
Abstract
The mechanisms of human birth seasonality have been debated for over 150 years. In particular, the question of whether sexual activity or fertility variations drive birth seasonality has remained open and difficult to test without large-scale data on sexual activity. Analyzing data from half-a-million users worldwide collected from the female health tracking app Clue in combination with birth records, we inferred that birth seasonality is primarily driven by seasonal fertility, yet increased sexual activity around holidays explains minor peaks in the birth curve. Our data came from locations in both the Northern Hemisphere (UK, US, and France) and the Southern Hemisphere (Brazil). We found that fertility peaks between the autumn equinox and winter solstice in the Northern Hemisphere locations and shortly following the winter solstice in the Southern Hemisphere locations.
Main Text
To our knowledge, the earliest identified written report of human birth seasonality was nearly 200 years ago (1). Since then a large body of scientific literature has grown around the topic. A consistent and striking pattern is that Northern Hemisphere countries—where the majority of work on birth seasonality has focused—had much stronger birth seasonality in the pre-industrial and early-industrial era, compared to today (2–4). The modern-day dampening of birth seasonality signals that birth seasonality is likely driven in-part by human connectedness to the natural versus built environment and/or sociological factors. In particular, it has been proposed that birth seasonality is driven by environmental influence on biological factors or behavioral practices that have been culturally modified over time. Biological factors that could impact birth seasonality include changes in fertility, broadly defined here as the ability to produce offspring. Proposed biological factors have included (i) seasonal biological rhythms in human fertility entrained by environmental light intensity/photoperiod and that may act via melatonin (5, 6), (ii) seasonal variation in male fertility driven by temperature effects on sperm (7), (iii) seasonal variation in female fertility driven by the seasonal availability of fat-rich food (8, 9), and (iv) seasonal variation in early pregnancy loss due to environmental hardships such as seasonal malnutrition (10, 11). All of these hypothesized mechanisms would be expected to dampen as societies become less affected by the natural world and seasonal fluctuations in photoperiod, temperature, and food availability.
The primary behavioral factor hypothesized to drive birth seasonality has been seasonal sexual activity. Studies from multiple countries have found correlations between holidays, including fertility festivals, and the timing of peak conception (12, 13). It has been proposed that the dampening of birth seasonality over time could be due to cultural changes that have made sexual activity less seasonally structured. Similarly, increased availability of family planning and the development of birth control may have resulted in births becoming more uniformly distributed throughout the year over the last century (14).
It is well established that birth seasonality varies geographically among countries. As previously mentioned, much of the research on birth seasonality has focused on the Northern Hemisphere. Only a few studies have focused on countries in Africa, Latin America, and Southeast Asia. The most extensive study to date revealed that throughout the 20th Century, births were highly heterogeneous in terms of timing of the birth peak worldwide (3, 4, 15). In the Northern Hemisphere, there is a latitudinal gradient in the timing of the birth peak, with Northern countries having their peak earlier in the year compared to countries closer to the equator (2, 3). In terms of birth amplitude, one study of countries in Sub-Saharan Africa found that modern-day birth seasonality in Guinea, Sierra Leone, Ivory Coast, and Nigeria ranged from 37-55%, relative to the mean; representing a three times higher amplitude than in the US (2, 16). If birth seasonality has a tendency to be higher amplitude in the Southern Hemisphere, which has been suggested by multiple studies (16, 17), this may be due to environmental factors including connectedness to the natural environment, lower exposition to artificial living and working environments and/or our inability to statistically detect strong seasonal patterns in Northern Hemisphere countries where populations typically have fewer births per year.
From a public health perspective, there are three potential implications of birth seasonality. First, birth seasonality has direct implications for maternal and infant health. Second, it has an impact on sexual and reproductive health. Lastly, if birth seasonality is driven by seasonal variation in fertility, then it could inform fertility treatments such as ovulation induction, intrauterine insemination or assisted reproductive technologies (ARTs) such as in vitro fertilization.
The uneven distribution of births throughout the year can influence maternal and infant health. Each country has a gestational peak, birth peak, and nursing peak. Any one of these peaks may coincide with environmental challenges, such as seasonal disease outbreaks, elevated food insecurity, and extreme weather events (e.g., heat waves, cold spells, flooding, etc.). Because of this, birth seasonality can put more pregnant individuals and newborns at risk. In particular, under certain environmental contexts, birth seasonality can further exacerbate maternal mortality, pregnancy loss, and/or preterm births.
Regarding the impact on sexual and reproductive health, depending on the drivers of birth seasonality, health services relating to contraception, miscarriages, abortion, and/or sexually transmitted infections (STI) may be utilized more at particular times of the year. Seasonal changes in sexual activity may increase the need for contraception and family planning services around holiday times, a time when these services may be less available, and people may be traveling away from home. A high fertility season, may, on the other hand, pose an unrecognized time of risk for unwanted pregnancy, which can be a danger for women and girls in many countries.
As for fertility treatments, if birth seasonality is driven by male and/or female seasonal fertility, this may open a window of opportunity for successful procedures, especially for those relying on or altering the endogenous hypothalamic-pituitary-ovarian (HPO) axis in females. Relevant procedures may include ovulation induction, intrauterine insemination, eggs or sperm donation, and in vitro fertilization. These procedures present multiple biological, economic, and psychological challenges. To date, there is conflicting evidence regarding seasonal effects on fertility treatments and ARTs (18–23) critical understanding of seasonal fertility may thus be invaluable for improving success rates and the health and wellbeing of patients.
Taken together, the potential biological and social/environmental determinants of birth seasonality represent three long-standing hypotheses: birth seasonality is driven by (A) social determinants, i.e., seasonal variation in sexual activity, (B) biological determinants, i.e., seasonal variation in fertility, and (C) a combination of social and biological determinants.
Birth Seasonality and Sexual Activity
We tested three hypotheses on birth seasonality by using sexual activity data collected from over 500,000 individuals, representing 180 million days of active tracking data. The data were collected from Clue by BioWink GmbH (24), a women’s health mobile phone app. Data was de-identified, users were informed that their data may be shared for scientific research and they may opt-out while still using the app. We used data from individuals residing in the United States, United Kingdom, France, and Brazil, that represent a geographically and culturally diverse set of countries with a high number of users. We also collated time series of monthly births for each country. Overall, we had six geographic locations for all analyses: U.K., France, Central-West Brazil, Northeast Brazil, California, and the Northeastern U.S. (Fig 1a). Data were combined with mathematical models developed explicitly to test our hypotheses.

(a) Time series of monthly births for each location in the study. Grey lines are the raw data, which are overlaid by births standardized to a 30-day month (in color). Vertical bar on the right axis represents a 5% amplitude for reference. (b) Snapshot of the Clue app smartphone interface. (c) Detrended time series of sexual activity aggregated for all locations and stratified by sex type: total sex, protected, and unprotected sex. Monthly aggregated time-series data are provided in the Supplementary Material (Fig. 5.10).
Data from all six locations demonstrated birth seasonality with variation in amplitude and peak timing from country-to-country (Fig 1a). Time series analysis of the app (Fig 1b) data revealed striking increases in sexual activity on weekends and around holidays for all countries taken together (Fig 1c) and each country uniquely with respect to local holidays (Supp Figs. 5.1-9).
To infer how sexual activity is impacted by holidays, weekends, and season, we fitted a statistical model to our data to measure relative sexual activity. Relative sexual activity output from our statistical model captured variation in sexual activity due to (i) day-of-week, specifically capturing elevated sexual activity on weekends, (ii) month of year, and (iii) specific holidays. Figure 2 depicts the holiday variation in sexual activity. Our analysis revealed that all locations in our study had elevated sexual activity on holidays. Each country also had elevated sexual activity ± 1 to ± 3 days about the holiday, typically. For a few holidays, such as Christmas and Good Friday, we observed decreased sexual activity on the days preceding or following the holiday.
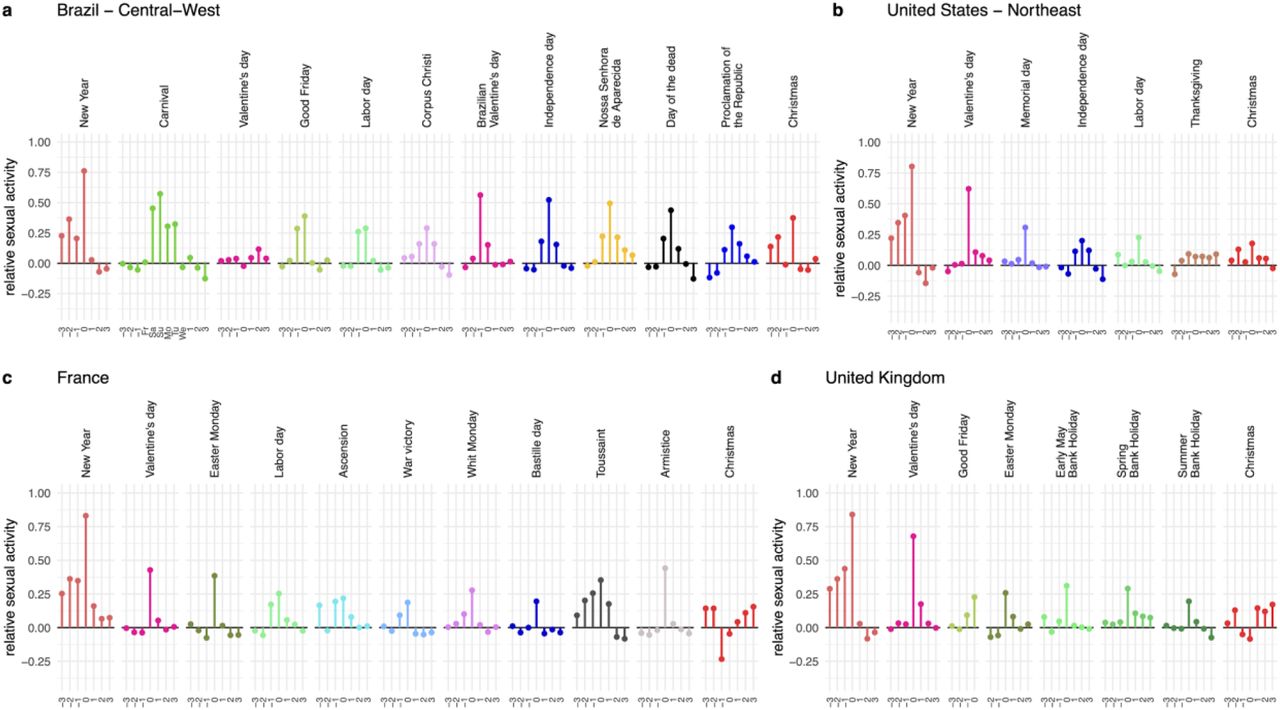
Relative level of sexual activity for each holiday and each country measured proportional to their mean.
For all locations, New Year had the highest magnitude increase in sexual activity. This was comparable to the increase in sexual activity measured in Brazil during Carnival and Valentine’s Day in the US and UK. Brazil was the country in which sexual activity was consistently higher around holidays whereas, France, the US, and UK had much more variation in sexual activity among holidays. One pattern consistent among countries was decreased sexual activity in the three days before Christmas, which was followed by elevated sexual activity on Christmas and the three days after.
The dominant axis of variation in sexual activity was the day-of-week, with all countries having elevated sexual activity on weekends and decreased sexual activity on weekdays, relative to the mean (Supp Fig 5.1-9, 5.14-19). For France, we also observed higher sexual activity in the summer months, July and August, due to increases in weekday sexual activity in these months. A slight increase in weekday sexual activity was also observed in the UK (Supp Fig 5.17), but was not as punctuated as France (Supp Fig 5.16). We ensured the variation in sexual activity measured here was not a statistical artifact of app tracking fidelity arising from individuals tracking more on weekends, holidays, and during the summer. We drew this conclusion based on analysis of variation in other app features including exercise, long sleep (>9 hr sleep duration), breast pain, and menstrual bleeding categorized as medium flow. If the weekend effect were a statistical artifact we would expect all features to be elevated on weekends. We observed, however, that exercise was reduced on weekends, long sleep was reported more often, and there was no weekend effect on breast pain or bleeding (Suppl. Fig 6.1-6.6). We therefore conclude that observed weekend and holidays effects were valid.
Mathematical Model Results
We translated each of the three birth seasonality hypotheses into a deterministic population-level mathematical model of conception and birth (Fig 3a). In each model, daily conceptions were modeled as the product of daily sexual activity and daily fertility. Daily conception was then used to predict daily births (approx. 9 months into the future) using empirical distributions of gestation period for each country (Fig 3b)(25–27). Daily births were aggregated monthly to allow the comparison with official birth records.

(a) Model equations representing conception as a function of sexual activity and fertility. (b) Assumed mean gestation period and distribution for each country in our study. (c) Schematic of model variants.
Model A assumed variation in sexual activity entered as a time-varying variable in the model and constant fertility (Fig 3c). The time-series of daily sexual activity were output from our statistical model fitted to the app data. Model B assumed constant sexual activity and seasonal variation in fertility expressed as a sinusoidal function with a period of 1 year (Fig 3c). Fertility was expressed as a sinusoidal function because this function is a good and low-parameter approximation to model an internal circannual clock or the effects of environmental changes such as daylight duration, temperature or rainfall, which, in all studied locations, have a single peak throughout the year. The phase and amplitude of this function was estimated for each geographical area. Model C assumed variation in sexual activity and seasonal variation in fertility (Fig 3c). Once again, seasonal sexual activity was entered as a time-varying variable. However, in Model C we added a scaling factor for sexual activity that allowed for changes in amplitude. The sexual activity scaling factor, along with the phase and amplitude of seasonal fertility, was estimated for each geographical location for Model C. Lastly, the mean daily conception rate was calculated based on the long-term trend in the birth time series.
Universally, the models that best fit the data were those that included seasonal fertility. Importantly, although the app data confirmed that sexual activity is not uniform throughout the year, models that included seasonal sexual activity as the sole driver of birth seasonality could not capture the shape, timing or amplitude of birth seasonality observed in each country. In fact, seasonal sexual activity alone would generate birth peaks in each country that do not match the peaks observed in the time series of births (Fig 4a-f top panels A).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
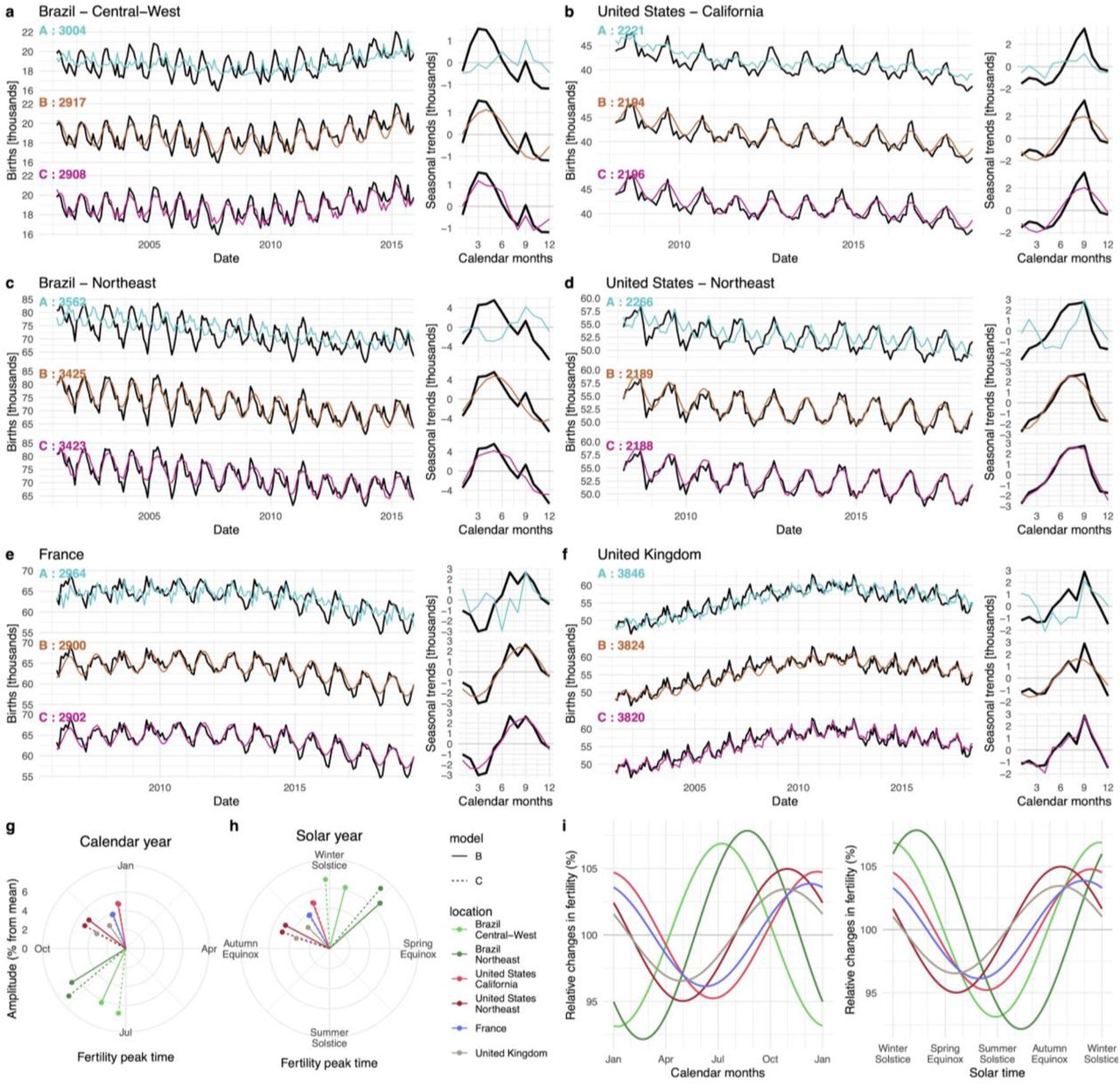
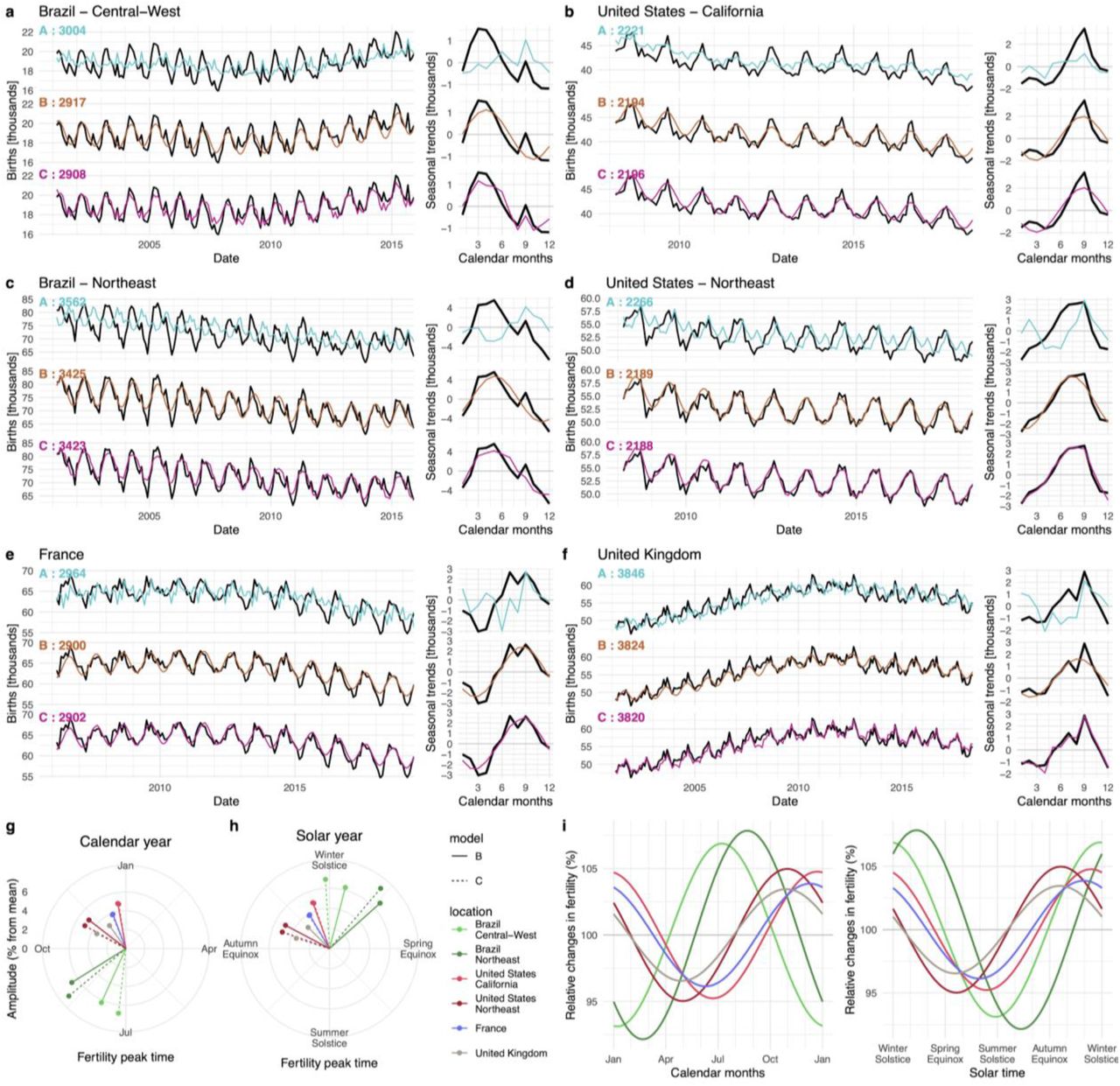
(a-f) Birth data and model simulations for each location, with models A-C shown top-to-bottom. Left panels are the full time series, while right panels show the seasonal decomposition for data and simulations. (g) Timing and amplitude of the fertility peak for each location and Models B and C shown by calendar month. (h) Timing and amplitude of the fertility peak for each location and Models B and C shown by solar year. (i) Estimated seasonal fertility curves by calendar and solar year.
For the UK, US Northeast, and both locations in Brazil, Model C best fit the data according to AIC, suggesting seasonal fertility and holiday sexual activity together shape birth seasonality (Fig 4.). For France and California, Model B best fit the data, suggesting that seasonal fertility is the dominant driver of birth seasonality in these locations and that seasonal sexual activity plays a negligible role (Fig 4 and refer to Supp Table 5.2-5.3 for AIC values and model comparison). In general, birth seasonality had a unique shape in each location. Some locations, like Brazil, had a distinct major peak and a minor peak (i.e., shoulder during the downswing). Other locations had more complex seasonal shapes. France and the UK had similar high frequency oscillations, with the major peak centered in the summer and punctuated by increases in Jan/Feb, July, and September. Seasonal births had the simplest shape in the US, and were distinct for each location. California birth seasonality had a strikingly narrow peak, triangular in shape; while, the Northeastern US had a shallower upswing and a plateau at top, followed by a sharp decrease. Despite these location differences, these patterns are very consistent from year to year for a given location (Suppl. Fig. 5.41-5.46).
As previously mentioned, Model C best fits the data in Brazil, the UK, and US Northeast. In Brazil, the inclusion of seasonal/holiday sexual activity allowed Model C to capture the distinct shape of the major and minor peaks. The major peak in Brazil is driven by seasonal fertility, while the minor peak is driven by sexual activity surrounding the New Year holiday (Fig 4a & c, bottom panels). In the UK, seasonal fertility explains the overall seasonal pattern of births; but the spike in September is driven by the New Year holiday. Therefore, Model C was also a good fit to the UK data. In the US Northeast, sexual activity allowed Model C to capture the non-sinusoidal peak and sharp decline in births after September. In France and California, however, Model C was penalized by the addition of seasonal sexual activity, because holiday sexual activity does not seem to result in elevated birth rates in these countries. Model results were robust to the type of sex. Model fits varied little by sex type (i.e., total sex, protected sex, and unprotected). All model combinations are reported in the Supplementary Materials.
Seasonal fertility was ubiquitous in our best fit models but because we were studying locations in the Northern and Southern Hemisphere, it was important to characterize seasonal fertility relative to the respective seasons in each country as opposed to the calendar time. All locations had their fertility peak between Autumn Equinox and Spring Equinox, centered about the winter solstice. Specifically, Brazil had a fertility peak in Aug-Sept, directly following winter solstice. The Northern Hemisphere locations had their fertility peaks from Oct-Dec, directly preceding the winter solstice (Fig 4g-i).
As for amplitude, the locations fell into three general categories of low, intermediate, and high amplitude seasonal fertility. The UK and France had the lowest amplitude seasonal fertility (half peak-trough difference < 4%). California and the Northeastern US had intermediate amplitude (< 6%) and Brazil had the highest amplitude (∼8%). Although these are relatively low-amplitude fluctuations, compared to birth seasonality observed in some parts of the world, seasonal fertility is operating at a population-scale resulting in substantial differences in the number of births. In the lowest amplitude countries, UK and France, seasonal fertility results in roughly 3000-4000 more births in peak versus trough months (Fig. 4). Despite all six locations being located at different latitudes, with different climate and seasons (i.e., temperate seasons at high latitude vs. rainy/dry seasons near the equator), it was remarkable that seasonal fertility peaked within a 3-4 month band centered about the winter solstice.
Discussion
Our study allowed us to confirm that seasonal fertility is the main driver of birth seasonality in industrial and post-industrial societies, which has been disputed for at least 150 years. We explicitly tested whether the seasonality of sexual activity is responsible for human birth seasonality. Our models found, universally, that seasonal sexual activity alone cannot explain birth seasonality. Births simulated from sexual activity alone did not match with those observed, in terms of peak timing, amplitude or seasonal shape. Consequently, models of birth seasonality required an additional seasonal driver to capture the data. Our models of explicit seasonal fertility from all four countries in this study best fit the data. Although there were differences in the best fit model (i.e., Model C vs. Model B) from country to country, we are confident that seasonal reproductive biology exists in humans. We were able to unmask this seasonal phenomenon due to the strength and size of our data and the simplicity of our models and assumptions.
Most past studies that have presented evidence of specific mechanisms of birth seasonality focused on rural and/or nomadic populations in which living conditions drastically changed seasonally. For example, extreme seasonal changes in birth rates in a nomadic Kenyan tribe were explained by variation in the seasonal availability of fat-rich food and in womens’ physical labor (28). In the Lese women of Central Africa, months of low food availability were correlated with reduced salivary progesterone, which may be associated with lower rates of implantation and/or ovulation (29, 30). Bolivian women living in high-altitude rural areas,subject to large seasonal variations in workload, have exhibited decreased salivary progesterone and elevated early pregnancy loss in the months of intensive physical labor (10). These mechanisms, however important for fertility and successful pregnancy in rural and nomadic populations, are not able to explain birth seasonality in industrial or post-industrial societies in which fat-rich food is available throughout the year, seasonal migration is limited, and physical work is likely stable throughout the year. While our data and models did not afford us the opportunity to determine the mechanisms by which seasonal fertility operates in industrial countries, specifically if it is is operating via male and/or female biology our study did allow us to confirm that seasonal fertility exists in the absence of high-amplitude seasonal stressors such as reduced food availability or increased physical workload.
There are various reproductive mechanisms that could be driving seasonal fertility, including fertility at conception and/or induced or spontaneous pregnancy loss. We show here that seasonal reproductive biology is the dominant underlying driver of birth seasonality and acts in combination with seasonal sexual activity to give the nuanced population-specific shape of birth curves. Our results raise the question of whether the external seasonal environment directly alters fertility or acts as a synchronizing factor to entrain an endogenous biological clock. Specifically, such endogenous circannual clocks, that remain rhythmic under constant conditions, have been known to exist in other mammals and contribute to seasonal physiology including reproduction, hibernation, molting, and migration (31–33).
Our study indicates humans are short-day breeders, with peak fertility being centered about the winter solstice in both hemispheres. Initiating pregnancy during short winter days is in keeping with observations from other mammals (e.g., sheep and deer) with long gestation periods, because gestation during the harsh winter months allows for births to be aligned with optimal food conditions and favorable environmental conditions in spring, summer, and early autumn. Seasonal fecundability peaking in fall/winter has also been observed in a recent cohort study in the Northern Hemisphere (34) and increased endometrial receptivity at the same period of the year was suggested in an earlier study (23).
Since seasonal fertility peaks around winter solstice, in the Northern Hemisphere it coincides with the dominant holiday season of New Year/Christmas when sexual activity is elevated. By contrast, in Brazil, in the Southern Hemisphere, the New Year/Christmas holiday is out-of-phase with the seasonal fertility peak. Inclusion of data from both the Northern and Southern Hemisphere is a key strength of our study. Cultural holidays have emerged within the context of the seasonal environment. Therefore, including countries with differing seasonal cycles (e.g., temperature seasons vs. tropical rainy/dry seasons) allows us to reveal seasonal features of human biology that may otherwise be hidden by cultural phenomena.
To our knowledge this is the most in-depth study of sexual activity by way of depth, time scale, geographical coverage and sample size (over 500,000 app users). We found that sexual activity is strongly structured around holidays, weekends, and, in some locations, summer months. As expected, elevated sexual activity was generally associated with leisure time and/or time off work/school. From this we infer that seasonal sexual activity arises from available time with sexual partners. The fact that there is more sex on weekends shows that having time off is conducive for sexual activity. In addition, romantic celebrations, such as Valentine’s Day and Dia dos Namorados (i.e., Brazilian Valentine’s Day) expectedly have increased sexual activity. This is in agreement with studies of sexual and reproductive health reporting an increase in sexual activity occurring around Christmas and other holidays and events (12, 13).
One limitation of our sexual activity data is that it originates from a self-selected, potentially biased population of app users that are typically young females. Data presented herein are aggregated over all age groups, all birth control types, and for unprotected sex, but our conclusions are robust to stratification by age and birth control use/type (see Supplementary Materials). Our users consisted of individuals born between 1965-2004. While the demographics of menstrual app users may differ from those of the general population, smartphone ownership is likely a negligible source of bias in our data. Smartphone ownership rates among reproductive-age individuals are high in all locations studied, ranging from 85% in Brazil to 97% in France (39). Thus, our sample may offer a good approximation of sexual activity. One limitation was that our data only covered two years. Thus, we could not fully quantify interactions between day-of-week and individual holidays; however, we were able to account for shifting holiday dates, such as Easter and Carnival, which differ by several weeks each year (Supplementary Fig 5.49). An interesting extension of this work would be to also include countries with different national holidays outside of the Judeo-Christian calendar. Within the countries we studied, one could also explore the effect of holidays that are not on the national calendar, such as Jewish, Muslim and Hindu holidays, that are celebrated by an increasing proportion of the population.
Globally, there are some countries with higher amplitude birth seasonality than those included in our study, such as in Sub-Saharan Africa. It is important to understand how seasonal fertility and seasonal sexual activity operate in countries with stronger seasonal rhythms. When in-phase, seasonal fertility and sexual activity could drive strong pulses via a multiplicative effect. This could occur, for instance, in seasonally migrant agricultural communities where household composition and behavioral activities are strongly tied to the seasonal environment, allowing for an alignment between physiology (fertility), social activities (including sex), and favorable environmental conditions.
Our results show that although humans have the capacity to reproduce year-round, there is seasonal structuring to our reproductive physiology. Early findings of increased estradiol in the winter (35) have recently been confirmed by a large-scale study (36) that revealed a winter-spring peak in estradiol and testosterone and a summertime peak in luteinizing hormone (LH) and prolactin (36). In addition to seasonal variations in reproductive hormones, humans have seasonal cycles in hormones involved in thermoregulation, metabolism, stress adaptation and growth (36), as well as seasonal changes in the immune system (37, 38). Overall, seasonal changes within individuals are important at a population-level because they are capable of manifesting as population-level phenomena, such as birth seasonality. Seasonal fertility, in particular, has clinical and public health implications. Times of elevated fertility may open a window of opportunity for reproduction and working with your seasonal body clock for planning pregnancy. By contrast, the high fertility season is a high risk period for individuals desiring or needing to avoid pregnancy. The public health community must recognize these risks and opportunities to improve sexual and reproductive health interventions.
Data Availability
Birth data, aggregated time series and model parameters are available on https://github.com/lasy/Seasonality-Public-Repo.
Authors contributions
L.S., M.M. contributed to the conceptualization and methodology. L.S., A.S., C.R.M., D.S. and M.M. contributed to the data acquisition and curation. L.S. contributed to the software and visualizations. L.S., M.M., P.S., D.S., C.R.M and S.H. contributed to the writing of the manuscript.
Competing interests
A.S. is an employee of Clue by BioWink GmbH, whose app data were used in this study.
Data and materials availability
code, birth data, aggregated time series and models are available on https://github.com/lasy/Seasonality-Public-Repo.
Acknowledgements
The authors thank V. Teixeira and J. Calixto for helping extract the Brazilian birth data from DATASUS and Dr. Vitzthum for helpful feedback on the manuscript.
References



