
Abstract
Background Opioid prescribing trends have been well investigated in many countries. However, the patterns of opioids purchased over-the-counter (OTC) without a prescription are mostly unknown. Codeine is an opioid that is widely available OTC in many countries. We aimed to assess national sales and public expenditure of OTC codeine-containing products purchased in 31 countries between 2013 and 2019.
Methods We conducted a retrospective observational study using electronic point-of-sale data from IQVIA. Countries included Argentina, Belgium, Brazil, Bulgaria, Canada, Croatia, Estonia, Finland, France, Germany, Greece, Ireland, Italy, Japan, Latvia, Lithuania, Mexico, The Netherlands, Poland, Portugal, Romania, Russia, Serbia, Slovakia, Slovenia, South Africa, Spain, Switzerland, Thailand, the UK, and the USA. We calculated the annual mean volume of sales per 1000 of the population and public expenditure (GBP, £ per 1000) between April 2013 and March 2019. We quantified changes over time and the types of products sold.
Results 31.5 billion units of codeine, costing £2.55 billion, were sold OTC in 31 countries between April 2013 and March 2019. Total sales increased by 3% (3025 units/1000 in 2013 to 3111 in 2019) and public expenditure doubled (£196/1000 in 2013 to £301 in 2019). Sales were not equally distributed across the 31 countries. South Africa accounted for the largest mean volume of sales (31 units/person), followed by Ireland (24 units/person), France (16 units/person), Latvia (15 units/person), and the UK (11 units/person). The types of products (n=569) and formulations (n=12) varied.
Conclusions In many parts of the world, a substantial number of people may be purchasing and consuming codeine from OTC products. Clinicians should ask patients about their use of OTC products. Public health measures are required to identify and prevent codeine misuse and abuse, increase awareness and education about the harms of codeine, and review medicines legislation to improve the collection of such data.
Pre-registration https://doi.org/10.17605/OSF.IO/AY4MC
Introduction
The prescribing patterns of opioids are well recorded in many countries [1–5]. However, opioids such as analgesic combinations containing codeine can be purchased over-the-counter (OTC) without a prescription or consultation with a doctor or prescriber in most countries. As the access to granular data on OTC sales has been limited, previous research on the use of non-prescribed codeine has relied on case reports [6–8], self-reported questionnaires [9–16], qualitative studies [17–20], and data from poisons centres, hospital admissions, or coronial systems [21–25]. It is therefore unknown whether OTC codeine sales have followed similar trends to prescribed opioids.
Codeine (3-methylmorphine) is a naturally occurring opium alkaloid, an agonist at MOP receptors [26]. It is used for its analgesic, antidiarrheal, and antitussive effects [27–29]. Codeine is often combined with other analgesics, such as paracetamol, and non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen. A Cochrane overview of systematic reviews on oral OTC analgesics for acute pain found no studies or data that could be extracted on combinations of analgesics containing low doses of codeine [30]. Observational studies have shown that products containing codeine have been associated with dependence, misuse, death, and collateral toxicity from combinations with paracetamol and ibuprofen [7,23]. Access to codeine without a prescription can bolster the perception of safety, and in some settings, abuse of OTC codeine is normalised and encouraged. Mixing codeine cough syrup with alcohol and or soft drinks, called “purple drank”, has been popularised in rap music and by American athletes [31]. OTC codeine has also been used to manufacture illicit morphine and heroin, including a cheap heroin substitute called “krokodil” [32,33]. The use of krokodil has been reported in Russia, Europe, the UK, and North America, and its adverse effects include damage to blood vessels, skin, muscles, and bones, multiorgan failure, and death [32,34]. Thus, the growing opioid problem is incomplete without evaluation of OTC sales of codeine.
Regulation of codeine-containing products varies across the world, making it difficult to estimate how much they are used [35]. Under the 1961 Single Convention on Narcotic Drugs, codeine is a Schedule III drug [36]. Drugs in this Schedule reportedly “are not liable to abuse and cannot produce ill effects”, and thus it is not mandatory to report data on their consumption to the International Narcotics Control Board (INCB). However, governments also mandate the regulation of codeine. Minnesota (July 2013), Manitoba (February 2016), France (July 2017), and Australia (February 2018) have reclassified codeine to prescription-only [35,37–39]. In our rapid review of codeine regulations in 31 countries (Table 1), codeine was available OTC in 42% of countries; 39% reported no access, 6% had variable access (i.e. Canada and the USA), and for 13% of countries, we did not identify legislation to validate the status of codeine. Despite variation in codeine’s regulatory status, we acquired sales data for all available countries from the human data science company IQVIA [40], formerly Quintiles and IMS Health. Previous studies have used data from IQVIA to examine the consumption of OTC cough syrup containing codeine in Taiwan [41] and to evaluate the impact of rescheduling codeine to prescription-only in Australia [42,43]. We therefore aimed to assess national sales and public expenditure on OTC codeine-containing products purchased in 31 countries between 2013 and 2019.
Rapid review of OTC codeine regulations in 31 countries included in this study, ordered alphabetically
Methods
We conducted a retrospective observational study using consumer health sales data from IQVIA [40], which has previously been used in observational research on a range of medications [41–43,53–56]. The data included products containing codeine in the adult pain relief category, which were collected using scan track barcodes from electronic point-of-sale (EPoS) store data. IQVIA extracted the data on 16 September 2019 and provided quarterly sales from 1 April 2013 to 31 March 2019. IQVIA’s sample of data is based on audits and covers a median of 73% (IQR: 58-86%) of pharmaceutical markets (Table S1 in Supplement 1). Annual population statistics in calendar years (2013 to 2018) were sourced from the World Bank [57].
We extracted details from the pack information and used descriptive statistics to determine the numbers and types of products, formulations, substances in combinations, pack sizes, and dosages sold across the 31 countries. We calculated the total volume of sales over the study period and the totals for each year (e.g. from quarter two in 2013 to quarter one in 2014). We also calculated the mean volumes of sales over six years, adjusted for population. We created an annual rate of units sold per 1000 of each year’s population for each country to examine trends over time. To standardise and combine sales for liquid and solid dosage forms, we used standard units calculated by IQVIA, as data on dosages were missing from the pack information for most countries. For expenditure, IQVIA converted sales to pounds sterling (GBP, £) for each country on the date of data extraction (16 September 2019). We calculated annual totals, mean public expenditure for each country, adjusted for population, and a rate of GBP per 1000 to assess changes over time.
Software and data sharing
We used Stata v16 and Python v3 in Jupyter Notebooks with pandas [58], seaborn [59], and matplotlib [60] libraries for analysis and figures. The data used is commercial information that requires a fee to access. Thus, we cannot openly share the data owing to contractual agreements with IQVIA. However, we have openly shared our statistical code at GitHub [61], preregistered [62] and published [63] our study protocol, and shared all our study materials via the Open Science Framework (OSF) [64].
Patient and public involvement
We involved three patients who have chronic pain and experience of taking opioids (including OTC codeine) and other medicines for pain at the analysis phase of our research. Lead author (GCR) presented the preliminary findings to the patients during a formal face-to-face patient and public involvement meeting in December 2019. Patients provided suggestions for final analyses, the presentation of results, and dissemination plans.
Results
31.5 billion units containing codeine were sold across 31 countries over the study period (April 2013 to March 2019). The total sales volume increased by 2.8%, from 3025 units/1000 in 2013-14 to 3111 units/1000 in 2018-19. However, the distribution of sales between countries was not uniform. Five countries represented 90% of all OTC codeine sales. South Africa accounted for the greatest volume of sales (34%), followed by France (20%), Japan (16.5%), the UK (14.5%), and Poland (5%). South Africa had the largest mean volume of OTC codeine sales (mean of 31 units/person, see Figure 1), followed by Ireland (24 units/person), France (16 units/person), Latvia (15 units/person), and the UK (12 units/person).
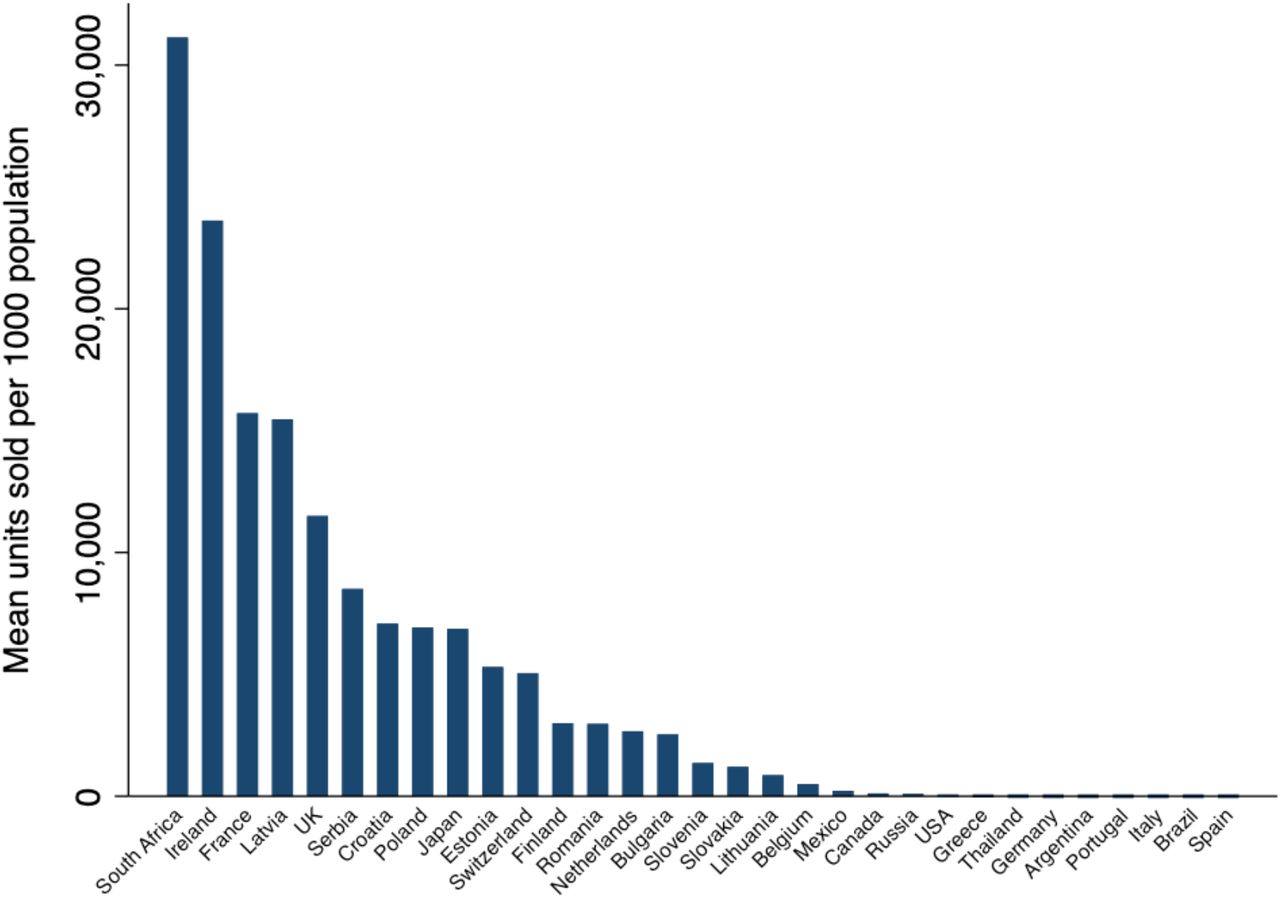
Mean volumes of OTC codeine-containing units sold over six years in 31 countries with available data, ranked by countries with the largest to least volumes of sales
In the most recent year (April 2018-March 2019), South Africa had the largest volume of sales (38 units/person), followed by Ireland (23 units/person), Latvia (16 units/person), the UK (11 units/person), and Japan (10.7 units/person), Table S2 in Supplement 1.
Over time, 48% of countries (15/31) had an increase in OTC codeine sales. For countries in the top quartile of sales (Figure 2A), trends increased in South Africa (30%), Ireland (8%), Latvia (11%), and Poland (19%), and sales fell in France (99%), the UK (7%), Serbia (4%), and Croatia (17%). For countries in the second-largest quartile of sales (Figure 2B), trends increased in Japan (1219%), Estonia (65%), Romania (10%), and Bulgaria (18%), and sales fell in Switzerland (50%), Finland (22%), The Netherlands (16%), and Slovenia (16%). Trends for countries in the bottom two quartiles are in Figure S1 and S2 in Supplement 1.

Sales of over-the-counter products containing codeine per 1000 of the population starting in April 2013-March 2014, and ending in April 2018-March 2019, for countries in the top quartile (A) and second quartile (B) of sales.
The public spent £2.55 billion on OTC codeine-containing products in 31 countries over six years; expenditure increased by 54%, from £196/1000 in 2013-14 to £301/1000 in 2018-19. Ireland had the largest mean public expenditure of £5.70 per person, followed by the UK (mean of £1.60/person), South Africa (£1.26/person), Croatia (£1.25/person), and Estonia (£1/person), Figure 3. In April 2018-March 2019, Ireland continued to have the largest public expenditure (£6.60/person), followed by South Africa (£1.64/person), the UK (£1.64/person), Japan (£1.47/person), and Estonia (£1.41), Table S2 in Supplement 1.

Public expenditure on OTC codeine-containing units sold over six years in 31 countries with available data, ranked by countries with the largest to least volumes of sales
Most countries (58%, 18/31) had increased public expenditure over time. There were simultaneous increases (45%, 14/31) and decreases (39%, 12/31) in both sales and expenditure in most countries, while other countries (16%, 5/31) had a discordance in the direction of their sales and expenditure (Figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage changes in sales volumes (units sold per 1000 of the population) and public expenditure (£ per 1000 of the population) for products containing codeine sold OTC in all 31 countries between April 2013 and March 2019
There were 569 products and 12 formulations sold across 31 countries. Tablets were the most common formulations sold, followed by syrups, soluble tablets, and coated tablets (Figure S3 in Supplement 1). Products contained a median of three substances per combination (IQR: 2-4, range: 1-16). Limited details were available in the pack information: the dosages of codeine were available in 17% of products (98 of 569) in 15 countries.
Discussion
Between April 2013 and March 2019, 31.5 billion units of codeine, costing £2.55 billion, were sold OTC in 31 countries, as collected by IQVIA. In line with increasing opioid use globally [65], total sales and public expenditure of OTC codeine increased by 3% and 54% respectively. South Africa, Ireland, and France had the greatest mean volumes of OTC codeine sales per person. Ireland, the UK, and South Africa had the largest mean public expenditure per person. However, sales were not equally distributed across the 31 countries.
At the country level, the wide variation of sales may be attributable to changes in regulations of OTC codeine and differences in trade exemptions and disclosures of commercial interests [35]. For example, our findings illustrate the regulatory impact of codeine becoming prescription-only in France. Countries that previously consumed large volumes of opioids, such as Canada, Germany, and the USA [66], had lower mean sales of OTC codeine products than others. However, IQVIA’s data coverage for the USA was low at 47% compared with the median coverage of 73%. Thus, whether the wide variation in mean sales volumes is a true representation of real differences between countries is difficult to quantify with available data.
Strengths and limitations of the study
We used IQVIA’s standard units to measure sales, which allowed for liquid and solid dosage forms to be combined. The figures represent population-level sales and expenditure based on IQVIA’s data coverage, providing a proxy for actual use. While the varying regulations of access to OTC codeine may play a role, the skewed distribution of mean sales volumes may also be attributed to IQVIA’s data coverage and the completeness of data. IQVIA provided their coverage at a single time point in 2020, which may have changed throughout the study period. Codeine-containing products may also be purchased from online pharmacies or the black market in large quantities [67], not captured in these data. IQVIA also converted expenditure to GBP for all countries at a single time point in 2019, which may not accurately represent each country’s currency value across the six years. Although the sales represented adult pain relief, we calculated rates using population statistics for all age groups, including children.
Implications for clinicians and policymakers
Our findings show that many people are purchasing OTC codeine products in many parts of the world. However, the impact of this level of access and use of codeine is unclear. According to IQVIA’s data, South Africa consistently had the largest volume of OTC codeine sales each year. A study of opioid dependence in South Africa showed that 5-8% of people in addiction treatment facilities reported problems with OTC codeine medications and cough mixtures as their primary or secondary drug of choice [68]. Availability of non-prescribed codeine may also have ramifications for neighbouring countries that restrict access. For example, there were reports in Zimbabwe, which outlawed OTC codeine syrups in 2015, that codeine-containing cough syrup was being illegally smuggled in from South Africa and sold on the streets [69]. Therefore, it is likely that the extent of harms and prevalence of codeine misuse, abuse, and dependence is under- and un-reported in many countries.
Abuse of OTC codeine products is being encouraged and normalised on social media and in hip-hop music [70–72], which is a growing public health concern. One study showed that drug-related messages in music predicted substance misuse in young adults aged 16-25 years and that drug-related slang was nearly 19 times more common in 2017 than in 2007 [72]. A scoping review on the non-medical use of pharmaceuticals identified several ways in which codeine was reportedly abused, including mixtures with alcohol or soft drinks (e.g. “purple drank”) and in the production of home-made opiates (e.g. “krokodil”) [73]. Public health interventions are needed to prevent abuse, misuse, and pharmacy shopping of OTC codeine products, particularly in young adults. The hip-hop song entitled “1-800-273-8255”, the US suicide prevention lifeline, significantly increased public awareness of and calls to the hotline [74]. Thus, hip-hop music can also be used to tailor public health messages to young adults and counteract the glamourisation of codeine misuse.
The growing recognition of codeine abuse and misuse has led several governments to reclassify codeine to prescription-only [37–39]. In South Africa, Canada, Switzerland, Ireland, and the UK, governments are proposing or considering plans to reclassify codeine-containing products to prescription-only [52,75–77]. Studies assessing the effect of rescheduling codeine to prescription-only in Australia showed a reduction in all codeine-related poisonings and no change in calls to poisons centres or sales of high-strength (>15 mg) prescribed codeine following reclassification [42,78]. The success of Australia’s rescheduling questions whether governments worldwide should make codeine prescription-only. But since many low- and middle-income countries experience barriers to accessing opioids [65,66,79], the WHO recommends that codeine should not be up-scheduled and continues to include codeine in its Model List of Essential Medicines [80]. If a consensus on the status of OTC codeine products cannot be reached, data should be collected globally to monitor the use and harms of OTC codeine products.
Our study illustrates the limitations of available OTC data and the need for a global strategy involving governments, regulators, researchers, and public health organisations to mandate the reporting and sharing of OTC sales of codeine by pharmacists, wholesalers, and manufacturers. Amendments to medicines legislation in the UK provides an example of how such data could be collected. The Misuse of Drugs Regulation 2001, the Medicines for Human Use (Administration and Sale or Supply) (Miscellaneous Amendments) Order 2007, and the Medicines (Sale or Supply) (Miscellaneous Provisions Amendment Regulations 2007) was updated to mandate that pharmacies must submit counts of private prescriptions for Schedule 2 and Schedule 3 controlled drugs to the NHS Prescription Services for analysis, audit, and monitoring [81,82]. A similar system could be enforced through a public health organisation such as the WHO or the INCB, which already collects annual drug statistics from governments on opioids [83]. Such data could then be used by governments and researchers to monitor sales of OTC codeine and measure the impact of regulatory changes.
Conclusions
Codeine is one of the most widely accessible and used opioids worldwide. However, monitoring its use and preventing its misuse is a public health challenge. Unlike the US-style opioid crisis, codeine misuse and abuse are not restricted to high-income countries or those over-prescribing opioids. Public health measures are needed to identify and prevent codeine misuse and increase awareness and education of the harms of codeine, particularly in young adults. Clinicians should ask patients about their use of OTC products and governments should review medicines legislation to improve the safety of products sold OTC containing codeine.
Data Availability
Study materials, protocol, and statistical code are openly available on our OSF repository [64] (https://osf.io/yt6bf/) and at GitHub [61] (https://github.com/georgiarichards/otc_codeine). We cannot openly share the data owing to contractual agreements with IQVIA, but the data can be accessed directly from IQVIA, which will require a fee.
Ethics approval
Not applicable
Contributions
GCR devised the research question, designed the methods, wrote the protocol, conducted a literature search and rapid review of OTC codeine regulations in 31 countries, sourced the data, cleaned, managed and analysed the data, created the figures, and wrote the first draft of the manuscript. JKA and CH reviewed the protocol and preliminary findings and provided supervisory support. FDRH reviewed the protocol and facilitated the grant application. BM reviewed preliminary findings and contributed to the interpretation of data. BG provided supervisory support. All authors have full access to all the data in the study, read, and approved the final manuscript, and accept responsibility to submit for publication.
Role of funding source
The Primary Care Research Trust of Birmingham and Midlands Research Practices Consortium provided the funds to purchase the sales data from IQVIA. The sponsor was not involved in the study design, collection, analysis or interpretation of data, writing of the manuscript, or decisions on submitting the manuscript for publication. The researchers had full access to all the data used in this study, which was independent from the funders. The authors take responsibility for the integrity of the data and the accuracy of the data analysis.
Declarations of interests
GCR was financially supported by the National Institute for Health Research (NIHR) School for Primary Care Research (SPCR), the Naji Foundation, and the Rotary Foundation to study for a Doctor of Philosophy (2017-2020), but no longer has any financial COIs. GCR is an Associate Editor of BMJ Evidence Based Medicine. JKA has published articles and edited textbooks on adverse drug reactions and interactions and has often given medicolegal advice, including appearances as an expert witness in coroners’ courts, often dealing with the adverse effects of opioids. BM works for NHS England as a pharmacist adviser. BG has received research funding from the Laura and John Arnold Foundation, the NIHR, the NIHR SPCR, the NIHR Oxford Biomedical Research Centre, the Mohn-Westlake Foundation, NIHR Applied Research Collaboration Oxford and Thames Valley, the Wellcome Trust, the Good Thinking Foundation, Health Data Research UK (HDRUK), the Health Foundation, and the World Health Organisation (WHO); he also receives personal income from speaking and writing for lay audiences on the misuse of science. FDRH acknowledges part support from the NIHR School for Primary Care Research (SPCR), the NIHR Applied Research Collaboration (ARC) Oxford Thames Valley, and the NIHR Oxford OUH BRC. CH is an NIHR Senior Investigator and has received expenses and fees for his media work, received expenses from the WHO, FDA, and holds grant funding from the NIHR SPCR and the NIHR SPCR Evidence Synthesis Working Group [Project 380], the NIHR BRC Oxford and the WHO. On occasion, CH receives expenses for teaching EBM and is also paid for his GP work in NHS out of hours (contract with Oxford Health NHS Foundation Trust). CH is the Director of the CEBM. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Transparency statement
The lead author (GCR) affirms that the manuscript is an honest, accurate, and provides a transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as originally planned have been explained.
Data sharing
Study materials, protocol, and statistical code are openly available on our OSF repository [64] (https://osf.io/yt6bf/) and at GitHub [61] (https://github.com/georgiarichards/otc_codeine). We cannot openly share the data owing to contractual agreements with IQVIA, but the data can be accessed directly from IQVIA, which will require a fee.
Supplementary material
Supplement 1: Supplementary tables and figures
References



