
Abstract
Background Saliva is an attractive sample for detecting SARS-CoV-2 because it is easy to collect and minimally invasive. However, contradictory reports exist concerning the sensitivity of saliva versus nasal swabs.
Methods We recruited and followed close contacts of COVID-19 cases for up to 14 days from their last exposure and collected self-reported symptoms, mid-turbinate swabs (MTS) and saliva every two or three days. Ct values and frequency of viral detection by MTS and saliva were compared. Logistic regression was used to estimate the probability of detection by days since symptom onset for the two sample types.
Results We enrolled 58 contacts who provided a total of 200 saliva and MTS sample pairs; 14 contacts (13 with symptoms) had one or more positive samples. Overall, saliva and MTS had similar rates of viral detection (p=0.78). Although Ct values for saliva were significantly greater than for MTS (p=0.014), Cohen’s Kappa demonstrated substantial agreement (κ=0.83). However, sensitivity varied significantly with time relative to symptom onset. Early in the course of infection (days -3 to 2), saliva had 12 times (95%CI: 1.2, 130) greater likelihood of detecting viral RNA compared to MTS. After day 2, there was a non-significant trend to greater sensitivity using MTS samples.
Conclusion Saliva and MTS specimens demonstrated high agreement, making saliva a suitable alternative to MTS nasal swabs for COVID-19 detection. Furthermore, saliva was more sensitive than MTS early in the course of infection, suggesting that it may be a superior and cost-effective screening tool for COVID-19.
Key Points
Saliva is more sensitive in detecting symptomatic cases of COVID-19 than MTS early in the course of infection.
Saliva performs best in the pre-symptomatic period.
Saliva and MTS demonstrated high agreement making saliva a suitable and cost-effective COVID-19 screening tool.
Introduction
The U.S. Centers for Disease Control and Prevention (CDC) recommend the use of upper respiratory specimens, including but not limited to nasopharyngeal, mid-turbinate nasal, anterior nasal and saliva specimens for the initial diagnosis of COVID-19 [1]. Although nasopharyngeal swabs (NPS) are considered to be the standard for the detection of COVID-19 by most researchers, collection requires the use of trained professionals, can cause discomfort to the patients, and may pose greater risks to healthcare workers during sample collection [1–4]. Mid-turbinate swabs (MTS) are sometimes used as an alternative to NPS in an effort to reduce patient discomfort and occupational exposures to healthcare workers [4–6]. Compared to swab-based collection, saliva is even less invasive, more affordable, and can be self-collected with minimal or no supervision [1,7,8].
Existing studies focusing on the sensitivity of NPS compared to MTS, and NPS compared to saliva have produced contradictory results [2,4,9–11]. Few studies directly compare saliva and MTS specimens. Previous studies demonstrated that pre-symptomatic transmission results in higher secondary attack rates for both symptomatic and asymptomatic transmission [12,13]. However, most of the existing studies only looked at detection of symptomatic cases after symptom onset [2,4,9,10] and few looked at detection sensitivity starting with the pre-symptomatic period. Therefore, a study that conducts a direct comparison of MTS and saliva, including an assessment of sensitivity over time (starting during the pre-symptomatic period) is critical to identifying optimally sensitive methods for early detection and effective control of SARS-CoV-2 transmission.
The purpose of this study was to compare the sensitivity of MTS and saliva specimens for detecting SARS-CoV-2 by actively following close contacts of COVID-19 cases and collecting MTS and saliva samples for real-time reverse transcription polymerase chain reaction (RT-PCR) during their post-exposure quarantine period.
Methods
Study population
We analyzed MTS and saliva sample data from individuals who reported close contact with confirmed COVID-19 cases as part of the University of Maryland StopCOVID study [14] from May 2020 to April 2021.
Questionnaire and sample collection
Participants were followed every two or three days for up to 14 days from their last exposure or until SARS-CoV-2 was detected in their samples. If one or more of their screening samples became positive, results were confirmed by an appropriate clinical diagnostic test and they were recruited to participate in the exhaled breath aspect of the study that also involved the collection of saliva and MTS [14]. On each day of sample collection, participants answered an online questionnaire to update their current symptoms and medications. For those who reported having any symptom, they also reported their symptom onset date (i.e., “When did you begin to feel sick?”).
The symptoms checklist in the baseline and follow-up questionnaires, as previously described [14], included runny nose, stuffy nose, sneezing, sore throat, earache, malaise, headache, muscle and/or joint ache, sweat/feverish/chills, nausea, loss of appetite, vomiting, abdominal pain or diarrhea, chest tightness, shortness of breath, and cough. Participants self-reported for each of these 16 symptoms on a scale of 0 to 3 (0 = “no symptoms,” 1 = “just noticeable,” 2 = “clearly bothersome from time to time, but didn’t stop me from participating in activities,” 3 = “quite bothersome most or all of the time and stopped me from participating in activities”).
For saliva collection, participants were instructed to not eat or drink 30 minutes prior to the visit and then collect approximately 0.5-1 mL of saliva drooled into a plastic collection tube. For MTS collection, trained clinical staff inserted a mid-turbinate swab approximately 1.5-2 inches into one of the participants’ nostrils, rotated once, and then withdrawn. This procedure was repeated in the other nostril for a total of two MTS per participant per visit.
Laboratory analyses
Saliva samples were processed using the SalivaDirect method [8] as previously described [14]. Briefly, 50 µL of individual saliva samples were treated with Proteinase K (New England Biolabs), heated at 95°C for 5 minutes, and kept at 4°C. MTS from both nostrils were combined and processed as previously described [14]. Briefly, total nucleic acid was extracted from 200 µL of MTS with MagMax Pathogen RNA/DNA Kit (Applied Biosystems) on KingFisher Duo Prime (Thermo Fisher Scientific), following the manufacturers’ protocols. The sample was eluted in 50 µL of Elution Buffer and kept at 4 °C. MS2 phage was spiked in each heat-treated saliva sample and extraction to control for extraction and PCR failure. RT-PCR was set up on the same day; each reaction consisted of 1X TaqPath 1-Step Master Mix, No ROX, 1X TaqPath COVID-19 Real Time PCR Assay Multiplex (both from Thermo Fisher Scientific), and 10 µL of heat-treated saliva or eluted nucleic acids. Each PCR plate contained a positive control provided in the TaqPath COVID-19 Combo Kit (Thermo Fisher Scientific) and a no template control. A positive sample was defined as having Ct (cycle threshold) values < 40 for at least two out of three SARS-CoV-2 targets (ORF1ab, N gene, and S gene)[15]. The average Ct values of all positive targets were used in the following analyses.
Statistical analyses
We analyzed only paired same-day saliva and MTS samples to ensure the comparability of the two samples. Group comparisons were made between participants having a positive result for either sample and those with both samples being negative. Continuous variables (age and BMI) were compared using t-test, and categorical variables were compared using Chi-square test (sex and chronic respiratory illness) and Fisher’s exact test (age group, race, and ever smoker).
To compare the Ct values from saliva and MTS, we conducted paired t-test and Bland-Altman analysis, and calculated the coefficient of determination (i.e., R squared from linear regression) and Pearson correlation coefficient. The Chi-square test was used to explore the relationship between detection and sample types. Cohen’s Kappa was calculated to demonstrate the degree of agreement between the two sample types.
For participants with a positive saliva or MTS sample, we used a generalized additive logistic model [16] to estimate and plot the probability of having a positive result by days since symptom onset for the two sample types. We also created a plot using the LOESS (locally weighted smoothing) method with 95% confidence interval for the change of Ct values by days since symptom onset for the two sample types. Logistic regression was used to estimate the relative odds of detection of SARS-CoV-2 in saliva over specified intervals since symptom onset.
All the analyses were carried out using RStudio and R (version 4.0.4) [17].
Ethics statement
This study was approved by the University of Maryland Institutional Review Board and the Human Research Protection Office of the Department of the Navy. Electronically signed informed consent was obtained from all participants and questionnaire data were collected and stored with REDCap [18].
Results
We enrolled 58 individuals with known close contact with an active COVID-19 case. Contacts provided a total of 200 saliva and MTS pairs. The number of days of sample collection per participant ranged from one to seven. Among the contacts, 14 (24%) had at least one positive sample including 11 with both positive saliva and MTS samples over the course of follow-up. One contact had only positive saliva on 3 out of 3 samples (on days -3, 0, and 1 post symptom onset) and 2 had only positive MTS samples; one was positive on 2 of 2 swabs (on days 7 and 10) and one on 1 of 5 swabs (day 21, negative on days 14, 17, 19, and 24). Most of the positive participants (92.9%) were symptomatic, whereas only one (2.3%) participant from the test negative group reported symptoms. Symptomatic participants were enrolled -3 to 14 days since symptom onset and gave samples for up to 24 days from onset of symptoms. Symptoms were mild across the follow-up period. One participant had an oral temperature ≥ 38 °C at the time of sampling; three in total had temperatures ≥ 37.8 °C, and six in total had temperatures ≥ 37.5 °C; all were in the positive group. No other significant differences were identified between the positive and negative groups (Table 1).
Characteristics of the study population
Viral RNA detection in and agreement between saliva and MTS
Among 200 pairs of saliva and MTS samples we detected viral RNA in 32 (16%) of the saliva and 29 (14.5%) of the MTS samples. The frequency of detection was similar for both sample types (p=0.781) (Table S1). Cohen’s Kappa demonstrated substantial agreement (κ=0.83) with 26 (14%) positive and 165 (82.5%) negative sample pairs (Table 2). The 14 participants who became positive by either sample type during the follow-up period provided 41 saliva-MTS sample pairs, among which 71% of MTS and 78% of saliva samples were positive (Table S2), without respect to time since symptom onset. When focusing on positive participants, however, the agreement was weak (κ=0.43 for all and κ=0.42 for those who were symptomatic) (Table S3a and S3b).
Viral RNA detection in paired saliva and MTS samples from all participants (N=58)
Comparison of Ct values between saliva and MTS
Each RT-PCR reaction contained 10 µL of heat-treated saliva sample or RNA extracted from MTS. Assuming no loss in the process, each reaction represented 7.78 µL of saliva sample or 40 µL of the MTS eluate. The Ct values for paired samples were highly correlated (rho = 0.84, r2 = 0.74, Figure 1a). The Ct values for saliva were on average slightly but significantly greater than for MTS samples (mean difference = 0.64, p=0.01) among all 58 participants (Figure 1b and Figure S1), partially reflecting the difference in their input amounts.
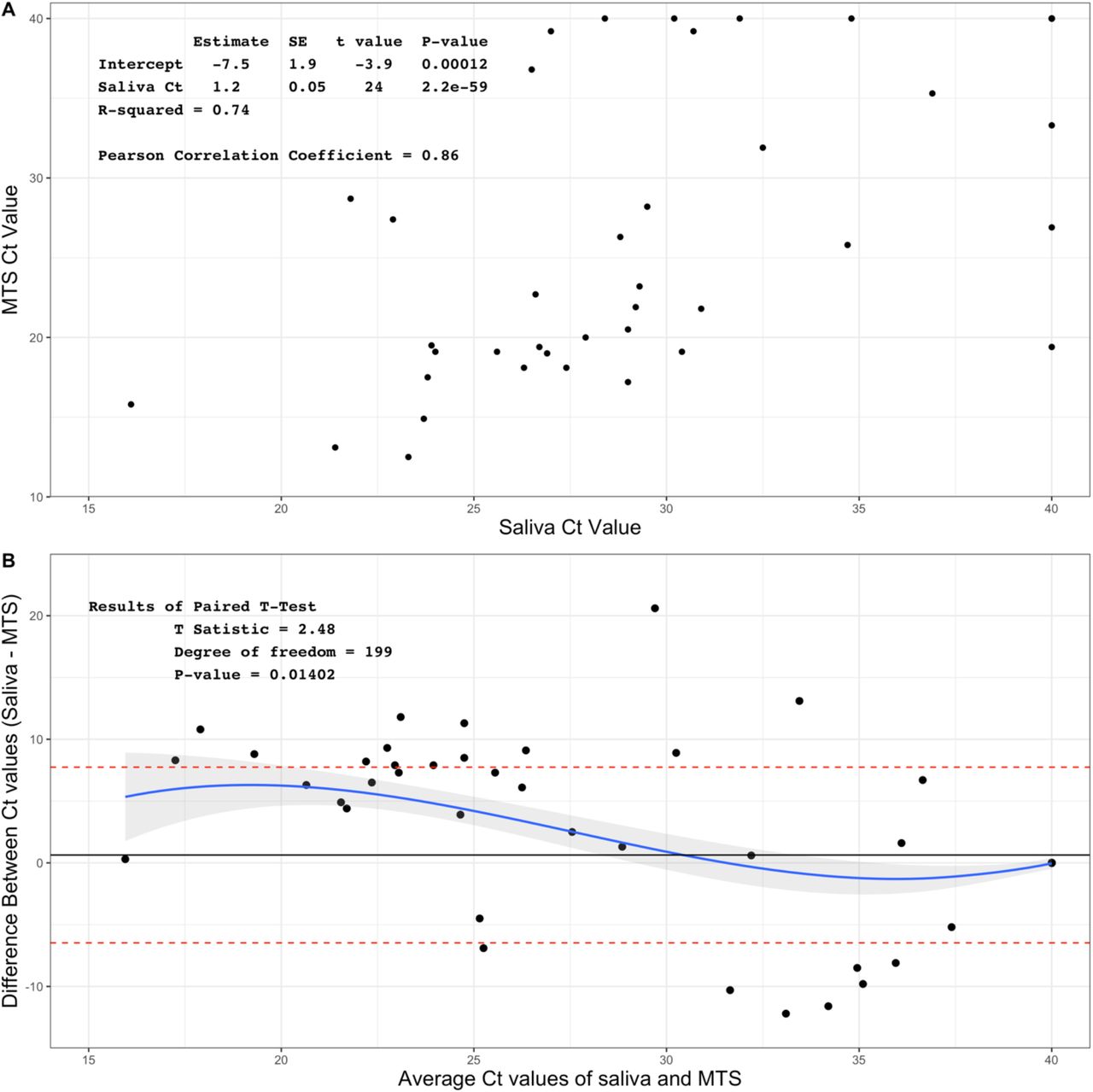
Association between Ct values of saliva and MTS samples among 58 participants and 400 samples
A. Scatter plot of Ct values of saliva and MTS
B. Bland-Altman plot for comparison of saliva and MTS
Relationship between days since symptom onset, sample types and probability of detection
The Ct values among the positive symptomatic participants increased over time (day -3 through 24), indicating decreasing viral load. Saliva tended to have lower Ct values compared to MTS from days -3 to 1.5, where MTS samples had lower Ct values thereafter (Figure 2A).

The change of Ct values and probability of testing positive by days since symptom onset. Data are for MTS and saliva samples from 13 participants who provided a total of 40 pairs of samples and had one or more samples positive for SARS-CoV-2 RNA.
A. Change of Ct values by days since symptom onset,
B. Probability of being tested positive by days since symptom onset estimated from a generalized additive logistic model.
Among symptomatic participants who had one or more positive saliva or MTS samples, the probability (sensitivity) of detecting viral RNA in saliva samples was 91% (10/11) from day -3 to day 2 (Table 3), was 89% (16/18) from day 3 through 8, and declined significantly thereafter (Figure 2B and Figure S2). The probability of detecting virus in MTS samples from day -3 through day 2 was lower 45% (5/11), was 94% (17/18) from day 3 through 8, and then dropped off again. Early in the course of infection (days -3 through 2) saliva had 12 times the odds of being positive compared to MTS (Odds ratio = 12, 95% CI: 1.2, 130). Although there was a trend toward greater sensitivity using MTS than saliva samples after day 2 post onset of symptoms, the difference was not statistically significant (Table 3).
Sensitivity of saliva and MTS and relative odds of detection of SARS-CoV-2 in saliva by day since symptom onset among 13 mildly symptomatic contacts of known cases
Asymptomatic case
Only one participant from our study population was an asymptomatic case. They provided one pair of saliva and MTS samples, both of which were positive, with an average Ct value of 25.8 for MTS and 34.7 for saliva (Table S4).
Discussion
Early in the course of infection, saliva was significantly more sensitive than mid-turbinate nasal swabs (MTS). We found that the optimal performance of saliva was in the pre-symptomatic period and was more sensitive than MTS before symptom onset. Several studies have shown that pre-symptomatic transmission plays a more important role than symptomatic and asymptomatic transmission in the spread of SARS-CoV-2 [12,13]. Furthermore, saliva tended to have lower Ct values compared to MTS from the pre-symptomatic period through the first few days post symptom onset. Together, these findings suggest that saliva may be the preferred sample for detecting SARS-CoV-2 early during the course of infection.
The CDC and the Infectious Disease Society of American recommendations for COVID-19 testing allow MTS, NPS, oral swabs, anterior nasal swabs, and saliva swabs as well as saliva.[1,19] Some studies have shown differences in the sensitivity between NPS and MTS. In older, more acutely ill populations, NPS appears to be more sensitive than MTS, especially later in the course of illness (greater than 7 days) [4,9]. In a study of ambulatory and symptomatic participants whose ages were more evenly distributed, NPS and MTS swabs were highly correlated with a mean of 7 days since onset of symptoms [20]. Congrave-Wilson et al., in agreement with the current study, found that saliva had the highest sensitivity in the first seven days post COVID-19 onset when using NPS as the reference [2]. Becker et al. compared the sensitivity of saliva and NPS for detecting COVID-19 in a convalescent cohort 8-56 days since first symptom and found that NPS performed better [21]. They also showed that saliva was about 30% less sensitive than NPS in a diagnostic cohort, however, days since symptom onset were not reported, so we cannot make direct comparison with our findings. Finally, a systematic review by Bastos et al. found that saliva had similar sensitivity to NPS and costs less [11].
Our findings have implications for improving public acceptance of COVID-19 testing, reducing the cost of mass COVID-19 screening, and improving the safety of healthcare workers who conduct testing. These findings are extremely important when considering large-scale screening of COVID-19 in schools and workplaces. In addition to its higher sensitivity in the early stage of the disease as demonstrated in our data, saliva has quite a few other advantages that make it an appealing screening tool. Saliva collection is less invasive and more acceptable to the general population [7,22]. One of the barriers hindering COVID-19 testing is people’s fear of nasal swabs due to misinformation [23]. Also, the discomfort brought by nasal swabs may also reduce people’s willingness to get tested regularly, especially among children [24,25]. With the use of saliva, screening in large groups with increased frequency may be more practicable. Saliva is cheaper than swab-based methods, especially if pooled samples are used [11,26]. Bastos et al. estimated that when sampling 100,000 individuals, using saliva saved more than $600,000 in comparison to using NPS [11]. These cost savings are especially important in the context of low resource settings.
Saliva collection is also safer for healthcare workers (HCWs). Amid the pandemic, one of the key concerns among HCWs is the occupational exposure to SARS-CoV-2 aerosols during some medical procedures [27]. The collection of nasal swabs introduces such exposure via the close interaction between patients and HCWs and by patients’ coughing and sneezing as a result of the procedures [28]. In contrast, saliva is the only upper respiratory specimen suggested by the CDC that can be self-collected without supervision [1] and hence protects HCWs from directly contacting the patients when the samples are being collected. Given all these advantages of saliva compared to NPS, our findings further support the use of saliva for large-scale screening, especially of pre-symptomatic patients.
The current study has several limitations. The contacts enrolled in this study who eventually tested positive for SARS-CoV-2 developed mild, and in some cases, transient infections. Some of these mild (low viral titer) infections would not have been detected by less frequent testing protocols and may not have posed a risk for onward transmission. The sample size of those who tested positive is relatively small. Only one asymptomatic case was identified in our study so we could not compare the sensitivity of the two types of samples among asymptomatic COVID-19 cases. The evidence for using saliva to detect asymptomatic cases was mixed in previous studies [2,10] and further studies are needed to clarify this issue.
In conclusion, the use of saliva is preferable for testing pre-symptomatic populations. It is more acceptable to people, which reduces barrier to testing. It is also more cost effective for individuals to collect their own saliva rather than using highly trained professionals to collect NPS and/or MTS. Finally, self-collected saliva samples eliminate the exposure to aerosols produced by sneezing, coughing and gagging of patients undergoing NPS/MTS.
Data Availability
Deidentified data and code for the accepted manuscript will be made available on github.
Funding
This work was supported by Prometheus-UMD, sponsored by the Defense Advanced Research Projects Agency (DARPA) BTO under the auspices of Col. Matthew Hepburn through agreement N66001-18-2-4015. This work was also supported by the National Institute of Allergy and Infectious Diseases Centers of Excellence for Influenza Research and Surveillance (CEIRS) Contract Number HHSN272201400008C, and the Centers for Disease Control and Prevention Contract Number 200-2020-09528. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position or policy of these funding agencies and no official endorsement should be inferred.
This work was also supported by a grant from the Bill & Melinda Gates Foundation, and a generous gift from The Flu Lab (https://theflulab.org). The funders had no role in study design, data collection, analysis, decision to publish, or preparation of the manuscript.
None of the authors have a potential conflicting interest or funding source.
Acknowledgements
We thank all the other members of the University of Maryland StopCOVID Research Group for their efforts in recruiting participants and sample collection and processing: Oluwasanmi Oladapo Adenaiye, Barbara Albert, P. Jacob Bueno de Mesquita, Yi Esparza, Aaron Kassman, Michael Lutchenkov, Dewansh Rastogi, Maria Schanz, Isabel Sierra Maldonado, Aditya Srikakulapu, Delwin Suraj, Faith Touré, Rhonda Washington-Lewis, Somayeh Youssefi, Stuart Weston, Matthew Frieman, Mara Cai, Ashok Agrawala. We also thank Dr. Jamal Fadul and his clinic in College Park, Maryland, for assistance in recruiting study participants.




{kind=link}
{kind=link}