
Abstract
Background Clostridioides difficile infection (CDI), its subsequent recurrences (rCDI), and severe CDI (sCDI) provide a significant burden for both patients and the healthcare system. Treatment consists of oral antibiotics. Fidaxomicin, bezlotoxumab and fecal microbiota transplantion (FMT) reduce the number of recurrences compared to vancomycin, but are more costly. Identifying patients diagnosed with initial CDI who are at increased risk of developing sCDI/rCDI could lead to more cost-effective therapeutic choices.
Objectives In this systematic review we aimed to identify clinical prognostic factors associated with an increased risk of developing sCDI or rCDI.
Methods PubMed, Embase, Emcare, Web of Science and COCHRANE Library databases were searched from database inception through March, 2021. Study selection was performed by two independent reviewers on the basis of predefined selection criteria; conflicts were resolved by consensus. Cohort and case-control studies providing an analysis of clinical or laboratory data to predict sCDI/rCDI in patients ≥18 years diagnosed with CDI, were included. Risk of bias was assessed with the Quality in Prognostic Research (QUIPS) tool and the quality of evidence by the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool, modified for prognostic studies. Overview tables of prognostic factors were constructed to assess the number of studies and the respective direction of an association (positive, negative, or no association).
Results and conclusions 136 studies were included for final analysis. Higher age and the presence of multiple comorbidities were prognostic factors for sCDI. Identified risk factors for rCDI were higher age, healthcare-associated CDI, prior hospitalization, PPIs started during/after CDI diagnosis and previous rCDI. Some variables that were found as risk factors for sCDI/rCDI in previous reviews were not confirmed in the current review, which can be attributed to differences in methodology. Risk stratification for sCDI/rCDI may contribute to a more personalized and optimal treatment for patients with CDI.
Background
Clostridioides difficile infection (CDI), its subsequent recurrences (rCDI), and severe CDI (sCDI) provide a significant burden for both patients and the healthcare system(1). Antibiotic treatment with oral vancomycin and fidaxomicin are the cornerstone of CDI treatment(2-4). Fidaxomicin reduces the number of recurrences compared to vancomycin (5). Bezlotoxumab, a monoclonal anti-Toxin B antibody, can be added to oral anti-CDI antibiotic therapy and reduces the number or recurrences in patients at high risk to develop rCDI (6). Fecal microbiota transplantation (FMT) is a highly efficacious treatment for rCDI, preventing subsequent recurrences, and can lower mortality risk and disease burden of sCDI (7, 8).
The costs of fidaxomicin, bezlotoxumab and FMT are higher compared to those of vancomycin. Identifying patients diagnosed with initial CDI who are at an increased risk of developing a severe episode or recurrences could lead to more cost-effective therapeutic choices. Identifying patients at risk, however, is challenging. Several prediction models have been developed (9-30), yet none has been widely adopted in clinical practice.
Objectives
In this systematic review we aimed to identify clinical prognostic factors associated with an increased risk of developing sCDI or rCDI.
Methods
Data sources
Two searches were performed to identify risk factors for (1) sCDI and (2) rCDI. The search terms and strategy were constructed by a trained librarian, see Supplementary data. PubMed, Embase, Emcare, Web of Science and COCHRANE Library databases were searched on October 4th, 2019. An update of the search was performed on March 13th, 2021. The search was restricted to articles published in English. Meeting abstracts were not considered. The search was not limited by year of publication. References of key papers were assessed for relevant papers.
Study eligibility criteria
Study eligibility was assessed in a two-step selection process. Two independent reviewers screened title and abstract for potentially eligible articles (TvR and RO); discrepancies were resolved by consensus. Full-text articles were retrieved for eligibility; data extraction and risk of bias assessment of included studies was performed by two researchers (TvR and RO).
Inclusion criteria: prospective and retrospective cohort and case-control studies including patients ≥18 years, diagnosed with CDI, and providing an analysis of clinical or laboratory data to predict severe/recurrent CDI.
Exclusion criteria: study in specific patient populations with a distinct medical condition other than CDI (e.g. study population comprises only hemodialysis patients), and small studies (less than 30 patients with severe/recurrent CDI). Laboratory values that were studied as prognostic factors, but which are not part of the regular work-up in CDI (e.g. assays for specific cytokines). Variables that are part of (some of) the definitions of sCDI (such as leukocytosis) were excluded as prognostic factor for sCDI to avoid circularity.
Studies on prognostic factors with conflicting results in the uni- and multivariable or with contradicting results when compared to previous meta-analyses, were assessed and graded by a third researcher (CV-G and JK) and scrutinized by weighing the results by the quality of evidence per study.
Outcomes of interest were:
Severe CDI:
ESCMID 2014/2021 definition: an episode of CDI with (one or more specific signs and symptoms of) severe colitis or a complicated course of disease, with significant systemic toxin effects and shock, resulting in need for ICU admission, colectomy or death (3, 31, 32); or:
IDSA/SHEA definition: an episode of CDI with a white blood cell count of ≥15×10^9 cells/mL or a serum creatinine level >1.5 mg/dL or increase of 50% or greater from baseline(33); or:
Any other author-constructed definition of severe/complicated/fulminant/fatal CDI.
Recurrent CDI: Recurrence is a new episode of CDI within 2-12 weeks after a previous episode, provided the symptoms of the previous episode resolved after completion of initial treatment (34, 35).
Assessment of risk of bias
Risk of bias was assessed with the Quality in Prognostic Research (QUIPS) tool (36), which is recommended by the Cochrane Prognosis Methods Group. The QUIPS tool appraises six domains: (1) study participation, (2) study attrition, (3) prognostic factor measurement, (4) outcome measurement, (5) study confounding and (6) statistical analysis and reporting. The overall risk of bias per study is scored as low, moderate, or high.
Quality assessment and data synthesis
The quality of evidence per study was assessed by using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool, modified for prognostic studies (Figure 1) (37). This tool is recommended by the Cochrane Prognosis Methods Group and consists of eight domains. The starting point for the quality of evidence is based on the phase of investigation. The quality can be up- or downgraded according to seven other domains. The QUIPS score is included in the second domain (‘Study limitations/risk of bias’) of the GRADE tool. The outcome of this assessment is the quality of evidence per study, which can be very low (+), low (++), moderate (+++) or high (++++).

Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool, modified for prognostic studies. The final outcome is the overall quality of evidence per study, which can be very low (+), low (++), moderate (+++) or high (++++).
Overview tables of prognostic factors were constructed to assess the number of studies and the respective direction of an association, i.e. positive, negative, or no association based on effect estimates, 95% CI intervals and p values, stratified by univariate and multivariate analyses. Similar prognostic factors (e.g. coronary artery disease and myocardial infarction) were combined to one factor for a more compact overview. No formal meta-analyses were performed.
Results
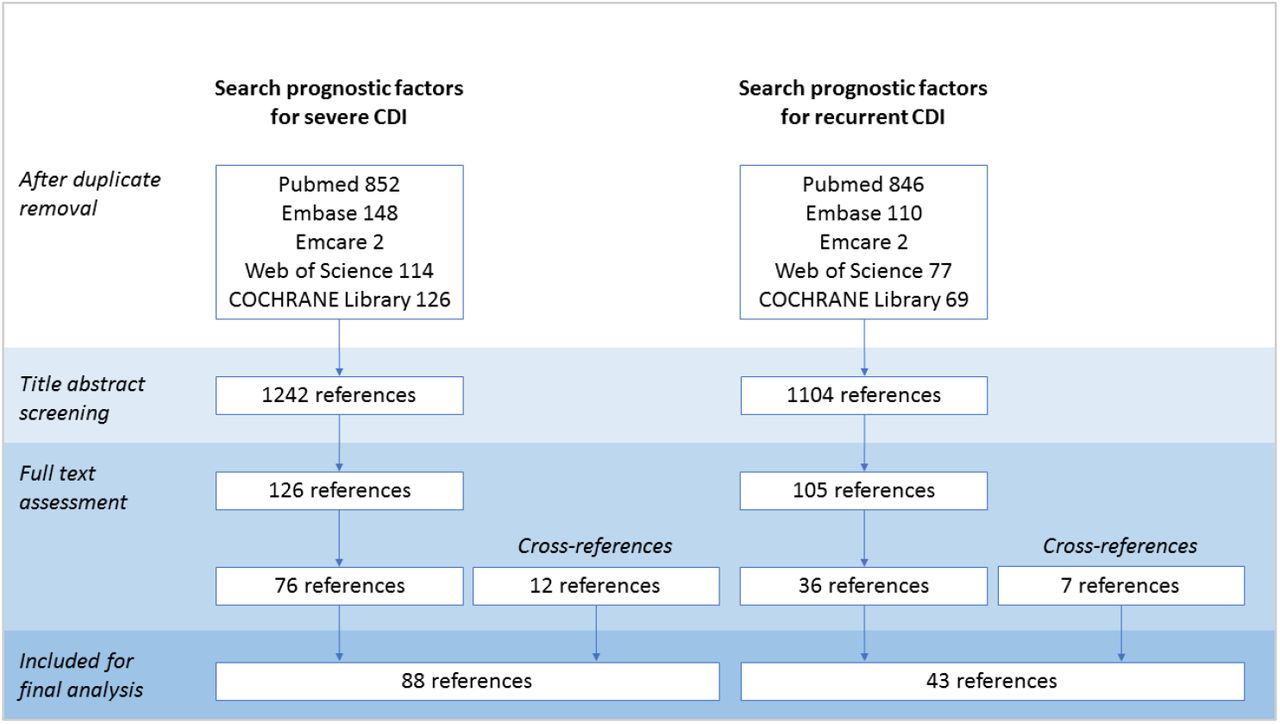
The search for prognostic factors for sCDI yielded 1242 references; 126 studies were assessed in more detail and 76 were included for analysis (20, 24, 25, 29, 38-109); twelve more studies retrieved from cross-references were also included (110-121) resulting in 88 studies for final analysis (Figure 2). The search for prognostic factors for rCDI yielded 1104 references; 105 studies were assessed in more detail and 36 were included for analysis (9, 10, 12-15, 102, 109, 122-149) as were seven studies from cross-references.) (111, 150-155). This resulted in 43 studies for final analysis (Figure 2). Additionally, data of the pivotal RCTs on fidaxomicin and bezlotoxumab were used to support findings (156-160).
{kind=link}
{kind=link}
Flow diagram of the selection process of studies on prognostic factors for severe/recurrent CDI
Prognostic factors for severe CDI
The overall quality of evidence ranged from very low to moderate, mainly due to the retrospective nature and small sample size of most studies. The prognostic factors studied in five or more articles are shown in Table 1.
Potential prognostic factors for severe CDI. Phase, phase of investigation. For uni- and multivariate analyses: +, number of significant effects with a positive value; 0, number of non-significant effects; -, number of significant effects with a negative value. For GRADE factors: ✓, no serious limitations; ✗, serious limitations (or not present for moderate/large effect size, dose effect); unclear, unable to rate item based on available information. For overall quality of evidence: +, very low; ++, low; +++, moderate; ++++, high.
Age was the most studied prognostic factor, and was investigated in 53 of 88 included studies (20, 24, 25, 29, 38-42, 44, 46-49, 52, 54, 55, 57, 59, 61-64, 66, 70, 71, 75, 77, 78, 80, 81, 83, 85-88, 91-94, 96, 97, 100, 104, 106, 109-111, 113, 114, 116-118). Fifty-one studies performed a univariate analysis and 40 studies (also) a multivariable analysis; 37/51 studies reported higher age as risk factor for sCDI in univariate analysis, and 26/40 studies in multivariable analysis (overall moderate quality of evidence).
Thirty-two studies assessed the presence of multiple comorbidities as risk factor for sCDI (25, 38-42, 46-49, 52, 62, 66, 70, 72-74, 80, 81, 85, 87, 88, 91-94, 96, 97, 109, 114, 116, 117); 20/30 studies found an association between the presence of multiple comorbidities and sCDI in univariate analysis and 11/23 studies in multivariable analysis (moderate quality of evidence).
For both higher age and the presence of multiple comorbidities a dose effect was observed: the higher the age or the more concurrent disorders, the higher the risk of severe disease. No specific medical condition was associated with sCDI.
For clinical decision making, a specific cut-off value for age and number of comorbidities would be convenient. However, in many studies age was used as a continuous variable (31/53 studies) or varying cut-off values are used. The majority of studies found a higher risk for sCDI in patients older than 65-70 years. For comorbidity, different established or self-constructed comorbidity scores were reported, the Charlson Comorbidity Index (CCI) most frequently (161). Again, most studies used CCI as continuous variable. Of the studies that identified more comorbidities as risk factor for sCDI, only three used a cut-off value: one study reported a higher risk in patients with a CCI of ≥3, and two found a higher risk in patients with ≥2 comorbidities (88, 93, 96). Thus, no statement can be made on the association between exact numbers of comorbidities and severe CDI.
Twenty articles studied the association between the presence of NAP1/RT027 strain and sCDI (44-46, 56, 60, 61, 73, 74, 81, 84, 85, 88, 89, 91, 94, 96, 100, 101, 108, 111); 8/19 studies reported a higher risk of sCDI in patients with NAP1/027 strain in univariate analysis, and 5/10 in multivariate analysis. One study found that NAP1/027 was more prevalent in patients with mild disease compared to patients with sCDI (44).
Furthermore, seven studies assessed C. difficile binary toxin as risk factor for sCDI (45, 82, 91, 94, 117, 119, 121). Of these, three identified C. difficile binary toxin as a risk factor for sCDI in univariate analysis, and only 1/1 study in multivariate analysis. The overall quality of evidence of these studies was low. We scrutinized the separate studies on the presence of NAP1/RT027 strain and/or binary toxin by weighing the results by the quality of evidence per study, but this did not alter the conclusion.
Another interesting finding was that the majority of studies did not find an association between the use of PPIs, H2 receptor antagonists or antibiotics and the occurrence of sCDI in uni- and multivariate analyses. However, the quality of evidence was low.
In conclusion, only the factors higher age (>65-70 years old) and the presence of multiple comorbidities were consistently associated with sCDI (Table 3).
Prognostic factors for recurrent CDI
The overall quality of evidence for the prognosis of recurrent CDI (rCDI) was low to moderate (Table 2). The majority of studies was retrospective, with a high to moderate risk of bias.
Potential prognostic factors for recurrent CDI. Phase, phase of investigation. For uni- and multivariate analyses: +, number of significant effects with a positive value; 0, number of non-significant effects; -, number of significant effects with a negative value. For GRADE factors: ✓, no serious limitations; ✗, serious limitations (or not present for moderate/large effect size, dose effect); unclear, unable to rate item based on available information. For overall quality of evidence: +, very low; ++, low; +++, moderate; ++++, high
Summary of findings
Higher age (≥65 years old) is the most studied factor and was investigated in 35/43 included studies (9, 10, 12-15, 109, 111, 122, 123, 125, 126, 128, 130-134, 136-141, 143-153), 15/30 studies identified higher age as risk factor for rCDI in univariate analysis, and 16/31 studies in multivariable analysis. Moreover, higher age was the only factor for which we found a moderate to large effect size and a dose-dependent effect.
Eight studies assessed whether a previous CDI recurrence in the preceding 3 months was a risk factor for a subsequent rCDI, and showed inconsistent results (9, 10, 15, 111, 125, 133, 140, 145). Two prospective studies of higher quality found a clear association of previous recurrence with the risk of a subsequent rCDI (111, 140). Also, data of the pivotal trials on fidaxomicin and bezlotoxumab indicate that recurrence rates are higher in patients with any previous CDI episode or patients that fulfill criteria for rCDI (156-160). Since these trials are considered high quality studies, we have upgraded the level of evidence from low to moderate (Table 3). Finally, we consider two or more episodes of CDI as risk factor for a subsequent rCDI.
Healthcare-acquired CDI was associated with rCDI in univariate analyses of 5/10 studies, and in multivariable analyses of 2/4 studies (9, 14, 111, 125, 128, 141, 144, 145, 149, 150). This is also reflected by the correlation of prior hospitalization (<3 months) with a recurrent episode of CDI (13, 15, 125, 128, 133, 138, 143, 149). The two largest cohort studies showed a significant association between prior hospitalization and rCDI in uni- and multivariable analysis (128, 149). Of note, one large cohort study reported a protective effect of community-acquired CDI for the development of rCDI (128).
Proton pump inhibitor use was studied in 23 included studies (9, 13, 14, 109, 122, 123, 130-135, 137, 139, 141, 145, 147-151, 153, 155). The results show no clear association between PPIs and rCDI in univariate analyses, while in multivariable analyses there appears to be an association. Of note, some studies made a distinction between the moment PPI was started, i.e. prior to initial CDI episode or during/shortly after the initial episode (12, 13, 15, 123, 125, 146, 149, 155); PPI prescribed during or shortly after initial CDI appears to be associated with an increased risk of rCDI (effect found in 6/7 studies in univariate analysis, and in 2/4 studies in multivariable analysis; low quality of evidence).
Eight studies reported on non-CDI antibiotic use after initial CDI diagnosis as a risk factor, but results were inconsistent (12, 123, 129, 136, 141, 145, 146, 148); 4/6 studies found an association between non-CDI antibiotic use and rCDI in univariate analysis, and 2/5 studies in multivariable analysis. A high-quality prospective study showed no significant association between antibiotic use and rCDI in both uni- and multivariate analysis (136). Several other studies investigated whether specific antibiotics that incited the primary CDI episode, were associated with recurrence; none of these antibiotic drugs was associated with rCDI. In conclusion, nor non-CDI antibiotic use prior to the primary CDI, nor concomitant non-CDI antibiotics used during the primary CDI episode, appeared to be convincing predictors for rCDI.
Although various definitions of sCDI are used in prognostic studies, most studies did not find severity of CDI to be a prognostic factor for rCDI (9, 123, 126, 131, 134, 140-142, 147, 150); 2/7 studies identified sCDI as risk factor for rCDI in univariate analysis, and 2/4 in multivariable analysis. In the MODIFY trials, sCDI was a prespecified risk factor for recurrence, but in the placebo arm the recurrence rate was lower in the sCDI subgroup (22.4%) than in the non-CDI subgroup (27.5%) (158). Since we expected sCDI to be a risk factor for rCDI, re-assessment of included studies was performed by a third researcher (CV-G); this did not alter our results. In conclusion, we found insufficient evidence to consider sCDI a risk factor for rCDI.
Several studies investigated specific comorbidities, including chronic renal failure, diabetes mellitus, and cardiovascular disease as risk factors for rCDI (9, 12-15, 111, 122, 123, 125, 126, 128, 130-134, 136, 138-154). Our review does not show any of these comorbidities to be clearly associated with an increased risk for rCDI. Even when combined into a robust score such as the Charlson Comorbidity Index, we did not identify a clear association (13, 65, 122, 130, 132-134, 140, 145, 146, 148, 150, 152). Since results of the uni- and multivariable analyses of studies reporting in renal failure were conflicting, these studies were re-assessed by a third researcher. This led to identical findings.
Immunocompromised status was a prespecified risk factor in the MODIFY trials; though in the placebo arm the recurrence rate in immunocompromised patients did not differ from that in immunocompetent patients (27.5% vs 26.6%) (158). A post-hoc analysis of the pivotal fidaxomicin trials investigated fever, leukocytosis and renal failure as prognostic markers, and identified renal failure as the only significant predictor for recurrence (RR, 1.45; 95% CI, 1.05–2.02). Overall, we found insufficient evidence to consider other comorbidities a risk factor for rCDI.
The ribotype 027 strain was not clearly associated with recurrence. However, only five studies reported on this ribotype as a possible risk factor (111, 123, 129, 145, 148); 2/5 studies found that the presence of a RT027 strain was associated with sCDI in univariate analysis, and only 1/3 studies in multivariable analysis. Since these results were inconsistent when compared to a previous systematic review, results were re-assessed by a third researcher (162). This reassessment did not result in different conclusions.
Laboratory parameters studied include white blood cell counts, and levels albumin, creatinine and C-reactive protein. None of these parameters was clearly associated with rCDI (10, 12-15, 111, 134, 141, 144-147, 149).
Our findings show the use of probiotics as prophylaxis for CDI seemed to be associated with rCDI (13, 14, 123, 133). However, this association is based on a small number of studies (n=4) and might be confounded by the fact that probiotics are started in patients with a high risk of rCDI and/or concomitant antibiotic use.
Conclusions
In this systematic review, we applied the GRADE methodology to weigh the evidence on prognostic factors for sCDI and rCDI (37). We found that the most important risk factors for sCDI were higher age (≥65-70 years old) and presence of multiple comorbidities. Higher age was also a prognostic factor for rCDI. Other factors associated with an increased risk of rCDI were the acquisition of CDI as a healthcare-associated infectionand prior hospitalization and the start of PPIs during/after CDI diagnosis. The evidence for having a previous recurrence of CDI as risk factor for rCDI was less strong.
Our systematic review on prognostic factors resulted in several expected and unexpected findings when compared with previous reviews rCDI (162-164). Our findings are in line with two recently published systematic reviews on predictors of sCDI that reported age and presence of comorbidities as the two most important severity predictors for CDI (162, 165). Similarly, previous reviews on prognostic factors for rCDI found that older age, prior CDI and PPI therapy were risk factors for rCDI (162-165). However, PPI therapy in general did not show a clear association in our study.
In contrast, we could not clearly identify several previously reported risk factors for sCDI or rCDI, such as infection caused by a ribotype 027/NAP1 strain, antibiotic use, PPI use prior to CDI diagnosis, and the presence of chronic or end-stage renal disease (162, 163). One possible explanation might be that many reviews excluded studies reporting solely univariate analyses. This might lead to an overestimation of the effect of certain prognostic factors, since many studies only include variables with a significant association in univariate analysis in their multivariable analysis. Another explanation for our findings might be index event bias: this bias arises in studies that select patients based on the occurrence of an index event, and can lead to ‘negative’ or even paradoxical findings in recurrence risk research (166). Here, we found that chronic renal failure did not appear to be associated with rCDI. Previous research shows that patients with kidney failure are prone to developing a primary CDI, but the direct association between kidney disease and rCDI is less clear (163, 167). Since reviews on rCDI select studies based on the occurrence of a primary CDI, this might explain why renal disease is not a strong predictor of rCDI in previous reviews, and not a significant risk factor in the current review.
Finally, when studying IBD as prognostic factor for sCDI/rCDI, another difficulty in interpretation arises, since symptoms of IBD are similar to those of CDI. Furthermore, patients with IBD are at higher risk of CDI and infection and colonization with C. difficile can induce an exacerbation of IBD (168). Also, diagnostic tests do not always allow to differentiate between C. difficile infection or colonization. Many clinicians pragmatically start antibiotic treatment in IBD patients without endoscopy. Subsequent false-positive CDI diagnoses may contribute to an overestimation of CDI (recurrence) risk. Aforementioned factors may have contributed to differences between the results of our current review and previous publications.
Our review has several strengths. First, we used a broad search strategy and included a large number of studies, minimizing the risk of missing data. Second, articles were selected based on strict predefined criteria by two independent researchers (TvR and RO). Third, the quality of the studies was judged by the structured prognostic GRADE approach. To our knowledge this approach has not been previously used for prognostic factors for sCDI and rCDI. Also, we reported results of both uni- and multivariable analyses. When results of the uni- and multivariable analyses of different studies were conflicting, we acknowledged this disparity and results were re-assessed by a third researcher. Reassessment was performed on the studies reporting the presence of RT027 strain, sCDI and renal disease as possible risk factors for rCDI, but this did not result in different conclusions. Finally, some disparity can be explained by the large number of studies where non-significant univariate prognostic factors were not included in the multivariate models.
A limitation is the generally low quality of available studies. Most studies have not performed a sample size calculation, allowing for possible type I and type II statistical errors. As many studies were retrospective, it was not always clear whether certain factors were already present before the occurrence of sCDI/rCDI (i.e. truly prognostic factors) or whether they co-existed. A second important limitation is the subjectivity how to weight different quality studies, which also resulted in stimulating discussions in our working group.
Identifying prognostic factors for sCDI and rCDI could aid clinicians to make an optimal treatment decision to reduce the risk of recurrent disease and decrease CDI complications. The findings of this review are especially relevant for rCDI: a risk stratification strategy may allow for selective use of more expensive novel treatments with less risk of recurrence. To implement risk stratification of in clinical practice, simple risk tools are needed. Currently, several prediction models or risk scores for scDI and rCDI have been developed (9-30). However, none has gained widespread clinical implementation. Based on the low quality of the studies and small effects of identified prognostic factors, it is not surprising that validation of prediction tools in external cohorts show disappointing results (169-171). Additional explanations are the heterogeneity and multimorbidity of the CDI population and variation in study setting, diagnostic criteria and CDI treatment regiments. The current review may be used as starting point for the development of a risk tool with a better performance in the overall CDI population. We suggest that future clinical trials on CDI treatment use standardized definitions for recurrence and severity and systematically collect and report the risk factors that we have discussed in this review, to allow for meaningful meta-analysis on risk factors using data of high-quality trials.
In conclusion, our approach identified higher age and the presence of multiple comorbidities as prognostic factors for sCDI. The only identified risk factors for rCDI were higher age, healthcare-associated CDI, prior hospitalization (<3 months), PPIs started during/after CDI diagnosis and rCDI. Some variables that were found as risk factors for sCDI/rCDI in previous reviews, were not confirmed in the current review, which can be attributed to differences in methodology. Risk stratification for sCDI/rCDI may contribute to a more personalized and optimal treatment for patients with CDI.
Data Availability
Not applicable (systematic review)
Transparency declaration
Conflict of interest disclosures, funding
TvR was supported by Netherlands Organization for Health Research and Development (ZonMw) grant Goed Gebruik Geneesmiddelen, project number 848016009. JK and EK received a research grant from Vedanta Biosciences (Boston, USA). The funders had no role in study design, data collection and interpretation, or the decision to submit the work for publication. All other authors: no conflicts of interest to disclose.
Contribution
JP and EK conceived the study on behalf of the ESCMID Study Group for Clostridioides difficile (ESGCD). JP designed the search strategy. TvR and RO selected the studies and acquired the data. TvR, RO, CV-G and JK graded selected studies. TvR, RO and OD analyzed the data. TvR and RO drafted the manuscript. All authors critically revised the manuscript and approved the final version.
Supplementary data
PICO’s
Two PICO’s were formulated:
Prognosis severe CDI:
P: patients with CDI
I: presence of clinical and laboratory parameters
C: absence of clinical and laboratory parameters
O: severe CDI
Prognosis recurrent CDI:
P: patients with CDI
I: presence of clinical and laboratory parameters
C: absence of clinical and laboratory parameters
O: recurrent CDI
Literature search prognosis severe CDI - Pubmed
((“Clostridium difficile Infection” [tw] OR “Clostridium difficile Infections” [tw] OR “C difficile Infection” [tw] OR “C difficile Infections” [tw] OR “clostridioides difficile infection” [tw] OR ((“Clostridium difficile” [majr] OR “Clostridium difficile” [ti] OR “C difficile” [ti] OR “c diff” [ti] OR “clostridioides difficile” [ti]) AND (“Clostridium Infections” [majr] OR “Clostridium Infection” [ti] OR “Clostridium Infection” [ti])) OR ((“Clostridium difficile” [majr] OR “Clostridium difficile” [ti] OR “C difficile” [ti] OR “difficile” [ti]) AND (“Clostridium Infections” [majr] OR “Clostridium Infection” [ti] OR “Clostridium Infection” [ti] OR “Infection” [majr] OR “infection” [ti] OR “infections” [ti] OR infect*[ti] OR “inflammation” [ti] OR inflammat*[ti] OR “Enterocolitis” [majr] OR “Enterocolitis” [ti] OR “colitis” [ti] OR “Digestive System Diseases” [majr])))
AND
(“Prognosis” [Mesh] OR prognos*[tw] OR “prognostic factor” [tw] OR “prognostic factors” [tw] OR “clinical parameter” [tw] OR “clinical parameters” [tw] OR “laboratory parameter” [tw] OR “laboratory parameters” [tw] OR “Age Factors” [mesh] OR “Age Factor” [tw] OR “Age Factors” [tw] OR “Age” [tiab] OR “Age Reporting” [tw] OR “Leukocytosis” [Mesh] OR “Leukocytosis” [tw] OR “Pleocytosis” [tw] OR “leucocytosis” [tw] OR “Leukemoid Reaction” [tw] OR “Lymphocytosis” [tw] OR (decreas*[tw] AND (“Serum Albumin” [mesh] OR “blood albumin” [tw] OR “serum albumin” [tw])) OR ((“rise” [tw] OR “rising” [tw] OR rise*[tw] OR increas*[tw]) AND (“serum creatinine” [tw] OR “Creatinine/blood” [mesh])) OR “severe underlying disease” [tw] OR “severe underlying diseases” [tw] OR “severe underlying illness” [tw] OR “severe underlying illnesses” [tw] OR “severe underlying condition” [tw] OR “severe underlying conditions” [tw] OR “Immunologic Deficiency Syndromes” [Mesh] OR “Immunologic Deficiency” [tw] OR “Immune Deficiency” [tw] OR “immunodeficiency” [tw] OR “Immunologic Deficiencies” [tw] OR “Immune Deficiencies” [tw] OR “immunodeficiencies” [tw] OR “Immunocompromised Host” [Mesh] OR “Immunocompromised” [tw] OR (strain*[tw] AND ribotype*[tw]))
AND
(“severe clostridium difficile” [tw] OR “severe cdi” [tw] OR “severe cd” [tw] OR “disease severity” [tw] OR “illness severity” [tw] OR “severity of disease” [tw] OR “severity of illness” [tw] OR “severe” [tw] OR “severity” [tw] OR sever*[tw])
NOT
((“Case Reports” [ptyp] OR “case report” [ti]) NOT (“Review” [ptyp] OR “review” [ti] OR “Clinical Study” [ptyp] OR “trial” [ti] OR “RCT” [ti])) NOT (“Animals” [mesh] NOT “Humans” [mesh])
AND
english[la])
Literature search prognosis recurrent CDI - Pubmed
((“Clostridium difficile Infection” [tw] OR “Clostridium difficile Infections” [tw] OR “C difficile Infection” [tw] OR “C difficile Infections” [tw] OR “clostridioides difficile infection” [tw] OR ((“Clostridium difficile” [majr] OR “Clostridium difficile” [ti] OR “C difficile” [ti] OR “c diff” [ti] OR “clostridioides difficile” [ti]) AND (“Clostridium Infections” [majr] OR “Clostridium Infection” [ti] OR “Clostridium Infection” [ti])) OR ((“Clostridium difficile” [majr] OR “Clostridium difficile” [ti] OR “C difficile” [ti] OR “difficile” [ti]) AND (“Clostridium Infections” [majr] OR “Clostridium Infection” [ti] OR “Clostridium Infection” [ti] OR “Infection” [majr] OR “infection” [ti] OR “infections” [ti] OR infect*[ti] OR “inflammation” [ti] OR inflammat*[ti] OR “Enterocolitis” [majr] OR “Enterocolitis” [ti] OR “colitis” [ti] OR “Digestive System Diseases” [majr])))
AND
(“Prognosis” [Mesh] OR prognos*[tw] OR “prognostic factor” [tw] OR “prognostic factors” [tw] OR “clinical parameter” [tw] OR “clinical parameters” [tw] OR “laboratory parameter” [tw] OR “laboratory parameters” [tw] OR “Age Factors” [mesh] OR “Age Factor” [tw] OR “Age Factors” [tw] OR “Age” [tiab] OR “Age Reporting” [tw] OR “severe underlying disease” [tw] OR “severe underlying diseases” [tw] OR “severe underlying illness” [tw] OR “severe underlying illnesses” [tw] OR “severe underlying condition” [tw] OR “severe underlying conditions” [tw] OR “Immunologic Deficiency Syndromes” [Mesh] OR “Immunologic Deficiency” [tw] OR “Immune Deficiency” [tw] OR “immunodeficiency” [tw] OR “Immunologic Deficiencies” [tw] OR “Immune Deficiencies” [tw] OR “immunodeficiencies” [tw] OR “Immunocompromised Host” [Mesh] OR “Immunocompromised” [tw] OR (strain*[tw] AND ribotype*[tw]) OR ((continued use*[tw] OR continuing use*[tw] OR prolonged use*[tw]) AND (antibiotic*[tw] OR antibacterial*[tw] OR anti-biotic*[tw] OR anti-bacterial*[tw])) OR “renal failure” [tw] OR “kidney failure” [tw] OR “Renal Insufficiency” [Mesh] OR “Renal Insufficiency” [tw] OR “Kidney Insufficiency” [tw] OR “kidney injury” [tw] OR “renal injury” [tw] OR previous infection*[tw] OR “Proton Pump Inhibitors” [Mesh] OR “Proton Pump Inhibitors” [Pharmacological Action] OR “Proton Pump Inhibitors” [tw] OR “Proton Pump Inhibitor” [tw] OR “initial severity” [tw] OR “initial disease severity” [tw] OR “initial illness severity” [tw] OR (strain*[tw] AND ribotype*[tw]))
AND
(“recurrent clostridium difficile” [tw] OR “recurrent cdi” [tw] OR “recurrent cd” [tw] OR “Recurrence” [Mesh] OR recurr*[tw])
NOT
((“Case Reports” [ptyp] OR “case report” [ti]) NOT (“Review” [ptyp] OR “review” [ti] OR “Clinical Study” [ptyp] OR “trial” [ti] OR “RCT” [ti])) NOT (“Animals” [mesh] NOT “Humans” [mesh])
AND
english[la])
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.
- 17.
- 18.
- 19.
- 20.↵
- 21.
- 22.
- 23.
- 24.↵
- 25.↵
- 26.
- 27.
- 28.
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.
- 40.
- 41.
- 42.↵
- 43.
- 44.↵
- 45.↵
- 46.↵
- 47.
- 48.
- 49.↵
- 50.
- 51.
- 52.↵
- 53.
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.
- 64.↵
- 65.↵
- 66.↵
- 67.
- 68.
- 69.
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.
- 77.↵
- 78.↵
- 79.
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.
- 87.↵
- 88.↵
- 89.↵
- 90.
- 91.↵
- 92.
- 93.↵
- 94.↵
- 95.
- 96.↵
- 97.↵
- 98.
- 99.
- 100.↵
- 101.↵
- 102.↵
- 103.
- 104.↵
- 105.
- 106.↵
- 107.
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.
- 113.↵
- 114.↵
- 115.
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.
- 121.↵
- 122.↵
- 123.↵
- 124.
- 125.↵
- 126.↵
- 127.
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.
- 158.↵
- 159.
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.↵
- 170.
- 171.↵



