
Abstract
Olfactory acuity, which includes detection thresholds, identification and appreciation/intensity, seems to decline with aging, obesity, and various neurological disorders. Knowing that the sense of smell influences energy intake, the interest in protecting this sense is constantly increasing. Physical activity might be a key intervention to counteract the loss of olfactory function. This systematic review aims to explore the literature on the effect of physical activity on olfactory acuity. The search strategy consisted of using index terms and keywords in MEDLINE, EMBASE, EBM Reviews – Cochrane Central Register of Controlled Trials, CINAHL, SPORTDiscus, and Web of Science search engine. Data from 17 studies that include 10 861 participants revealed that physical activity has improved olfactory thresholds, identification, and intensity. More precisely, chronic physical activity seemed to have better effects on olfactory components than acute practice. Even though this review clarified evidence about the effect of physical activity on the sense of smell, better methodological consistency is needed across studies such as standardized experimental conditions, the time of the day data are collected, and similar relative energy intake between participants to produce more robust results.
1 Introduction
Olfactory acuity is the ability to discriminate the presence or the absence of an odor. This concept could be divided into three components: odor detection threshold, odor identification, and odor intensity. The odor detection threshold represents the lowest odor concentration that the participant can perceive. Odor identification highlights the participant’s ability to discriminate the type of odor. Finally, odor intensity represents the degree of potency or vigor perceived by a participant to a certain type of odor. Also, odor intensity is usually inversely proportional to odor appreciation since a high odor intensity might feel uncomfortable while breathing. This main concept, with its three components, is often correlated with odor concentration. Indeed, the higher the concentration, the easier it should be to detect and identify the odor, and the higher the intensity.
Unfortunately, olfactory acuity seems to decrease in several situations, such as in aging, Parkinson’s and Alzheimer’s diseases, and people living with obesity [1-9]. This deterioration of the sense of smell can affect diet differently in each person. For example, there may be a decrease in the feeling of hunger, a lower quality energy intake, or even a lower protein consumption which could increase the loss of autonomy [10, 11]. In addition, there are also relations between loss of smell and social isolation [11-13], reduced cognitive functions [11, 14-18], fragile mental health [11, 19], and nutritional problems [10, 11]. Adequate energy intake is crucial to execute daily tasks with full autonomy or to perform a more intense activity, such as sports or other forms of exercise [11, 20]. Also, food consumption is directly connected to environmental stimuli such as the appearance of the food, its smell and the social context [21]. Correspondingly, olfactory sensitivity could affect energy balance by influencing energy intake. A study by Ginieis, Abeywickrema [22] suggested that a decreased olfactory sensitivity would lead to greater snack consumption between meals. Considering that many snacks consumed are energetically dense [23], it is possible to observe the simultaneous increase between the number of obesity cases and the growing habit of consuming snacks daily [24, 25]. Consequently, the sense of smell is an essential component of the quality of life, and that is why it needs to be preserved.
Interestingly, physical activity (PA) seems to protect against the deterioration of the sense of smell. Indeed, treating the loss of olfactive acuity in Parkinson’s patients using PA might offer the same benefit as pharmacologic therapies, and this type of intervention showed to improve not only the olfactive function, but also motor symptoms [26, 27]. It is also possible to look into the physiological process of the olfactory loss to better understand the PA’s impact. A study comparing patients with type 2 diabetes to healthy adults found that high blood pressure could decrease olfactory acuity for both groups [28]. Also, a Schiffman [9] study investigating olfactory loss documented some physiological changes that occurred with aging such as the loss of cells and neurotransmitters in the hippocampus and the olfactory bulb in the brain. These changes could explain olfactory loss and could be positively modified by PA. Erickson, Voss [29] showed that chronic PA reduced the effect of normal aging of hippocampus volume. Knowing that this cerebral structure is involved in the olfactory function, there could be a link between PA and olfactory acuity.
A deeper understanding of the effects of PA on olfactory acuity would be beneficial to highlight the mechanisms modulating energy intake. This systematic review, therefore, aims to highlight the scientific consensus on the influence of PA on olfactory acuity. We will explore the effect of different types of PA on the three component of olfactory acuity, namely, odor detection thresholds, odor identification and odor intensity.
2 Methods
2.1 Search Strategy
This systematic review followed the “Preferred Reporting Items for Systematic Reviews and Meta-Analysis” (PRISMA) guidelines. Six databases were used to perform the search: Medline (1946-present), Embase (1974-present), EBM Reviews – Cochrane Central Register of Controlled Trials (1991-present), CINAHL Plus with Full Text (1937-present), SportDiscus with Full Text (1930-present) and Web of Science (1945-present). The last research was performed on December 22, 2021. The following keywords were used to search the concept of physical activity: “aerobic training” OR exercise* OR “physical activity” OR “physical training” OR “resistance training” OR sport* OR “strength training” OR “weight training” OR weightlifting OR “weight lifting” OR running OR football OR hockey OR athletes OR exertion OR “athletic performance”. For olfaction, the following keywords were used: odor OR odour OR aroma OR fragrance* OR smelling OR smell OR olfactory OR olfaction OR normosmic OR normosmia OR hyposmic OR hyposmia OR anosmic OR anosmia OR odorant* OR sniff OR sniffing.
Included studies had to meet the following inclusion criteria: (1) investigate the effect of PA on olfactory acuity; (2) involving humans, both adults and children. On the other hand, studies were not included if (1) olfactory acuity had changed following head trauma or surgery; (2) studies were not completed or accepted in peer-review journals; (3) studies were written in a language other than English or French.
2.2 Study Selection
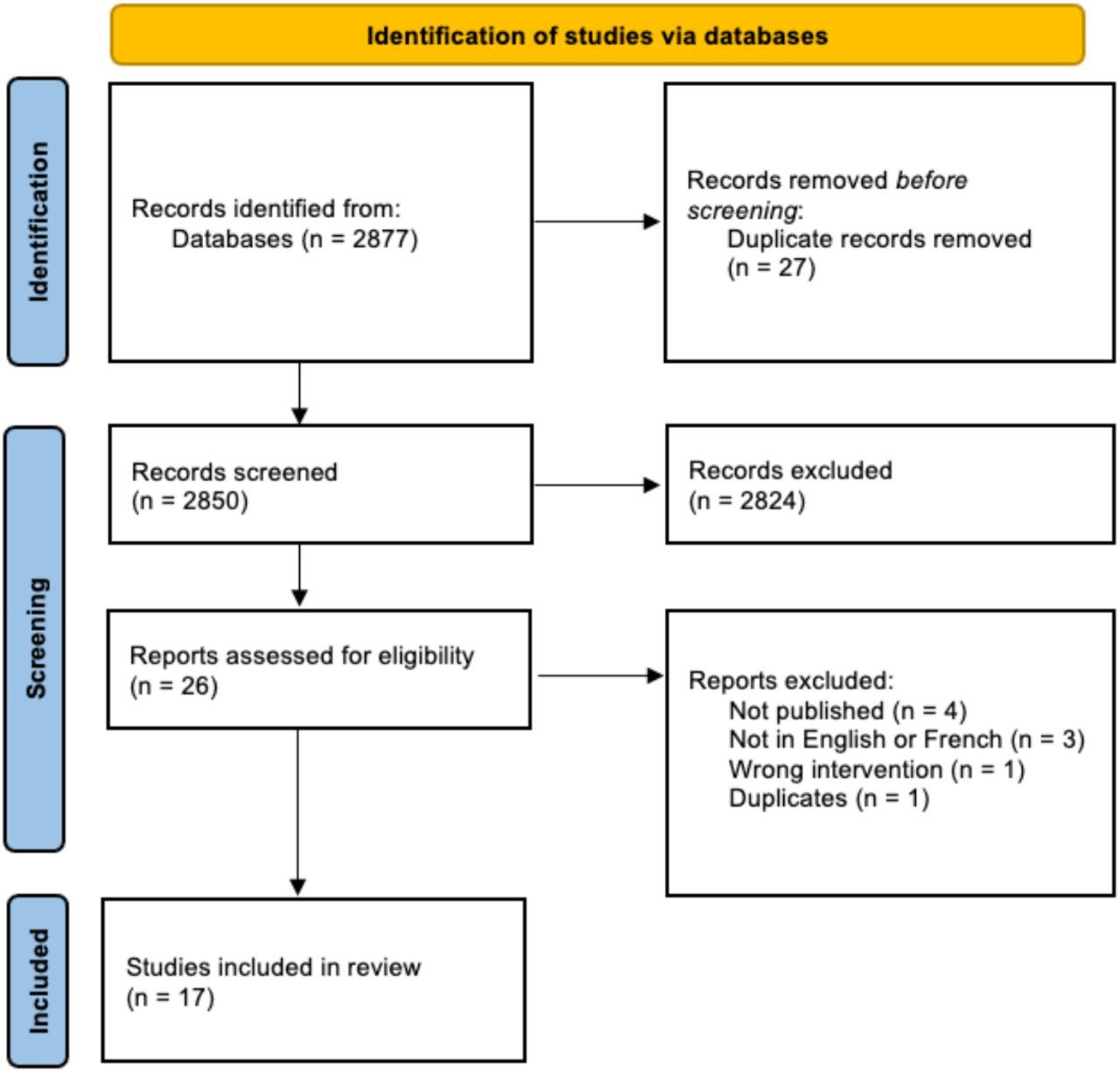
Figure 1 shows the evolution of the number of articles retained and excluded at each stage. Duplicates were removed after studies identification. The first screening of articles was done only using titles by two authors (MC, AD). The second screening of articles was done using abstracts by two authors (MC, AD). Subsequently, a final sorting was done by two authors (MC, AD) using the full texts of the remaining studies. All authors’ conflicts were discussed internally and resolved by a third author (ACG).
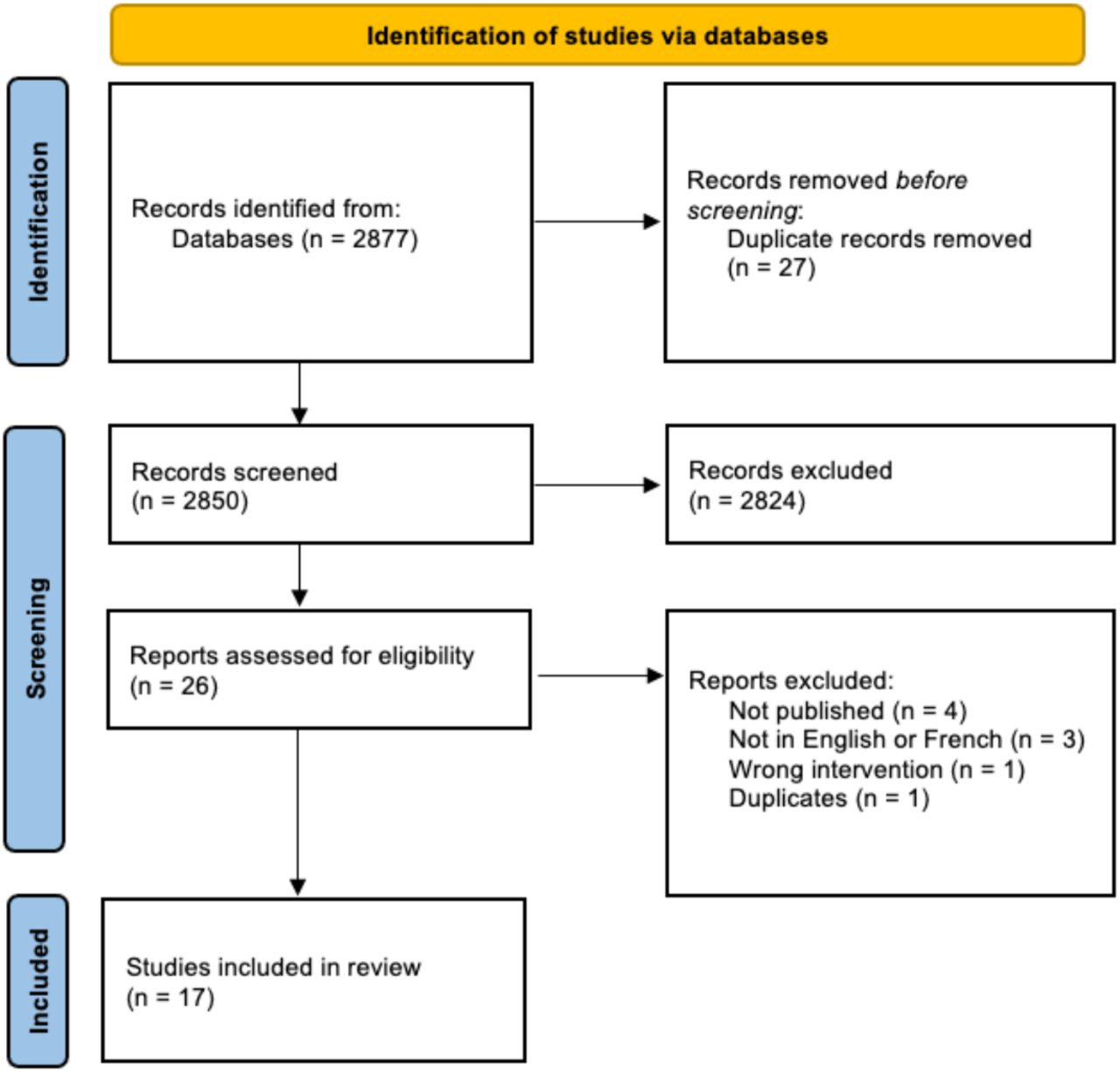
Flowchart of studies selection from their identification to final inclusion
2.3 Data Extraction and Analyses
Articles included following the selection process were read and analyzed by two authors (MC, AD). The data were processed by MC, extracted by MC and validated independently by AD. If differences were present, the authors reached a consensus following a discussion. If necessary, a third author (ACG) was consulted to make the decision. Data from included studies are summarized in Table 1, and their protocols are summarized in Table 2.
Included studies’ characteristics
Protocol description
2.4 Risks of Bias and Quality Assessment
Risks of bias and quality assessment were analysed using the QUADAS-2 tool [30]. This tool consists of four key domains, which cover 1) patient selection, 2) index tests, 3) reference standards, and 4) flow of patients through the study and timing of the index test(s) and reference standard (“flow and timing”) [30]. All domains were assessed in terms of their risk of bias. Patient selection, index tests, and reference standards were also assessed in terms of concerns regarding applicability. The risk of bias was assessed by one author (ACG), and a consensus was reached through discussion with two authors (MC and AM).
3 Results
3.1 Study Selection
Two thousand eight hundred seventy-seven studies were screened based on their titles, of which 26 were kept for full-text studies assessment. Of those studies, 17 were analyzed, and data were extracted. As presented in Table 1, the latter had between 6 and 4926 participants, which gives a total of n = 10 861 participants. There were also 14 of the 17 selected studies with an experimental design [31-44], including non-randomized studies [41-44]. The three remaining studies had a cross-sectional [45, 46] or a longitudinal [47] design. All 17 studies assessed the effect of PA on odor detection thresholds, odor identification, and/or odor appreciation/intensity for different type of odors.
3.2 Study and Physical Activity Intervention Characteristics
As presented in Table 1, studies took place in Canada [40, 44], China [41], Italy [34, 36, 42], Japan [32], the Netherlands [39], Poland [43], and the United States of America [31, 33, 35, 37, 38, 45-47]. The majority were conducted on healthy participants [33, 34, 36-42, 44-47] or participants living with a disease (e.g., Parkinson’s Disease)[31, 32, 35, 43]. Each study had an intervention time ranging from one session [32, 34, 37, 41, 43] to a 26-week program [31]. There was also one study with a 21-year follow-up [45]. Some exercise interventions consisted of cycling on an ergometer or running on a treadmill, and the intensity of the exercise was often based on the participant’s maximal oxygen consumption [31, 33, 35, 36, 38, 40, 44]. Other exercise interventions were the amount of daily movement that was associated to olfactory function [32], and an ultramarathon race (e.g., Tor des géants) [42]. Finally, the remaining studies assessed PA levels with a questionnaire (e.g. International Physical Activity Questionnaire [43]), and therefore included various types of PA [34, 37, 41, 43, 45-47].
3.3 Olfactory Protocols and Tests
As presented in Tables 1 and 2, 13 out of the 17 studies used sniffin’ sticks or odor pens with different odors [31, 32, 34-37, 40-44, 46, 47]. Two studies presented the odors in jars [38, 39]. The two remaining studies used a flow olfactometer [33, 45]. Olfactory tests included 8 to 40 odors. The odor detection threshold tests mainly included unfamiliar odors such as n-butanol and heptanol. Participants usually had two or three sticks presented to them, and they had to identify the one with the odor. The studies with a flow olfactometer [33, 45] had a different protocol in which participants were asked if they detected the odor or not. For the odor identification tests, most of the odors presented were familiar ones (e.g., strawberries, smoke). Participants had to identify the odor inhaled between various odors shown on a list. Finally, two studies investigated the appreciation/intensity of odors [38, 44] with visual analogue scales. Participants had to rate those variables following an odor exposure.
3.4 Effect of PA on the Three Components of Olfactory Acuity
Odor detection threshold
Of the 17 studies, six of them tested odor detection thresholds [33, 34, 36, 40, 41, 45]. While two studies showed no significant effect of PA on odor detection thresholds [33, 36], all the others showed significantly higher scores for the odor detection thresholds for the people who were physically more active (e.g., better detection threshold scores by 15% [41]).
Odor identification
Twelve studies explored odor identification [31, 32, 34, 35, 37, 39-43, 46, 47]. Four of these 12 studies showed no significant effect of PA on odor identification [31, 32, 39, 40]. Although one study showed a significant decrease in odor detection after a long PA session, more specifically after an ultramarathon of 332,5 km [42], the seven other studies reported a significant increase in odor identification in the physically active group (e.g., better identification scores by 13.12% [41]) [34, 35, 37, 41, 43, 46, 47].
Odor appreciation/intensity
In two studies in which appreciation and intensity of odors were assessed, it was revealed that an acute PA session significantly increased the perceived intensity and appreciation aversion [38, 44]. Nevertheless, these results seem to be odor-dependent, and the effect might change with different odors. For example, PA significantly increases odor intensity with food-related odors such as coffee and orange, which was not the case for non-food-related odors such as leather and rose.
3.5 Risk of Bias Assessment
While most of the studies had non-existent bias risks/applicability concerns, some were deemed as ‘’unclear’’ OR at ‘’high risk’’ of bias/applicability concerns (Table 3). Concerning patient selection, out of the 17 studies included in this review, two had an unclear potential risk of bias [45, 47], and one was considered at a higher risk [33]. Also, concerning reference standards, three studies were deemed unclear for their potential risk of bias [33, 42, 43]. Concerning flow and timing, two were classified as unclear [32, 34]. Concerning patient selection, four studies were categorized as unclear for their applicability concerns [33, 42, 45, 47]. Concerning the index test, only one study was classified at a higher risk for applicability concerns [32]. Finally, concerning reference standards, two were deemed unclear applicability concerns [33, 43]. While there were two instances where studies were classified at a higher risk of bias/applicability concerns [32, 33], their methodology and overall framework still made them eligible for data extraction in this systematic review.
Risk of Bias Assessment [30]
4 Discussion
The objective of this systematic review was to document the effect of PA on olfactory acuity. After the selection process, 17 studies were included. For the odor detection thresholds, four studies showed increased scores [34, 40, 41, 45], and two studies showed no significant results [33, 36]. For odor identification, seven showed an increase [34, 35, 37, 41, 43, 46, 47], one study showed a significant decrease following a prolonged PA session [42], and four studies showed no significant results [31, 32, 39, 40]. For odor appreciation/intensity, one of two studies showed an increase in intensity [44], while the other showed a significant appreciation aversion [38].
4.1 Odor Detection Thresholds
The effect of PA on odor detection thresholds has been explored by six studies [33, 34, 36, 40, 41, 45]. Half of these studies compared before and after PA intervention [33, 36, 40], while the other half compared an active and inactive group on a daily basis [34, 41, 45]. Four of the six studies revealed that PA increased odor detection thresholds [34, 40, 41, 45]. Studies that compared active and inactive groups on a daily basis all showed significant increases in odor detection threshold in the active group [34, 41, 45]. Also, two of the three studies that compared before and after a single PA intervention in the same group had no significant results [33, 36]. The only study that offered the same comparison with a significant increase had a longer total intervention. Indeed, the total duration of the experimental protocol lasted four days including three straight days of PA sessions, and significant results were obtained during the last day of the testing, which was on the fourth day [40]. All these results suggest that chronic PA would yield a better impact on odor detection thresholds than acute exercise.
Exercise intensity also seems an important variable to consider with the improvement of odor detection thresholds. Indeed, Zhang, Li [41] compared results between different exercise modalities and highlighted better olfactory outcomes for those who practiced dancing (3-11.3 metabolic equivalents (METS); thresholds score: 8.1/16) or running (3.5-23 METS; thresholds score: 7.4/16) in comparison to walking (1.5-3.8 METS; thresholds score: 4.0/16) [48]. Knowing that dancing and running can be performed at high intensity and that high-intensity exercise induces an anorexigenic effect [49, 50], which means a reduced energy intake following exercise, the hormonal changes described thereafter might play a role in this increased odor detection thresholds [3, 51].
Also, with the knowledge that chronic PA can generate weight loss by increasing energy expenditure and modulating some hormones by lowering leptin levels [52, 53], those two factors might play a crucial role in the odor detection threshold’s function. Indeed, in a systematic review by Peng, Coutts [3], there was a negative association between odor detection threshold and participant’s weight. Also, obesity is often associated with metabolic and hormonal dysfunctions, which can negatively impact the olfactory function. More precisely, obesity is positively correlated with lower ghrelin levels [3, 54], which stimulates the olfactory bulb, and with higher leptin, which is an olfactory inhibitor [3]. The differences between studies with a PA intervention (acute) and studies with a physically active group on a daily basis (chronic) might be due to the differences that chronic vs acute PA have on weight and hormone levels.
4.2 Odor Identification
The effect of PA on odor identification was the most documented olfactory component. In this review, 12 of the 17 studies covered this topic. Five studies compared odor identification before and after a PA intervention [31, 35, 39, 40, 42]. Three of them showed no significant effect of PA [31, 39, 40], and one showed a decrease in odor identification after PA [42]. This negative change in olfaction following an exercise session might have been produced by the extreme effort in this study as participants ran an ultra-marathon (332,5 km). However, this result is not consistent with hormonal changes that happened during and following such efforts. In fact, Roupas, Mamali [55] demonstrated that hormones such as leptin and insulin are significantly lowered following an ultra-marathon. As previously discussed, those changes should increase olfactory sensitivity [3, 51].
From the seven other studies comparing active and inactive groups on a daily basis [32, 34, 37, 41, 43, 46, 47], only one had no significant results [32]. Although acute PA seems to have little to no impact on odor identification, chronic PA produced much more conclusive and positive results. Once again, this effect might be related to weight loss and hormonal changes associated with the regular practice of PA. However, Peng, Coutts [3] identified no changes between different weight groups for odor identification in their systematic review, even though they admitted that the literature included conflicting results. For the hormonal changes, studies demonstrated that higher fasting blood glucose levels and hypertension might increase the risk of olfactory impairment by diminishing ghrelin and increasing leptin levels [3, 28]. Long-term PA might help regulate these hormones and protect the sense of smell [53].
Furthermore, Serby [56] demonstrated that odor identification decreased in patients with Parkinson’s and Alzheimer’s disease compared to healthy people of the same age. Jalali, Roudbary [2] also explained that odor identification varied between Parkinson’s patients and their stages in the disease. In the present review, three studies had patients with neurodegenerative disease, two with Parkinson’s [32, 35] and one with Alzheimer’s [31]. Rosenfeldt, Dey [35] documented a significant improvement of the odor identification score following an aerobic exercise with Parkinson’s patients (e.g., UPSIT scores four weeks after the treatment: the exercise group had +0.2 points and the control group had - 2.7 points versus the baseline evaluation). Alternatively, Terashi, Taguchi [32] showed no association between olfactory dysfunction and physical activity. In these three studies, diagnosed populations were compared altogether. Even though there are only a few studies with neurodegenerative participants, those results are less optimistic than studies with healthy populations that had better odor identification scores after PA. Those non-significant results with neurodegenerative patients suggest that the effect of PA is population-specific. This difference in the odor identification ability between healthy and neurodegenerative patients might be explained by various factors dependent of the specific disease [57]. For Alzheimer’s and Parkinson’s patients, one of the factors might be the higher reduction of the olfactory bulb volume [57-62]. A study by Brown, Cooper-Kuhn [63] showed that PA could not protect against the neurogenesis of the olfactory bulb. This fact could explain the differences observed in term of odor identification in the studies included in this review.
4.3 Odor Appreciation/Intensity
With the lack of articles in the literature regarding the effect of PA on odor appreciation and intensity, this review only identified two studies on this topic [38, 44]. These studies compared the results of before and after an intervention, showing a significant increase in odor intensity [44] and odor appreciation aversion [38]. These two studies focused on young participants and used visual analogue scales to measure odor appreciation/intensity, which might explain their consistent results. They also documented significant effect of PA on odor appreciation/intensity with some odors such as coffee and orange and no effect with other odors such as rose, which suggest that the effect of PA intervention is odor-specific. In fact, PA intervention changed the perception of food-related odors only. A study by Sorokowska, Schoen [64] highlighted that the right insula, anterior cingulate cortex, and putamen brain regions involved in odor processing are more active in response to food-related odors than other type of odor, which may explain these results. Indeed, those brain regions play a key role in reward loops, and hormonal changes such as higher ghrelin, which normally happens before eating, can affect those brain regions [64, 65]. Also, as mentioned earlier in the discussion, ghrelin is a hormone which stimulates the olfactory bulb [3]. Therefore, a higher concentration of this hormone could generate odor aversion [66]. However, it is important to note that it is unlikely that a higher ghrelin level is caused by the PA intervention since a systematic review showed that the ghrelin level will change after chronic physical activity practice and not acute [67]. In light of that information, food odor may have the ability to increase the activation of some brain regions while non-food odor would not. Therefore, these results align with the findings of both studies included in this systematic review.
Another potential cause for the effect of PA on odor intensity might be related to the timing of the testing sequence of the olfactory tests. Indeed, as evidenced by Josaphat, Drapeau [44], there was an increase in odor intensity between 8:30 a.m., and 11:30 a.m., which evidences a time-related effect and not a treatment effect which is the PA intervention. Therefore, it seems possible that the delay between the last energy intake and the odor presentation could impact the perception of odor intensity. In the same direction, ghrelin level, an olfactory stimulator [3], increases as the last caloric ingestion is far away [68]. However, more studies on odor appreciation and intensity are needed to explore these hypotheses, and protocols should identify specific timing for PA intervention and odor tests.
4.4 How Can We Measure Olfactory Acuity with a Novel Scope and How Can We Produce More Robust Results?
Over the years, studies that investigated the effect of PA on olfactory acuity have used different experimental paradigms. Some standardized the conditions before the experimentation [31, 33, 35, 36, 38-40, 44] while others tested in natural conditions the participant [32, 34, 37, 41-43, 45-47]. Even though the latter has been useful in determining the effect of acute and chronic PA on olfactory acuity, better standardization of the pre-experimentation conditions would generate more robust results. For example, knowing that hormonal changes can affect olfactory acuity [3], the exact time of the day the experimentation takes place should be controlled. This concept has been well documented in the study of Josaphat, Drapeau [44], which evidenced a time effect on the perceived intensity of food-related odors. Also, all participants should have the same relative energy intake before/during the experimentation to limit hormonal variations since olfaction can vary depending on the satiety state [69]. Furthermore, studies should measure participants’ bodyweight and use this bodyweight status for further analysis since hormone levels, such as ghrelin, change with this variable [3, 53].
In addition, future research should use more precise and easily regulated tools in odor testing. Indeed, most studies included in this review used Sniffin’ Sticks and questionnaires. Although these methods are commonly used, perhaps due to their simplicity, a more objective approach could strengthen the results. In this sense, some recent studies have started using an automatic olfactometer and an electroencephalogram to measure brain responses to odor stimuli [70, 71]. Therefore, this method makes it possible to understand better the brain mechanisms linked to the sense of smell while obtaining reproducible results. The same aspect about regulated tools should apply to PA. Indeed, it is also necessary to better monitor exercise to understand better which exercise modality (frequency, intensity, time, and type) is optimal for improving olfactory acuity.
4.5 Strengths and Limitations
Most of the studies included in this systematic review were relatively recent with the majority published in the last ∼10 years. This observation made it possible to have consistency in data collection and methods. In fact, every study that assessed the acute effect of PA used aerobic exercise such as running on a treadmill or pedalling on an ergometer, limiting findings to cardiovascular exercises. This review also included two types of PA, chronic and acute, which made possible to cover a larger portion of the literature to highlight the effects of each one. For odor appreciation and intensity, although a very small number of studies explored this concept, they both used a visual analogue scale, considered the gold standard for subjective sensory data collection [72]. The main limitation would be the time of the day at which data collection was made in every study. There was no consistency between each study for this parameter, which may have modulated the participants’ hunger level/hormones during the olfactory stimulations. Also, the measurement of PA could have been more precise since most of the studies used self-reported questionnaires [34, 37, 41, 43, 45-47]. Indeed, a study demonstrated that a questionnaire such as the International Physical Activity Questionnaire-Long Form overestimates PA time and underestimates sedentary behavior time [73]. All those inconsistencies in the methods made the possibility of performing a meta-analysis impossible. Better measurements of PA could help find the impact of its effect on olfactory thresholds, identification, and appreciation/intensity. In addition, studies rarely measured participants’ bodyweight and body composition to compare them with those having a similar bodyweight but different PA levels. Considering that hormone levels can change with PA and with bodyweights, bodyweight status and PA levels should be controlled to provide more robust results [3, 53]. Since this review includes all the studies mentioned in this paragraph, the same strengths and limitations apply to this review.
5 Conclusion
Physical activity, especially chronic, can improve olfactory acuity. More precisely, the detection threshold, identification, and intensity of odors are improved with a chronic practice of PA. Concerns about the loss of smell have recently surfaced in the healthcare community. Therefore, studies evaluating the impact of PA on the sense of smell are important to deepen our understanding of this therapeutic intervention on olfactory acuity.
Data Availability
All data produced in the present work are contained in the manuscript
Funding
Mathieu Cournoyer and Alexandre-Charles Gauthier received scholarships from the Université de Montréal. Fabien Dal Maso is a research scholar from the Fonds de recherche du Québec – Santé (Junior 1). Marie-Eve Mathieu holds a Canada Research Chair (Tier 2).
Disclosure of interest
The autors declare no conflict of interest.
Acknoledgement
The authors thank Denis Arvisais for his help with the search strategy.




{kind=link}