
Abstract
Digital clinical decision support tools have contributed to improved quality of care at primary care level health facilities. However, data from real-world randomized trials are lacking.
We conducted a cluster randomized, open-label trial in Tanzania evaluating the use of a digital clinical decision support algorithm (CDSA), enhanced by point-of-care tests, training and mentorship, compared with usual care, among sick children 2 to 59 months old presenting to primary care facilities for an acute illness in Tanzania (ClinicalTrials.gov NCT05144763). The primary outcome was the mean proportion of 14 major Integrated Management of Childhood Illness (IMCI) symptoms and signs assessed by clinicians. Secondary outcomes included antibiotic prescription, counselling provided, and the appropriateness of antimalarial and antibiotic prescriptions.
A total of 450 consultations were observed in 9 intervention and 9 control health facilities. The mean proportion of major symptoms and signs assessed in intervention health facilities was 46.4% (range 7.7% to 91.7%) compared to 26.3% (range 0% to 66.7%) in control health facilities, an adjusted difference of 15.1% (95% confidence interval [CI] 4.8% to 25.4%). Only weight, height, and pallor were assessed more often when using the digital CDSA than in controls. Observed antibiotic prescription was 37.3% in intervention facilities, and 76.4% in control facilities (adjusted risk ratio 0.5; 95% CI 0.4 to 0.7; p<0.001). Appropriate antibiotic prescription was 81.9% in intervention facilities and 51.4% in control facilities (adjusted risk ratio 1.5; 95% CI 1.2 to 1.8; p=0.003).
The implementation of a digital CDSA improved only slightly the mean proportion of IMCI symptoms and signs assessed in consultations with sick children, and most symptoms and signs were assessed infrequently. Nonetheless, antibiotics were prescribed less often, and more appropriately Innovative approaches to overcome barriers related to clinicians’ motivation and work environment are needed.
Introduction
Millions of preventable deaths are attributed to suboptimal healthcare quality [1]. Factors such as staff shortages, inadequate budget allocation, poor clinical knowledge, and limited access to quality medical education, mentorship and supervision collectively contribute to this issue [2–4]. In response to this challenge, and with the aim of reducing childhood mortality, the World Health Organization developed the Integrated Management of Childhood Illness (IMCI) Chartbook [5]. Since its inception, over 100 countries have implemented the guidelines, and IMCI may reduce mortality and improve quality of care [6, 7]. However, poor adherence to IMCI is common, limiting its benefits [8–10].
Digital Clinical Decision Support Algorithms (CDSAs) were devised with the aim of enhancing adherence to clinical guidelines. These tools, typically operating on electronic tablets or mobile phones, guide health providers through the consultation process, by prompting the evaluation of symptoms, signs, and recommended diagnostic tests, to finally propose the appropriate diagnosis and treatment [11, 12]. While several studies have found that using these digital CDSAs improve adherence to IMCI, it is noteworthy that many of these investigations were conducted in controlled study settings, and most lacked randomization [13–20].
ePOCT+, a digital CDSA, was developed based on insights from two previous generations of CDSAs [21, 22], specifically addressing challenges by our CDSAs and others, such as limited scope and information technology difficulties [23]. The aim of the present study was to assess whether this CDSA associated with point-of-care tests, training, and mentorship, would improve quality of care for sick children compared to usual care, by comparing adherence to IMCI in a pragmatic cluster randomized trial.
Methods
Study design
The present study is an open-label, parallel-group, cross-sectional cluster randomized trial within the DYNAMIC Tanzania project. An external clinical researcher observed a sample of consultations from health facilities from both study arms documenting adherence of health care providers to quality-of-care indicators. The study was a planned ancillary study within a larger cluster randomized trial that was conducted between 1 December 2021 and 31 October 2022 using a sample of the clusters [24]. A cluster design was chosen since the intervention was targeted at the health facility and healthcare provider. The trial design and rationale are outlined in the protocol available in the parent trial registration on ClinicalTrials.gov number NCT05144763 and in the supplementary materials (S1 File). The detailed statistical analysis plan for this ancillary study is also available in the supplementary materials (S2 File).
The study design and implementation were collaboratively executed between both Tanzanian (Ifakara Health Institute, National Institute for Medical Research - Mbeya Medical Research Centre) and Swiss (Centre for Primary Care and Public Health [Unisanté] – University of Lausanne, and Swiss Tropical and Public Health Institute) partners. The design was guided by input from patients, and health providers during the implementation of similar trials in Tanzania [14, 22, 25]. Over 100 community engagement meetings involving over 7,000 participants were conducted before and during the study. These meetings included discussions with Community and Regional Health Management Teams in Tanzania.
Participants
The health facility was the unit of randomization since the intervention targeted both the healthcare provider and health facility. Primary care health facilities (dispensaries or health centres) were eligible for inclusion if they performed on average 20 or more consultations with children 2 months to 5 years per week, were government or government-designated health facilities, and were located less than 150 km from the research institutions. Specific to this study, consultations were only included if healthcare providers had been trained to use ePOCT+, and the ePOCT+ tool was functioning on the day of observation (no IT issues related to power outages, or crashes reported).
In contrast to the larger trial that included children aged 1 day to 14 years, this ancillary study included only children aged 2 to 59 months old presenting for an acute medical or surgical condition at participating health facilities. Children presenting solely for scheduled consultations for a chronic disease (e.g. HIV, tuberculosis, malnutrition), for routine preventive care (e.g. growth monitoring, vaccination), or for a follow-up consultation were excluded.
The study was conducted in 5 councils within the Mbeya and Morogoro regions of Tanzania, with two councils being semi-urban and three rural. Malaria prevalence in febrile children was low in three councils, and moderately high in two. HIV prevalence among children less than 5 years old in Tanzania is 0.4% [26]. Healthcare for children under 5 years of age is free for all acute illnesses at government or government-designated primary health facilities, including the cost of medications [27]. Nurses and clinical officers routinely provide outpatient care in dispensaries, while in health centers medical doctors sometimes provide care as well. Clinical Officers, the predominant healthcare providers at primary health facilities, are non-physician health professionals with 2-3 years of clinical training following secondary school [28].
Interventions
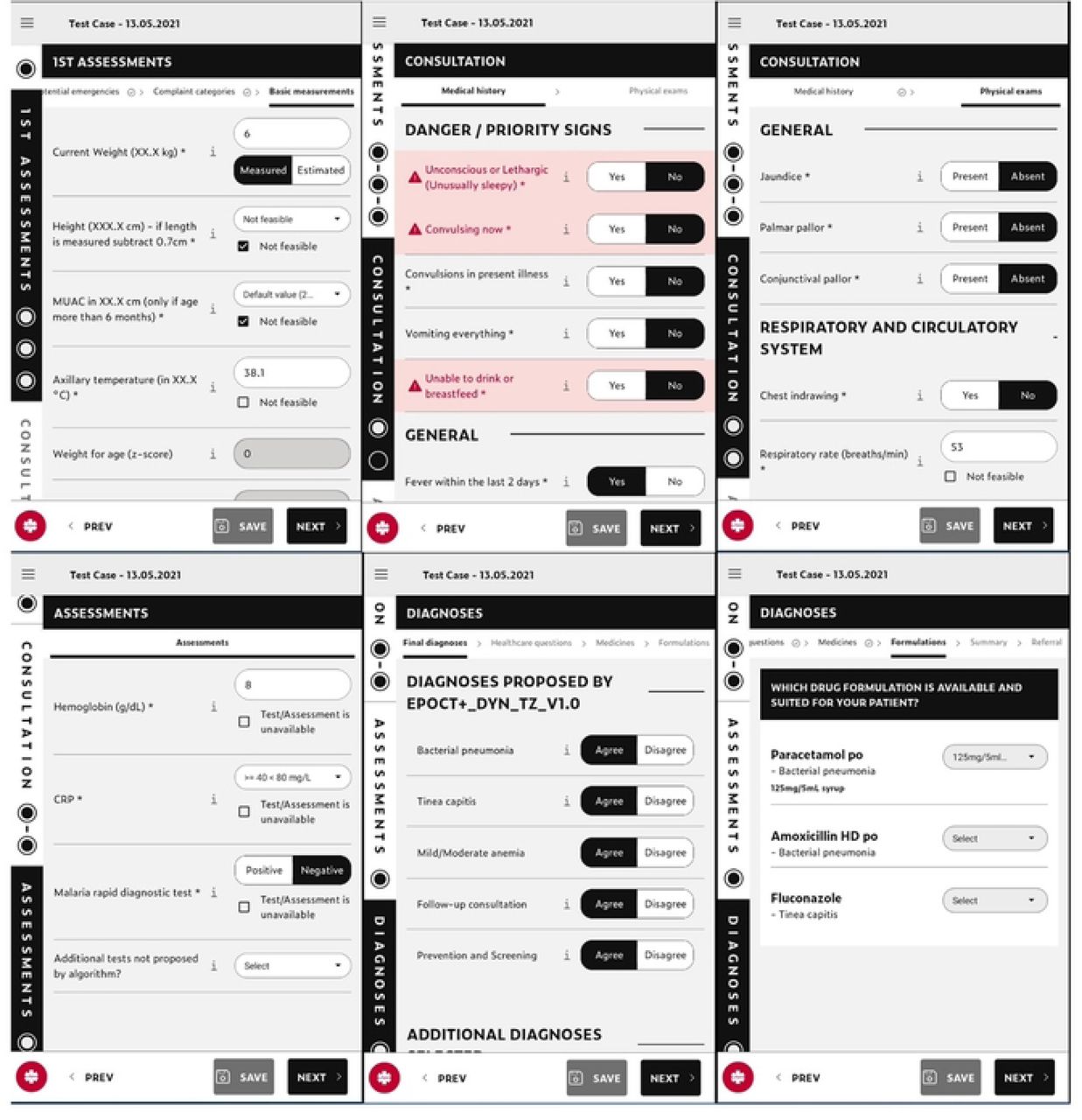
The intervention involved equipping health facilities with ePOCT+, an electronic clinical decision support algorithm on an Android based tablet (Fig 1), along with associated point-of-care tests (C-Reactive Protein, Hemoglobin, pulse oximetry), training, and mentorship. ePOCT+ prompts the healthcare provider to answer questions about demographics, symptoms, signs, and tests [23].

Based on the answers, ePOCT+ proposes one or more diagnoses, treatments, and management plans, including referral recommendation. Healthcare providers had the possibility to deviate from ePOCT+ recommendations. In order to move forward within the different sections of the digital tool, it was mandatory to respond to all IMCI symptoms and signs, except for height and mid-upper arm circumference (MUAC) which was optional. The tool allowed some signs to be estimated (temperature, respiratory rate) or based on recent measurements (weight).
The implementation team provided mentorship to intervention health facilities. This mentoring consisted of regular visits to health facilities every 2-3 months, and frequent communication via phone calls or group messages (3-4 times per month) to address issues, offer guidance, and gather feedback on the new tools. Quality-of-care dashboards were shared through group messages, enabling healthcare providers to compare their antibiotic prescription rates, uptake, and other quality-of-care indicators with other facilities (benchmarking). Control health facilities continued with usual care, did not have access to clinical data dashboards, and only received visits from the implementation team to help resolve issues related to the electronic case report forms (eCRFs).
The infrastructure provided to all health facilities (control and intervention) included a tablet for each outpatient consultation room, a router, a local server (Raspberry Pi), internet connectivity, and backup power (battery or solar system if needed). If unavailable weighing scales, mid-upper arm circumference (MUAC) bands, and thermometers were provided to all health facilities. Healthcare providers from both intervention and control facilities underwent equivalent clinical refresher training on IMCI and concepts of antibiotic stewardship. Additionally, specific training was provided on the use of the ePOCT+ CDSA in intervention facilities and the use of the eCRF in control facilities.
Outcomes
The primary outcome was the mean proportion of 14 pre-identified major IMCI symptoms and signs assessed by the healthcare provider, as observed by an external clinical research assistant. The included symptoms were fever, cough or difficult breathing, convulsions in this illness, diarrhea, ear pain or discharge, child unable to drink or breastfeed, and child vomits everything. The included signs were measurement of temperature, respiratory rate, pallor, weight, mid-upper arm circumference (MUAC), height, and skin turgor. In specific circumstances, some patients were not included in the denominator for specific signs as they were not clinically indicated as defined by IMCI: they include MUAC in children less than 6 months old, respiratory rate in the absence of cough or difficult breathing, and skin turgor in the absence of diarrhea. If cough or difficult breathing was not assessed, then we took the most conservative approach assuming that respiratory rate should have been measured, and the same for diarrhea and skin turgor. Of note “lethargic and unconscious” was considered as assessed if the clinician asked the caregiver if it was present during the illness, and not based on observation of the child as being “lethargic or unconscious”.
Secondary outcomes include the proportion of consultations during which each major IMCI symptom and sign were assessed, proportion of which other symptoms and signs were assessed (Supplementary Material Note 1), proportion of consultations where different IMCI counselling was conducted, and proportion of consultations for which antibiotics were prescribed. The rationale for the distinction between “major” IMCI and “other” symptom and signs are described in detail in the statistical analysis plan (Supplementary Material Note 1). Prescription of antibiotics was assessed by the research assistant by observing the actual prescription prescribed. The appropriateness of antibiotic prescription in relation to the retained diagnosis were also assessed. An appropriate antibiotic prescription was a prescription if one of the retained diagnoses required an antibiotic as per IMCI or the WHO hospital pocket book, and the absence of a prescription if no diagnosis required an antibiotic [29, 30]. An appropriate antimalarial prescription was a prescription of any antimalarial if there was a positive malaria test. Assessment of appropriateness was conducted blind to the study arm.
All outcomes pertained to the cluster level (health facility), and were assessed by an external clinical research assistants who observed the consultations in the consultation room without interfering with the consultation. The external clinical research assistants were clinical officers with experience in primary care consultations for children. Data was collected using a structured and pre-tested observation form programmed on ODK, and collected on an Android-based tablet. The observation form was based on the 2012 DHS Service Provision Assessment Survey form [31]. Of note, a more recent modification to this survey was developed after the initial planning of this study [31]. Modifications were made to the survey form, to shorten the duration of the evaluation and align it more closely with the aim of the evaluation, to incorporate additional signs and symptoms in line with IMCI 2014 guidelines such as duration of symptoms and the symptomatic assessment of lethargic or unconscious, and additions used by similar evaluations conducted previously [17].
Initially, antibiotic prescription was considered a co-primary outcome alongside the current primary outcome (proportion of 14 major IMCI symptoms and signs), but was later reclassified as a secondary outcome. We made this change to focus the analysis on quality of care, given that antibiotic prescription was already the primary outcome of the large longitudinal cluster randomized trial [24].
Sample size
The original sample size calculation was based on the previous co-primary outcome of antibiotic prescription. To detect a 25% absolute decrease in mean antibiotic prescription from a baseline of 50%, using an intraclass correlation coefficient (ICC) of 0.10 and an alpha of 0.05, a sample size of 25 patients in 9 clusters (health facilities) per arm was required to have 80% power. The ICC was based on studies evaluating prescription variations among different health care facilities/practices, ranging from 0.07 to 0.10 [32–35].
Expecting a high variability in baseline values of symptoms and signs assessed by a clinician and between clinicians [8, 13, 17, 36], the above sample size would have 67-93% power to detect a 30% absolute increase in the assessment of major IMCI symptoms and signs, considering a baseline value of 40-60%, an ICC of 0.15 – 0.25, and an alpha of 0.05.
Randomization
Within the parent trial, health facilities were randomized 1:1 by an independent statistician, stratified by monthly attendance, type of health facility (dispensary or health centre), region, and council [37]. For the present ancillary study, another independent statistician sampled 18/40 facilities to be included. This included 8/8 health centers (4 intervention, and 4 control), and 10/32 dispensaries. Among the 32 dispensaries, 10 were randomly sampled, stratified by study arm and region (following the same 3:2 ratio in favor of the Morogoro region as done in the parent trial). Due to the nature of the intervention, it was not feasible to blind the healthcare providers, patients, study implementers, or external clinical research asssitants (observers) to the intervention.
A convenience sampling was employed, whereby the external clinical researcher observed all eligible consultations while present at the health facility during normal standard working hours (Monday to Friday, 8:00 to 15:00).
Statistical methods
All analyses were performed using an intention-to-treat approach, i.e. all children with a recorded outcome were included in the analysis regardless if the intervention, ePOCT+, was used or not. All analyses were performed using a clustered-level analysis approach instead of an individual-level analysis due to the small number of clusters included [38, 39]. The analysis was performed using a two-stage approach as outlined by Hayes et al [39, 40], to adjust for both the cluster-level and individual-level covariates. In the first stage, we used a logistic regression model for binary outcomes and linear regression model for continuous outcomes adjusting for covariates and ignoring clustering and trial arm. Cluster-level residuals were then calculated for each cluster. In the second stage the residuals were compared to estimate risk ratios for the binary outcomes and mean risk difference for the continuous outcome (including the primary outcome) between study arms. Pre-specified cluster level covariates were type of health facility, council, healthcare worker cadre, and healthcare worker years of experience. Pre-specified individual level covariates of patients were age and sex. All analyses were performed using Stata v16, v17, and v18.
Ethics
Written informed consent was obtained from all parents or guardians of participants when attending the participating health facility during the enrollment period. We also requested, written informed consent from all healthcare providers for which their consultations were observed during this ancillary study. Ethical approvals were granted from the Ifakara Health Institute (IHI/IRB/No: 11-2020), the Mbeya Medical Research Ethics Committee (SZEC-2439/R.A/V.1/65), the National Institute for Medical Research Ethics Committee (NIMR/HQ/R.8a/Vol. IX/3486 and NIMR/HQ/R.8a/Vol. IX/3583) in Tanzania and from the cantonal ethics review board of Vaud (CER-VD 2020-02800) in Switzerland.
Results
Baseline characteristics of health facilities, health providers, and patients
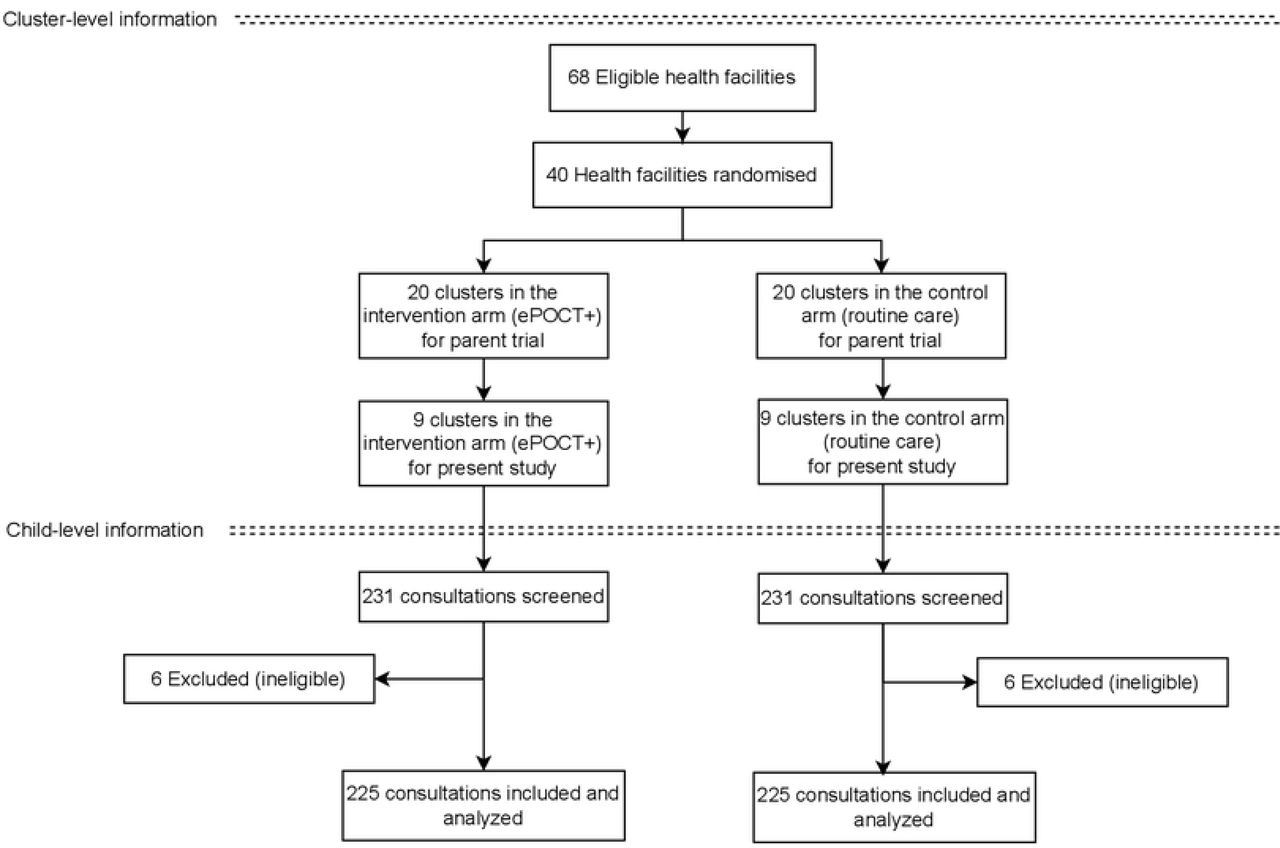
Between 23 March 2022 to 3 June 2022, 225 consultations were observed in 9 intervention facilities, and 225 consultations in 9 control facilities (Fig 2). Type of health facility, urban/rural localization, and region was well distributed between study arms (Table 1). A total of 17 healthcare providers saw patients in the control arm, and 22 in the intervention arm during the study. Distribution of sex, age, working experience and cadre of healthcare providers were similar in study arms. The number of healthcare providers with less than 3 years of experience was slightly higher in the control arm. Among included patients, there were slightly more female patients and median age was slightly higher in intervention arm compared to control. Within the intervention arm, ePOCT+ was used throughout the whole consultation in 213/225 (95%) of consultations, partially used in 5/225 (2%), used after the consultation in 6/225 (3%), and not used at all in 1/225 (0.4%) of consultations.

Assessment of symptoms and signs, and counselling
The primary outcome of mean proportion of major IMCI symptoms and signs assessed was higher by an adjusted difference of 15.1% (95% confidence interval [CI] 4.8% to 25.4%), p-value 0.007) in intervention health facilities (mean of 46.4%, range 7.7% to 91.7%) compared to control health facilities (mean of 26.3%, range 0% to 66.7%) (table 2). Weight, mid-upper arm circumference (MUAC) and pallor were the only individual assessments among the pre-identified major IMCI symptoms and signs that showed a statistically significant difference in the adjusted risk ratio (table 2). Among other symptoms and signs assessed, there was a statistically significant difference in the proportion of patients for which duration of cough, duration of diarrhea, mother’s HIV status were assessed, and the proportion of children who were undressed for the physical examination (table 3). There was no statistical difference in the proportion of counselling topics covered by health providers between study arms (table 4). For most outcomes the intraclass correlation coefficient (ICC) was relatively high suggesting high variability in adherence to IMCI between health facilities.
For the primary outcome of major IMCI symptoms and signs assessed, the ICC was higher in intervention health facilities (0.608) compared to control health facilities (0.354). This difference can also be seen when visualizing the mean proportion of major IMCI symptoms and signs assessed from each health facility in a scatterplot (Figure 3).

{kind=link}
{kind=link}
{kind=link}
Antibiotic and antimalarial prescription
Antibiotic prescription as observed by the external clinical researcher was lower in intervention health facilities compared to control health facilities with an adjusted risk ratio of 0.5, 95%CI 0.4 to 0.7 p-value <0.001 (table 5). The documented antibiotic prescription by healthcare providers (in the ePOCT+ tool for intervention facilities, and eCRF in control facilities) during the same 5-week period collected by the external clinical researchers in the same health facilities of the present analysis, was slightly lower than that observed by the external clinical researchers. The adjusted risk ratio remained nonetheless similar, 0.4, 95% CI 0.2 to 0.7, p-value 0.005.
81.9% of antibiotic prescriptions were appropriate in the intervention arm, compared to 51.4% in the control arm, adjusted relative risk of 1.5, 95% CI 1.2-1.5, p-value 0.003. All patients with malaria appropriately received an antimalarial treatment, and no patient without malaria received an antimalarial in both study arms.
Discussion
This cluster randomized controlled trial in Tanzania found that the use of ePOCT+, a digital clinical decision support algorithm, for the management of sick children aged 2-59 months old, moderately increased (by 15%) the mean proportion of major IMCI symptoms and signs assessed by health providers in primary care level health facilities. The overall proportion of IMCI symptoms and signs assessed at each individual consultation however remained low.
The overall increase in the mean proportion of major IMCI symptom and signs assessed by health providers aligns with previous studies in Tanzania [13], Afghanistan [36], Nigeria [17], and Burkina Faso [16], but in contrast to findings in South Africa [15], that did not find improvements in the assessment of IMCI symptoms and signs. While these findings suggest that digital clinical decision support algorithms can positively enhance quality of care for sick children, there is much room for improvement. Indeed, the proportion of most individual IMCI symptoms and signs assessed in both control and intervention arms were low, much lower than previous studies, and many symptoms and signs were not assessed more frequently in intervention health facilities. Differences compared to other studies, may be explained by the more pragmatic nature of the study compared to other studies conducted in more controlled settings (shorter pilot studies) where the Hawthorne effect may have a greater influence on health care provider behavior [13]. In addition, our study found much worse adherence to IMCI in the control arm compared to most other similar studies, such differences could partly be explained by differences in the setting and healthcare providers, notably the frequency and type of IMCI training provided to healthcare providers [16, 17]. The low proportion of children assessed for danger signs to identify children at highest risk of mortality is most concerning (33% for convulsions, 48% for unable to drink or breastfeed, and 36% for vomiting everything in the intervention arm). Respiratory rate was also infrequently assessed (29% in intervention arm), despite being an essential sign to distinguish children with cough or difficulty breathing requiring antibiotics or not [29].
The statistically significant increase in the assessment of weight (aRR 4.9 [95% CI 1.9 to 12.9]), and MUAC (aRR 5.5 [95% CI 1.7 to 17.6]) is noteworthy, as they are critical anthropometric measures to identify children with malnutrition, a condition that contributes significantly to childhood morbidity and mortality. Systematically measuring weight and MUAC to identify and manage severe malnutrition can indeed improve clinical outcomes as well as the long term health status of children [41]. The low proportion of children assessed for height/length however, reflects the difficulty and constraints of this measurement in particular [42], and the impact of not requiring the measurement to be mandatory within the digital tool.
While improved adherence to the assessment of IMCI symptoms and signs would likely be beneficial, translation to improved clinical outcomes should not automatically be assumed. Health providers often integrate a number of clinical cues that may allow them to distinguish which child would truly require danger signs to be assessed, or respiratory rate to be measured. For example, a 2 year old child presenting to a primary care health facility smiling and playing in the consultation room, with complaints of cough and runny nose for the past 2 days without difficulty breathing or fever, is unlikely to have danger signs and very often not have fast breathing or chest indrawing. This raises the important question on how to best assess quality of care, and whether it can be done without assessment of clinical outcome.
The large variation in mean proportion of major IMCI symptoms and signs between intervention health facilities provide clues to higher potential benefits of the intervention. The three best health facilities have a mean score of 60% or above, and the three worst below 30%. While clinical decision support algorithms may help improve knowledge and information on what symptoms and signs to assess, it would not address the other barriers and bad habits linked to poor adherence to IMCI [9, 10]. As with many complex health interventions, implementation of new interventions, and or guidelines may often not succeed with training alone, instead meaningful mentorship must be accompanied [43]. Indeed training, mentorship, and dashboards integrating benchmarking were part of the current intervention package, however these supportive interventions were not targeted towards assuring adherence to the assessment of many IMCI symptoms and signs but rather targeted on antibiotic stewardship, and overall uptake on the use of the tools. Adaptations to these supportive tools to target specific IMCI quality of care measures may help [44–46]. Further qualitative investigations are underway to better understand healthcare provider perspectives on barriers in adhering to ePOCT+ and the IMCI chartbook.
The study also revealed a two-fold reduction in antibiotic prescriptions (adjusted relative risk 0.5, 95% CI 0.4 to 0.7), and 50% improvement in the appropriate use of antibiotics in health facilities using ePOCT+ (adjusted relative risk 1.5 (95% CI 1.2 to 1.8), critical findings given the global concern for bacterial antimicrobial resistance [47]. Similar reductions were found in the parent trial using the intention-to-treat results over the full 11 month trial period (adjusted relative risk 0.6 (95% CI 0.5 to 0.6),[24] and in the same 5-week period as the present trial (adjusted relative risk 0.4, 95% CI 0.2 to 0.7). However, the documented antibiotic prescription as observed by external clinical researchers was slightly higher than what was documented by the health providers in ePOCT+ (intervention health facilities) and the eCRF (control health facilities), suggesting that some health providers may under report antibiotic prescription in ePOCT+ and the eCRF.
There were several limitations to this study. First, the Hawthorne effect, the presence of an external clinical researcher observing the consultation may have influenced the healthcare provider’s practice in both study arms. Indeed the uptake of the ePOCT+ tool in this study was higher compared to the parent trial (95% versus 76%), likely due to the presence of the researchers. Despite this, adherence to the IMCI chartbook was relatively low, and substantially lower compared to other studies, suggesting that the Hawthorne effect may not have had such a big impact, and the desirability bias minimal. Second, sample size; while the study was sufficiently powered for the primary outcome, interpretation of the secondary outcomes would have benefited from a higher sample size. Indeed many secondary outcomes did not show statistical significance despite relatively high effect size, likely due to the higher than expected heterogeneity between health facilities as indicated by the high ICC. Third, the intervention package included not only the digital tool, but also mentorship and benchmarking quality of care dashboards. It is thus not possible to understand what part of the intervention package and to what extent, impacted quality of care. Finally as discussed in previous paragraphs, adherence to IMCI is an imperfect proxy for the measurement of quality of care.
In conclusion, a digital clinical decision support algorithm package can help improve quality of care, however adherence to IMCI remained low for many symptoms and signs in a close to real world assessment. Further efforts including innovative approaches to improve quality of care are highly needed. The implementation of multiple interventions, such as the development and improvement of supportive mentorship of clinicians, better healthcare provider incentives, task-shifting, ongoing training and performance accountability may help address the many barriers to quality of care.
Data Availability
De-identified data can be found at 10.5281/zenodo.10849644
Supporting information
S1 File. DYNAMIC Tanzania study protocol
S2 File. Statistical analysis plan
S3 CONSORT Checklist
Acknowledgments
We would like to first thank all the participating healthcare providers, patients and caregivers. We acknowledge the contributions of the research assistants at the Ifakara Health Institute and Mbeya Medical Research Centre – National Institute of Medical Research, who assisted in the data collection, the Information Technology staff at Unisanté (Sylvain Schaufelberger, Greg Martin), and staff at Wavemind (Emmanuel Barchichat, Alain Fresco, and Quentin Girard) for their work on the medAL-suite during the study, and Community Health Management Team members in the 5 participating councils in Tanzania for their collaboration in implementing the study. We acknowledge researchers of the Tools of Integrated Management of Childhood Ilness and DYNAMIC Rwanda project for their contributions to ePOCT+ and the many common research activities (Dr Fenella Beynon, Dr Lena Matata, Dr Helene Langet, Dr Ludovico Cobuccio, Dr Victor Rwandacu, Dr Robert Moshiro). Finally we would like to acknowledge the work of Dr Irene Masanja on the initial development of the study, who regretably passed away before the start of the study.
Footnotes
↵† Deceased
References



