
Abstract
Vaccine breakthrough SARS-CoV-2 infection was monitored in 3694 healthcare workers receiving 2 doses of BNT162b2. SARS-CoV2 infection was detected in 33 subjects, with a 3-months cumulative incidence of 0.90% and 0.42% in SARS-CoV-2-naïve and experienced subjects, respectively. Vaccine protection was 87% in naïve and 94% in experienced subjects when compared with a pre-vaccination control group. The infection was mildly symptomatic in 16 (48%) and asymptomatic in 17 (52%) subjects. Virus isolation was positive in 7/13 (54%) symptomatic and 4/8 (50%) asymptomatic subjects tested, and B.1.1.7 lineage was detected in all subjects. Antibody and T-cell responses were not reduced in subjects with breakthrough infection. Evidence of virus transmission, determined by contact tracing, was observed in two (6.1%) cases.
This real-world data confirm the protective effect of BNT162b2 vaccine. A triple antigenic exposure, as occurring in experienced subjects, may confer a higher protection. Virus transmission from vaccinated subjects is infrequent.
Since the identification of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) as etiological agent of Coronavirus Disease 19 (COVID-19), several efforts have been made in order to prevent infection and disease. Moreover, recently, highly effective vaccines have been introduced [1–4].
The licensed vaccines showed high efficacy in protection from SARS-CoV-2 infection in clinical trials, ranging from 70 to 95% [1–4]. However, post-authorization real-life studies are an important complement to evaluate the vaccine efficacy in different populations and in the face of non-controlled real world challenges.
Initial nationwide data collection are confirming the efficacy of the licensed vaccines, showing an effect size consistent with that reported in clinical trials [5–8].
However, clinical, virological and immunological characteristics of breakthrough SARS-CoV-2 infections after vaccination have been poorly investigated, due to lack of prospective systematical testing in vaccinated cohorts. Two studies conducted on healthcare workers reported a lower rate of symptomatic vs asymptomatic infections in vaccinated with respect to unvaccinated individuals [9–10], while data on the actual presence of infectious virus in SARS-CoV-2 RNA-positive samples recovered from vaccinated individuals are missing. Whether infected vaccinated subjects can transmit the infection, and to which extent, is a major concern for public health policy. Finally, whether post vaccine infections are associated with a deficient immune response to vaccination has not been investigated yet.
Healthcare workers have a high risk of exposure to SARS-CoV-2, therefore representing a challenging cohort for the evaluation of vaccine efficacy and breakthrough infections. In Italy, the vaccination campaign started on December 27th, 2020, prioritizing healthcare workers and fragile and elderly individuals [11].
Aim of the present study was to investigate prospectively the risk of SARS-CoV-2 infection in vaccinated healthcare workers in a single Italian Center (Fondazione IRCCS Policlinico San Matteo, Pavia). Data were compared with that observed in the same Institution during the second pandemic wave in the pre-vaccination setting. The characteristics of breakthrough infections, the underlying immune response and the risk of virus transmission to other individuals were investigated.
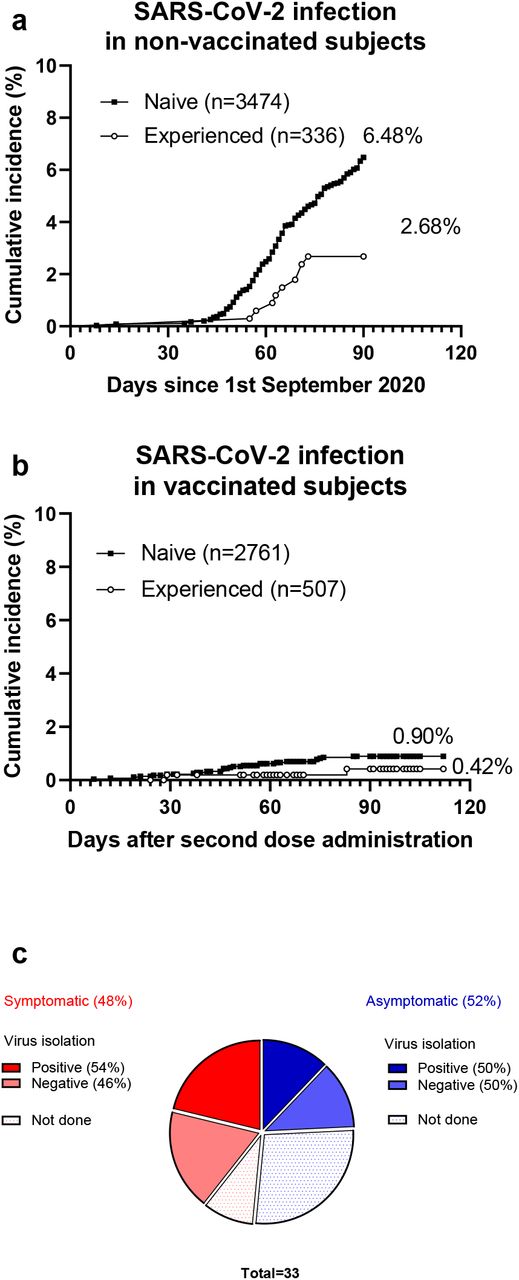
In the period April 29-June 30 2020, 3810 healthcare workers were tested for previous SARS-CoV-2 infection according to serostatus determination: 336 subjects resulted SARS-CoV-2 experienced and 3474 SARS-CoV-2 naïve. During the second pandemic wave, SARS-CoV-2 infection was detected in 9 SARS-CoV-2-experienced and 225 SARS-CoV-2 naïve subjects. The 3-months cumulative incidence of SARS-CoV-2 infection (Fig 1a) was 2.68% in experienced vs 6.48% in naïve subjects (p=0.006), with a hazard ratio of 0.41 (95%CI: 0.26-0.61). The protective effect of the immunity elicited by natural infection was 59% (95% CI: 39-74%) Data on symptoms were available for 112 subjects: 1/4 (25%) naïve and 85/108 (79%) experienced subjects developed mild symptoms and no patient required hospitalization.

a, Cumulative incidence of SARS-CoV-2 infection in SARS-CoV-2-naïve and experienced subjects during the second pandemic wave (period: September 1st-November 30th 2020). b, Cumulative incidence of SARS-CoV-2 infection in SARS-CoV-2-naïve and experienced subjects who received two doses of BNT162b2 vaccine.
During the period January 18-March 31 2021, 3720 healthcare workers received the second dose of BNT162b2 vaccine. SARS-CoV-2 serostatus before vaccination was determined in 3268 subjects after the first and second pandemic waves (determined by anti-S1/S2 IgG and anti-N Ig, respectively): 230/2934 (7.84%) subjects tested after the first wave and 444/2446 (18.15%) subjects tested after the second wave resulted SARS-CoV-2 seropositive. Overall, before vaccination 507 subjects resulted SARS-CoV-2 experienced and 2761 SARS-CoV-2 naïve, while SARS-CoV-2 serostatus was unknown for 426 subjects and dubious for 26 subjects. After complete vaccination schedule, SARS-CoV2 infection was detected in 33 subjects (median time: 47, range 7-90, days after vaccination): 2 subjects among the 507 SARS-CoV-2-experienced, 24 among the 2761 SARS-CoV-2 naïve individuals, and 7 among the 452 individuals with unknown or dubious serostatus. The 3-months cumulative incidence of SARS-CoV-2 infection in the overall population of vaccinated healthcare workers was 0.93%. Considering separately experienced and naïve subjects (Fig 1b), the 3-months cumulative incidence was 0.42% in SARS-CoV-2-experienced and 0.90% in SARS-CoV-2 naïve subjects (p=0.272). The incidence of SARS-CoV-2 infection after vaccination in naïve subjects was compared to that observed in naïve subjects during the second pandemic wave. The odds ratio for developing SARS-CoV-2 infection after vaccination with respect to unvaccinated subjects was 0.13 (95% CI: 0.08-0.19), with an estimated protective effect of 87% (95% CI: 81-92%). The odds ratio for developing SARS-CoV-2 infection after vaccination in experienced subjects was 0.06 (95% CI: 0.01-0-20), with an estimated protective effects of 94% (95% CI: 80-99%).
The infection was mildly symptomatic in 16 (48%) and asymptomatic in 17 (52%) subjects (Fig 2). No subjects required hospitalization. Virus isolation from nasal swab was attempted in 21 subjects (13 symptomatic and 8 asymptomatic subjects). Infectious virus was recovered in 7/13 (54%) symptomatic and 4/8 (50%) asymptomatic subjects (Fig 1c). Lineage characterization was available in 23 subjects in whom the amount of viral RNA was sufficient for genome sequencing. All analyzed patients were infected by the B.1.1.7 variant, also recently renamed as alpha variant. Evidence of virus transmission to family members or close contacts of the 33 infected subjects was observed in 2 (6.1%, 95% CI: 1.1-19.6%) cases, both of whom had a symptomatic infection.
{kind=link}
{kind=link}
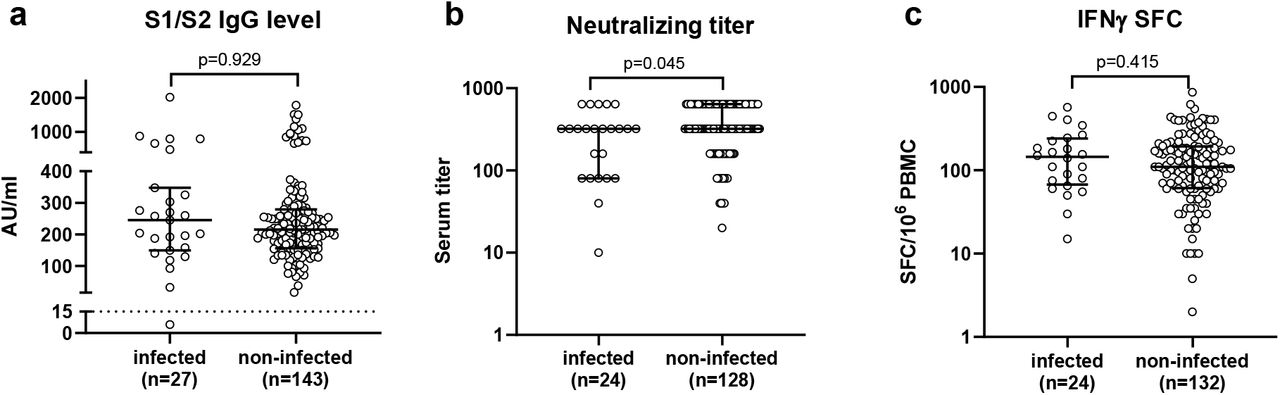
a, Anti-spike IgG level (AU: arbitrary units); b, serum neutralizing titer; c, IFNγ-producing spot forming cells (SFC)/106 peripheral blood mononuclear cells (PBMC).
The antibody and T-cell response was determined in a subset of infected subjects at the moment of diagnosis of infection and in a control subset of non-infected subjects who were SARS-CoV-2 naïve before vaccination. Anti-S1/S2 IgG antibodies were detected in all but one of 27 infected subjects at levels not significantly different from that observed in 143 non-infected controls (Fig 2a). Neutralizing serum titer was determined in 24 infected subjects and compared to that observed in 128 controls (Fig 2b). Median serum neutralizing titer was 1:320 (range 1:10-≥1:640), slightly lower (two-fold) than that observed in controls (median titer: ≥1:640; range: 1:20-≥1:640; p=0.045). Finally, the T-cell response to peptide pool of the Spike protein was not significantly different between 24 infected subjects and 132 controls (Fig 2c). Antibody and T-cell response was not different between symptomatic and asymptomatic subjects (data not shown).
Results of this study confirm the protective effect of BNT162b2 vaccine in healthcare workers. By comparing the incidence of vaccine breakthrough infections with the incidence of SARS-CoV-2 infection in unvaccinated subjects from the same institution during the second pandemic wave (pre-vaccination period), an 87% vaccine protection was estimated. All vaccine breakthrough infections were asymptomatic or mildly symptomatic, and the frequency of symptomatic infections was lower in vaccinated than unvaccinated subjects (48% vs 79%). Live infectious virus was detected only in half of the cases of breakthrough infections, and virus transmission to other individuals was documented in 6.1% of the cases. Finally, breakthrough infections were not associated with failure in developing antibody or T-cell response after vaccination.
The 87% protective efficacy of BNT162b2 vaccine observed in our study is slightly lower than the 95% protection reported in the phase 2/3 clinical trial [1] but is consistent with those reported in a retrospective analysis conducted in Israel [9] and in the SIREN study conducted in England [10], both involving healthcare workers. The reason for this lower effect may reside in the fact that healthcare workers have a higher exposure to SARS-CoV-2 infection than the general population in which the clinical trial was conducted. Moreover, the active surveillance and screening performed in our as well as in the other above-mentioned studies may have led to the identification of a number of subclinical infections that were not ascertained in the clinical trial. Nevertheless, vaccine protection observed by this real-world analysis in healthcare workers remains high, and results are consistent among different countries.
Immune protection after SARS-CoV-2 infection appears effective and sustained for at least 10 months [12]. The immune protection provided by the vaccine appears even higher than that induced by natural infection (87% vs 59%, as observed in the retrospective analysis of our study). We analysed separately the incidence of breakthrough infections in individuals who were either SARS-CoV-2 naïve or experienced before vaccination. Although we observed a lower incidence of breakthrough infections in experienced than naïve subjects (0.42% vs 0.90%) and a higher protective effect (94% vs 87%), the population size was too low to verify whether SARS-CoV-2-experienced achieve a significantly higher protection after vaccination than naïve subjects. Nevertheless, immunogenicity studies showed that vaccination is able to boost the pre-existing immunity in experienced subjects, who develop higher antibody and T-cell levels than naïve subjects [13–15]. In addition, we observed that vaccination of experienced individuals elicited neutralizing antibody at levels that overcome the partial antibody escape of the B.1.351 variant [15]. It is tempting to speculate that three antigenic exposures, as in the case of SARS-CoV-2-experienced subjects receiving two vaccine doses, may confer a higher and broader protection.
Breakthrough infections were either mildly symptomatic or completely asymptomatic. To assess whether the detection of SARS-CoV-2 RNA in naso-pharingeal samples of vaccinated subjects with breakthrough infection was associated with the presence of live infectious virus, we attempted virus isolation on cell cultures in 21 of the 33 subjects, recovering infectious virus only in half of the cases. We could not compare the rates of infectious virus recovery in vaccinated vs unvaccinated SARS-CoV-2 RNA positive subjects, since we did not perform virus isolation in the retrospective control group. However, the low rate of detection of infectious virus is in line with a recent report showing decreased viral load in infected vaccinated subjects [16], and suggests a lower contagiousness, along with the lower severity, of the vaccine breakthrough infections. Thus, SARS-CoV-2 RNA detected in fully vaccinated is likely to be often a sign of an abortive infection limited and blocked on mucosal surfaces by the elicited immunity.
Most importantly, we documented a lack of transmission of the virus in the great majority of cases, since only 2/33 subjects transmitted the infection to a family member. This data support the very low contagiousness of SARS-CoV-2 infection in vaccinated subjects and the effectiveness of SARS-CoV-2 vaccination in blocking the infection spreading at the population level.
In order to verify the hypothesis that a poor individual response to the vaccine is the cause of breakthrough infections, we compared the antibody and T-cell responses of the infected individuals with a control group of vaccinated uninfected subjects. No difference was observed for anti-Spike IgG and T-cells, while a slight reduction in the neutralizing serum titers was detected in the infected subjects. However, it was not possible to define a cutoff level of neutralizing titer able to identify poor responders that are at higher risk for vaccine breakthrough infections. We could exclude also that a viral variant associated to potential vaccine escape was causing the infection, since in all cases in which the RNA amount was sufficient for sequencing, the B.1.1.7 variant, which is now accounting for the great majority of viral strains circulating in Italy, was detected.
The strength of this study resides in the prospective systematical collection of virological data (viral RNA detection and infectious virus recovery), clinical symptoms, immune response and virus transmission to other individuals, providing an insight on the characteristics of vaccine breakthrough infection and evidence for their low contagiousness. The limitation resides in the lack of a prospective control group for the evaluation of vaccine protection, since the comparison was performed with a retrospective cohort. Nevertheless, we can assume that virus circulation among healthcare workers was similar during the two periods, while the surveillance protocol was similar. In addition, the estimated vaccine efficacy was similar to that observed in other real-world analysis on healthcare workers.
In conclusion, our analysis confirms the protective efficacy of the BNT162b2 vaccine, while breakthrough infections are poorly symptomatic and associated with a low contagiousness. This evidence may support the policy of loosening containment measures in vaccinated individuals, while the duration of the vaccine protection should be evaluated in the next future.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author contribution
FR and DL analyzed and interpreted the data and drafted the manuscript; AM, VN, AM, AMG, GG, collected and managed the data; CR, MD performed patients’ follow-up; FeB and IC, performed experiments on T-cell response; JCS, AF, AS performed experiments on antibody response; EP performed virus isolation; SP, AP, FG sequenced viral genomes; CM, AT supervised participants enrollment; FaB supervised the study and revised the manuscript. All the authors critically reviewed the manuscripts.
Competing interests
The authors have no competing interest to declare.
Online Methods
Study subjects and design
The occurrence of SARS-CoV-2 infection was monitored prospectively in 3720 healthcare workers of Fondazione IRCCS Policlinico San Matteo, Pavia receiving 2 doses of the BNT162b2 vaccine. Subjects completed vaccination schedule between January 18 and March 31, 2021 and data were collected until May 10, 2021.
Data on incidence of SARS-CoV-2 infection during the second pandemic wave in 3810 healthcare workers from the same institution who had serological definition of previous SARS-CoV-2 infection were used as control (data were collected in the period September 1st-November 30 2021).
In both periods, naso-pharingeal swabs were collected and tested for SARS-CoV-2 RNA positivity in subjects with symptoms suggestive for SARS-CoV-2 infection or in case of contact with infected subjects as previously reported [1]. In vaccinated subjects who resulted SARS-CoV-2 RNA-positive, blood samples for immune response analyses were collected 24-48h after nasopharyngeal swab sampling. The transmission of the infection from SARS-CoV-2 RNA-positive vaccinated subjects was investigated by contact-tracing and monitoring for SARS-CoV-2 RNA detection in nasal swabs in coworkers and family members of the infected subjects. Study procedures were approved by Fondazione IRCCS Policlinico San Matteo and all the subjects gave their written informed consent.
Virus isolation and sequencing
Virus isolation was performed by inoculation of 200µl nasopharyngeal swab suspension medium, after decontamination with an antibiotics pool for 30 min at room temperature, on Vero E6 cells cultured in 24well plate, and detection of cytopathic effect after one week culture. Complete genome sequencing was performed on samples showing cytopathic effect as previously described [2]. Lineages were assigned from alignment file using the Phylogenetic Assignment of Named Global Outbreak LINeages tool PANGOLIN v1.07 (https://github.com/hCoV-2019/pangolin).
SARS-CoV-2-specific antibody and T-cell determination
To detect subjects with SARS-CoV-2 infection after the first pandemic wave, serological analysis was performed in the period April 29-June 30 2020 using chemiluminescent assay (Liason SARS-CoV-2 S1/S2 IgG, Diasorin, Saluggia, Italy) for the quantitative measurement of SARS-CoV-2 anti-S1 and anti-S2 IgG antibody. Results higher than 15 AU/mL were considered positive and defined SARS-CoV-2 experienced subjects, whereas results below 12 AU/mL were considered negative and defined SARS-CoV-2 naïve subjects. Subjects with borderline results ranging from 12 and 15 AU/mL were not included in the analysis. A further serological screening was conducted after the second pandemic wave in the period December 15 2020-February 3 2021. Since this second screening overlapped with the initiation of the vaccination campaign, the electrochemiluminescent assay Elecsys Anti-SARS-CoV-2 N (Roche Diagnostics Rotkreuz, Switzerland), which provides quantitative measures of mainly IgG (but also IgA and IgM) specific for SARS-CoV-2 Nucleocapsid protein (not present in the vaccine) was used. Results were given as units (U)/ml and are considered positive when ≥0.8 U/ml. Subjects with positive serological results after either or both screenings were considered SARS-CoV-2 experienced before vaccination.
Antibody and T-cell response to Spike protein was determined in vaccinated subjects after detection of SARS-CoV-2 infection and in a control group of SARS-CoV-2-naïve subjects 21 days after complete vaccination. Anti-Spike IgG antibody was determined using Liason SARS-CoV-2 S1/S2 IgG (Diasorin). Neutralizing antibody serum titre was determined as previously reported [3]. Spike specific T-cell response was determined with an IFNγ ELISpot assay after peripheral blood mononuclear cell stimulation with a peptide pool (15mers overlapping by 10 aminoacids) spanning the entire Spike protein [4]. Results were given as IFNγ spot forming cells/106 cells.
Statistical analysis
The cumulative incidence of SARS-CoV-2 infection was calculated with the Kaplan-Meier method and log-rank test was adopted for statistical comparison. The hazard ratio (HR) and 95% confidence interval (CI) for SARS-CoV-2 infection in experienced vs naïve subjects in the pre-vaccination period was calculated with the log-rank approach. The odds ratio (OR) and 95% CI for SARS-CoV-2 infection in experienced or naïve vaccinated vs unvaccinated subjects was calculated using as reference control group SARS-CoV-2-naïve individuals of the pre-vaccination period. The protective efficacy of immunity elicited by SARS-CoV-2 infection against secondary infections was calculated as 100% x (1-HR), and the relevant 95% CI were calculated as 100% x (1-95% CIHR), where CIHR is the 95% CI of the HR. The vaccine protective efficacy was estimated as 100% x (1-OR), and the relevant 95% CI were calculated as 100% x (1-95% CIOR), where CIOR is the 95% CI of the OR. The antibody and T-cell levels in vaccinated subjects with or without breakthrough infections were compared with the Mann-Whitney U-test.
Acknowledgments
This work was supported by Fondazione Cariplo [grant CoVIM, no. 2020-1374] and Ministero della Salute, Ricerca Finalizzata [grants no. COVID-2020-12371760 and COVID-2020-12371817]. AP and FB have received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 101003650.
References



