
Summary
Being unable to suppress SARS-CoV-2 transmission, the majority of countries worldwide have resorted to a mitigation approach towards COVID-19, allowing some degree of viral circulation in the population. Here, we investigate the expected outcomes of the interplay between vaccination rollout and adaptive mitigation measures constantly altering the epidemic trajectory and keeping the reproduction number around the unit. Using a novel mathematical modeling framework, we estimate that, for vaccination capacities of at least 4 daily doses administered per 1,000 inhabitants, a complete release of mitigation measures can be expected within 7 to 13 months since the start of vaccination, with a two-year cumulative incidence of deaths between 0.18 and 0.46 per 1,000 population. A heavier burden of deaths and a delayed “return-to-normal” is expected for lower vaccine capacities, if viral transmissibility exceeds by >60% the one estimated at the beginning of the pandemic, or if vaccine protection is short-lived. Failure to prioritize the elderly or a premature release of mitigation measures after vaccination of the most fragile will conspicuously increase the expected mortality. Finally, strategies oriented to prioritize the suppression of SARS-CoV-2 by maintaining strict restrictions will take a similar time as a mitigation approach, possibly resulting in acceptability issues. Persisting unknowns about the evolving epidemiology of SARS-CoV-2 variants and on the effectiveness of available and upcoming vaccines may warrant a future reassessment of these conclusions.
Main Text
Since December 2020, vaccinations against COVID-19 are being rolled out in many countries of the world, in a race to put an end to a pandemic that has caused millions of lives lost [1], devastating economic effects [2], and a tremendous impact on mental health [3]. Limitations in the supply of COVID-19 vaccines and in the logistics of rollout imply that several months will elapse before immunization campaigns can have a significant impact [4]. Meanwhile, non-pharmaceutical interventions (NPIs) will remain the main tool to maintain control of the epidemic. While China and a few other countries in South-East Asia and Oceania have successfully pursued a zero-COVID policy [5] with suppression of transmission via aggressive localized lockdown policies and strict border control, most countries in the world resorted to mitigation strategies [6], adjusting physical distancing restrictions (PDRs) in the attempt to balance a low level of viral circulation with individual freedoms and economic losses. In practice, this balance is not always achieved as desired, resulting in an alternance between periods of constant or declining circulation and new resurgences, to which correspond phases of relaxation and intensification of PDRs. Projecting the impact of vaccination under unstable conditions is complex and most approaches today have assumed constant restrictions and various degrees of epidemic severity while vaccination is implemented [4, 7-10]. Here, we propose a different approach by simulating the effect of a vaccine rollout under perfect mitigation, i.e., assuming that governments will be capable to maintain an approximately constant incidence by adjusting PDRs as immunity accumulates.
Vaccination programs under mitigation
We developed a susceptible-infectious-recovered (SIR) mathematical model of SARS-CoV-2 transmission, structured by age and accounting for age-specific susceptibility, contacts, and prevalence of comorbidities. Incidence is maintained approximately constant over time during vaccine rollout by continuously recalibrating a scaling factor, roughly representing the proportion of pre-pandemic contacts allowed by the existing PDRs (see Appendix). As population immunity accrues due to natural infection and vaccination, the proportion of allowed contacts will increase until all pre-pandemic contacts are eventually resumed, representing the process of PDRs relaxation.
The impact of vaccination is quantified in terms of cumulative deaths and of the relaxation of PDRs. The latter is reported as the percent increase in allowed contacts, with 0% representing restrictions needed to have a constant incidence at the start of the vaccination program, and 100% representing complete reopening. Additionally, we estimate the time to “zero-COVID” defined as no reported cases for at least two consecutive weeks; by zero-COVID we refer to a situation similar to the one achieved by countries in Asia and Oceania, where no cases are usually detected but local flare-ups may occur due to importation of cases (e.g., outbreaks in under-vaccinated communities). We take Italy as a case study and simulate the process over a time horizon of two years.
As a baseline, we consider a two-dose vaccination campaign under the following assumptions: i) an incidence of reported cases maintained at about 50 cases per week per 100,000 population; ii) a vaccination coverage of 75%; iii) a daily capacity of 4 doses per 1,000 population; iv) prioritization based on the WHO SAGE roadmap [11] (Appendix); v) vaccines prevent infection; vi) protection is long-lasting (> 2 years); vii) vaccine is administered independently of a previous COVID-19 infection. These assumptions are then modified in a number of alternative scenarios and sensitivity analyses.
In the absence of vaccination and under mitigation measures, we estimate 1.68 cumulative COVID-19 deaths per 1,000 population (95%CI: 0.95-2.79), occurring uniformly over the two years (Figure 1A). The natural immunity achieved by viral circulation allows a limited relaxation of PDRs, estimated between 20 and 30% in the fourth semester (Figure 1B), with a large residual potential for new epidemic waves: the effective reproduction number at the end of simulations is estimated at 1.4-1.6 (Appendix). These results suggest that in the absence of vaccination, the only viable way to control COVID-19 infections would be to maintain strict PDRs in the very long term.

A) Estimated incidence of deaths within each of the four simulated semesters. B) Average amount of PDRs relaxation over each semester. Bars indicate the mean and vertical lines the 95% projection interval. C) overall comparison using the cumulative incidence of deaths and the average relaxation of PDRs over the two simulated years. Individual stochastic simulations are shown as points, the mean of their bivariate distribution as crosses and its 75-percentile as closed curves.
In the baseline scenario, the vaccination campaign is expected to be completed after about 13 months. Vaccination can limit cumulative deaths to 0.36 per 1,000 (95%CI: 0.21-0.59), i.e., almost 80% less than in absence of vaccination (Figure 1A). In addition, PDRs might be completely relaxed by month 12, with most of the relaxation occurring rapidly over the second semester (Figure 1B), and zero-COVID might be achieved after about 18 months (95%CI: 17-20).
The effect of a vaccination campaign may depend on several factors. Some of these depend on organizational and public health choices, e.g., how fast available vaccine doses are administered, or which population segments are prioritized. A halved vaccination capacity (2 daily doses per 1,000 population) would imply a completion of the program after over 2 years, with continued circulation after that date. In addition, it would result in a higher mortality compared to the baseline (0.63 per 1,000; 95%CI: 0.36-1.03) and in a slower relaxation of PDRs, which is expected to be complete by month 21 (95%CI: 19-22, Figure 2A). Vaccination capacities higher than the baseline would have a limited impact on the burden of deaths, but they would allow a quicker relaxation of PDRs, reaching complete reopening at month 9 and 8 for vaccination capacities of 6 and 8 daily doses per 1,000 population, respectively. Simulations of alternative prioritizations (details in Appendix) suggest that targeting population segments with highest contact rates may allow a more rapid relaxation of PDRs (3 to 5 months earlier than the baseline when prioritizing schoolchildren, but only 1 month earlier when prioritizing working-age adults), at the cost of a two- to three-fold mortality burden compared to the baseline (Figure 2B).

A) vaccination capacities; B) vaccine prioritizations (details in Appendix); C: vaccine coverages; D) duration of vaccine protection. Top panels show the estimated incidence of deaths within each of the four simulated semesters. Middle panels show the average amount of PDRs relaxation over each semester. Bars indicate the mean and vertical lines the 95% projection interval. Bottom panels compare scenarios using the cumulative incidence of deaths and the average relaxation of PDRs over the two simulated years. Individual stochastic simulations are shown as points, the mean of their bivariate distribution as crosses and its 75-percentile as closed curves.
The population’s willingness to receive the vaccine is represented by the achievable coverage. A 60% coverage would anticipate the relaxation of PDRs by switching earlier from high-risk to high-transmission population segments, but it would result in about 0.46 cumulative deaths per 1,000 population (95%CI: 0.26-0.79) in two years (Figure 2C). Conversely, an increased coverage to 90% would not significantly reduce the mortality burden, but it would delay the complete relaxation of PDRs by about 1.5 months compared to the baseline.
One of the main unknowns on vaccine performance is the duration of vaccine protection. When assuming that protection wanes on average 1 year or 6 months after administration, in absence of a re-vaccination campaign we estimate a steep resurgence of deaths starting from the third semester, and the need to reinstate stricter PDRs during the fourth semester to counter the rising reproduction number of SARS-CoV-2 driven by the refueling of the susceptible reservoir. In these scenarios, we estimate 1.34-1.57 deaths per 1,000 population (with a wide uncertainty ranging from 0.63 to 2.56 per 1,000, Figure 2D) in two years. We note however that the end of the vaccination campaign around month 13 in the baseline scenario implies that even with a short duration of vaccine protection, re-vaccination is feasible before the deterioration of the epidemiological situation, if vaccine stockpiles/supplies are sufficient.
Increased transmissibility
Another major uncertainty in the evolving SARS-CoV-2 epidemiology is the emergence of viral lineages with increased transmissibility [12-14]. We tested the effect of vaccine rollout assuming a transmissibility that is 20% to 80% higher than what estimated initially for SARS-CoV-2. In such case, we expect a possibly substantial increase in total deaths by up to 140% higher for transmissibility increased by 80% (Figure 3A) and by up to 290% when considering also a higher lethality of the variants [15-16] (Appendix). Zero-COVID is generally not achieved in two years unless the increase in transmissibility remains below 20%. PDRs will have to be intensified in the first semester compared to the baseline (represented in Figure 3A by negative values), maintaining levels similar to the baseline’s initial ones throughout the second semester; however, the complete relaxation is expected within month 14 (95%CI 13-15) even with a transmissibility increased by 60%. Only in the worst case we expect a complete reopening later than month 17.

A) increased transmissibility; B) limits to PDR relaxations to suppress transmission; C) complete reopening after immunization of the most fragile. Top panels show the estimated incidence of deaths within each of the four simulated semesters. Middle panels show the average amount of PDRs relaxation over each semester. Bars indicate the mean and vertical lines the 95% projection interval. Bottom panels compare scenarios using the cumulative incidence of deaths and the average relaxation of PDRs over the two simulated years. Individual stochastic simulations are shown as points, the mean of their bivariate distribution as crosses and its 75-percentile as closed curves.
We evaluated the sensitivity of model outputs with respect to several other variables (Appendix). When allowing incidence levels higher than 50 weekly cases per 100,000, the accumulation of immunity from natural infections speeds up the relaxation of PDRs but the death burden increases proportionally. When considering a vaccine efficacy reduced by 15%, we found up to 50% more deaths, with minimal impact on the time to complete relaxation of PDRs. If the vaccine provides protection against disease, but not against infection, we expect a doubled number of deaths at the end of the two years, and PDRs would not be relaxed by more than 40%. A homogeneous susceptibility to infection (rather than reduced in children and increased in older adults [17-18]) would reduce deaths by 40%. Finally, model results were substantially insensitive to uncertainties in the value of initial immunity.
Alternative strategies: SARS-CoV-2 suppression or early reopening
Governments may choose to use the population immunity conferred by vaccines to achieve zero-COVID sooner by not lifting PDRs until it is safe to do so without the risk of new resurgences. Mixed strategies may also be adopted where PDRs are lifted up to a certain point, and then priority is given to suppression. When no relaxation of PDRs is allowed since the start of vaccination, zero-COVID would be anticipated at month 12 since vaccination start (95%CI: 10-13, Figure 3B), after which a complete reopening could be safe due to the below-threshold transmission potential (Appendix). We estimate a cumulative incidence of 0.18 deaths per 1,000 population (95%CI: 0.11-0.30) for this scenario, roughly half than the baseline. When allowing a 25%, 50% or 75% relaxation of PDRs before aiming for suppression, zero-COVID would occur on month 14, 16 and 17, and the resulting cumulative incidence of deaths would be 0.28 (0.17-0.46), 0.33 (0.19-0.54) and 0.35 (0.20-0.58) per 1,000 (Figure 3B).
An opposite strategy might be to maintain mitigation measures until the most fragile population segments (individuals above 60 years of age or with comorbidities) are protected. After this milestone, occurring around month 6 since vaccination start under baseline assumptions, all PDRs are completely removed. Despite the protection of the high-risk population, a high incidence of cumulative deaths is expected (1.14 per 1,000, 95%CI: 0.70-1.63, Figure 3C), due to a large epidemic wave that would occur following the premature dismission of mitigation measures.
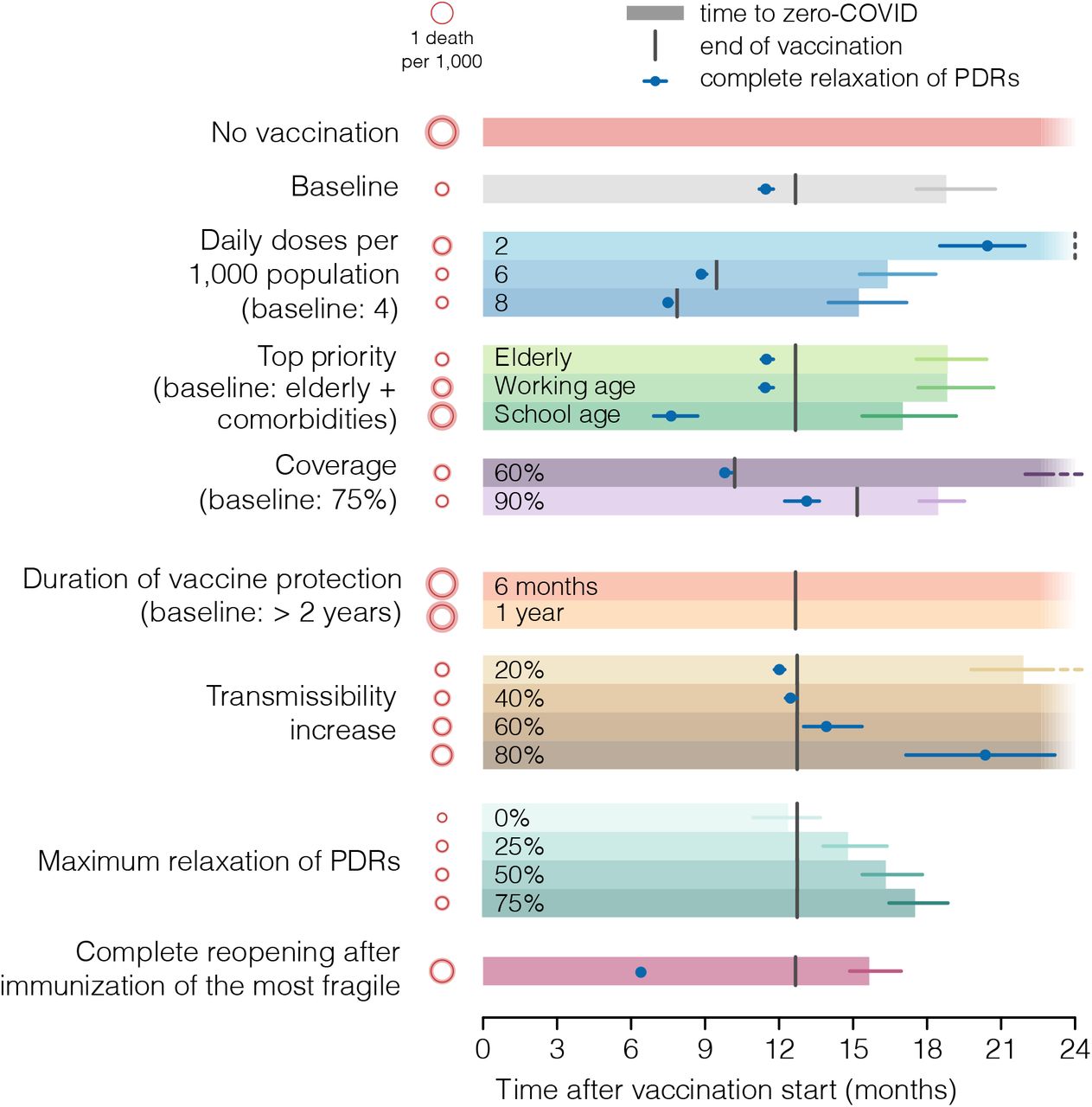
A summary comparison of key results for all considered scenarios is represented in Figure 4.

Red circles show the mean estimated mortality burden over the two years with shaded areas representing the 95% projection intervals. Bars show the mean time to zero-COVID and horizontal lines the 95% projection interval. Fading bars indicate no zero-COVID on average within 24 months; for scenarios with 60% coverage and 20% increased transmissibility, about 30% and 93% of simulations are expected to result in zero-COVID before month 24 respectively (dashed horizontal lines). Vertical lines indicate the end of vaccination programs (fixed, given capacity and coverage). A dashed vertical line indicate completion after 24 months. Blue points and horizontal blue lines indicate the mean and 95% projection interval for the time at which a complete relaxation of PDRs is reached. For scenarios with limited relaxations of PDRs, blue lines are not shown because complete relaxation occurs when zero-COVID is achieved.
Discussion
We examined the effect of COVID-19 vaccination programs in countries which were not able, to date, to suppress circulation of the virus. Under the assumption that existing vaccines confer protection from infection (rather than just disease) and that immunity is long-lived (>2 years), the combination of vaccine roll-out and effective mitigation strategies is expected to prevent a large proportion of deaths while at the same time allowing a progressive lifting of physical distancing restrictions. A complete return to a pre-pandemic lifestyle can be expected between 7 and 15 months since the start of vaccination in most scenarios (Figure 4), provided that a vaccination capacity of at least 4 doses per 1,000 population per day is achieved. Zero-COVID, i.e., suppression of transmission similar to the one observed in some Asian and Oceanian countries, would occur approximately 6 months thereafter. Higher capacities are not expected to produce major reductions in the number of deaths but will help release restrictions more rapidly. Another critical parameter will be the duration of vaccine-induced protection: if vaccine protection will last 1 year or less on average, re-vaccination must be deployed as soon as the primary campaign is over (13 months since its start in the baseline case); otherwise, the relaxation of PDRs will need to be reversed at some point, and the number of deaths will rise dramatically. We also explored the impact of more transmissible variants [12-14]: stricter mitigation measures than those existing in many countries in December 2020 are required throughout at least the first semester, but the timing to complete reopening should remain within 15 months as long as the increase in transmissibility does not exceed 60% compared to historical lineages. In any case, the additional transmissibility will result in a much larger number of lives lost (up to four-fold the baseline value if variants are also more lethal [15-16]).
We also evaluated the possibility that countries will relax PDRs only up to a certain point, using the buildup of population immunity to pursue suppression of transmission. In the case that no relaxation of PDRs is allowed, zero-COVID can be obtained in about 12 months, after which the transmission potential will have fallen below the epidemic threshold and a complete reopening may be allowed. This suppression-oriented approach requires a similar time until complete reopening than the mitigation approach with a halved burden of deaths. However, the tradeoff here is the need to maintain restrictions for a long period, with negative effects on the economy and population’s mental health and likely acceptability issues for the public, faced with a steadily declining incidence. On the opposite, pressures to reopen society may be expected after the daily incidence of deaths will have dropped to low values due to the vaccination of the most fragile. We show that if social contacts are completely resumed after the vaccination of fragile individuals is completed (about 6 months into the vaccination program), a major epidemic is to be expected with a large death toll.
There are a number of limitations that must be kept in mind when interpreting our results. First, we did not explicitly model which PDRs are relaxed as vaccination progresses; instead, we assumed a generic relaxation of measures that impacts all ages proportionally. The age-specific effect of relaxing existing PDRs is extremely hard to quantify, and their prioritization is a peculiarly political decision, depending on the governments’ strategic interests. Second, we assume mitigation measures to maintain an approximately constant incidence; although this dynamic is clearly idealized, we consider this an acceptable approximation of the fluctuating incidence observed in most countries. We anticipate that possible resurgences due to imperfect mitigation will contribute to speed up the population immunity and therefore the relaxation of PDRs, however at the cost of more lives lost. Third, we did not explicitly model the effect of other possible features of emerging variants, such as reductions in vaccine effectiveness [19-20] or the ability to escape natural immunity [13, 21-22], or a combination of them. We estimate that a 15% lower efficacy of vaccines under the transmissibility of historical lineages would imply an increase in deaths of up to 50%, without affecting the time to a complete relaxation of PDRs. The possibility of escape from natural immunity is not expected to be a major driver of our conclusions, considering the limited share of population immunity due to natural infection even in scenarios without vaccination (up to 30% at the end of the two years) and to the fact that vaccination is administered independently of a previous COVID-19 infection [23]. Similar considerations apply to the possibility that immunity from natural infection wanes over time [24].
Fourth, we assume that vaccines will protect from infection. This seems to be the case for at least some of the licensed vaccines, according to recent studies [25-27]; however, it needs to be further confirmed also for other vaccines under approval and with respect to circulating variants. In the unlikely case that vaccines only avoid symptomatic disease with no reduction on susceptibility nor infectiousness, our simulations suggest dramatically different results, especially in terms of the ability of countries to relax PDRs. Fifth, we did not consider possible changes in viral transmissibility due to seasonality, such as the closure of schools or the larger amount of time spent outdoors during the summer. This may help reduce deaths and expand the margins for reopening during the summer.
Finally, we assumed that vaccination for children under 16 years old will be available before month 11, when the program is scheduled to be extended to school-aged children in the majority of scenarios. Although there are no licensed pediatric vaccines against COVID-19 yet, several manufacturers have already started phase 2/3 trials for children as young as 3 years old [28]. Therefore, the expectation of having an effective vaccine in the second half of the year is not unrealistic.
There are still many uncertainties on characteristics of vaccines and on the evolving epidemiology of SARS-CoV-2. However, we show that vaccination programs under mitigation scenarios may allow a return to normal within one year since their start if a sufficient capacity and coverage is achieved. The epidemiological characteristics of emerging variants, especially with respect to their increased transmissibility and the effectiveness of vaccines, will need to be closely monitored to promptly reassess these conclusions as more evidence will become available.
Data Availability
Data used in the manuscript are publicly available.
Competing interest and funding
M.A. has received research funding from Seqirus. The funding is not related to COVID-19. All other authors declare no competing interest. V.M., G.G., P.Po., F.T., M.M. and S.M. acknowledge funding from EU grant 874850 MOOD (catalogued as MOOD 000). The contents of this publication are the sole responsibility of the authors and don’t necessarily reflect the views of the funders.




{kind=link}
{kind=link}
{kind=link}
{kind=link}