
Abstract
Background Weak muscle strength has been associated with a wide range of adverse health outcomes. Yet, whether individuals with weaker strength are more at risk for hospitalization due to severe COVID-19 is still unclear. The objective of this study was to investigate the independent association between muscle strength and COVID-19 hospitalization.
Methods Data from 3600 adults 50 years of age and older were analyzed using logistic models adjusted for several chronic conditions, body mass index, age, and sex. Hand grip strength was repeatedly measured between 2004 and 2017 using a handheld dynamometer. COVID-19 hospitalization during the lockdown was self-reported in summer 2020 and was used an indicator of COVID-19 severity.
Results Results showed that higher grip strength was associated with a lower risk of COVID-19 hospitalization (adjusted odds ratio [OR] per increase of 1 SD in grip strength = .64, 95% confidence interval [95% CI] = .45–.87, p = .015). Results also showed that age (OR for a 10-year period = 1.70, 95% CI = 1.32–2.20, p < .001) and obesity (OR = 2.01, 95% CI = 1.00– 3.69, p = .025) was associated with higher risk of COVID-19 hospitalization. Sensitivity analyses using different measures of grip strength as well as robustness analyses based on rare-events logistic regression and COVID-19 patients were consistent with the main results.
Conclusion Muscle strength is an independent risk factor for COVID-19 severity in adults 50 years of age and older.
Introduction
As of January 27, 2021, more than 100 million people were diagnosed with the coronavirus disease 2019 (COVID-19) and over 2 million died due to this infection (1). The majority of infected people are asymptomatic (2, 3) or have mild symptoms such as fever, cough, dyspnea, fatigue, or anosmia/dysgeusia (4, 5). However, severe COVID-19 symptoms can also be life-threatening and require to be hospitalized (6). Thus, identifying risk factors for severe COVID-19 is important to inform clinical decisions and public-health strategies.
Several risk factors have already been identified, including older age, male sex, as well as underlying health conditions such as obesity, cardiovascular disease, respiratory disease, kidney disease, diabetes, and cancer (7-9). In addition to these established risk factors for severe COVID-19, the latest studies suggest that physical fitness should also be considered (10-12). For example, maximal exercise capacity was associated the risk of COVID-19 hospitalization (11), slower walkers showed higher risk of severe COVID-19 than brisk walkers (12), and the overall level of fitness was associated with survival in COVID-19 hospitalized patients (13). Whether muscle strength, another dimension of physical fitness, is a risk factor of severe COVID-19 remains unclear.
Muscle strength is an indicator of muscle function, which is essential to health (14, 15), and has shown to be a robust predictor of multiple diseases and all-cause mortality (14, 16-18). Therefore, muscle strength should be considered as a potential risk factor for severe COVID-19 (19). The objective of this study was to investigate the association between muscle strength and COVID-19 severity. We hypothesized that maximal muscle strength would be independently and inversely associated with COVID-19 hospitalization.
Methods
Study overview
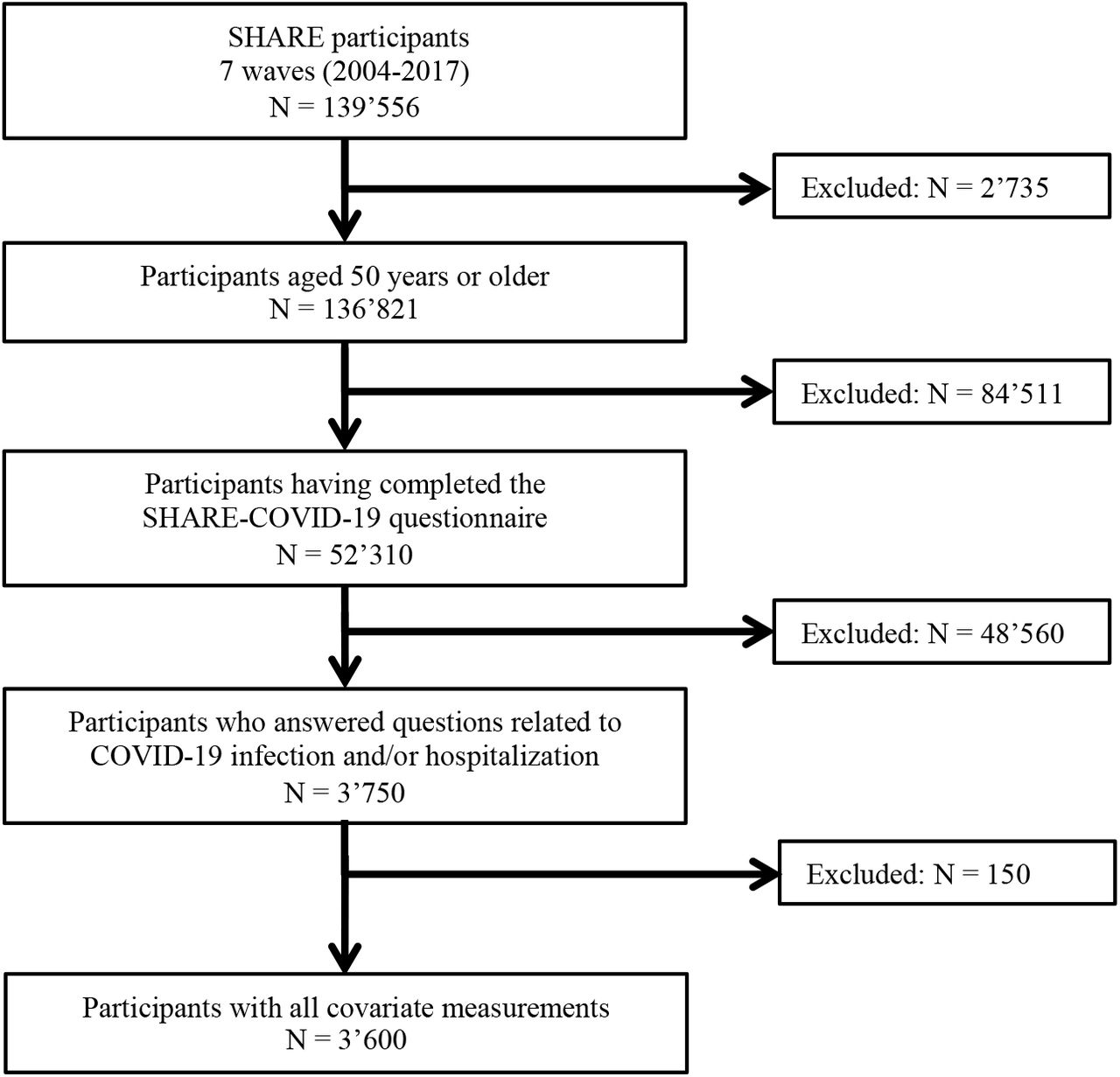
Data from the Survey of Health, Ageing and Retirement in Europe (SHARE) were collected every two years between 2004 and 2017 (7 waves of data collection) on adults 50 years of age and older living in 27 European countries (n = 139556). From June to September 2020, SHARE participants (n = 52310) responded to the SHARE COVID-19 questionnaire (20). Questions included whether they had been tested positive for the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and whether this infection had resulted in hospitalization. To be included in the study, participants should be aged 50 years or older, have completed at least one SHARE questionnaire between 2004 and 2017, and have indicated whether they were infected by the SARS-CoV-2 and/or they were hospitalized due to COVID-19 in the SHARE COVID-19 questionnaire (Figure 1). SHARE was approved by the Ethics Committee of the University of Mannheim (waves 1-4) and the Ethics Council of the Max Plank Society (waves 4-7).
Measures
Outcome: COVID-19 hospitalization
Hospitalization due to COVID-19 was derived from the question: “Have you, or anyone close to you, been hospitalized due to an infection from the coronavirus?”. If participants answered “yes”, the interviewer asked who was hospitalized. Participants who indicated they were hospitalized were included in the analyses as COVID-19 hospitalized. If the participant indicated that their “spouse or partner” was hospitalized, the spouse or partner was included in the analyses as COVID-19 hospitalized.
Independent variable: Muscle strength
Hand grip strength (kg) was used as an indicator of muscle strength and was measured twice with each hand (alternating between hands) using a handheld dynamometer (Smedley, S Dynamometer, TTM, Tokyo, 100 kg). Participants were instructed to stand (preferably) or sit, with the elbow flexed at a 90° angle, the wrist in a neutral position, and the upper arm in a vertical position against the trunk. Interviewers applied standardized instructions to ensure that the grip was performed with maximum effort. The maximum value was used as an indicator of muscle strength (14, 21). Grip strength was assessed at each data-collection wave, but only the most recent measure was included in the analyses.
Covariates and established risk factors
The following covariates were included in the analysis: Age (in 2020, when responding to the SHARE COVID-19 questionnaire), sex (male, female), height (cm), body mass index (normal: <25, overweight: ≥25 and <30, obese: ≥30 kg/m2), cardiovascular disease (heart attack, including myocardial infarction or coronary thrombosis, or any other cardiovascular problem including congestive heart failure, high blood cholesterol, high blood pressure or hypertension, stroke or cerebral vascular disease), respiratory disease (includes chronic bronchitis or emphysema, and asthma), diabetes, cancer, chronic kidney disease, and rheumatoid arthritis. All these covariates are established risk factors for severe COVID-19 (7-9) and were measured using self-reported questionnaires. When a participant had repeated measurements on a variable, the most recent measure was included in the analyses. As recommended (17, 22, 23), self-reported height (cm) was included in the analyses to ensure that the associations observed between muscle strength and COVID-19 hospitalization was not due to a difference in height.
Data analyses
Main analyses
Three logistic regression models were fitted. Model 0 tested the association between muscle strength and COVID-19 hospitalization, adjusting only for height. Model 1 tested the association between the established risk factors (i.e., age, sex, height, body mass index, cardiovascular disease, respiratory disease, diabetes, cancer, chronic kidney disease, and rheumatoid arthritis) and COVID-19 hospitalization. Model 2 tested the association between grip strength and COVID-19 hospitalization, while adjusting for the established risk factors. Age was centered on mean age (i.e., 68.8 years) and divided by 10, so that the coefficient yielded effects of an increased odds of COVID-19 hospitalization over a 10-year period (24). Grip strength was standardized so that the coefficient yielded effects associated with an increase of 1 SD. Statistical analyses were conducted in R using the glm package. Statistical assumptions associated with general logistic models were met (i.e., normality of the residuals, multicollinearity, and undue influence). To illustrate the association between grip strength and COVID-19 hospitalization from the estimates obtained in Model 2, we computed the odds ratio of hospitalization in individuals with weaker and stronger grip strength by centering grip strength on mean – 1 standard deviation (SD) and mean + 1SD, respectively.
Sensitivity analyses
Two sensitivity analyses were conducted. In the first sensitivity analysis, average grip strength over the study duration (i.e., from wave 1 to 7) replaced the most recent measure to test the association with a more stable level of muscle strength. The second sensitivity analysis included grip strength assessed only in the wave preceding the SHARE COVID-19” questionnaire” (i.e., wave 7) (N = 2884) to shorten the time between the measure of grip strength and the COVID-19 hospitalization event.
Robustness analyses
Tow robustness analyses were conducted. In the first robustness analysis, the dataset was analyzed using a rare-events logistic regression (25), which corrects for the bias associated with rare events. To account for the estimated fraction of patients hospitalized due to COVID-19 in the European population from June to September 2020, we used a tau parameter of 84/100000 based on COVID-19 hospitalization data that were available from May 2020 on (Table S3). These data are thought to underestimate the true number of COVID-19 hospitalization as the ones earlier than May 2020 were not included, thereby likely overcorrecting the results of the analysis. In addition, we corrected for our case-control sampling design using the weighting method (R Zelig package) (26). The second robustness analysis included only patients who were tested positive to the COVID-19 (N = 289) to examine whether muscle strength is a risk factor in the population of COVID-19 patients. This subsample was based on the question: “Have you, or anyone close to you, been tested for the coronavirus and the result was positive, meaning that the person had the COVID disease?”.
Results
The study sample included 3600 individuals (68.8 α 8.8 years, 2044 females), from which 83 (2.3 %) were hospitalized due to COVID-19 (Figure 1). Table 1 summarizes the characteristics of the participants stratified by COVID-19 hospitalization status. COVID-19 hospitalization (vs. no hospitalization) was associated with older age (p < .001), higher body mass index (p = .062), cardiovascular disease (p = .064), chronic kidney disease (p = .052), and weaker muscle strength (p = .027). The number of participants who completed their last measure of grip strength in wave 1, 2, 3, 4, 6, and 7 was 10, 7, 3, 39, 188, 413, and 2940, respectively.
P-values are based on the analysis of variance and chi-square tests for continuous and categorical variables, respectively, testing the association between hospitalization (vs. non-hospitalization) and these variables. SD = standard deviation,*p-value is based on muscle strength accounting for height.
Univariate model
Model 0 showed that the most recent measure of maximal grip strength was associated with COVID-19 hospitalization (OR = .60, 95% CI = .45–.81, p < .001, per increase of 1 SD in grip strength) (Table 2).
Age was centered on mean age (i.e., 68.8 years) and divided by 10, so that the coefficient yielded effects of an increased odds of COVID-19 hospitalization over a 10-year period. Hand grip strength was standardized so that the coefficient yielded effects associated with an increase of 1 standard deviation. OR = Odds Ratio; 95% CI = 95% Confidence Interval.
Established risk factors and COVID-19 hospitalization
Model 1 showed that older individuals were at higher risk of COVID-19 hospitalization than younger individuals (adjusted odds ratio [OR] = 1.70, 95% confidence interval [95% CI] = 1.32–2.20, p < .001). The OR was also higher in obese individuals than in individuals with a normal body mass index (OR = 2.01, 95% CI = 1.0–3.69, p = .025). The other associations were not statistically significant (ps > .089) (Table 2).
Grip strength and COVID-19 hospitalization
Model 2 showed that the most recent measure of maximal grip strength (34.43 ± 11.79 kg; mean ± SD) was associated with the risk of COVID-19 hospitalization (OR = .64, 95% CI = .45–.92, p = .015 per increase of 1 SD in grip strength) (Table 2). Results showed that the odds ratio was higher in individuals with weaker grip strength (mean - 1SD = 22.64 kg, OR = .019, 95% CI = .01–.03, p < .001), compared to individuals with stronger grip strength (mean + 1SD = 46.22 kg, OR = .008, 95% CI = .003–.016, p < .001) (Figure 2). When grip strength was included in the model, the association of age (OR = 1.50, 95% CI = 1.14–1.97, p = .003) and body mass index (OR = 2.11, 95% CI = 1.14–3.88, p = .016) with COVID-19 hospitalization remained significant (Table 2).

{kind=link}
{kind=link}
Odds ratios (OR) were adjusted for age, sex, height, body mass index, cardiovascular disease, respiratory disease, chronic kidney disease, rheumatoid arthritis, diabetes, and cancer (see Model 2). 95% CI = 95% confidence interval.
Sensitivity and robustness analyses
The sensitivity (Tables S1 and S2) and robustness analyses (Tables S4 and S5) yielded similar results as the main analysis. Specifically, results of the sensitivity analyses showed that muscle strength averaged across the 7 waves (OR = .62, 95% CI = .42–.92, p = .017) and muscle strength assessed only in wave 7 (OR = .65, 95% CI = .44–.96, p = .029) were associated with the risk of COVID-19 hospitalization. Results of the robustness analysis based on the rare-events logistic regression showed that the most recent measure of maximal grip strength was associated with the risk of COVID-19 hospitalization (OR = .63, 95% CI = .43–.92, p = .016). Finally, results of the robustness analysis that included only patients who were tested positive to COVID-19 showed that the most recent measure of maximal grip strength was associated with the risk of COVID-19 hospitalization (OR = .56, 95% CI = .33–.94, p = .031).
Discussion
Recent findings suggest that physical fitness should be considered as a risk factor for severe COVID-19 (10-12). Here, muscle strength was assessed using hand grip strength and severe COVID-19 was derived from self-reported COVID-19 hospitalization. Results showed that weaker muscle strength was associated with a higher risk of severe COVID-19, after adjusting for established risk factors for severe COVID-19. Hence, our study lends direct empirical support for the hypothesized relationship between muscle strength and COVID-19 severity.
The association between muscle strength and COVID-19 severity can be explained by the essential role of muscle in health and disease (14). Particularly, skeletal muscle weakness has been shown to affect the motor function, respiratory function and has been linked to poor immune response and metabolic stress when facing acute infection (19, 27-29). Therefore, adults with weaker muscle strength may be more vulnerable to SARS-CoV-2 infection and at higher risk of developing severe forms of COVID-19. This hypothesis is indirectly supported by previous results. For example, some conditions associated with muscle weakness such as age, chronic diseases, and cancer have been identified as risk factors for COVID-19 severity (30-32). Likewise, patients with sarcopenia have been associated with an impaired respiratory function (33), which is the function affected by SARS-CoV-2. Finally, our findings are consistent with recent studies showing that other dimensions of physical fitness are associated with an increased risk of COVID-19 hospitalization (10-13).
Among the strengths of the present study are the large sample size, the longitudinal design, and a measure of hand grip strength based on a well-established procedure. Moreover, the results were consistent across multiple independent variables, different statistical approaches, and two different population samples (i.e., general population and patients tested positive to COVID-19). However, potential limitations should be noted. First, the established risk factors were assessed with self-reported questionnaires, which may have reduced measurement validity. Second, the latest assessment of these factors was in 2017, that is two years before participants’ potential infection to COVID-19. Therefore, participants may have contracted a disease between the assessment of these heath conditions and the COVID-19 pandemic, which may have resulted in a misclassification bias. Third, COVID-19 severity was inferred by COVID-19 hospitalization. However, this measure lacks sensitivity. For example, the questionnaire did not assess the lengths of hospitalization or whether the patients have to be transferred to intensive cate unit, which would have allowed to assess with a finer grained COVID-19 severity. Similarly, our sample did not included participants who were hospitalized during the data collection (except when the information can be extract from the spouse or partners) and participants who died due to COVID-19. These limitations may explain the absence of statistical evidence supporting the effect of established risk factors for COVID-19 hospitalization (34, 35).
Conclusion
This study shows that muscle strength is associated with the risk of severe COVID-19 in adults 50 years of age and older. These findings further highlight muscle strength as an important factor to monitor in COVID-19 patients (19, 36, 37). Finally, hand grip strength could improve the accuracy of composite scores used to predict COVID-19 severity (19, 38, 39).
Data Availability
This SHARE dataset is available at http://www.share-project.org/data-access.html.
Statement of Conflict of Interest and Adherence to Ethical Standards
All authors declare that they have no conflict of interests.
Author Contributions
All the authors designed the study. S.S. cleaned the data. B.C. analyzed the data. B.C., M.P.B. drafted the manuscript. All authors critically appraised the manuscript, worked on its content, and approved its submitted version.
Ethical approval
This study was part of the SHARE study, approved by the relevant research ethics committees in the participating countries
Inform Consent
All participants provided written informed consent.
Funding
B.C. is supported by an Ambizione grant (PZ00P1_180040) from the Swiss National Science Foundation (SNSF).
Data sharing
This SHARE dataset is available at http://www.share-project.org/data-access.html.
Supplemental Material
Sensitivity analyses
Results based on average hand grip strength (2004-2017)
Results based on hand grip strength assessed in wave 7
Robustness analyses
Cumulative proportion of COVID-19 cases
Results based on the rare-events logistic regression with a tau parameter of 84/100,000
Results in COVID-19 patients (N = 289)
Acknowledgements
This paper uses data from SHARE Waves 1, 2, 3 (SHARELIFE), 4, 5,6, 7 and 8 (DOIs: 10..6103/SHARE.w1.600, 10..6103/SHARE.w2.600, 10..6103/SHARE.w3.600, 10..6103/SHARE.w4.600, 10..6103/SHARE.w5.600, 10..6103/SHARE.w6.600,10.6103/SHARE.w7.711,10.6103/SHARE.w8cabeta.001). The SHARE data collection was primarily funded by the European Commission through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812) and FP7 (SHARE-PREP: no.211909, SHARE-LEAP: no.227822, SHARE M4: no.261982). Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C) and from various national funding sources is gratefully acknowledged (see www.share-project.org).
Footnotes
↵† SC and MPB are joint senior authors.
References



