
Abstract
Healthcare workers have had the longest and most direct exposure to COVID-19 and consequently may suffer from poor mental health. We conducted one of the first repeated multi-country analysis of the mental wellbeing of medical doctors (n=5,275) at two timepoints during the COVID-19 pandemic (June 2020 and November/December 2020) to understand the prevalence of anxiety and depression, as well as associated risk factors. Rates of anxiety and depression were highest in Italy (24.6% and 20.1%, June 2020), second highest in Catalonia (24.6% and 17.4%, June 2020), and lowest in the UK (11.7% and 13.7%, June 2020). Across all countries, higher risk of anxiety and depression symptoms are found among women, individuals below 60 years old, those feeling vulnerable/exposed at work, and those in poor health. We did not find systematic differences in mental health measures between the two rounds of data collection, hence we cannot discard that the mental health repercussions of the pandemic are persistent.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has affected many individuals both directly and indirectly, disrupting routines and introducing new stressors [1]. Recent studies have shown that the pandemic has unequal effects on the psychological wellbeing of individuals, with women, younger individuals, and ethnic minorities being disproportionately affected [2,3]. Effects also vary by occupational groups as certain jobs expose workers more directly to the disease [4–6]. The mental wellbeing of healthcare workers has been particularly affected by the pandemic [7–10].
Healthcare workers have been directly involved in the management of COVID-19 patients since the beginning of the pandemic. Drawing on the experiences of healthcare workers during the 2003 SARS outbreak, various mental health risk factors have been identified: lack of personal protective equipment (PPE), overwhelming workload, lack of institutional support, and fear of infecting others [11–14]. Several studies have documented high rates of anxiety and depression symptoms among healthcare workers during the COVID-19 pandemic, with various risk factors such as fear of infection being identified as important [7,8]. The majority of the studies are from China [8,9,15] and a handful document similar patterns in other regions [10].
Various local and national mental health institutions around the world have begun to offer psychological assistance to those in need, with some services targeted specifically at healthcare workers [16–19]. Poor mental health among healthcare workers may have downstream effects on patients via worsened attention span, cognitive function, and clinical-decision making [10]. Providing such assistance to healthcare workers requires understanding the state of their mental wellbeing, factors associated with mental health symptoms, and how these outcomes and factors vary across time and countries.
This study provides one of the first repeated cross-country analyses of mental wellbeing among healthcare workers during the COVID-19 pandemic. Our sample comprises medical doctors working in Catalonia, Italy, or the UK in June (first data collection round) and November/December 2020 (second data collection round). In contrast to existing studies, these data allow us to quantify the prevalence of and risk factors associated with anxiety and depression symptoms across countries and to examine these outcomes at two timepoints. While previous studies have investigated heterogeneous samples of healthcare workers, our analysis focuses on medical doctors. The results of our study can inform how to protect and promote the mental wellbeing of medical doctors in current and future pandemics.
Methods
We conducted an anonymous survey, The Healthcare Workers Survey, approved by the University of Exeter Business School Research Ethics Committee (eUEBS003024). Informed written consent was provided by all survey participants prior to their participation. Participants understood that they may withdraw from the study at any time. We followed the reporting guidelines of the American Association for Public Opinion Research (S1 Appendix, Table S1).
The study is a repeated cross-sectional survey among members of 6 medical organizations: COMB (Barcelona Medical Council) and COMG (Girona Medical Council) in Catalonia (Spain), Anaao-Assomed (Union of physicians and healthcare executives) and FIMMG (Union of general practitioners) in Italy, as well as RCPSG (Royal College of Physicians and Surgeons of Glasgow) and RCSEd (Royal College of Surgeons of Edinburgh) in the UK.
Due to different membership rules, members of the Catalan and Italian institutions work in Catalonia and Italy, while the Scottish institutions have members who work in different parts of the UK (S1 Appendix, Table S2). The survey was designed in Qualtrics and was distributed via email by the corresponding institutions.
Participants
Our data collection relied on the mailing lists of the respective medical organizations. The COMB invited 5,062 members in June and November 2020 (19.9%), focusing on those with medical license numbers ending in 1 or 2. This random sampling was chosen to avoid over-burdening members, given other surveys were taking place at the same time. The other institutions sent invitations to all members. The COMG invited 3,120 members in June and November 2020. Similarly, the Anaao-Assomed invited 23,379 members, and the FIMMG invited 17,686 members in June and December 2020. The RCPSG invited 3,990 members in June 2020 and 4,300 members in November 2020 (S1 Appendix, Figure S1). The RCSEd invited 4,992 members in June 2020 and 4,912 members in November 2020 (S1 Appendix, Figure S2). In the first round, out of approximately 55,000 invited members, the final sample size was 3,025 (5.5%). In the second round, the final sample size was 2,250 (4.1%). Table S3 (S1 Appendix) documents the response rates across institutions.
Outcomes and covariates
The outcomes of the study are anxiety and depression symptoms. Anxiety is measured with the Generalized Anxiety Disorder (GAD-7) questionnaire, a seven-item self-report anxiety questionnaire designed to assess health status during the previous two weeks [20,21]. It has been validated as an anxiety screening tool and severity measure in different populations [20,22–24]. GAD-7 scores range from 0 to 21. When used as a binary anxiety indicator, a score of 10 is the recommended threshold for referral for further evaluation [20,25]. Using this threshold, the GAD-7 has sensitivity of 89% and specificity of 82% for generalized anxiety disorder [20,25].
Depression is measured with the depression module of the Patient Health Questionnaire (PHQ-9), which focuses on the nine diagnostic criteria for DSM-IV depressive disorders [26]. It is a useful tool to assist clinicians in diagnosing depression and a reliable and valid measure of depression severity [26,27]. It has been validated in a variety of populations [21,28,29]. PHQ-9 scores range from 0 to 27. When used as a binary depression indicator, 10 is the recommended cut-off point. Using this threshold, the PHQ-9 has sensitivity and specificity of 88% for major depression [26,28].
The following covariates were included in our analysis: demographic characteristics (sex, age, household composition), survey round (June vs. November/December 2020), perceptions about workplace safety (availability of PPE, reported feelings of vulnerability and exposure, perceived workplace concerns about workers safety), COVID-19 exposure (symptoms, directly treating COVID-19 patients, helping with COVID-19 tasks, healthcare worker deaths due to COVID-19 in the workplace), and health and lifestyle factors (self-reported health status, underlying health condition, working over 40 hours in the previous week, smoking behavior, whether the respondent had a flu vaccine this season). Table S4 (S1 Appendix) describes all these variables. The replication data and code will be available at https://sites.google.com/site/climentquintanadomeque/healthcare-workers-survey.
Statistical analysis
First, we described the demographic characteristics of our respondents. Second, we calculated the prevalence of anxiety and depression symptoms by country over time. Third, we calculated the prevalence of anxiety and depression by sex and age in each country. Fourth, we estimated the perceptions of workplace safety and exposure to COVID-19 by country over time. Finally, we used multivariable logistic regression to estimate odds ratios (ORs) for the association between anxiety (and depression) symptoms and the aforementioned covariates, controlling for occupational categories (e.g. in the UK: Consultant, SAS doctor, Specialty registrar, Junior doctor core training, Junior doctor foundation year, General practitioner, General practitioner trainee) and institutional fixed effects (i.e. COMB, COMG, Anaao-Assomed, FIMMG, RCPSG, RCSEd). Stata statistical software version 16.1 (StataCorp) was used for statistical analyses. P-values were 2-sided and statistical significance was set at p<0.05. Data were analyzed from March 4 to June 4, 2021.
Results
Table 1 presents demographic characteristics of the participants by medical organization and round. The total number of respondents is as follows: 1,849 in Catalonia (n=876 in round 1, n=973 in round 2); 2,574 in Italy (n=1,637 in round 1, n=937 in round 2); 852 in the UK (n=512 in round 1, n=340 in round 2). Table S5 (S1 Appendix) documents the number of observations from the raw data to the study sample. The percentage of respondents who were women and men differs across countries. In Italy, it is similar (50%). However, over 64% of respondents were women in Catalonia and below 35% in the UK. The age distribution of respondents also varies by country. The percentage of respondents younger than 60 years is over 83% in the UK, below 73% in Catalonia and below 60% in Italy. Both the monthly COVID-19 case and rates increased between the two data collection rounds. COVID-19 cases per 100,000 increased from 33.3 (June 2020) to 809.6 (November 2020) in Catalonia, from 12.5 (June 2020) to 836.3 (December 2020) in Italy, and from 55.6 (June 2020) to 927.1 (November 2020) in the UK. Between the two rounds of data collection, COVID-19 deaths per 100,000 increased from 2.4 to 22.2 in Catalonia, from 2.2 to 30.7 in Italy, and from 4.4 to 17.8 in the UK.
Demographic characteristics of respondents and prevalence of and mortality from COVID-19
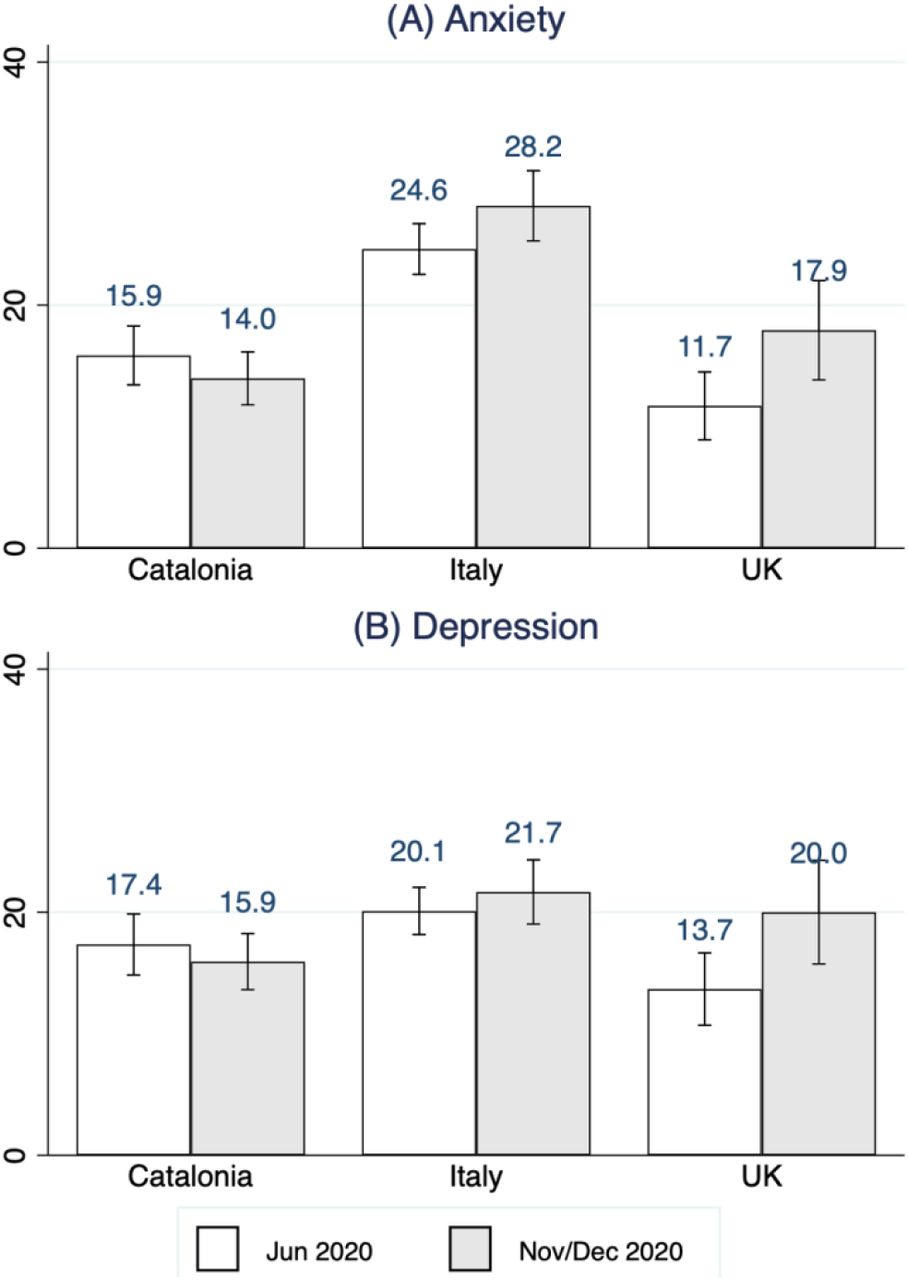
Fig 1 documents the prevalence of moderate/above-moderate symptoms of anxiety (GAD-7≥10) and depression (PHQ-9≥10) by country over time. In June 2020 the prevalence of moderate anxiety (panel A) was higher in Italy (24.6% [95% CI, 22.5%-26.7%]) than in Catalonia (15.9% [95% CI, 13.4%-18.3%]) and the UK (11.7% [95% CI, 8.9%-14.5%]). A similar conclusion emerges when looking at round 2. In June 2020, the prevalence of moderate/above-moderate depression (panel B) was highest in Italy (20.1% [95% CI, 18.2%-22.0%]), second highest in Catalonia (17.4% [95% CI, 14.8%-19.9%]), and lowest in the UK (13.7% [95% CI, 10.7%-16.7%]). In round 2, the prevalence of moderate/above-moderate depression is higher in Italy (21.7% [95% CI, 19.0%-24.3%]) than in Catalonia (15.9% [95% CI, 13.6%-18.2%]). Figure S3 (S1 Appendix) presents a further breakdown of the prevalence of symptoms depending on intensity.
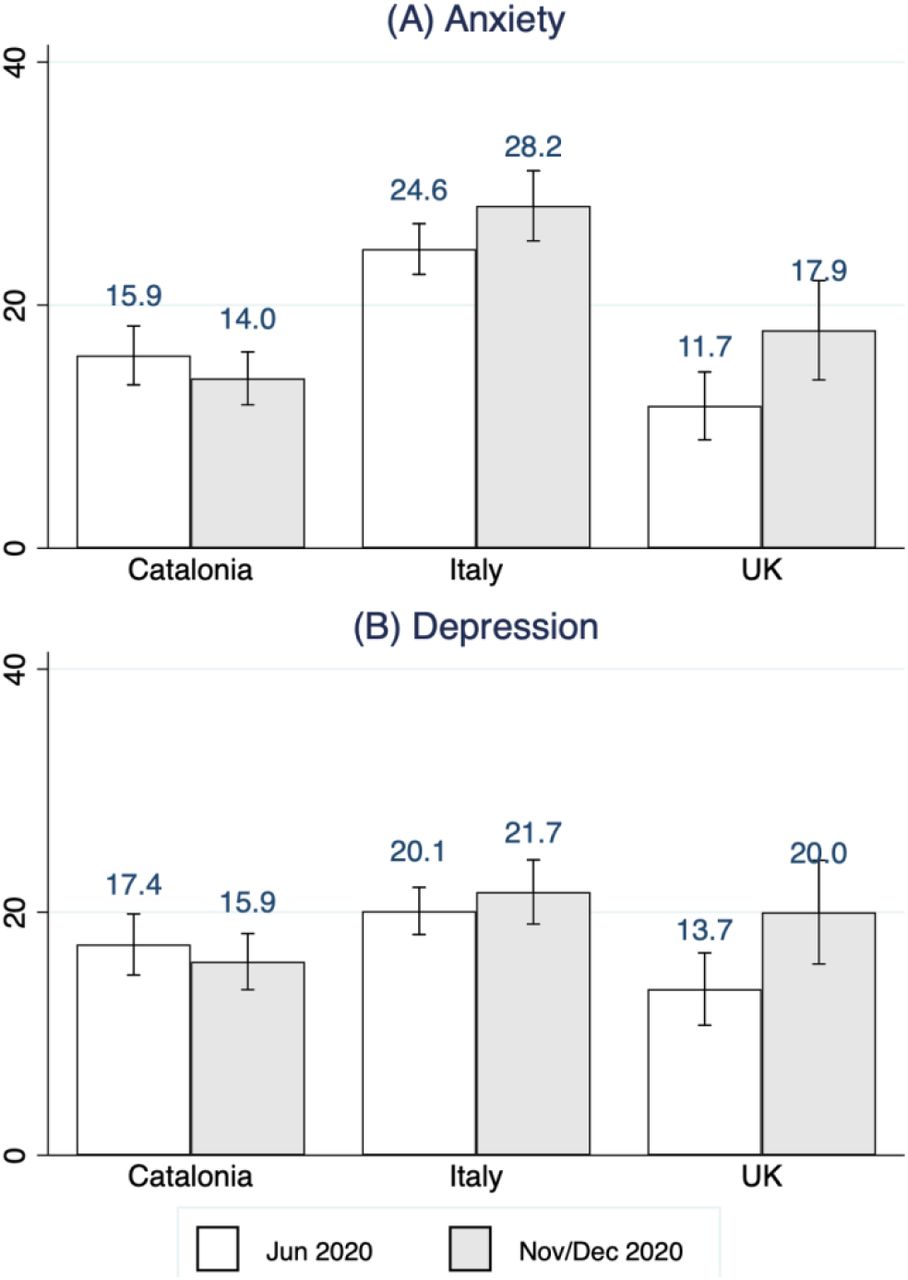
Grey bar corresponds to Nov 2020 for Catalonia and UK, and to Dec 2020 for Italy. Anxiety symptoms =1 if GAD-7 ≥ 10 and depression symptoms =1 if PHQ-9 ≥ 10. 95% confidence intervals.
Fig 2 investigates the differences in the prevalence of moderate/above-moderate symptoms of anxiety and depression by sex and age across countries. Panel A shows that the prevalence of moderate/above-moderate symptoms of anxiety is higher among women than among men in Catalonia (women: 17.3%, [95% CI, 15.2%-19.5%], men: 10.2%, [95% CI, 7.9%-12.6%]) and Italy (women: 32.4%, [95% CI, 29.8%-35.0%], men: 19.7%, [95% CI, 17.6%-21.9%]). Panel B shows that the prevalence of moderate/above-moderate symptoms of depression is higher among women than among men in Catalonia (women: 19.0%, [95% CI, 16.8%-21.2%], men: 12.1%, [95% CI, 9.6%-14.6%]) and Italy (women: 26.3%, [95% CI, 23.8%-28.7%], men: 15.3%, [95% CI, 13.4%-17.3%]). Panel C shows that the prevalence of moderate/above-moderate symptoms of anxiety is higher among younger (<60 y) than older (≥60 y) respondents in all three countries: Catalonia (<60 y: 17.0%, [95% CI, 15.0%-19.0%], ≥60 y: 9.3%, [95% CI, 6.8%-11.9%]), Italy (<60 y: 29.3%, [95% CI, 26.9%-31.6%], ≥60 y: 21.5%, [95% CI, 19.0%-23.9%]), and the UK (<60 y: 15.6%, [95% CI, 12.9%-18.2%], ≥60 y: 7.2%, [95% CI, 2.8%-11.5%]). Similarly, Panel D shows that the prevalence of moderate/above-moderate symptoms of depression is higher among younger (<60 y) than older (≥60 y) respondents across all countries.

Grey bars are for women (panel A and B) and over 60 (panels C and B). Anxiety symptoms =1 if GAD-7 ≥ 10 and depression symptoms =1 if PHQ-9 ≥ 10. 95% confidence intervals.
Fig 3 describes perceptions of workplace safety and exposure to COVID-19. Around half of Italian respondents disagreed with the statement “my workplace is providing me with the necessary PPE” was found in Italy in June 2020 (50.1%, [95% CI, 47.6%-52.6%] (panel A). This decreased to 30.1% [95% CI, 27.1%-33.1%] in December 2020. In Catalonia, the percentage was 25.8% [95% CI, 22.8%-28.7%] in June 2020, and decreased to 15.4% [95% CI, 13.0%-17.7%] in November 2020. In the UK, 16.1% [95% CI, 12.9%-19.4s%] of respondent disagreed with this statement in June 2020 and only 1 in 10 respondents disagreed with this statement in November 2020 (10.1%, [95% CI, 6.8%-13.3%]). Panel B shows that the percentage of respondents who agreed with the statement “I feel vulnerable and exposed at work” remained constant between rounds; including 1 in 5 respondents in Catalonia and the UK, and nearly 1 in 2 in Italy. It is notable that the country with the lowest rates of perceived workplace safety (Italy) also has the highest rates of anxiety symptoms.

Panel A: Percentage of respondents who do not agree with the statement “my workplace is providing me with the necessary Protective Personal Equipment”. Panel B: Percentage of respondents who agree/strongly agree with the statement “I feel vulnerable and exposed at work”. Panel C: Percentage of percentage of respondents who “directly looked after COVID-19 patients last week. Panel D: Percentage of respondents who are aware of “at least one COVID-19 death among healthcare workers in their workplace”.
Panel C illustrates that the proportion of respondents that have “directly looked after COVID-19 patients last week” increased between June and November 2020 in Catalonia (29.6%, [95% CI, 26.6%-32.7%] to 43.4%, [95% CI, 40.4%-46.8%]) and between June and November 2020 in Italy (25.0% [95% CI, 22.9%-27.1%] to 58.0% [95% CI, 54.8%-61.2%]). In contrast, the percentage remained similar between the two rounds in the UK (30.2% [95% CI, 26.1%-34.2%] vs. 34.3% [95% CI, 29.2%-39.4%]). Lastly, Panel D shows that 1 in 5 respondents in Catalonia were aware of at least one COVID-19 death among healthcare workers in their workplace in June 2020 and November 2020. In Italy, this ratio increased from 1 in 3 in June 2020 (31.4%, [95% CI, 29.1%-33.7%]) to 2 in 5 in December 2020 (40.6%, [95% CI, 37.4%-43.8%]). In the UK, it remained constant at about 1 in 3 respondents. The increase across survey rounds in the percentage of medical doctors directly treating COVID-19 patients in the last week in Catalonia and Italy, matches the evolution of the pandemic reported in Table 1.
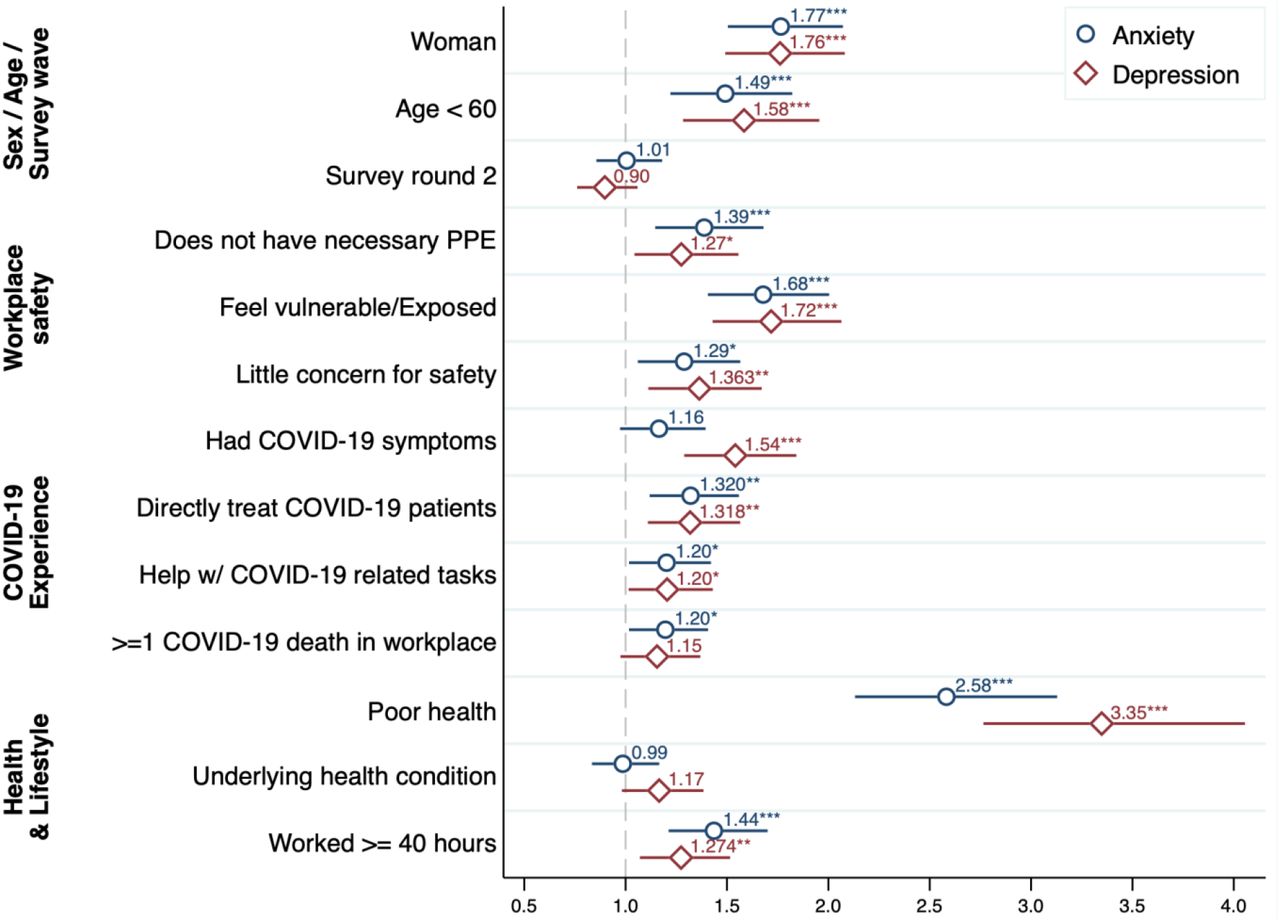
After pooling together all countries and the two rounds of data, Fig 4 displays the odds-ratios (ORs) of various risk factors estimated using a multivariable logit specification with binary anxiety and depression indicators as the dependent variables. Controlling for health behaviors (smoking behavior, having had the flu vaccine), household composition (living with children under 5 and living with someone over 60), occupational categories and medical organizations indicators, women, younger individuals (< 60 years), those who feel vulnerable and exposed at work, those who think that their workplace has shown little concern for their safety, those who directly looked after COVID-19 patients last week, those with poor health status, and those who worked over 40 hours last week had higher odds of anxiety and/or depression symptoms.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The figure displays the odds ratio of each variable (and its corresponding 95% CI) from a multivariable logistic regression pooling across all countries and timepoints. The dependent variable are binary indicators for anxiety (circle markers) or depression (diamond markers). In addition to the variables listed in the figure, the regression also controls for indicators for smoking, a flu vaccine this season, living with a child under 5, living with someone over 60, occupational codes, and institutional codes. Table S6 (S1 Appendix) reports full regression tables for the pooled sample and separate countries.
Women had higher odds of anxiety (OR=1.77 [95% CI, 1.50-2.07]) and depression (OR=1.76 [95% CI, 1.49-2.09]) compared to men. Compared with individuals above 60 years, younger individuals had higher odds of anxiety (OR=1.49 [95% CI, 1.22-1.82]) and depression (OR=1.58 [95% CI, 1.28-1.96]). A reported lack of necessary PPE in the workplace was associated with higher odds of anxiety (OR=1.39 [95% CI, 1.15-1.68]) and depression (OR=1.27 [95% CI, 1.04-1.56]). Respondents who felt vulnerable or exposed in their workplace had greater odds of anxiety and depression symptoms compared with people who did not feel vulnerable or exposed (OR=1.68 [95% CI, 1.41-2.00]; OR=1.72 [95% CI, 1.43-2.06]). Compared with people who reported a fair/good health status, individuals who reported a poor health status had higher odds of anxiety (OR=2.58 [95% CI, 2.13-3.13]) and depression (OR=3.35 [95% CI, 2.76-4.06]). Compared with individuals who worked below 40 hours, those who worked 40 hours or more last week had higher odds of anxiety (OR=1.44 [95% CI, 1.21-1.70]) and depression (OR=1.27 [95% CI, 1.07-1.52]). Table S6 (S1 Appendix) shows that these patterns hold for specific countries too.
Discussion
This is one of the few studies to provide a multi-country analysis of the mental wellbeing of medical doctors at two timepoints during the COVID-19 pandemic. Among respondents from Italy, Catalonia and the UK, the prevalence of anxiety and depression was highest among medical doctors in Italy, with 1 in 4 suffering from anxiety symptoms in June and December 2020 and 1 in 5 suffering from depression symptoms over the same period. Within each country, no difference in the prevalence of anxiety and depression were reported between the first and second rounds of the survey. Hence, we cannot discard that the mental health repercussions of the pandemic are persistent.
In Catalonia, Italy, and the UK, higher risk of anxiety and depression symptoms are found among women, individuals below 60 years old, those feeling vulnerable/exposed at work, and those in poor health. These associated risk factors provide a few possible reasons for the variation in the prevalence of anxiety and depression across countries. For example, the percentage of respondents who report a lack of necessary PPE and report feeling vulnerable and exposed at work are highest in Italy, where rates of anxiety and depression are also highest.
Our findings are consistent with other studies that have examined the rates of anxiety and depression among healthcare workers during the pandemic. In Spain, Alonso et al [30] find that among 9,138 respondents (26.4% physicians, 77.3% women) working in 6 places (including Catalonia) during May and September 2020, the prevalence of depression (PHQ-8≥10) and anxiety (GAD-7≥10) is 22.4% (vs. 16.5% in our Catalan sample) and 17.0% (vs. 14.9% in our Catalan sample). In Italy, Rossi et al [31] find that among 1,379 respondents (31.4% physicians, 77.2% women) surveyed in March 2020, the prevalence of depression (PHQ-9≥15) and anxiety (GAD-7≥15) was 24.7% (vs. 6.6% in our Italian sample) and 19.8% (vs. 9.5% in our Italian sample). Conti et al [32,33] find similar magnitudes. In the UK, Greenberg et al [34] find that among 709 staff (41% doctors) working in English hospitals in summer 2020, the prevalence of moderate (PHQ-9≥10) and severe (PHQ-9≥20) depression was 37% and 6%, respectively (26% and 6% among doctors, vs. 16.2% and 2.7% in our UK sample), and that the prevalence of moderate (GAD-7≥10) and severe (GAD-7≥15) anxiety was 27% and 11%, respectively (20% and 8% among doctors, vs. 14.2% and 5.9% in our UK sample). Greene et al [35] find comparable rates.
Our findings are also consistent with studies investigating risk factors of mental health among healthcare workers. In a review of 24 studies, De Kock et al. [7] show that risk factors include underlying health, being female, concerns about workplace safety [36,37], contact with COVID-19 [8,38,39], and concerns about the wellbeing of others [36]. In Spain, Alonso et al [30] find that healthcare professionals frequently exposed to COVID-19 patients are statistically significantly more like to experience mental health disorders (OR=3.98, 95% CI: 3.27-4.85). In Italy, Rossi et al [31] find that being female is associated with higher GAD-7 (OR=2.18, 95% CI: 1.49-3.19) and PHQ-9 scores (OR=2.03, 95% CI: 1.44-2.87). In the UK, Siddiqui et al. [40] find that among 558 healthcare professionals (51% doctors, 31% nurses), concerns about exposure to COVID-19 and the lack of PPE are important causes of anxiety.
Contributions
Our study contributes to monitoring the mental wellbeing of medical doctors during the COVID-19 pandemic. Including multiple countries and timepoints allow comparison between different settings, and how the pandemic has impacted medical doctors at different points during the pandemic. The similar patterns across countries suggest that our findings may be generalizable to other European settings. Rather than relying on online convenience samples, our sampling technique relies on the institutional mailing lists of medical organizations. In comparison to previous studies, we focus on medical doctors rather than a broader group of healthcare workers.
Limitations
This study has several limitations. First, when comparing two cross-sectional surveys for each country, we were not comparing the same individuals. Differences in prevalence of mental health symptoms could be driven by changes in sample composition across waves. Relatedly, the survey did not take place at the same point during an epidemic wave in data collections round 1 and 2.
Second, participants in our survey are not necessarily representative of the underlying populations of medical doctors and may be self-selected since they voluntarily take part in the survey. Reporting bias is likely. If individuals with symptoms were more likely to respond (e.g. to express grievances), then our estimates may be higher than the population average. Conversely, if individuals with above-average symptoms are less likely to respond (e.g. due to time constraints), then our estimates may be below the population average.
Third, anxiety and depression symptoms may not be comparable across countries due to different reporting norms in the GAD-7 and PHQ-9 questionnaires. Reassuringly, our pooled multivariable logistic regressions produce similar results even when controlling for occupation and institution fixed effects.
Finally, our measures of anxiety and depression are not based on an objective diagnosis made by a clinician.
Conclusion
The COVID-19 pandemic has been classified as a traumatic event [1]. Healthcare workers have arguably had the most direct and longest exposure to this disease. Our study identified a high prevalence of anxiety and depression among medical doctors in both first and second wave of the pandemic, contributing to a wider literature examining the effects of traumatic events on mental wellbeing [41], especially on those who are most exposed because of the demands of their occupation. The results of this study suggest that institutional support for healthcare workers, and in particular medical workers, is important in protecting and promoting their mental health in the current and in future pandemics.
Data Availability
All data will be made publicly available at https://sites.google.com/site/climentquintanadomeque/healthcare-workers-survey.
Acknowledgements
This study was approved by the University of Exeter Business School Research Ethics Committee (eUEBS003024).
We are grateful to COMB (Barcelona Medical Council), COMG (Girona Medical Council), Anaao-Assomed (Union of physicians and healthcare executives), FIMMG (Union of general practitioners), RCPSG (Royal College of Physicians and Surgeons of Glasgow), and RCSEd (Royal College of Surgeons of Edinburgh) for their collaboration. We are grateful to the participants in our survey. We thank Sr. Miquel Creixell Tramuns and Dr. Climent Quintana Escandell for their help in the design and translation of the survey in Catalan, and Sra. Anna Mitjans, Sra. Mariajosé Verdú, Dr. Jaume Padrós i Selma, Dr. Josep Vilaplana, Prof. Jackie Taylor, Mr. David Thomson, Dottoresa Silvia Procaccini, Prof. Vincenzo Galasso and Dr. Francesco Longo for their help in distributing our survey.
References



