
ABSTRACT
Background The purpose of this study was to evaluate whether a bivalent COVID-19 vaccine protects against COVID-19.
Methods Employees of Cleveland Clinic in employment on the day the bivalent COVID-19 vaccine first became available to employees, were included. The cumulative incidence of COVID-19 was examined over the following weeks. Protection provided by vaccination (analyzed as a time-dependent covariate) was evaluated using Cox proportional hazards regression. The analysis was adjusted for the pandemic phase when the last prior COVID-19 episode occurred, and the number of prior vaccine doses received.
Results Among 51011 employees, 20689 (41%) had had a previous documented episode of COVID-19, and 42064 (83%) had received at least two doses of a COVID-19 vaccine. COVID-19 occurred in 2452 (5%) during the study. Risk of COVID-19 increased with time since the most recent prior COVID-19 episode and with the number of vaccine doses previously received. In multivariable analysis, the bivalent vaccinated state was independently associated with lower risk of COVID-19 (HR, .70; 95% C.I., .61-.80), leading to an estimated vaccine effectiveness (VE) of 30% (95% CI, 20-39%). Compared to last exposure to SARS-CoV-2 within 90 days, last exposure 6-9 months previously was associated with twice the risk of COVID-19, and last exposure 9-12 months previously with 3.5 times the risk.
Conclusions The bivalent COVID-19 vaccine given to working-aged adults afforded modest protection overall against COVID-19, while the virus strains dominant in the community were those represented in the vaccine.
Summary Among 51011 working-aged Cleveland Clinic employees, the bivalent COVID-19 vaccine booster was 30% effective in preventing infection, during the time when the virus strains dominant in the community were represented in the vaccine.
INTRODUCTION
When the original Coronavirus Disease 2019 (COVID-19) vaccines first became available in 2020, there was ample evidence of efficacy from randomized clinical trials [1,2].Vaccine effectiveness was subsequently confirmed by clinical effectiveness data in the real world outside of clinical trials [3,4], including an effectiveness estimate of 97% among employees within our own healthcare system [5]. This was when the human population had just encountered the novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) virus, and the pathogen had exacted a high burden of morbidity and mortality across the world. The vaccines were amazingly effective in preventing COVID-19, saved a large number of lives, and changed the impact of the pandemic.
Although the vaccines were very effective, the majority of the population in resource-poor countries could not get vaccinated in time, and waves of infection occurred around the world. Continued acquisition of mutations in the virus, from natural evolution in response to interaction with the immune response among the human population, led to the emergence and spread of SARS-CoV-2 variants. Despite this, those previously infected or vaccinated continued to have substantial protection against reinfection by virtual of natural or vaccine-induced immunity [6]. The arrival of the Omicron variant in December 2021, brought a significant change to the immune protection landscape. Previously infected or vaccinated individuals were no longer protected from COVID-19 [6]. Vaccine boosting provided some protection against the Omicron variant [7,8], but the degree of protection was not near that of the original vaccine against the pre-Omicron variants of SARS-CoV-2 [8]. After the emergence of the Omicron variant, prior infection with an earlier lineage of the Omicron variant protected against subsequent infection with a subsequent lineage [9], but such protection appeared to wear off within a few months [10]. During the Omicron phase of the pandemic, protection from vaccine-induced immunity decreased within a few months after vaccine boosting [8].
Recognition that the original COVID-19 vaccines provided much less protection after the emergence of the Omicron variant, spurred efforts to produce newer vaccines that were more effective. These efforts culminated in the approval by the US Food and Drug Administration, on 31 August 2022, of bivalent COVID-19 mRNA vaccines, which contained antigens represented in the original vaccine as well as antigens representing the BA.4/BA.5 lineages of the Omicron variant. Given the demonstrated safety of the earlier mRNA vaccines and the perceived urgency of need of a more effective preventive tool, these vaccines were approved without demonstration of effectiveness in clinical studies.
The purpose of this study was to evaluate whether the bivalent COVID-19 vaccine protects against COVID-19.
METHODS
Study design
This was a retrospective cohort study conducted at the Cleveland Clinic Health System (CCHS) in the United States. The study was approved by the Cleveland Clinic Institutional Review Board as exempt research (IRB no. 22-917). A waiver of informed consent and waiver of HIPAA authorization were approved to allow the research team to access to the required data.
Setting
Since the arrival of the COVID-19 pandemic at Cleveland Clinic in March 2020, employee access to testing has been a priority. Systems were designed to enable Occupational Health to interview and remotely monitor symptoms for all employees while the latter were isolated at home. Voluntary vaccination for COVID-19 began on 16 December 2020, and the monovalent vaccine as a booster became available to employees on 5 October 2021. The bivalent COVID-19 vaccine began to be offered to employees on 12 September 2022. This date was considered the study start date.
The circulating variants of SARS-CoV-2 varied over the course of the study. The majority of infections in Ohio were caused by the BA.4 or BA.5 lineages of the Omicron variant during the first 10 weeks of the study, based on SARS-CoV-2 variant monitoring data available from the Ohio Department of Health. By December, the BQ.1, BQ.1.1, and BF.7 lineages accounted for a substantial proportion of the infections.
Participants
CCHS employees in employment at any Cleveland Clinic location in Ohio on 12 September 2022, the day the bivalent vaccine first became available to employees, were included in the study. Those for whom age and gender were not available were excluded.
Variables
Covariates collected were age, gender, job location, and job type categorization into clinical or non-clinical, as described in our earlier studies [5–7]. Institutional data governance rules related to employee data limited our ability to supplement our dataset with additional clinical variables. Subjects were considered pre-pandemic hires if hired before March 16, 2020, the day COVID-19 testing became available in our institution, and pandemic hires if hired on or after that date.
Prior COVID-19 was defined as a positive NAAT for SARS-CoV-2 any time before the study start date. The date of infection for a prior episode of COVID-19 was the date of the first positive test for that episode of illness. Subsequent positive tests within 90 days were considered part of the same episode of illness. A positive test more than 90 days following the date of a previous infection, was considered a new episode of infection. Since the health system never had a requirement for systematic asymptomatic employee test screening, most of the positive tests during the study period would have been tests done to evaluate suspicious symptoms. Some would have been to evaluate known exposures. A small proportion could have been tests done as part of pre-operative or pre-procedural screening.
The pandemic phase during which a subject had his or her last prior episode of COVID-19 was also collected as a variable. To determine this, the pandemic was divided into pre-Delta, Delta, Omicron BA.1/BA.2, and Omicron BA.4/BA.5 phases, based on which variant/lineages accounted for more than 50% of infections in Ohio at the time. The data for this determination was obtained from variant proportion data provided by the Centers for Disease Control and Prevention (CDC) [11].
Outcome
The study outcome was time to COVID-19, the latter defined as a positive NAAT for SARS-CoV-2 any time after the study start date. Outcomes were followed until December 12, 2022.
Statistical analysis
A Simon-Makuch hazard plot [12] was created to compare the cumulative incidence of COVID-19 in the bivalent vaccinated and non-vaccinated states, by treating bivalent vaccination as a time-dependent covariate. Individuals were considered bivalent vaccinated 7 days after receipt of a single dose of the bivalent COVID-19 vaccine. Subjects who had not developed COVID-19 were censored at the end of the study follow-up period. Those whose employment was terminated during the study period before they had COVID-19 were censored on the date of termination of employment. Curves for the non-vaccinated state were based on data while the bivalent vaccination status of subjects remained “non-vaccinated”. Curves for the bivalent vaccinated state were based on data from the date the bivalent vaccination status changed to “vaccinated”.
Multivariable Cox proportional hazards regression models were fitted to examine the association of various variables with time to COVID-19. Bivalent vaccination was included as a time-dependent covariate [13]. The primary model included all study subjects. The secondary model included only those with prior exposure to SARS-CoV-2 by infection or vaccination. Vaccine effectiveness was calculated from the hazard ratios for bivalent vaccination in the models.
The analysis was performed by N. K. S. and A. S. N. using the survival package and R version 4.2.2 (R Foundation for Statistical Computing) [13–15].
RESULTS
Of 51977 eligible subjects, 966 (1.9%) were excluded because of missing age or gender. Of the remaining 51011 employees included in the study, 34507 (68%) had been in employment since before the onset of the COVID-19 pandemic (pre-pandemic hires). 1794 subjects (3.5%) were censored during the study period because of termination of employment before the end of the study. By the end of the study, 10804 (21%) were bivalent vaccine boosted. The bivalent vaccine was the Pfizer vaccine in 9595 (89%) and the Moderna vaccine in the remaining 1178. Altogether, 2452 employees (5%) acquired COVID-19 during the 13 weeks of the study.
Baseline characteristics
Table 1 shows the characteristics of subjects included in the study. Notably, this was a relatively young population, with a mean age of 42 years. Among these, 20689 (41%) had previously had a documented episode of COVID-19 and 12029 (24%) had previously had an Omicron variant infection. 44592 subjects (87%) had previously received at least one dose of vaccine, 42064 (83%) had received two doses, 27254 (53%) had received at least three doses, and 3858 (8%) had received four or more doses. 46340 (91%) had been previously exposed to SARS-CoV-2 by infection or vaccination.
Risk of COVID-19 based on prior infection and vaccination history
The risk of COVID-19 varied by the phase of the epidemic in which the subject’s last prior COVID-19 episode occurred. In decreasing order of risk of COVID-19 were those never previously infected, those last infected during the pre-Delta or Delta phase, those last infected during the Omicron BA.1/BA.2 phase, and those last infected during the Omicron BA.4/BA.5 phase (Figure 1).
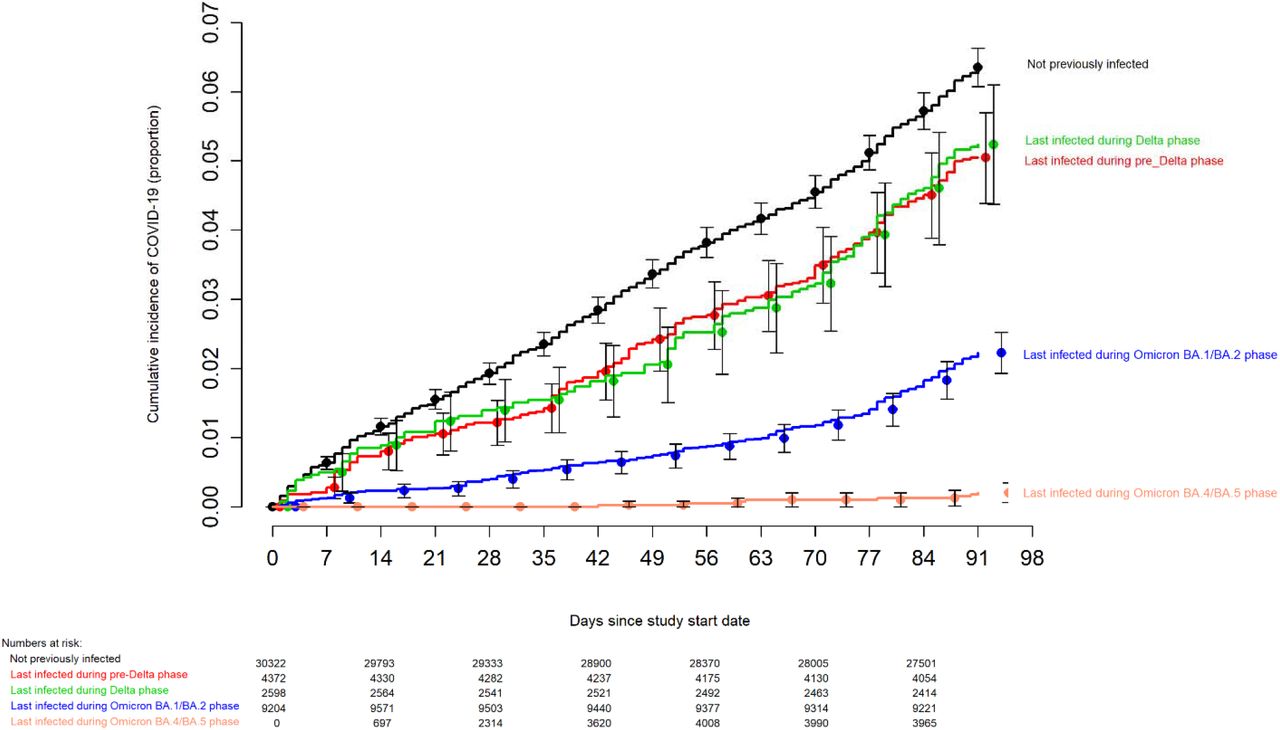
Simon-Makuch plot comparing the cumulative incidence of COVID-19 for subjects stratified by the pandemic phase during which the subject’s last prior COVID-19 episode occurred. Day zero was 12 September 2022, the day the bivalent vaccine began to be offered to employees. Point estimates and 95% confidence intervals are jittered along the x-axis to improve visibility.
The risk of COVID-19 also varied by the number of COVID-19 vaccine doses previously received. The higher the number of vaccines previously received, the higher the risk of contracting COVID-19 (Figure 2).
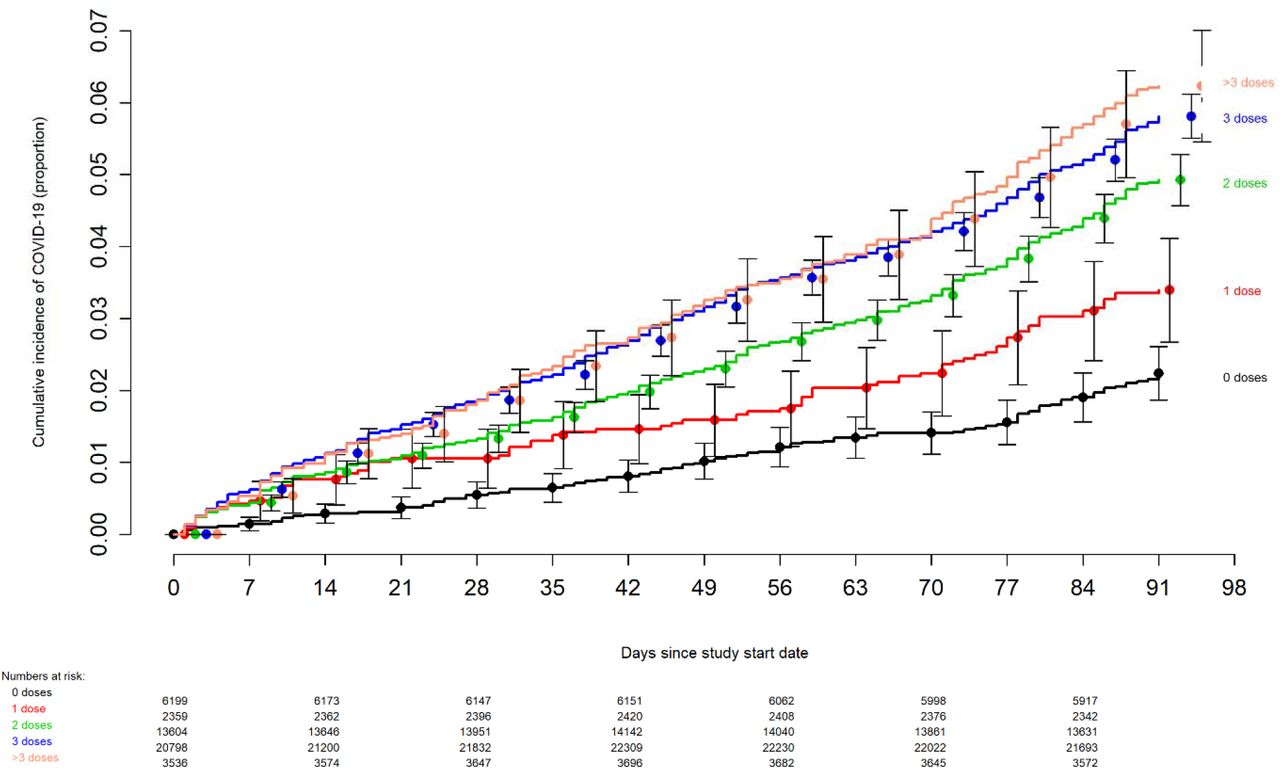
Simon-Makuch plot comparing the cumulative incidence of COVID-19 for subjects stratified by the number of COVID-19 vaccine doses previously received. Day zero was 12 September 2022, the day the bivalent vaccine began to be offered to employees. Point estimates and 95% confidence intervals are jittered along the x-axis to improve visibility.
Bivalent vaccine effectiveness
In a multivariable Cox proportional hazards regression model adjusted for age, gender, hire cohort, job category, number of COVID-19 vaccine doses prior to study start, and epidemic phase when the last prior COVID-19 episode occurred, a bivalent vaccine provided some protection against COVID-19 (HR, .70; 95% C.I., .61-.80; P-value, <.001). Point estimates and 95% confidence intervals for hazard ratios for the variables included in the unadjusted and adjusted Cox proportional hazards regression models are shown in Table 2. The calculated overall vaccine effectiveness from the model was 30% (95% C.I., 20% – 39%).
The multivariable analyses also found that, the more recent the last prior COVID-19 episode was the lower the risk of COVID-19, and that the greater the number of vaccine doses previously received the higher the risk of COVID-19.
Bivalent vaccine effectiveness among those with prior SARS-CoV-2 infection or vaccination
Given that both natural immunity and vaccine-induced immunity protect against COVID-19, and both forms of immunity wane over time, one way to assess the effectiveness of a vaccine is to adjust for time since the proximate SARS-CoV-2 exposure by infection or vaccination. Among persons with prior exposure to SARS-CoV-2 by infection or vaccination, hazard ratios for bivalent vaccination for individuals, after adjusting for time since proximate SARS-CoV-2 exposure, are shown in table 3. This analysis shows that, in addition to a 21% protective effect of bivalent vaccination, those with last exposure to SARS-CoV-2 6-9 months previously have twice the risk, and those exposed 9-12 months previously have 3.5 times the risk, of COVID-19, compared to those with last exposure within the preceding 90 days.
DISCUSSION
This study found that the current bivalent vaccines were about 30% effective overall in protecting against infection with SARS-CoV-2, when the Omicron BA.4/BA.5 lineages were the predominant circulating strains. The magnitude of protection afforded by bivalent vaccination was similar to that estimated in a recent study using data from the Increasing Community Access to Testing (ICATT) national SARS-CoV-2 testing program [16].
The strengths of our study include its large sample size, and its conduct in a healthcare system where a very early recognition of the critical importance of maintaining an effective workforce during the pandemic led to devotion of resources to have an accurate accounting of who had COVID-19, when COVID-19 was diagnosed, who received a COVID-19 vaccine, and when. The study methodology, treating bivalent vaccination as a time-dependent covariate, allowed for determining vaccine effectiveness in real time.
The study has several limitations. Individuals with unrecognized prior infection would have been misclassified as previously uninfected. Since prior infection protects against subsequent infection, such misclassification would have resulted in underestimating the protective effect of the vaccine. However, there is little reason to suppose that prior infections would have been missing in the bivalent vaccinated and non-vaccinated states at disproportionate rates. Those who chose to receive the bivalent vaccine might have been more worried about infection and might have been more likely to get tested when they had symptoms, thereby disproportionately detecting more incident infections among those who received the bivalent vaccine. This risk is mitigated by the time-dependent treatment of bivalent vaccination, because with such treatment, risk of disproportionate detection is actually in the opposite direction. If individuals received the bivalent vaccine thinking it would reduce their risk of infection, they would have been less inclined to get tested for the same symptoms after getting the vaccine (bivalent vaccinated state) than before getting the vaccine (non-bivalent vaccinated state), providing greater opportunity to detect infection in the non-boosted than the boosted state, thereby having the effect of overestimating vaccine effectiveness. Those who chose to get the bivalent vaccine were also more likely to have lower risk-taking behavior with respect to COVID-19, having the effect of a higher risk of COVID-19 in the non-boosted state (as those who chose not to get the bivalent vaccine, expectedly with higher risk-taking behavior, remained in the non-boosted state throughout the duration of the study), thereby again potentially overestimating vaccine effectiveness. The widespread availability of home testing kits might have reduced detection of incident infections. This potential effect should be somewhat mitigated in our healthcare cohort because one needs a NAAT to get paid time off, providing a strong incentive to get a NAAT if one tested positive at home. Even if one assumes that some individuals chose not to follow up on a positive home test result with a NAAT, it is very unlikely that individuals would have chosen to pursue NAAT after receiving the bivalent vaccine more so than before receiving the vaccine, at rates disproportionate enough to affect the study’s findings. We were unable to distinguish between symptomatic and asymptomatic infections, and had to limit our analyses to all detected infections. Variables that were not considered might have influenced the findings substantially. There were too few severe illnesses for the study to be able to determine if the vaccine decreased severity of illness. Our study of healthcare personnel included no children and few elderly subjects, and the majority would not have been immunocompromised. Lastly, during most of the study the circulating variants were those represented in the vaccine. It is not known if the vaccine will be equally effective when the strains circulating in the community are not those represented in the vaccine.
A possible explanation for a weaker than expected vaccine effectiveness is that a substantial proportion of the population may have had prior asymptomatic Omicron variant infection. About a third of SARS-CoV-2 infections have been estimated to be asymptomatic in studies that have been done in different places at different times [17–19]. If so, protection from the bivalent vaccine may have been masked because those with prior Omicron variant infection may have already been somewhat protected against COVID-19 by virtue of natural immunity. A seroprevalence study conducted by the CDC found that by February 2022, 64% of the 18-64 age-group population and 75% of children and adolescents had serologic evidence of prior SARS-CoV-2 infection [20], with almost half of the positive serology attributed to infections that occurred between December 2021 and February 2022, which would have predominantly been Omicron BA.1/BA.2 lineage infections. With such a large proportion of the population expected to have already been previously exposed to the Omicron variant of SARS-CoV-2, there could be some concern that a substantial proportion of individuals may be unlikely to derive substantial benefit from a bivalent vaccine.
The evolution of the SARS-CoV-2 virus necessitates a more nuanced approach to assessing the potential impact of vaccination than when the original vaccines were developed. Additional factors beyond vaccine effectiveness need to be considered. The association of increased risk of COVID-19 with higher numbers of prior vaccine doses in our study, was unexpected. A simplistic explanation might be that those who received more doses were more likely to be individuals at higher risk of COVID-19. A small proportion of individuals may have fit this description. However, the majority of subjects in this study were generally young individuals and all were eligible to have received at least 3 doses of vaccine by the study start date, and which they had every opportunity to do. Therefore, those who received fewer than 3 doses (>45% of individuals in the study) were not those ineligible to receive the vaccine, but those who chose not to follow the CDC’s recommendations on remaining updated with COVID-19 vaccination, and one could reasonably expect these individuals to have been more likely to have exhibited higher risk-taking behavior. Despite this, their risk of acquiring COVID-19 was lower than those who received a larger number of prior vaccine doses. This is not the only study to find a possible association with more prior vaccine doses and higher risk of COVID-19. A large study found that those who had an Omicron variant infection after previously receiving three doses of vaccine had a higher risk of reinfection than those who had an Omicron variant infection after previously receiving two doses of vaccine [21]. Another study found that receipt of two or three doses of a mRNA vaccine following prior COVID-19 was associated with a higher risk of reinfection than receipt of a single dose [7]. We still have a lot to learn about protection from COVID-19 vaccination, and in addition to a vaccine’s effectiveness it is important to examine whether multiple vaccine doses given over time may not be having the beneficial effect that is generally assumed.
In conclusion, this study found an overall modest protective effect of the bivalent vaccine booster against COVID-19, among working-aged adults. The effect of multiple COVID-19 vaccine doses on future risk of COVID-19 needs further study.
Data Availability
All data produced in the present study are available upon reasonable request to the authors
Notes
Author contributions
N. K. S.: Conceptualization, methodology, validation, investigation, data curation, software, formal analysis, visualization, writing-original draft preparation, writing-reviewing and editing, supervision, project administration. P. C. B.: Resources, investigation, validation, writing-reviewing and editing. A. S. N.: Methodology, formal analysis, visualization, validation, writing-reviewing and editing.
J. F. S.: Resources, writing-reviewing and editing. A. H.: Resources, writing-reviewing and editing. S. M. G.: Project administration, resources, writing-reviewing and editing.
Potential conflicts of interest
The authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Funding
None.




{kind=link}
{kind=link}