
Abstract
Introduction Polycystic ovary syndrome (PCOS) is a common disorder that is not fully understood. Multiple hormonal and metabolic factors impact on disease pathophysiology resulting in various phenotypic characteristics among the PCOS population. Luteinizing hormone beta subunit (LHβ) (protein ID P01229) is mapped on (chr19p13.3) and consists of three exons. It is specific beta (β) subunit giving luteinizing hormone (LH) from the anterior pituitary its specific function. LH has a central role in stimulation ovarian steroidogenesis, in particular androgen production, and the promotion of ovulation.
Objectives To determine genetic mutations associated with PCOS among Sudanese families.
Methods A prospective laboratory based cross-sectional study to examine genetic mutations in LHB that associate with PCOS in families (cases; n=35 families, 90 females and controls; n=11 families, 30 females) in Khartoum State, Sudan. Quantitative Enzyme Linked Immuno-Sorbent Assay (ELISA), enzymatic methods and polymerase chain reaction (PCR) used to analyze both the biochemical parameters and polymorphism detection followed by Sanger sequencing for genotyping in addition to bioinformatics software for protein structure and function.
Results The PCOS caseshad significantly different biochemicalparameters from the controls (LH: p<0.001; testosterone: p<0.001; fasting glucose: p=0.02; insulin: p=0.01; triglycerides: p=0.03; total cholesterol: p<0.001; high density lipoprotein (HDL): p=0.012; low density lipoprotein (LDL): p<0.001). There were no differences in follicle stimulating hormone (FSH) (p=0.984) or prolactin (p=0.068). Sanger sequencing revealed 5 single nucleotide polymorphisms (rs5030775, A18T; rs746167425, R22K; rs1800447, W28R; rs35270001, H30R; and rs34349826, I35T) located on (exon 2) of LHB gene that were statistically correlated with serum LH, Testosterone and insulin levels among PCOS families.
Conclusion This is the first molecular family-based study in Sudan exploring the genetics of the LHβ gene in women manifesting PCOS. These novel mutations give further information about the genetic inheritance and may explain some of the altered ovarian function and responses in women with PCOS.
Introduction
Polycystic ovary syndrome (PCOS) is a disorder which is associated with a hormone imbalance, anovulation andmultiple paused follicles in the ovaries and linked to different metabolic disorders.1,2 It has a complex etiology with genetic, epigenetic and environmental factors. Adherence to the three common diagnostic criteria of increased androgens, polycystic ovaries on ultrasound scan and anovulation (1990 National Institutes of Health’s (NIH), the Rotterdam criteria and the Androgen Excess Society) that cover the different phenotypic features of PCOS suggests a prevalence of1.6-18% among women within the reproductive age.2-4
Binding of GnRH to its G-protein coupled receptor on the pituitary gonadotropic cells actives the guanine nucleotide-binding protein subunit α (Gαq/11) protein that stimulates phospholipase Cb, with subsequent activation of inositol trisphosphate (IP3) and diacylglycerol (DAG) that mobilize intracellular calcium from the endoplasmic reticulum. This causes expression of the LH and follicle stimulating hormone (FSH) subunits which are required for the formation of both LH and FSH. LH stimulates androgen synthesis in theca cells to drive steroidogenesis and ultimately androgen production. Excessive theca cell androgen secretion can lead to variety of hormonal and metabolic abnormalities such as hirsutism, anovulation, hyperinsulinemia, insulin resistance (IR), and obesity which are more common amongst women with PCOS population.8
There are epigenetic factors that can promote PCOS. In various animal models, and in women, increased exposure of the developing fetus to increased androgen concentrations before birth can result in developmental programming of the features of PCOS. Prenatal androgens result in dynamic changes in gene expression, resulting hyperinsulinemia, adipocyte dysfunction, visceral obesity, and PCOS in offspring.9, 10
There are environmental factors involved in PCOS. An increase of weight can unmask a PCOS phenotype in adulthood. However there are genetic elements of PCOS, although the genes involved remain poorly characterized. Various familial aggregation studies suggest that PCOS is an autosomal dominant syndrome and there is an association in both sisters and brothers of women with PCOS with infertility problems. In addition monozygotic and dizygotic twin studies suggest a genetic contribution to PCOS. Recent genome-wide association studies (GWAS) in Han Chinese women with PCOS identified 11 genetic loci that related to PCOS. These loci were in genes involved in steroidogenesis, steroid hormone action, gonadotrophin action, regulation of internal secretion, energy balance,chronic inflammation, and other pathways relevant to PCOS.11-16
PCOS as neuroendocrine disorder resulting on exaggerated LH pulse frequency and amplitude associated with defect of androgen synthesis that results in enhanced ovarian androgen production and finally alteration in cortisol metabolism resulting in enhanced adrenal androgen production 17-19. Moreover, excessive theca cell androgen secretion results on many types of hormonal and metabolic abnormalities which are characterized by hirsutism, anovulation, clinical and/or biochemical hyperandrogenism, hyperinsulinemia, insulin resistance (IR), and obesity are more common syndromes beside the polycystic ovarian morphology on ultrasound 1-3. Therefore, assessment of hormonal profile among PCOS population using high-quality techniques such as liquid chromatography tandem mass spectrometry (LC-MS/MS), plays a key diagnostic marker of PCOS.
As androgens are driven by LH, we focused on theLHB gene. We aimed to examine the relationship between single nucleotide polymorphisms (SNPs) of the LHB gene with the clinical features of PCOS among Sudanese women within the reproductive age.
Methodology
This study was approved by the national ethics committee - Federal Ministry of Health (3-12-19). The inclusion criteria for PCOS families werewomen diagnosed with PCOS, according to the Rotterdam criteria that had one or two sisters diagnosed as PCOS within the reproductive age (20-40) years. In control families neither the woman nor any sisters had any features of PCOS. Any women below the reproductive age or with family history of adrenal hyperplasia, hyperprolactinemia, Cushing syndrome, thyroid disorders, ovarian cancer or breast cancer and causes of infertility rather than PCOS were excluded from the study.
This prospective laboratory based cross-sectional study involved blood sampling carried out in different fertility centers as well as different localities (families’ homes) in Khartoum State. Hormonal profile estimations were carried out using validated tests within the clinical service laboratory with quantitative enzyme linked immunosorbent assay (ELISA) and enzymatic methods for measurement of fasting blood glucose and lipid profile. DNA extraction from whole blood was carried out using a commercial kit according to manufacturer’s instructions. Primer 3 was used to design the LHB primers (Table 1).Routine polymerase chain reaction (PCR) and gel electrophoresis was used for band amplification and visualization. The Sanger dioxnucleotidue sequencing methodwas used for genotyping and the bioinformatics software (BLAST, USCF Chimera, Project Hope and Raptor X) was used for protein structure, function and prediction.
The LHB gene primers for PCR protocol.
Descriptive and biological information about study groups were analyzed by SPSS version 23 using descriptive analysis for age, BMI, and biochemical analysis. In addition to t-testswere used for statistical significance after testing for normality. Chi square test and Person correlation were used for statistical association and the significance was p<0.05.
Results
The patient characteristics and biochemical parameters are shown in (Table 2). There was no difference in age and BMI, serum levels of FSH and PRL assessment between the groups. However, there were clear increases in LH and testosterone concentrations (p<0.001) in the PCOS group. This meant that the LH: FSH ratio was significantly elevated in women with PCOS (P<0.001). In addition, there was evidence of insulin resistance and dyslipidaemia in the women with PCOS (Table 2). The BMI was increased in women with PCOS. This highlights the validity of the cohort of PCOS patients when compared to controls.
There was no effect of obesity on PCOS phenotypes and it did not interfere with their menstrual regularity (Table 3). While PCOS cases suffered from signs of hyperandrogenism hirsutism (42.9%), Acne (54.5%) and Seborrhea (30%) exposedirregular menstrual cycle which is statistically significant (p-value= 0.011) (Table 4).
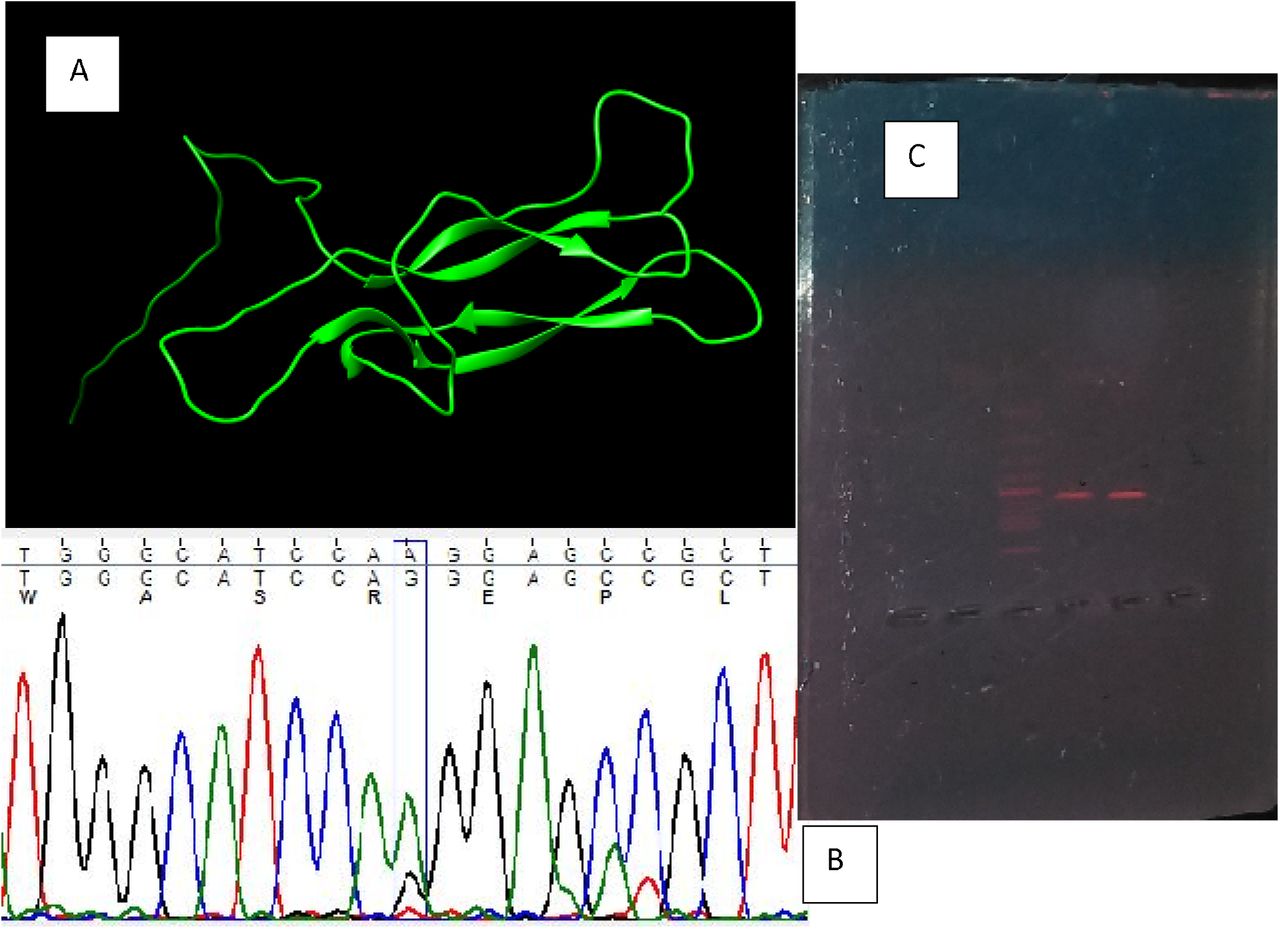
DNA was extracted and sequenced from the cases and the chemical structure of the LH protein determined (figure 3). Within the PCOS families there were five SNPs that were identified within exon (2) of LHβ which is statistically significant with serum levels of LH, testosterone and menstrual irregularity.(Table 5 &6).

The frequencies of presence of Acne, hirsutism, and status of MC between study groups; (54, 5) but 57.1% of them had no facial hirsutism similar to 77% of control group.84.6% of our control had regular menstrual cycle and only 15.3 had irregular menstrual cycle, while the case group had the higher distribution than control group.
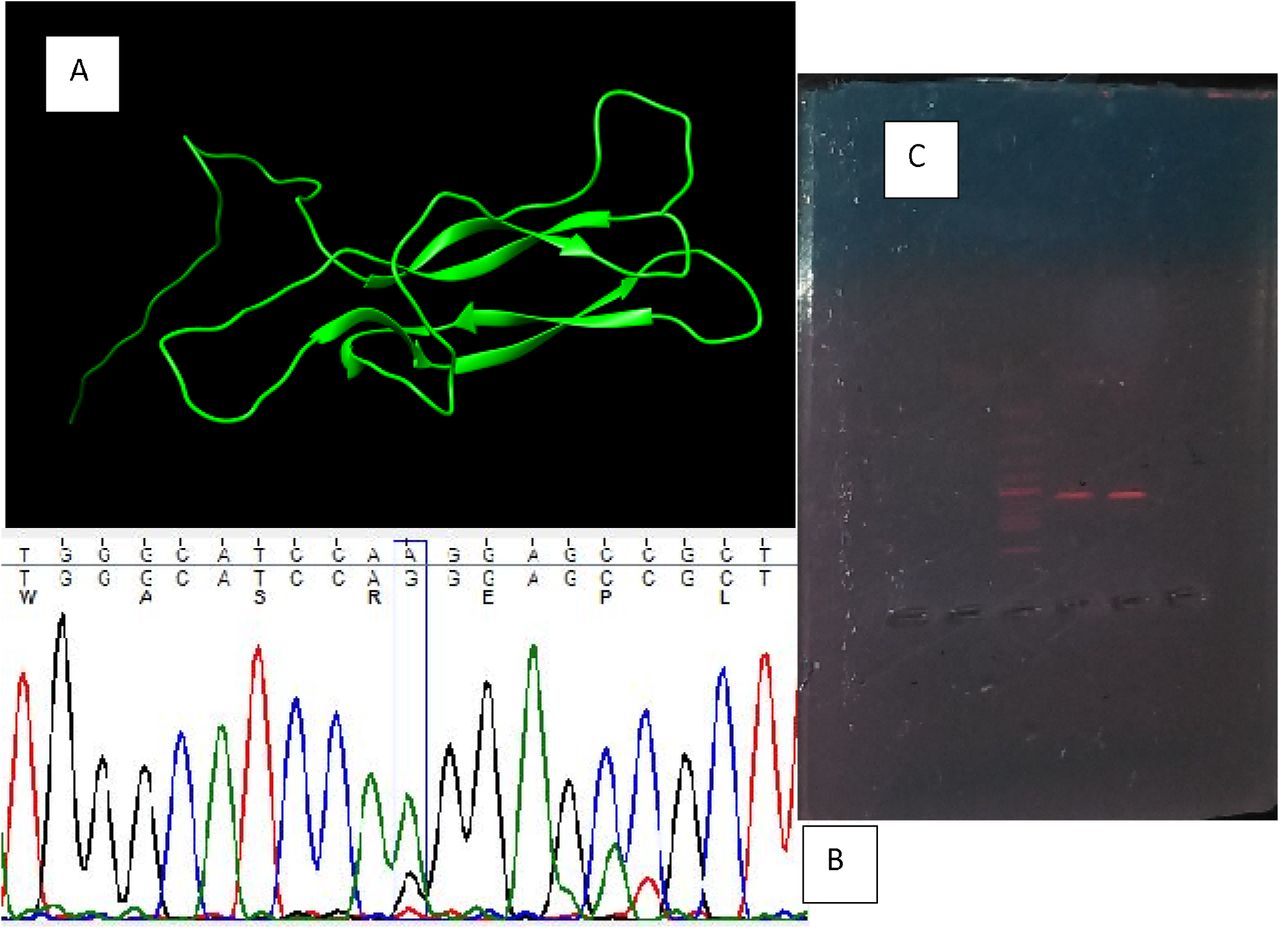
(A)The normal chemical structure of LH protein, (B) The chromatogram graph for the sequenced protein, (C) The gel electrophoresis showing the PCR product band (571bp).
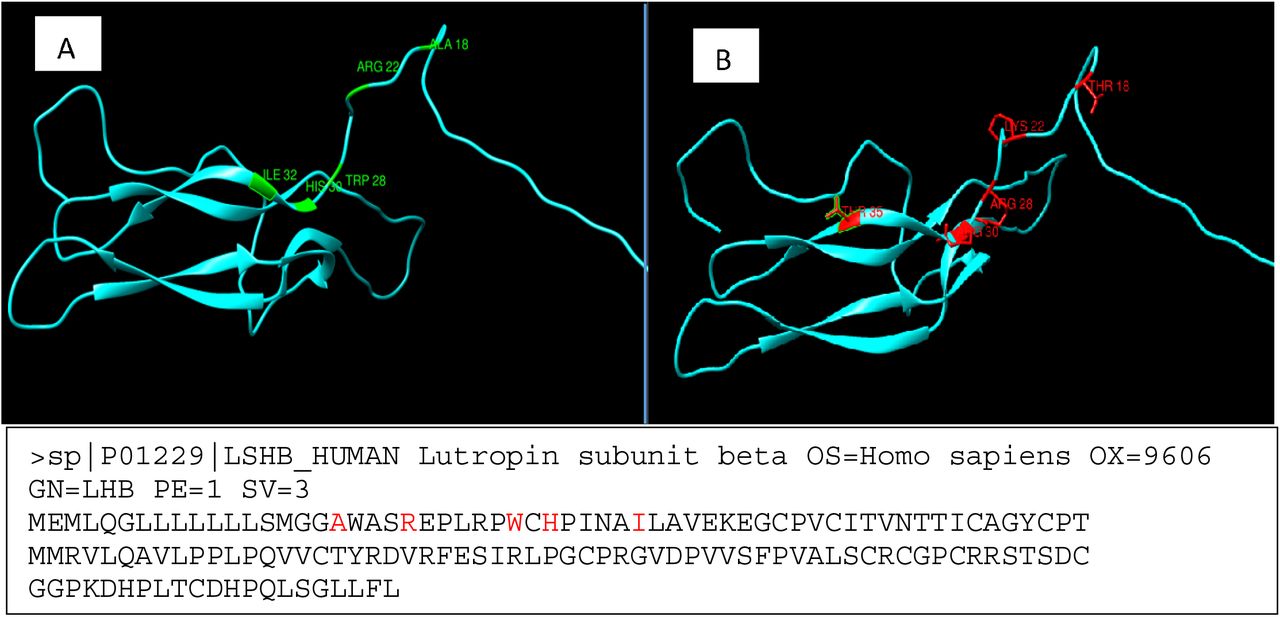
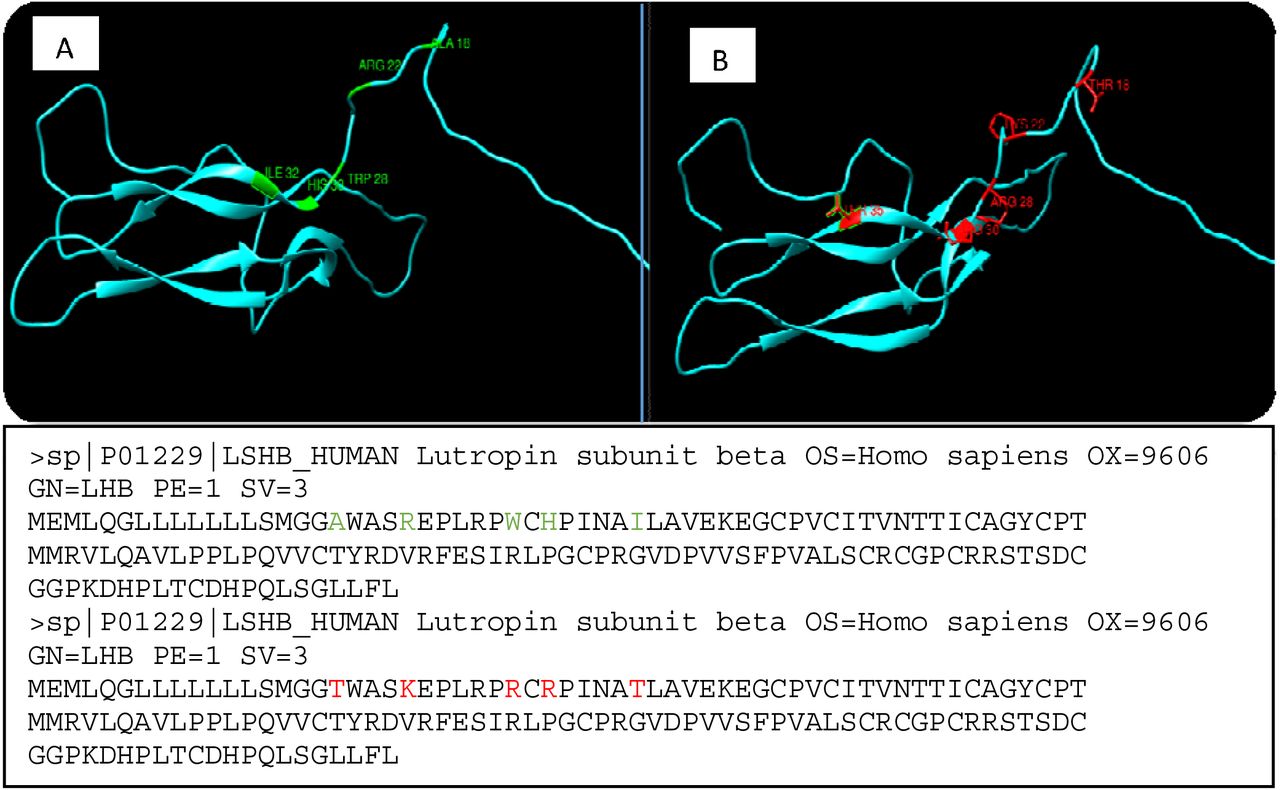
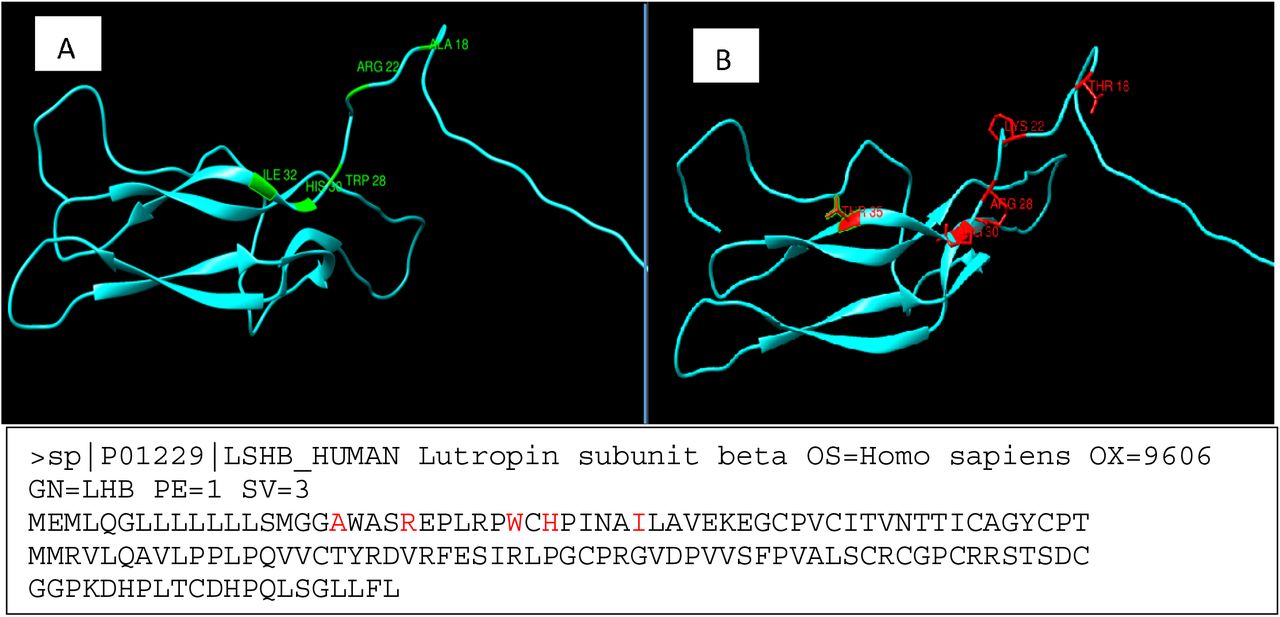
illustrated both normal and mutated amino acids on sequenced exon (2) LHβ Gene
Characteristics of PCOS and controls cohorts
the effect of obesity on menstrual cycle
The association between hormonal profile and menstrual cycle status among study groups.
The association between clinical hyperandrogenism and menstrual cycle status among study groups.
The association of hormonal profile and recurrent miscarriage among PCOS group
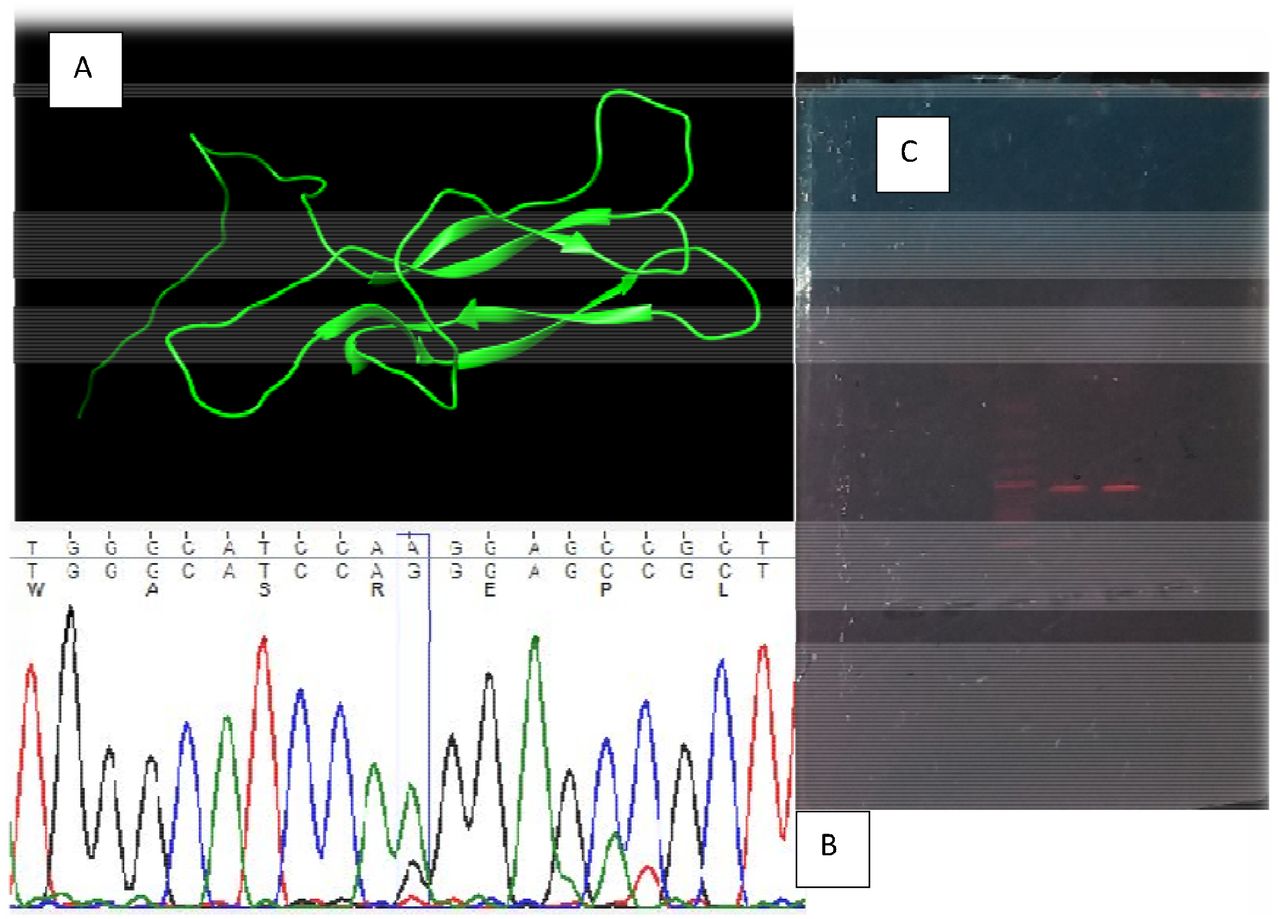
(A)The normal chemical structure of LH protein, (B) The chromatogram graph for the sequenced protein, and (C) The gel electrophoresis showing the LH band.
DNA was extracted and sequenced from the cases and the chemical structure of the LH protein determined. Within the PCOS families there were five SNPs that were identified within LHβ.
and figure (3.2): Distribution of LHβ genotypes and allele frequencies in healthy controls and patients with PCOS
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
normal (A) and mutated amino acids (red color) on sequenced exon (2) LHβ gene (B).
The association of LHβ polymorphisms and menstrual irregularity among study groups
The association of LHβ polymorphisms and hormonal profile among study groups
The association of LHβ polymorphisms and recurrent miscarriage among study groups
4. Discussion
In this study we investigated if different biochemical parameters were associated with polymorphisms of the LHB gene among Sudanese families who had more than one PCOS sufferer and compared this to control families without women with PCOS. The biochemical parameters within the PCOS group were consistent with PCOS and showed that they were different to the control group. We identified five polymorphisms in the LHB gene in the families with PCOS in Sudan.
In this study the biochemical parameters were within the normal ranges but significantly different from the control group of the study, except BMI, serum levels of FSH and PRL. Findings of this study revealed that PCOS women suffered from menstrual irregularity (46.8%), signs of clinical hyperandrogenism; facial hirsutism (42.9), Acne (54.5%), Seborrhea (33.3%) and Alopecia (35.6%) (Esmaeilzadeh et al., 2014) 51 and (Patel, 2018)52in compare to controls with consensus to the international hallmarks of PCOS of hormonal imbalance (Act, 2018),(Azziz, 2016) and (EscobarMorreale, 2018), menstrual irregularity (Harris et al., 2017) and dyslipidemia (Esmaeilzadeh et al., 2015)(Shoaib et al., 2015)48, (Bennal et al., 2014) 49. In contrast to (Sadeghi et al., 2014)50 showed that there is no association between serum lipid profile, total cholesterol level, LDL cholesterol and HDL cholesterol (p-value =0.86, 021, 0.76 respectively) and PCOS except in the term of TG (p-value =0.0.4) in PCOS women with BMI > 25 due to small sample size and less biochemical parameters. While only obese PCOS women showed significant difference on serum TC as well as LDL-C (p=0.000) when compared with overweight/normal PCOS indicating that obese women were more susceptible to dyslipidemia and cardiovascular disease similar to Castelo-Branco et al., and (Spalkowska et al., 2018).
With regard to these findings, PCOS women were more predisposing to T2DM on their future life similar to (Forslund et al., 2020) and (Rashidi, 2018) among different BMI groups. Nevertheless, There is no effect of obesity on hormonal profile among PCOS population but there is an adverse effects of obesity on serum testosterone level which is an inverse correlation among PCOS women with BMI ≥ 30 (p=0.014) while lean PCOS women had positive correlation (p=0.009) similar to (Spalkowska et al., 2018) and (Saxena et al.., 2013). Hyperandrogenemia is responsible for accumulationof the adipose tissue in the upper body (android fat distribution pattern). In contrast to Good et al., Aydin et al., concluded that no differences in body composition between lean women with PCOS and healthy controls.
We report that sisters of affected women have irregular menstrual cycles and this agrees with the Turkish study that showed that sisters were having menstrual irregularity and larger ovaries with higher serum androstenedione and dehydroepiandrosterone sulfate levels than sisters without PCO, suggesting a spectrum of clinical phenotypes in PCO families. This parallels what was reported in a multicenter study with (1466) subjects, of whom (363) had PCOS and (79) polycystic ovaries (PCO) without other symptoms of PCOS.Here the LHB polymorphism (rs1800447 (W28R) and rs34349826 (I35T) homozygotes (CC) had an association with recurrent spontaneous abortions, menstrual irregularities with infertility, and elevation of serum testosterone level (Furui et al., 1994), whereas the Finnish subjects whom were homo- or heterozygous for the polymorphic LHB allele were largely healthy. In contrast, the first report of this mutation among the male population was a patient with hypogonadotropic hypogonadism provided clinical and experimental evidence that this novel mutation causes selective LH deficiency.Other studies showed significantly higher serum LH concentrations in V-LH carriers among the young Baltic men and Estonian male infertility patients.
Herein we described the presence of 5 single nucleotide polymorphisms of LHB gene, that shared between the investigated cases were with homozygous (AA) inheritance mode. They are located on the signal peptide and the homologue glycoprotein parts and thus could have significant influence on serum level of the hormone without inactivating or damaging its biological function. The most reported mutations of this research findings were (rs1800447 (W28R) and rs34349826 (I35T)) which are associated with protein glycosylation and have been linked to response to controlled ovarian stimulation, male infertility and PCOS.In particular, protein glycosylation is one of the most frequent and relevant post-translational modifications and plays a key role in the modulation of protein properties particularly with regard to the half-life of the hormone, heterodimer stability and the intrinsic bioactivity. The carbohydrate content of LH is approximately 15%(N50) while that of FSH is 20%(N25,N42), and that of hCG is 30%(N33,N50) and the circulatory half-lives of the gonadotropins are about 20 mins for LH, 2 hours for FSH, and 12–24 hoursfor hCG. Molecular alterations of V-LHB, due to rs1800447 (Trp28Arg) and Ile35Thr (rs34349826) create an extra glycosylation signal (Asn-X-Thr) into the LHB chain, which introduces an oligosaccharide side chain into Asn13, similar to that present in HCG. This might increase the affinity binding between the peptide portion of the hormone and the receptor and also increase the lifespan of the hormone (Shafaghiet al., 2019). Findings using serum variant homozygotes showed that V-LH is more active than WT-LH in bioassays in vitro, but it has a shorter half-life in circulation. The shorter half-life of V-LH is possibly compensated for by about (40%) higher promoter activity of the gene, explained by 8 SNPs in the (50-flanking regions) of V-LHB. They were reported as having a modulatory effect on the hyperandrogenemia of PCOS. More recently, Alviggi et al. have confirmed that v-LHB polymorphism produces a less active form of the hormone which is not able to support satisfactorily FSH activity during controlled ovarian stimulation, and that the v-LHβ carriers experience a considerable decrease of the number of transferred embryos.Presence of this mutation statistically associated with high serum levels of LH and testosterone and irregular menstrual cycles but not linked to recurrent abortions that highlights the essential role of LH/FSH cooperation in the latest stages of follicle maturation.
The polymorphism rs5030775 (A18T) is associated with more potent stimulation of the IP3 response than wild type LH mapped on the signal peptide position, which is a short peptide located in the N-terminal of proteins which is responsible for protein recognition and secretion and it is often cleaved to generate the mature protein. Therefore, presence of this mutation within the leader sequence,which has been reported as potential stimulator of IP3 in contrast to the cAMP pathway, could cause an alteration of GnRH pulse frequency due to overstimulation of IP3. This in turn increase would LHb gene expression and might influence abnormal recognition of the prohormone within the endoplasmic reticulum when binding with SRP occurs. This would affect its interaction with the LHCGR receptor. Interestingly, a point mutation associated with autosomal recessive familial isolated hypoparathyroidism caused improper cleavage by signal peptidase at the normal position. Remarkably, this mutation ((historically reported as Thr-3A) A18T) was also found in 3% of the Rwanda population with a heterogeneous pattern that might be a sign of the evolutionarily background origin of PCOS and support the idea that a high level of serum LHB isassociated with increased pulse frequencies because of high GnRH pulse frequencies that favor LHB gene expression, whereas low GnRH pulse frequencies favor FSHB gene expression.
We are not aware of any literature in regarding to rs746167425 (R22K) and rs35270001 (H30R).With regards to their physiochemical properties Arginine mutated into a Lysine at position 22, which is smaller,would not be expected to affect protein stability. However, Histidine, located very close to a residue that makes a cysteine bond, formsa hydrogen bond with Tryptophan on position 28. When mutated to Arginine there is positive charge and a reduction in size. This creates an extra glycosylation site on the mutated formthat might cause loss of hydrophobic interactions with other molecules on the surface of the protein.
In conclusion, giving a patient the diagnosis of PCOS makes the patient aware of possible fertility concerns, dysfunctional bleeding, endometrial cancer, obesity, diabetes, dyslipidemia, hypertension, and theoretical increased risk of cardiovascular disease. Since PCOS has genetic elements, knowledge of polymorphisms that affect LH action may bring awareness of PCOS to family members and future children. Given that insulin resistance is heavily associated with PCOS, these individuals could be directed to increased screening and will likely have better long-term outcomes with early lifestyle interventions, as well as insulin sensitizing medication, such as metformin when indicated. In addition, screening for hyperlipidemia could lead to earlier lifestyle/medical intervention could likely help reduce cardiovascular outcomes.
Data Availability
I Nidal Essa under signed, declare and affirm that this thesis is our own original work. I have followed all ethical and technical principles in the preparation, data collection, data analysis and compilation of this Thesis. Any scholarly matter that is included in the Thesis has been given recognition through citation. I, solemnly declare that this Thesis has not been submitted to any other institution anywhere for the award of any academic degree, diploma or certificate.
Footnotes
The results part updated with the addition of more tables, also the discussion part updated with more refereance.
References




