
Abstract
Background A two-dose regimen of ChAdOx1 coronavirus disease 19 (Covid-19) vaccine with an inter-dose interval of three months has been implemented in many countries with restricted vaccine supply. However, there is limited evidence for the effectiveness of ChAdOx1 by dose in elderly populations in countries with high prevalence of the Gamma variant of severe acute respiratory syndrome 2 (SARS-CoV-2).
Methods We conducted a test-negative case-control study to estimate the effectiveness of ChAdOx1 vaccine in adults aged 60 years or older during a Gamma-variant-associated epidemic in São Paulo state, Brazil, between 17 January and 2 July 2021. Cases and matched test-negative controls were individuals, identified from surveillance databases, who experienced an acute respiratory illness and underwent SARS-CoV-2 RT-PCR testing. We used conditional logistic regression to estimate the effectiveness by dose against RT-PCR-confirmed Covid-19, Covid-19 hospitalization, and Covid-19-related death.
Results 61,164 individuals were selected into matched case-control pairs. Starting ≥28 days after the first dose, adjusted effectiveness of a single dose of ChAdOx1 was 33.4% (95% CI, 26.4 to 39.7) against Covid-19, 55.1% (95% CI, 46.6 to 62.2) against hospitalization, and 61.8% (95% CI, 48.9 to 71.4) against death. Starting ≥14 days after the second dose, the adjusted effectiveness of the two-dose schedule was 77.9% (95% CI, 69.2 to 84.2) against Covid-19, 87.6% (95% CI, 78.2 to 92.9) against hospitalization, and 93.6% (95% CI, 81.9 to 97.7) against death.
Conclusions Completion of the ChAdOx1 vaccine schedule afforded significantly increased protection over a single dose against mild and severe Covid-19 outcomes in elderly individuals during widespread Gamma variant transmission.
Introduction
Multiple vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the etiologic agent that causes coronavirus disease 19 (Covid-19), have been developed, proven efficacious, and deployed in mass vaccination campaigns1–3. Prominent among these vaccines, particularly in lower- and middle-income countries, is the viral vector vaccine, ChAdOx14. Randomized controlled trials (RCT) of ChAdOx1 delivered with a four-week inter-dose interval demonstrated 70.4% (95% CI, 54.8 to 80.6) efficacy against symptomatic Covid-19 in the period starting 14 days after the second vaccine dose4, and 64.1% 95% CI, (50.5-73.9) starting at 21 days following the first dose5. Based on measured immunogenicity and efficacy following a single dose, many countries have implemented a dose-spacing strategy that uses an inter-dose interval of up to 12 weeks to maximize vaccine coverage6 and has been endorsed by the World Health Organization (WHO)7.
The emergence of variants of concern (VOC) associated with decreased neutralization activity has created an urgent need to continuously monitor vaccine effectiveness8. Recent evidence has suggested reduced effectiveness of a single dose of ChAdOx1 against the Gamma and Delta VOCs9–11. Local Gamma VOC transmission has been observed in countries in Latin America which are using ChAdOx1 in mass vaccination12. A key question for these countries is the effectiveness of ChAdOx1 by dose against mild and severe Covid-19 outcomes, particularly in priority populations for vaccination such as the elderly.
The Gamma VOC was first detected in the city of Manaus13 and has been a driver of Covid-19 resurgence in Brazil and across South America14. The Brazilian national immunization program initiated a mass vaccination campaign in January 2021, which administered ChAdOx1 with three-month dose-spacing and provided an opportunity to evaluate vaccine effectiveness following one and two doses during a prolonged Gamma-variant-associated epidemic in São Paulo, the most populous state in Brazil.
Methods
Study setting
The study setting and design have been described in detail elsewhere15,16. São Paulo State has experienced three Covid-19 epidemic waves, the latest peaking in March 2021, with cumulatively over 3.89 million reported cases, 430,000 hospitalizations, and 130,000 deaths due to Covid-19 as of 9 July 202117 (Figure 1A). During the second and third waves, the Gamma variant increased in prevalence, reaching 80.2% from March to May 2021 among sequenced isolates, to become the predominant circulating variant in the state (Figure 1B). The State Secretary of Health of São Paulo (SES-SP) initiated a mass vaccination campaign on 17 January 2021, prioritizing healthcare workers and elderly populations. Two primary vaccines are being distributed: a two-dose regimen of ChAdOx1, separated by a 12-week interval, and a two-dose regimen of CoronaVac, separated by a two- to four-week interval18. As of 9 July 2021, 1.61 million doses of ChAdOx1 (1.11 million first doses and 0.51 million second doses) and 9.07 million doses of CoronaVac (5.62 million first doses and 3.45 million second doses) (Figure 1C) have been administered19.

Panel A shows the weekly case count of cases, hospitalizations, and deaths based on positive RT-PCR/Antigen tests for the age group ≥60 years. Panel B shows the monthly prevalence of main SARS-CoV-2 variants of concern among genotyped isolates in the GISAID database12 (extraction on July 7 2021). Prevalence was omitted for June and July due to low sample count. Panel C shows daily cumulative vaccination coverage for age group ≥60 years. Population estimates were obtained from national projections for 202037. Vertical lines, from left to right in each panel, show the dates that adults ≥90, 80-89, 70-79, 65-69 and 60-64 years of age in the general population became eligible for vaccination. The gray shaded area represents the study period.
We obtained individual-level information on demographic characteristics, comorbidities, SARS-CoV-2 testing, and Covid-19 vaccination by extracting information on 9 July 2021 from the SES-SP laboratory testing registry, the national surveillance databases for acute respiratory illness (ARI) and severe ARI, and the SES-SP vaccination registry. We retrieved information on SARS-CoV-2 variants from genotyped isolates deposited in the GISAID database12. The protocol, including statistical analysis plan, further details of study design, and power calculations, is publicly available (https://github.com/juliocroda/VebraCOVID-19). The study was approved by the Ethical Committee for Research of Federal University of Mato Grosso do Sul (CAAE: 43289221.5.0000.0021).
Study population and design
The study population was adults ≥60 years of age who had a residential address in São Paulo State and complete and consistent information between data sources on age, sex, residence, and vaccination and testing status and dates. We selected cases who had an ARI, received a positive SARS-CoV-2 RT-PCR test during the study period of 17 January 2021 to 2 July 2021 with sample collection date within 10 days after symptom onset, and without a positive SARS-CoV-2 RT-PCR test in the previous 90 days. We selected test-negative controls who had an ARI, received a negative SARS-CoV-2 RT-PCR test during the study period with sample collection date within 10 days after symptom onset, and without a positive SARS-CoV-2 RT-PCR test in the previous 90 days or following 14 days. Cases and controls who had received a dose of another Covid-19 vaccine before their RT-PCR test were excluded. We matched one control to each case by date of testing (±3 days), age (in 5-year bands), sex, self-reported race (brown, black, yellow, white, or indigenous)20, municipality of residence, and prior ARI (defined as at least one previous symptomatic event that was reported to surveillance systems between 1 February 2020 and 16 January 2021).
Outcomes and Covariates
We estimated the effectiveness of ChAdOx1 against the primary outcome of symptomatic Covid-19 during the period ≥28 days after a single vaccine dose, and 0-13 and ≥14 days after two vaccine doses. Furthermore, we estimated the effectiveness of a single dose during the period 14-27 days after the first dose to understand the onset of protection, and in the period 0-13 days, when the vaccine has no or limited effectiveness21,22. An association during this period may serve as a negative control exposure to detect unmeasured confounding in the effectiveness estimate in later time periods23. In a secondary analysis, we estimated the vaccine effectiveness following the first dose in the time windows 28-41 days, 42-55 days, and ≥56 days separately. The reference group for vaccination status was individuals who had not received a first vaccine dose before the date of sample collection.
In addition, we estimated vaccine effectiveness against secondary outcomes of Covid-19 hospitalization, ICU admission with Covid-19, mechanical ventilation for Covid-19, and Covid-19-related death. We estimated single-dose effectiveness during the period ≥28 days after the first dose for all outcomes within subgroups defined by age (60-69 years vs. ≥70 years), sex, number of chronic comorbidities (none vs. at least one), reported cardiovascular disease, reported diabetes, and region of residence (“Grande São Paulo” health region vs. others).
Statistical analysis
We performed conditional logistic regression to estimate vaccine effectiveness for each time window following vaccination. Multivariable models were adjusted for the number of reported comorbidities (categorized as none, one-two, and at least three), previous positive SARS-CoV-2 RT-PCR or antigen test, and age as a continuous variable because we used 5-year age bands as a matching factor. For each outcome, we selected matched pairs in which cases had the outcome of interest, and fit the model described above to each subset.
Our protocol specified that we would conduct proposed analyses after achieving ≥80% power to identify a vaccine effectiveness of 40% against symptomatic Covid-19 ≥28 days after a single dose of ChAdOx1, and 80% power to identify 50% effectiveness of two doses ≥14 days after the second dose. The power was estimated by fitting conditional logistic regressions on 1,000 simulated datasets. After extracting the surveillance databases on July 9 2021 and generating matched case-control pairs, we determined that the power of the study was >99.8% for each analysis and performed the pre-specified analyses. All analyses were performed in R, version 4.0.2.
Results
Study population
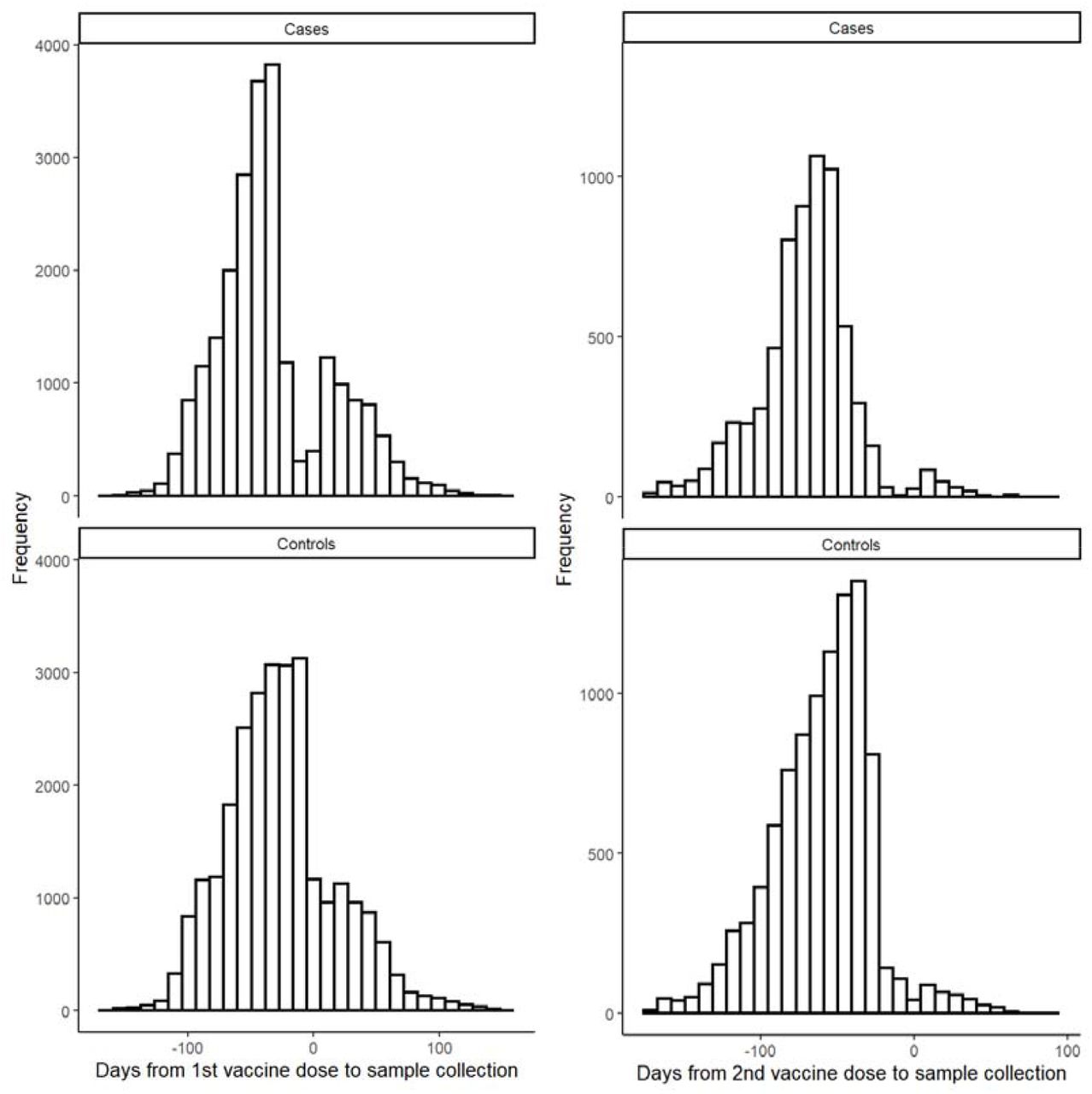
Among 137,744 individuals eligible for selection as a case or control (Figure 2), 61,164 (44.4%) who provided 61,360 RT-PCR test results were selected into 30,680 matched case and control pairs. Table 1 shows the characteristics of eligible individuals and matched cases and controls. Supplementary Tables 1-3 show the distribution of matched pairs according to vaccination status of cases and controls at the time of RT-PCR testing for the analysis of symptomatic Covid-19, hospitalization, and death. Supplementary Figure 1 shows the timing of discordant pair enrollment, while Supplementary Figure 2 shows the distribution of intervals between administration of vaccine doses and RT-PCR testing.

Flowchart of the identification of the study population from surveillance databases and selection of matched cases and controls.
Characteristics of adults ≥60 years of age who were eligible for matching and selected into case-test negative pairs.
Vaccine effectiveness
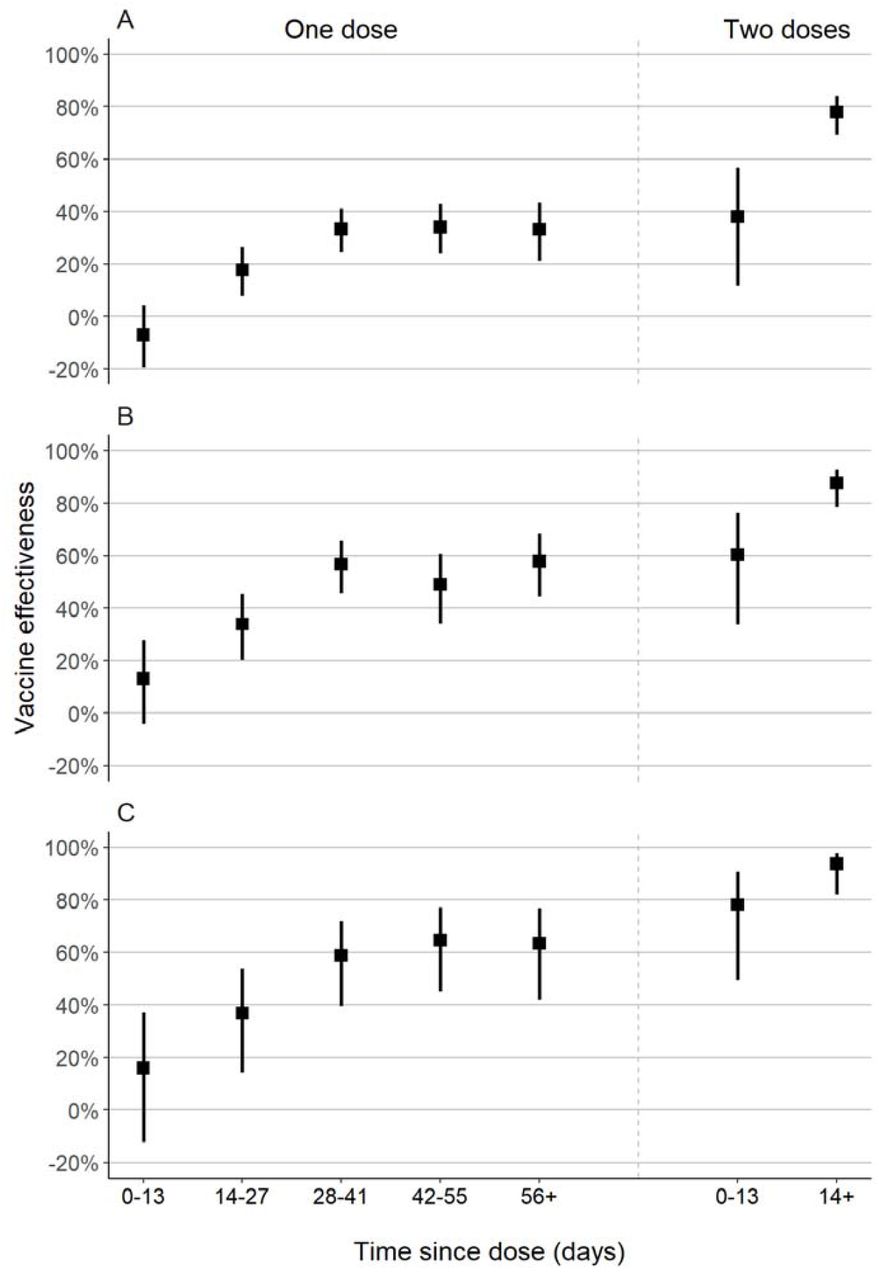
The adjusted effectiveness of a single dose of ChAdOx1 against symptomatic Covid-19 was 33.4% (95% CI, 26.4 to 39.7) for the period ≥28 days after administration of the first dose (Table 2). The effectiveness of a single dose reached a plateau after 28 days (Figure 3), with no increase observed in later time periods. The adjusted effectiveness of the full two-dose schedule against symptomatic Covid-19 was 38.1% (95% CI, 11.9 to 56.5) in the period 0-13 days after administration of the second dose, and 77.9% (95% CI, 69.2 to 84.2) in the period ≥14 days after administration of the second dose. The estimated effectiveness in the period 0-13 days following the first dose, which serves as a negative control exposure to indicate bias, was -7.1% (95% CI, -19.6 to 4.1). Increasing number of comorbidities were significantly associated with increased odds of Covid-19 in the adjusted analyses (aOR 1.54, 95% CI, 1.49 to 1.60, for one-two comorbidities, and aOR 2.20, 95% CI, 1.98 to 2.45, for three or more comorbidities compared to no comorbidities). A previous positive SARS-CoV-2 viral test was associated with lower odds of Covid-19 (aOR 0.65, 95% CI, 0.37 to 1.17).
Adjusted effectiveness of a ChAdOx1 against clinical Covid-19 outcomes in adults ≥60 years of age.
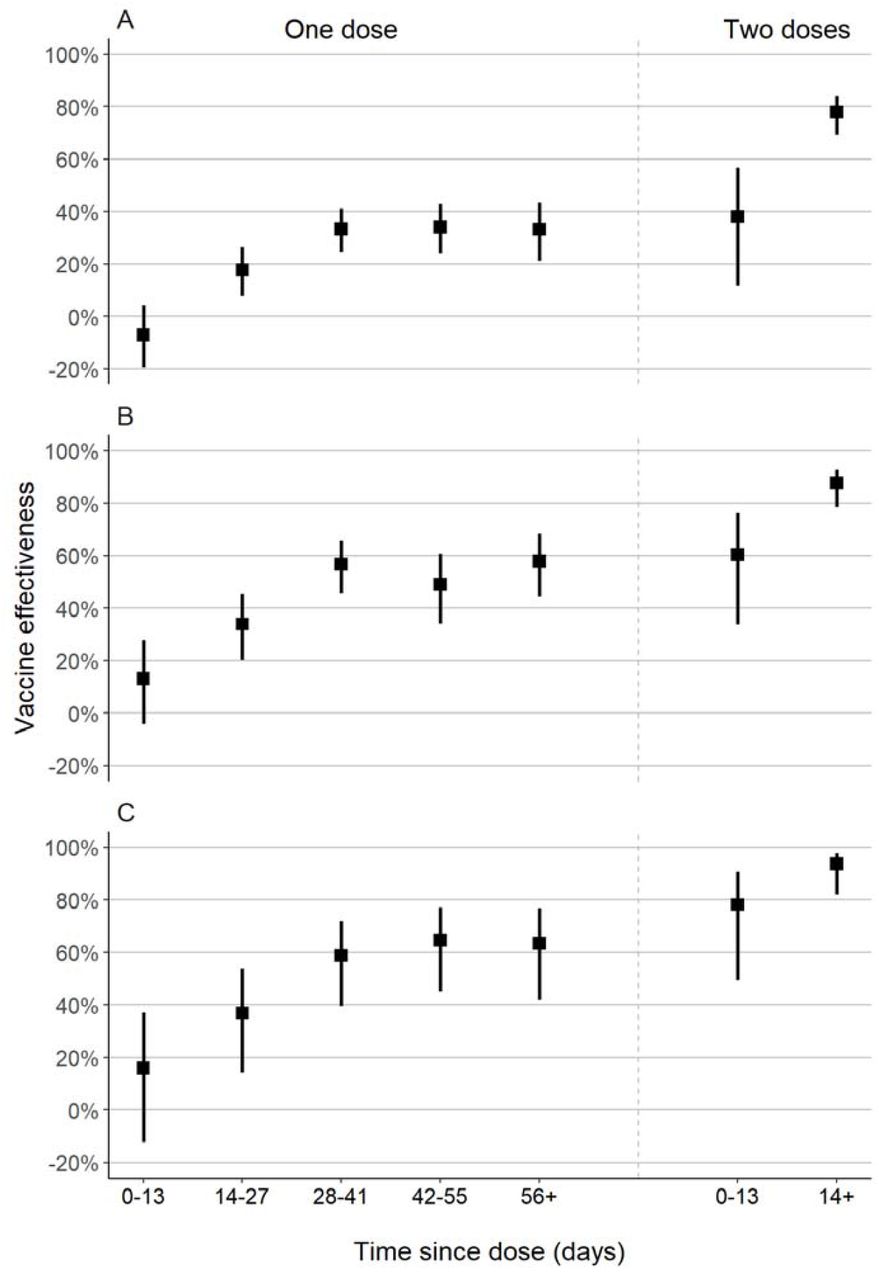
Adjusted vaccine effectiveness of one and two doses of ChAdOx1, by time since vaccination, against symptomatic Covid-19 (A), Covid-19 hospitalization (B), and Covid-19-related death (C)
In the period starting 28 days after the first dose, the adjusted effectiveness of a single dose was 55.1% (95% CI, 46.6 to 62.2) against hospitalization, and 61.8% (95% CI, 48.9 to 71.4) against death (Table 2). The adjusted effectiveness of the two-dose schedule starting 14 days after the second dose was higher: 87.6% (95% CI, 78.2 to 92.9) against hospitalization, and 93.6% (95% CI, 81.9 to 97.7) against death (Table 2). Effectiveness against ICU admission and mechanical ventilation was similar to effectiveness against hospitalization (Table 2). In general, vaccine effectiveness in the “bias-indicator” period 0-13 days after the first dose was low.
The effectiveness of a single dose against symptomatic Covid-19 was lower among those with reported diabetes (24.2%, 95% CI, 11.0 to 35.4) than in those without reported diabetes (35.3%, 95% CI, 28.3 to 41.6) (pinteraction = 0.03) (Supplementary Table 4). Similarly, effectiveness was lower among those with at least one reported comorbidity compared to those without a reported comorbidity (Supplementary Table 4). Finally, single-dose effectiveness against hospitalization and death was lower among older individuals, but these analyses lacked sufficient power (Supplementary Table 5).
Discussion
A key priority for mass vaccination campaigns is to reduce morbidity and mortality in the elderly and other vulnerable populations, especially in the context of limited vaccine supply and VOC emergence. Our test-negative case-control study found that the two-dose schedule of ChAdOx1 in the elderly had robust effectiveness against Covid-19 and severe outcomes during a Gamma-variant-associated Covid-19 epidemic in the period starting 14 days after administration of the second dose: 77.9% (95% CI, 69.2 to 84.2) against symptomatic Covid-19, 87.6% (95% CI, 78.2 to 92.9) against Covid-19 hospitalization, and 93.6% (95% CI, 81.9 to 97.7) against Covid-19-related death. However, a single dose of ChAdOx1 in adults 60 years of age had effectiveness of 33.4% (95% CI, 26.4 to 39.7) against symptomatic Covid-19, 55.1% (95% CI, 46.6 to 62.2) against hospitalization, and 61.8% (95% CI, 48.9 to 71.4) against death. Additionally, no clinically significant effectiveness was detected within 28 days of administration of the first dose.
Randomized controlled trials of ChAdOx1 conducted in multiple countries reported pooled vaccine efficacy of 70.4% (95% CI, 54.8 to 80.6) against symptomatic Covid-19 in the period starting 14 days after the second vaccine dose, and 100% (95% CI, not calculated) against hospitalization for Covid-194. A secondary analysis estimated efficacy of 64.1% (95% CI, 50.5 to 73.9) starting at 21 days following the first dose5. Subsequent observational studies have largely supported the effectiveness of ChAdOx1 against symptomatic Covid-19 and hospitalization in elderly populations21,22,24–26. In addition, these studies provided further evidence for the effectiveness of a single dose of ChAdOx1 against infection with SARS-CoV-226, symptomatic Covid-1921 and hospitalization22,24,25, with onset of clinical effectiveness occurring between 21 and 28 days.
Emerging VOCs have been associated with reduced neutralization by serum from individuals who have been infected with non-VOC strains, and vaccinated27,28, including those who are elderly29, raising the possibility of decreased effectiveness. An RCT of ChAdOx1 conducted in South Africa found no effectiveness, albeit with low precision, of the two-dose vaccine schedule against mild-to-moderate Covid-19 caused by the Beta VOC30. Further evidence from observational studies has suggested reduced vaccine effectiveness against symptomatic disease for a single dose of vaccine against Gamma: 48% (95% CI, 28 to 63) after 14 days for ChAdOx111, 61% (95% CI, 45 to 72) after 21 days for mRNA vaccines31, and 11% (95% CI, -4 to 23) after 14 days for CoronaVac16. However, the complete BNT162b2 schedule has shown robust effectiveness against the Gamma VOC11, and a complete schedule of CoronaVac was effective against mild and severe outcomes in settings of widespread Gamma VOC transmission16. These findings are consistent with reduced effectiveness of a single dose of BNT162b2 and ChAdOx1 against the Delta VOC observed in the UK9,10. Our study adds to this evidence base by estimating single-dose effectiveness of ChAdOx1 over the duration of the inter-dose interval, and demonstrating the substantial benefit of the second dose in elderly individuals in a setting of high Gamma VOC prevalence.
Our findings have implications for vaccination policy in countries experiencing Gamma-variant-associated Covid-19 epidemics. Several countries, including Brazil, are administering the two-dose schedule of ChAdOx1 with a 12-week gap between doses to increase coverage, as WHO currently recommends7. The public health benefits of dose-spacing strategies were predicated on robust effectiveness following a single dose32–34. In the specific context of VOC emergence and spread, national programs should consider the reduced vaccine effectiveness of a single dose against the Gamma and Delta VOCs in the elderly, together with vaccine supply limitations, speed of vaccination, and logistics, when quantifying the benefits of dose-spacing strategies.
The design of this study lends strength to our findings. The six-month period during which the Gamma variant-associated epidemic and vaccination campaign occurred provided the opportunity to obtain robust estimates of single-dose effectiveness beyond 28 days, and effectiveness of the completed schedule in the same population for direct comparison. The test-negative design reduces bias caused by healthcare-seeking behavior35, and we have controlled for additional sources of bias by matching on several predictors of healthcare access and utilization and Covid-19 risk36. We used a negative control exposure of vaccine effectiveness within 13 days of receiving the first dose to detect bias in our estimates, and found limited measured effectiveness in this period. This null association suggests that unvaccinated and vaccinated individuals were similar in their underlying risk of Covid-19 and healthcare-seeking behavior23. The large sample size allowed us to produce robust estimates even against rare outcomes such as death and to perform subgroup analyses.
Our study has several limitations. We could not estimate the effectiveness against Gamma and non-Gamma Covid-19 cases within this study population, as we did not have access to individual-level genetic data on the virus. In addition, there was likely a proportion of the population that was seropositive without having received a previous positive RT-PCR or rapid antigen test before the study period. These individuals, even if unvaccinated, would be protected from reinfection by natural immunity, thus causing downward bias in our vaccine effectiveness estimates. Controls for the analysis of severe outcomes included controls with mild ARI, who may have had better access to healthcare, leading to bias in our estimates of effectiveness against severe outcomes. Finally, our results cannot be extrapolated to younger populations.
In a setting of widespread transmission of the SARS-CoV-2 Gamma variant, in the general population of elderly individuals, completion of the two-dose schedule of ChAdOx1 afforded a significant increase in protection against mild and severe Covid-19 outcomes compared to a single dose.
Data Availability
Deidentified databases as well as the R codes will be deposited in the repository https://github.com/juliocroda/VebraCOVID-19
Author contributions
All authors conceived the study. OTR, MDTH and MD completed analyses with guidance from JRA, DATC, AIK, and JC. MSST, OFPP, OTR and MDTH curated and validated the data. OTR and MDTH wrote the first draft of the manuscript. TLD, RCP, OFPP, EFMV, MA, RS, JCG, WNA provided supervision. All authors contributed to, and approved, the final manuscript. JC is the guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Declaration of interests
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethics approval
The study was approved by the Ethical Committee for Research of Federal University of Mato Grosso do Sul (CAAE: 43289221.5.0000.0021).
Data sharing
Deidentified databases as well as the R codes will be deposited in the repository https://github.com/juliocroda/VebraCOVID-19
Role of the funding source
All funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The Health Secretary of State of São Paulo and PRODESP reviewed the data and findings of the study, but the academic authors retained editorial control. OTR, MDTH, MSST, and JC had full access to de-identified data in the study and OTR and MDTH verified the data, and all authors approved the final version of the manuscript for publication.
Supplementary appendix
Supplement to: Effectiveness of the ChAdOx1 vaccine in the elderly population during a Gamma variant-associated epidemic of Covid-19 in Brazil
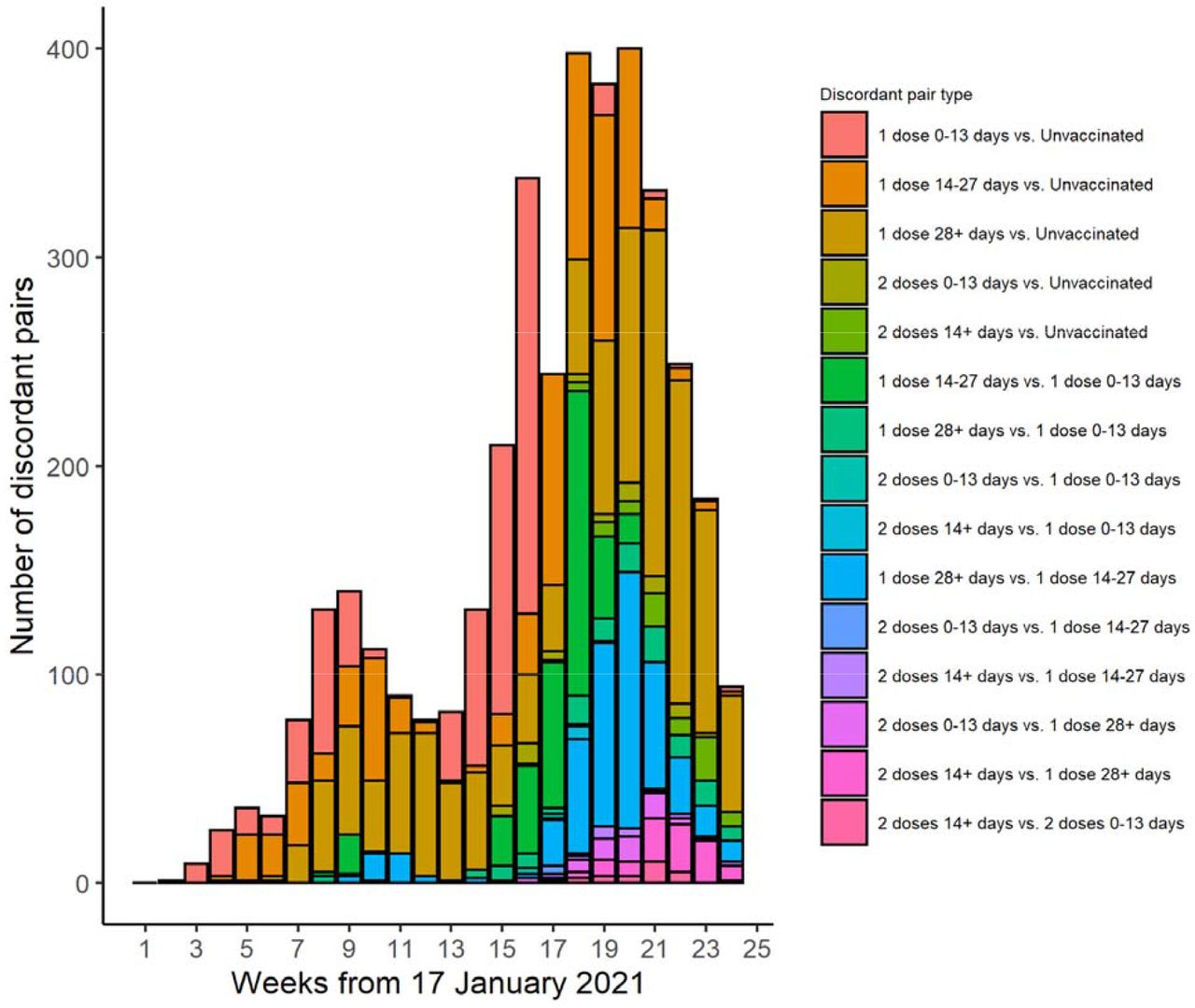
Timing of enrolment of discordant case-control pairs by vaccination category

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Timing of RT-PCR sample collection date relative to 1st (left column) and 2nd (right column) vaccine dose date, among cases (top row) and controls (bottom row) who were vaccinated during the study period.
Distribution of concordant and discordant matched case-control pairs.
Distribution of concordant and discordant matched case-control pairs with hospitalized cases.
Distribution of concordant and discordant matched case-control pairs with cases who died.
Adjusted single-dose vaccine effectiveness against symptomatic Covid-19, ≥28 days after first dose, within subgroups
Adjusted one- and two-dose effectiveness against Covid-19 hospitalization and Covid-19-related death by age
Acknowledgements
We are grateful for the Pan American Health Organization’s support and the São Paulo State in making the databases available for analysis. JC is supported by the Oswaldo Cruz Foundation (Edital Covid-19 – resposta rápida: 48111668950485). OTR is funded by a Sara Borrell fellowship (CD19/00110) from the Instituto de Salud Carlos III. OTR acknowledges support from the Spanish Ministry of Science and Innovation through the Centro de Excelencia Severo Ochoa 2019-2023 Program and from the Generalitat de Catalunya through the CERCA Program.
References



