The absence of band at different rpoB gene wild type was assessed and the high pooled estimated pooled prevalence was observed in rpoBWT8 and rpoBWT3 with 58.21% and 19.92%, respectively (Table 3).
Results of mutations pattern of 847 any RIF resistance tuberculosis patients.

Forest plot showing the pooled prevalence of rpoBMUT3 (S531L) resistance among RIF-resistant Mtb cases.

Funnel plot for publication bias, PREV (prevalence) represented in the x-axis and standard error (SE) of prevalence of rpoBMUT3 (S531L) in the y-axis.

Forest plot showing the pooled prevalence of rpoBMUT2A (H526Y) resistance among RIF-resistant Mtb cases.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot for publication bias, PREV (prevalence) represented in the x-axis and standard error (SE) of prevalence of rpoBMUT2A (H526Y) in the y-axis
Discussion
The global TB control and prevention program is challenged due to the emergence of drug resistant bacilli [1, 2, 49], particularly due to the evolution of MDR-TB, resistance to both RIF and INH, the two “backbone” of the present recommended TB treatment [1, 3].
Isoniazid is a prodrug need to be converted into the active form by catalase-peroxidase enzyme encoded by the katG gene. After activation, “INH has an effect/inhibits the bacilli’s mycolic acid synthesis through the NADH-dependent enoyl-acyl carrier protein reductase, encoded by the inhA gene” [50, 51]. The molecular basis of INH resistance is arbitrated by mutations in the katG gene and inhA promotor region. The most frequent INH resistance mechanism has been identified as the katGS315T gene mutation, which results an inefficient INH-NAD product inhibiting the antimicrobial actions of INH. This mechanism is associated with high-level INH resistance in MDR-TB isolates. Besides, the gene mutation at the promotor region of inhA gene, the most frequent occurring at the position -15, result in an overexpression of inhA [52-55]. However, the frequency patterns of the most common gene mutations conferring INH resistance differ between individual genes. Recent studies revealed that, the majority (64%) of INH resistance in Mtb isolates is associated with a single gene mutation in katG315 [3, 52-55]. “The dominance of this mutation is hypothesized to be the result of a low or zero fitness cost for this mutation, allowing it to propagate without negative selection pressure” [3]. Other mutations in the katG gene, other than katG315 appear to occur at low (<1%) frequencies and devastatingly in combination with the katG315 gene mutation [3]. This systematic review and meta-analysis demonstrated that a prevalence of 95.8% for katG315 mutation and 5.9% for inhA promotor region gene mutation in patients with drug resistant Mtb, suggesting a major epidemic of DR-TB among these patients. Similarly, a study conducted by Campbell et al. in 212 INH-resistance in Mtb isolates estimated the global frequency of the katG315 gene mutation to be 85%, and 17% for inhA-15, while the cumulative frequency was 91% [56]. A recent study revealed that the estimated global frequencies of katG315 and inhA-15 was suggestively higher at 86% and 34, respectively [57]. In contrast, a meta-analysis conducted by Alagappan et al. revealed that the katG315 mutation was 71.0%, and 29.0% for inhA mutation [7]. This slight inconsistency may be due to the type of TB patients and kind of INH resistance, that Alagappan et al estimated these gene mutations among INH-monoresistance and PTB patients, while our review assessed the prevalence of these gene mutations among any INH resistance and all type of TB patients. However, a study carried out from California (USA), identified a worldwide frequency of 61% for katG315 mutation, and 23% for inhAMUT1(-15) mutation resembling the frequencies of these gene mutations as measured in this review [3].
Several previous studies have reported vastly variable frequencies of these mutations; with katG315 gene mutations accounting for 42 to 95% and mutation in the inhA-15 promotor region accounting for 6 to 43% of phenotypic INH resistance [12, 16, 17, 22, 23].
This meta-analysis resulting a pooled katGMUT1(S315T1) resistant Mtb prevalence of 89.18% (95% CI 81.94-96.43%), and prevalence of 0.91% (95% CI 0.195-1.63%) for katGMUT2 (S315T2) resistance gene. Besides, our review estimated the prevalence of inhAMUT1 (C15T) at inhA promotor region was 77.48% (95% CI 57.84-97.13%). Similarly, Alagappan et al. in 1150 INH-monoresistance Mtb isolates from India estimated the pooled prevalence of katGMUT1(S315T1) was 63.2%, while the prevalence of katGMUT2(S315T2) was 0.3% [7]. This analysis revealed a robust association between the percentage of INH resistance-conferring mutation due to katG (S315T) evaluated in clinical isolates and many different indicators of TB transmission intensity, supporting the suggestion that gene mutation at the 315-codon position of katG confer INH resistance in Mtb without reducing virulence or transmissibility.
Rifampicin is one of the utmost effective antitubercular drugs, since it has significant effect against actively metabolizing and slow metabolizing bacilli, making RIF a key component of the existing first line treatment option used to the treatment of drug sensitive TB (DS-TB) [16, 50, 51, 58]. The gene mutations associated with RIF resistance are well known and seem to occur in a single gene region of phenotypically RIF resistant Mtb isolates [7].
In Mtb, RIF binds to the β-subunit of the RNA polymerase, subsequently inhibiting the elongation of mRNA. RIF resistance in Mtb is mediated by the gene mutations clustered in codons 507-533 of the gene coding for the RNA polymerase β-subunit (rpoB) [49, 50].
Although, the gene mutations outside the RIF resistance-determining region (RRDR) have been reported in RIF resistant Mtb isolates [59], the 81-base pair β-subunit (rpoB) region is known as RRDR, which is the target of current genotypic/molecular based assays and accounts for 96% of RIF resistance. The amino acid or codons 531 and 526 comprise the most frequent gene mutations associated with RIF resistance in Mtb isolates [50, 51, 60-64]. RIF monoresistance is rare and it occurs in combination with resistance to other drugs, most frequently INH, making RIF targets a surrogate marker of the MDR-TB phenotype [65]. Several studies revealed that RIF resistance commonly occurs due to rpoB gene mutation, which accounts approximately 96% of RIF resistance [50, 51, 60-64]. This review demonstrated that a prevalence of 90.8% for rpoB gene mutation in patients with DR-TB, suggesting a serious epidemic of RIF resistant Mtb among these patients. The present meta-analysis derived the most common gene mutation associated with RIF resistance was rpoBMUT3(S531L) with a pooled prevalence of 74.20 % (95% CI 66.39-82.00%). Besides, the second most frequent RIF resistance conferring mutation in this review was rpoBMUT2A (H526Y) with 17.20% estimated pooled prevalence. Similarly, a study conducted by Elbir et al. from Sudan reported that the frequency of gene mutation at codon 531, 526 and 516 were 64.1%, 17.9%, and 7.7%, respectively [9]. The same repot revealed that all genetic alterations were occurred by single base substitutions, and the most common mutation was observed at codon S531L [9]. Several previous studies have reported supporting evidence to our review result, that the most common gene mutation associated with RIF resistance in Mtb is due to the nucleotide (codon) change at 531 and 526 in rpoB/RRDR [6, 9, 49, 66].
Limitations
As a limitation, first, in this systematic review and meta-analysis, only English published articles were included for the analysis. Second, due to lack of detail information in few included studies, this review did not present prevalence of RIF and INH monoresistance and have not estimated the pooled prevalence of gene mutations associated with RIF and INH monoresistance. Third, majority of the studies have not explained proportions of gene mutations based on sex and age of participants; so that, this review did not explain sex and age-wise comparison of RIF and INH resistance mutations. Four, the development of gene mutations in Mtb strains associated with different anti-TB drug resistance varies across different TB patient’s treatment outcome (failure, loss of follow-up, retreatment cases) and diagnostic test results (e.g. retreatment smear negative and positive case, any follow-up smear positive cases) as well as other patient’s associated health conditions; however, due to the lack of detail information regarding these issues, this review failed to explain the estimated pooled prevalence of different gene mutations associated with RIF and INH among those TB patient categories.
Conclusions
In conclusion, RIF resistance was most commonly occurred due to mutations in the S531L followed by H526Y genes, while INH resistance was most frequently due to mutations in the katG315 gene, and these mutations were also associated with MDR and polydrug resistance, whereas mutations in inhA promotor region were less frequent. Commonly, the gene mutations in both katG gene and inhA promotor region rise the development of MDR-TB and the risk of relapse. However, the increasing frequencies of these gene mutations seem to vary by region, which could lead to differences in the sensitivity of genotypic/molecular diagnostics tools, if the tests are based only on these gene mutations. This would permit for modifying of genotypic/molecular tests to specific geographical locations, better understanding/interpretation of the molecular tests being used, and better therapy recommendations.
Data Availability
The datasets anlyzed during this review can be accessed from the corrosponding author upon reasonable request.
Funding
None
Authors’ contributions
MAR: conceived the study, took the primary role in data acquisition, formal analysis, interpretation, writing the manuscrpit for publication. BA and BBA: took revision of the study protocol, particpated in result interpretation and review final manuscrpit for publication. All authors read and approved the final maunscrpit for publication.
Transparency declaration
The authors declare no conflict of interest
Supplementary Figure S1. Representative DNA patterns obtained by the GenoType®MTBDRplus assay.
Supplementary Table S1: The PRISMA checklist.
Supplementary Table S2: Table S2. Search strategy used for one of the databases (Medline/PubMed)
Supplementary Table S3: Quality appraisal result of included studies; Using Joanna Briggs Institute (JBI) quality appraisal checklist for cross-sectional studies.
Supplementary Table S4: Characteristics of included studies.
Supplementary Table S5: Characteristics of included studies.
Acknowledgments
Our aknowldgement goes to all corrosponding authors who provided us information when we requested them.
Abbreviations
- DR-TB
- drug resistant tuberculosis
- DST
- drug susceptibility testing
- DS-TB
- drug senstetive tuberculosis
- INH
- isoniazid
- MDR-TB
- multidrug resistant tuberculosis
- Mtb
- Mycobacterium tuberculosis
- PRISMA
- Preferred Reporting Items for Systematic review and Meta-analysis
- RIF
- rifampicin
- TB
- tuberculosis
- WHO
- world health organization
- XDR-TB
- extensive drug resistance TB.
References




