
Abstract
Background Since the first year of the COVID-19 global pandemic, a hypothesis concerning the possible protection/immunity of beta-thalassemia carriers remains in abeyance.
Methods Three databases (Pubmed Central, Scopus and Google Scholar) were screened and checked in order to extract all studies about incidence of confirmed COVID-19 cases OR mortality rate OR severity assessment OR ICU admission among patients with beta-thalassemia minor, were included in this analysis. The language was limited to English. Studies such as case reports, review studies, and studies that did not have complete data for calculating incidences were excluded.
Results and discussion Three studies upon 2265 were selected. According to our systematic-review meta-analysis, beta-thalassemia carriers could be less COVID-19 affected than general population [IRR= 0.9250(0.5752;1.4877)], affected by COVID-19 with a worst severity [OR=1.5933(0.4884;5.1981)], less admissible into ICU [IRR=0.3620(0.0025;51.6821)] and more susceptible to die from COVID-19 or one of its consequences [IRR=1.8542(0.7819;4.3970)]. However, all of those results stay insignificant with a bad p-value (respectively 0.7479, 0.4400, 0.6881, 0.1610). Other large case-control or registry studies are needed to confirm these trends.
Introduction
The world has had to face a COVID-19 pandemic for two years and then SARS-CoV-2 variants successive waves. This infection was first discovered in December 2019 in the South China Seafood Market Hubei Province, China [1]. Since the pandemic first months, an epidemiological particularity has been observed concerning minor beta-thalassemia patients: they seem to be protected against severe COVID-19 forms and in this way, the beta-thalassemic trait would confer a certain immunization against COVID-19 [2,3]. Few times after, a scientific niche debate (ed. between experts) was opened on the question: some epidemiological datasets supported this hypothesis [4-7] despite the fact that in vitro experiments tend to demonstrate a lack of a mechanistic link between Hb variants and disease effects [8]. This hypothesis is currently developed on the physiopathological side [9]. However, there are also epidemiological studies which support this hypothesis [10,11] and there is no evidence of a significant relationship between COVID-19 infection and the oxy-hemoglobin dissociation curve [12]. The main purpose of our manuscript is to do an epidemiological systematic-review meta-analysis on this subject in order to support (or not) the possible beta-thalassemia minor protection against COVID-19 (and its severe forms). In this systematic review study, we wanted to determine the prevalence, severity, the ICU admission and mortality rate of COVID-19 in beta-thalassemic minor patients.
Methods
This systematic review and meta-analysis has been done according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) checklist [13]. The review was registered at International Prospective Register of Systematic Reviews (PROSPERO) with the registration number CRD42022345452.
Searched databases
Searches were conducted in PubMed (www.ncbi.nlm.nih.gov/), Elsevier (www.elsevier.com) and Google Scholar (www.scholar.google.com) from 11 July to 17 July 2022, to identify original research articles, reviews and case reports that described β-thalassemic minor patients affected by coronavirus. The screening period for the studies would be from January 2020 to May 2022. Combinations of the following medical subject headings (MeSH), terms and keywords, were used to conduct a comprehensive literature search: (beta-thalassemia OR Cooley’s anemia) AND (SARS-CoV-2 OR COVID-19 OR novel coronavirus).
Reference lists of the eligible studies will be screened manually for the identification of additional relevant reports.
Inclusion and exclusion criteria
One author (Edouard Lansiaux) independently screened the articles by endnote software version 9 (https://endnote.com). The human observational studies, which reported the incidence of confirmed COVID-19 cases OR mortality rate OR severity assessment OR ICU admission among patients with beta-thalassemia minor, were included in this analysis. The language was limited to English. Studies such as case reports, review studies, and studies that did not have complete data for calculating incidences were excluded.
Data extraction
The same author would individually extract the following data for each study (each author willcheck a separate database): title of the study, DOI, study design, timeline (retrospective or prospective), country, study type, age, gender, number of patients, number of patients with beta-thalassemic traits, number of COVID-19 patients, number of COVID-19 patients with beta-thalassemic trait, severity of COVID-19 (asymptomatic or mild, moderate, severe), mortality number, ICU admission, comorbidities [Diabete mellitus, Hypertension, Cardiovascular disease, Pulmonary hypertension, Cancer, Chronic Pulmonary Disease (emphysema or/and bronchitis), Autoimmune disease (Hashimoto thyroiditis, rheumatoid arthritis, systemic lupus and autoimmune hepatitis), Hypercholesterolemia, Stroke). Reference lists of the included articles will be screened for additional relevant studies.
Datasets will be extracted and managed on Microsoft Excel. For MS Excel extraction sheet, we would use the Cochrane Effective Practice and Organisation of Care (EPOC) Template modified for the needs of our study.
Study quality assessment
The quality of the included studies was assessed by two independent assessors (Supplementary File 1). The JBI (Joanna Briggs Institute) critical appraisal checklist for cross-sectional and observational studies reporting incidence data. This checklist consists of nine items that evaluate the sampling process, data analysis process and statistical methods, study settings, measurement tools and response rate. The quality score of more than 5 was considered as moderate-high quality and included in meta-analysis. If there was any disagreement between assessors, it was resolved by discussion with authors.
Statistical analysis
Data will be aggregated based on study design, location of reporting (country), participants demographic characteristics, etc.
Firstly, we will make a qualitative synthesis, describing the main characteristics of the studies. If possible based on data reported in extracted studies, meta-analyses will be performed on each of the included parameters using R and its package “meta”. Statistical significance will be set at P 0.05 unless stated otherwise in the study.
Concerning the meta-analysis first outcomes (such as the COVID-19 incidence, ICU admission incidence and mortality incidence estimations), they will be assessed with Freeman-Tukey, the variance estimation with a DerSimonian and Laird method, and the Cochran Q and I2 method to explore statistical heterogeneity at a significance value of 0.10. For studies with heterogeneity, we used a random effect model, while for those without significant heterogeneity, the fixed-effect model was applied [14]
Concerning the other main outcomes (severity odd-ratios), relative risks/risk ratios/hazard ratios for individual studies will be combined using a random-effects meta-analysis (based on type of variables - KM orCox regressional model). Each one will be assessed individually.
Moreover, pooled and individual data of the included surveys were depicted by Forest Plots. Publication bias was checked by the Egger test [15].
Results
Literature search and study characteristics
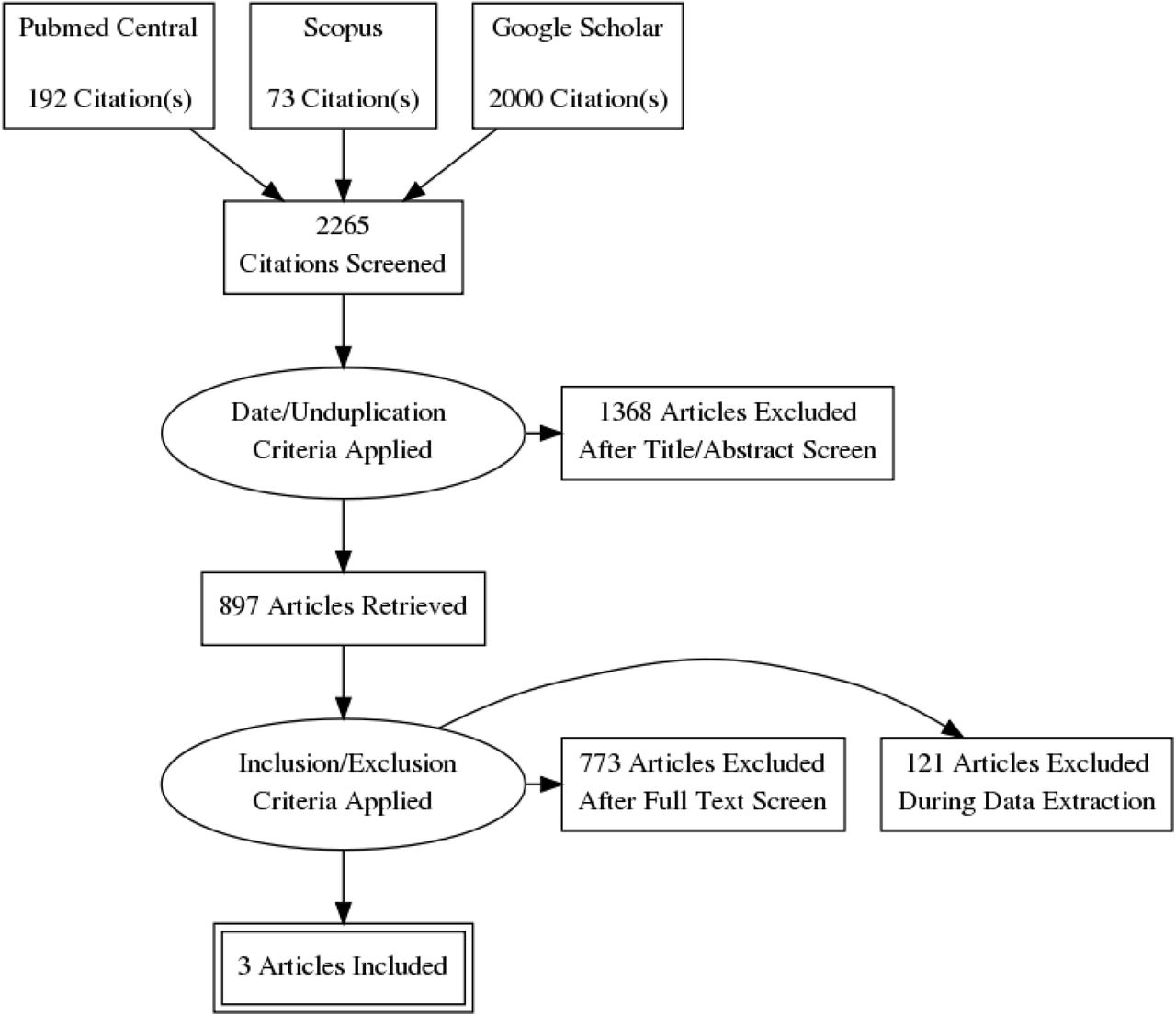
Figure 1 shows the PRISMA flowchart of the data selection process. The systematic search resulted in 2265 initial records, of which 871 were excluded as duplicates, 497 as irrelevant records due to the study date. 897 full-text articles were assessed for eligibility according to our inclusion criteria. Finally, 3 articles (3 studies) were found to be appropriate for quantitative synthesis [6,10,11] (Figure 1). The main characteristics of the studies are summarized in Table 1. The study designs mainly included cross-sectional methods. Publication bias was not significant according to the Egger’s test [15] (Table 2).
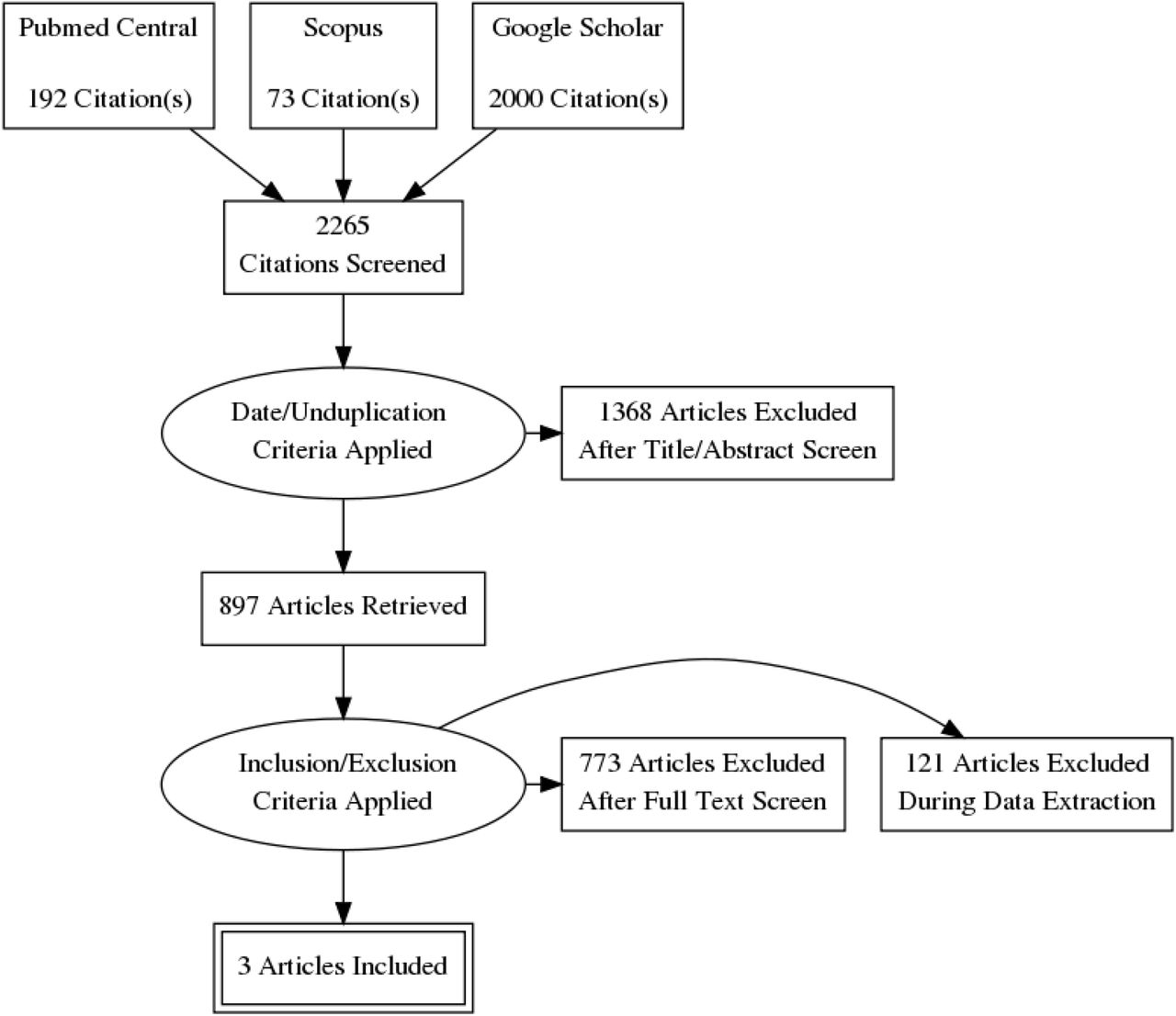
Flowchart of study identification and selection process
Main characteristics of the included studies
Computed results concerning the different studied outcomes
Main outcomes
COVID-19 incidence
Only one study [6] was included into the analysis of the COVID-19 incidence into beta-thalassemic carriers. Therefore, we obtained a reduction of the incidence with an Incidence Rate Ratio of 0.9250 but it was not significant with its p-value of 0.7479 and the trust interval [0.5752;1.4877] (Figure 1).
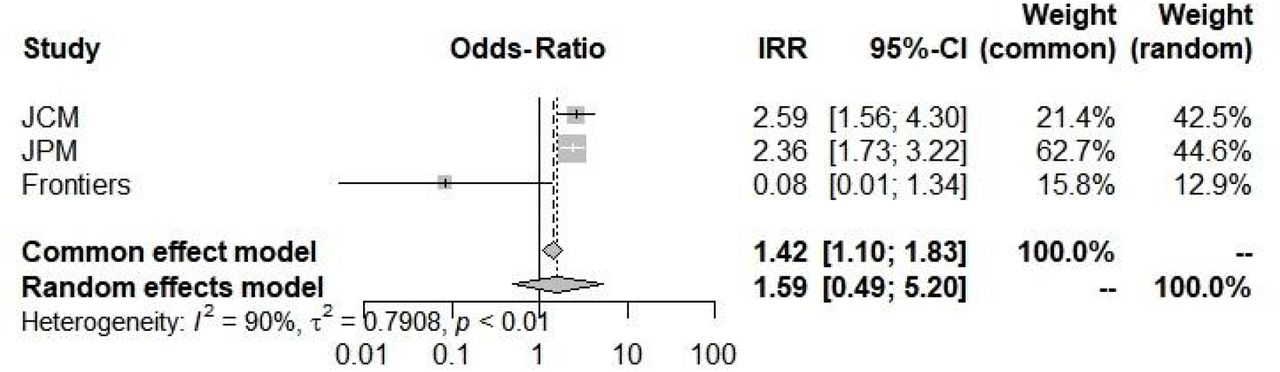
COVID-19 severity Odds-Ratio
All of the three studies [6,10,11] were included here to compute an Odds-Ratio of 1.5933 which suggested an increase of severity into the beta-thalassemic carriers compared to the normal population. However, it stays insignificant with a 0.4400 p-value and a [0.4884;5.11981] trust interval. The random-model effect was used due to the heterogeneity (I2=90.0%) (Figure 2). Furthermore, selected studies have a large heterogeneity I2=91.7%(71.0%-97.6%) but didn’t indicate the presence of funnel plot asymmetry according to the Egger’s test (Table 2).

Incidence Rate Ratio of COVID-19 into beta-thalassemia carriers
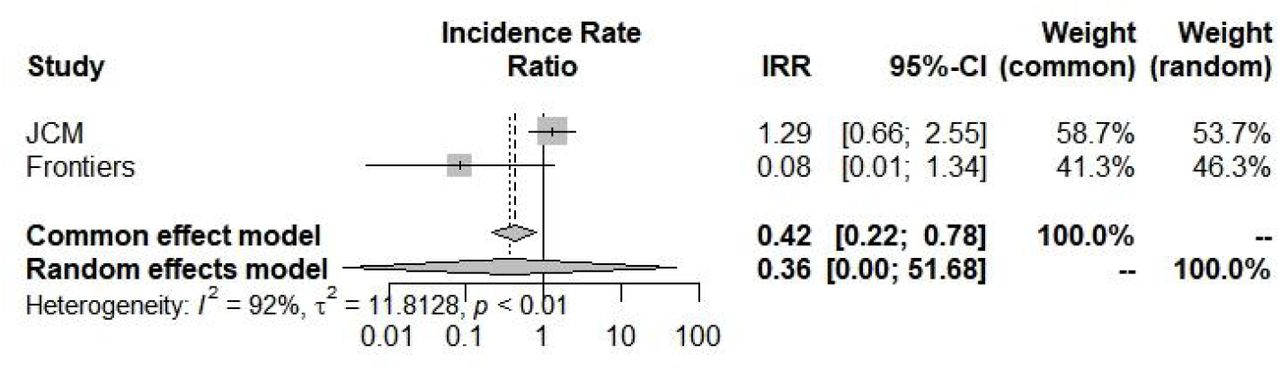
ICU admission incidence
Concerning ICU admission incidence, according to the random-effects model, we have computed an Incidence Rate Ratio of 0.3620(0.0025;51.6821) which suggests a large and insignificant decrease into the COVID-19 ICU admission concerning beta-thalassemia carriers compared to general population (Figure 4 and Table 2). Moreover, selected studies [6,10] have a broad heterogeneity I2=91.7%(71.0%-97.6%).

Odd-Ratios of COVID-19 severity into beta-thalassemia carriers

Incidence Rate Ratio of ICU admission for COVID-19 into beta-thalassemia carriers
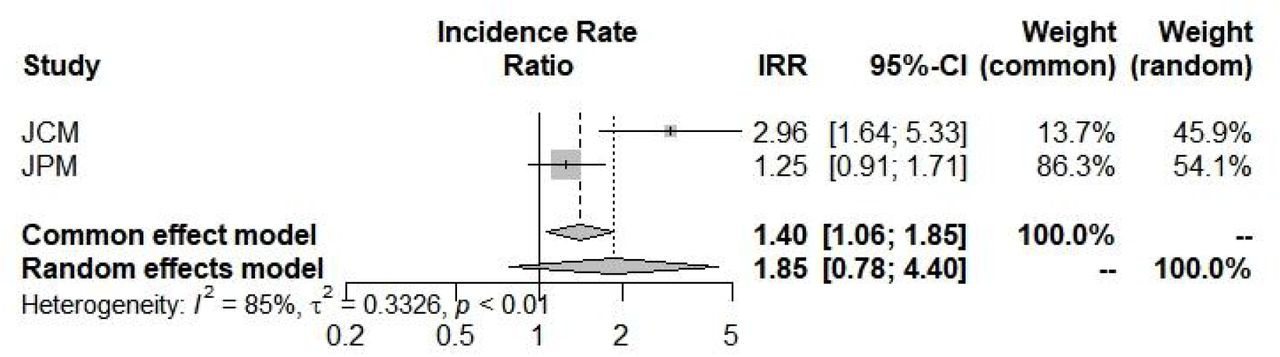
Mortality incidence rate
The last outcome was the mortality incidence rate : beta-thalassemia carriers have shown a larger but insignificant propensity 1.8542(0.7819;4.3970) to die with a COVID-19 infection (Figure 5 and Table 2). Selected studies [10,11] have a broad heterogeneity I2=85.1%(39.7%;96.3%).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mortality Incidence Rate Ratio for COVID-19 into beta-thalassemia carriers
Discussion
According to our systematic-review meta-analysis, beta-thalassemia carriers could be lessCOVID-19 affected than general population [IRR= 0.9250(0.5752;1.4877)], affected by COVID-19 with a worst severity [OR=1.5933(0.4884;5.1981)], less admissible into ICU [0.3620(0.0025;51.6821)] and more susceptible to die from COVID-19 or one of its consequences [1.8542(0.7819;4.3970)]. However, all of those results stay insignificant with a bad p-value (respectively 0.7479, 0.4400, 0.6881, 0.1610).
This non-significance could be mainly explained by the small number of included studies (n=3). That’s our first limitation. The second consists into studies type; indeed, we couldn’t assess a real incidence based on only one case-control study and two others selected studies were COVID-19 positive cohorts.Therefore, more datasets are needed to be published in order to obtain significant incidence rate ratios and odds-ratios.
In spite of those terrible limits, this systematic-review meta-analysis opens the way to the confirmation of a possible protection/immunity of beta-thalassemia carriers against COVID-19 concerning incidence and ICU admission markers [7,8]. However, more epidemiological studies are required in the aim to obtain a strong signal.
Data Availability
All data produced in the present work are contained in the manuscript
Footnotes
Transparency declaration: All authors declare no support from any organization for the submitted work other than that described above; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years; and no other relationships or activities that could appear to have influenced the submitted work.
Funding: There was no specific funding for this manuscript.
References



